Calcaneal Malunion Correction: Extensile Lateral Approach
Key Takeaway
The extensile lateral approach for calcaneal malunion correction provides optimal exposure for lateral wall exostectomy, subtalar arthrodesis, and hindfoot realignment. This comprehensive surgical technique addresses subfibular impingement and post-traumatic arthritis. Key steps include meticulous subperiosteal flap elevation, sural nerve protection, en bloc resection of the lateral wall exostosis for autografting, and rigid internal fixation to restore hindfoot biomechanics and alleviate chronic pain.
Comprehensive Introduction and Patho-Epidemiology
The management of calcaneal malunions presents one of the most formidable and technically demanding challenges in reconstructive foot and ankle surgery. Following either nonoperative management of displaced intra-articular calcaneal fractures or failed surgical fixation, patients frequently develop a predictable, progressive, and debilitating cascade of pathoanatomic changes. The classic calcaneal malunion is characterized by a multiplanar deformity: profound loss of calcaneal height, significantly increased heel width, severe varus malalignment of the calcaneal tuberosity, and advanced, symptomatic post-traumatic subtalar arthritis. This complex spatial distortion not only alters the intrinsic biomechanics of the hindfoot but also severely compromises the adjacent soft tissue envelope, rendering surgical reconstruction a high-risk endeavor requiring meticulous planning and execution.
Epidemiologically, the incidence of symptomatic calcaneal malunions remains significant, largely due to the inherent controversies surrounding the initial management of calcaneal fractures. While modern internal fixation techniques have improved primary outcomes, a substantial subset of patients—particularly those with severe comminution, compromised soft tissues at the time of injury, or significant medical comorbidities—are initially managed nonoperatively. A significant percentage of these patients will progress to symptomatic malunion within one to three years post-injury. Furthermore, even with operative intervention, inadequate reduction of the tuberosity fragment or failure to restore the posterior facet can lead to late collapse and subsequent malunion. The resulting disability is profound, with patients frequently reporting intractable lateral hindfoot pain, inability to ambulate on uneven surfaces, and severe limitations in both occupational and recreational activities.
The clinical presentation of a calcaneal malunion is heavily dictated by the specific pathoanatomy, which was elegantly categorized by Stephens and Sanders. Their classification system remains the cornerstone of surgical decision-making. Type I malunions are characterized primarily by a lateral wall exostosis resulting in subfibular impingement, but critically, the subtalar joint remains congruent and asymptomatic. Type II malunions present with the same lateral wall blowout and subfibular impingement, but are complicated by the presence of post-traumatic subtalar arthritis, necessitating subtalar arthrodesis. Type III malunions represent the most severe end of the spectrum, combining lateral wall exostosis, subtalar arthritis, and profound varus malalignment of the calcaneal tuberosity. This varus deformity is particularly deleterious, as it forces the patient to ambulate on the lateral border of the foot, leading to lateral column overload, recurrent ankle instability, and eventual breakdown of the transverse tarsal joints.
The extensile lateral approach remains the unequivocal gold standard for addressing these complex, multiplanar deformities. It provides unparalleled, panoramic access to the lateral calcaneal wall for exostectomy, the subtalar joint for comprehensive debridement and arthrodesis, and the calcaneal body for corrective osteotomies. While minimally invasive techniques have gained traction for acute fracture management, the chronic, consolidated nature of a malunion—coupled with the necessity for extensive bony resection, structural grafting, and multiplanar realignment—demands the robust exposure afforded by the extensile lateral approach. This masterclass details the step-by-step surgical execution of calcaneal malunion correction, adhering to the biomechanical and anatomic principles popularized by Clare, Lee, Myerson, and Sanders.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the complex surgical anatomy and altered biomechanics of the hindfoot is absolutely paramount for the successful execution of a calcaneal malunion correction. The lateral aspect of the hindfoot is covered by a relatively thin, precarious soft tissue envelope that is notoriously unforgiving. The vascular supply to the lateral extensile flap is predominantly derived from the lateral calcaneal artery, a terminal branch of the peroneal artery. This vessel arborizes extensively within the subcutaneous tissues, forming a delicate angiosome that supplies the lateral heel and the skin overlying the lateral calcaneal wall. The surgical incision must be meticulously designed to incorporate this vascular network within a full-thickness fasciocutaneous flap. Any attempt to develop subcutaneous planes or thin the flap will inevitably result in ischemic necrosis, a catastrophic complication that can expose the underlying hardware and bone graft.
Neurologically, the sural nerve is the primary structure at risk during the extensile lateral approach. The nerve typically courses distally along the posterolateral aspect of the calf, passing approximately 1.5 to 2.0 centimeters posterior and inferior to the tip of the lateral malleolus before branching into the lateral dorsal cutaneous nerve. In the setting of a calcaneal malunion, the normal anatomic landmarks are frequently distorted by the lateral wall blowout, and the nerve may be displaced or tethered by dense scar tissue. The vertical limb of the surgical incision must be placed posterior to the anticipated course of the sural nerve, allowing the nerve to be safely elevated and protected within the anterior aspect of the full-thickness flap. At the distal extent of the horizontal limb, the terminal branches of the sural nerve frequently cross the surgical field near the calcaneocuboid joint and must be meticulously identified and preserved to prevent painful postoperative neuromas.
Biomechanically, the normal calcaneus functions as a critical lever arm for the Achilles tendon and serves as the foundational strut for the lateral column of the foot. In the setting of a malunion, the loss of calcaneal height significantly decreases the talocalcaneal angle (talar declination angle). This loss of height forces the talus into a dorsiflexed, horizontal position within the ankle mortise. The horizontal talus alters the instantaneous center of rotation of the ankle joint, leading to anterior tibiotalar impingement, restricted ankle dorsiflexion, and a functionally shorter Achilles lever arm, which manifests clinically as a profound loss of push-off strength during the terminal stance phase of gait. Restoring calcaneal height is therefore not merely an aesthetic consideration, but a critical biomechanical imperative to restore normal ankle kinematics and gastrocsoleus efficiency.
The lateral wall blowout, a hallmark of the calcaneal malunion, results in severe fibulocalcaneal abutment. As the calcaneus fractures and collapses, the lateral wall is extruded laterally, directly abutting the distal tip of the fibula. This osseous impingement obliterates the normal subfibular space, severely compressing the peroneal tendons (peroneus longus and brevis) and the sural nerve against the lateral malleolus. This compression is a primary driver of chronic lateral hindfoot pain and frequently leads to peroneal tendinopathy, tenosynovitis, or frank tearing of the tendons. Furthermore, the varus malalignment of the calcaneal tuberosity shifts the mechanical axis of the lower extremity medial to the subtalar joint axis. This creates an obligate varus thrust during weight-bearing, overloading the lateral collateral ligaments of the ankle and the lateral column of the foot. Correction of this varus deformity, either through a structural opening wedge bone block or a closing wedge Dwyer osteotomy, is absolutely essential to centralize the mechanical axis and protect the adjacent articulations from accelerated degeneration.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention for a calcaneal malunion requires a comprehensive evaluation of the patient's symptoms, functional demands, medical comorbidities, and the specific pathoanatomy of the deformity. Surgery is generally indicated for patients who have failed an exhaustive trial of nonoperative management, which typically includes custom orthotics with lateral wedges and heel lifts, rigid ankle-foot orthoses (AFOs), non-steroidal anti-inflammatory drugs (NSAIDs), and targeted physical therapy. The primary surgical indications include intractable lateral hindfoot pain secondary to subfibular impingement and peroneal tendon compression, severe midfoot or subtalar pain due to post-traumatic arthritis, and significant gait dysfunction resulting from a horizontal talus, anterior ankle impingement, or severe varus malalignment of the tuberosity.
Patient selection is arguably the most critical determinant of surgical success. The extensile lateral approach carries a notoriously high risk of wound complications, and these risks are exponentially magnified in patients with specific medical comorbidities. A rigorous preoperative medical optimization protocol is mandatory. Smoking is considered an absolute contraindication by many reconstructive surgeons due to its profound deleterious effects on microvascular perfusion and bone healing. Patients must commit to absolute smoking cessation for a minimum of six weeks prior to surgery and three months postoperatively, ideally confirmed by negative serum or urine cotinine levels. Similarly, poorly controlled diabetes mellitus (HbA1c > 7.5%), severe peripheral vascular disease, and active local or systemic infections are absolute contraindications to this major reconstructive procedure.
Relative contraindications include advanced patient age, severe osteoporosis (which compromises hardware purchase and bone graft incorporation), and a history of non-compliance with postoperative weight-bearing restrictions. Patients with pre-existing neuropathic conditions, such as Charcot neuroarthropathy, require highly individualized decision-making, as the risk of catastrophic failure and progressive deformity is significantly elevated. In cases where the soft tissue envelope is severely compromised by previous incisions, extensive scarring, or prior skin grafting, the extensile lateral approach may be contraindicated, and alternative techniques, such as a medial approach for subtalar arthrodesis combined with a percutaneous lateral wall exostectomy, may need to be considered.
| Indication / Contraindication Category | Specific Conditions and Parameters | Clinical Rationale and Surgical Implications |
|---|---|---|
| Absolute Indications | Intractable subfibular impingement; Symptomatic post-traumatic subtalar arthritis (Types II/III); Severe varus malalignment causing lateral column overload. | Mechanical impingement and end-stage arthritis will not improve with conservative care. Varus malalignment inevitably leads to adjacent joint breakdown. |
| Relative Indications | Anterior ankle impingement secondary to a horizontal talus; Peroneal tendinopathy/tearing due to lateral wall blowout. | Restoring calcaneal height improves ankle kinematics. Decompression of the subfibular space is required to salvage the peroneal tendons. |
| Absolute Contraindications | Active smoking or nicotine use; Poorly controlled diabetes (HbA1c > 7.5%); Severe peripheral arterial disease (ABI < 0.5); Active infection. | Unacceptable risk of catastrophic flap necrosis, deep infection, and nonunion. Vascular surgery consultation is mandatory if PAD is suspected. |
| Relative Contraindications | Advanced age with low functional demands; Severe osteopenia/osteoporosis; History of medical non-compliance; Compromised lateral soft tissue envelope. | Poor bone quality limits hardware purchase. Non-compliance with strict NWB protocols will result in hardware failure and graft collapse. |
Pre-Operative Planning, Templating, and Patient Positioning
Comprehensive preoperative planning and meticulous imaging are the absolute foundations of a successful calcaneal malunion correction. Standard weight-bearing radiographs must be obtained, including anteroposterior (AP), lateral, and Harris axial views of the hindfoot. The lateral radiograph is critically evaluated to quantify the loss of calcaneal height, the reduction or reversal of Böhler’s angle, the alteration of Gissane’s angle, and the presence of anterior tibiotalar impingement caused by the horizontal talus. The lateral view also provides an initial assessment of the subtalar joint congruency and the degree of post-traumatic arthritic change. The Harris axial view is indispensable for evaluating the overall heel width, the precise degree of varus or valgus malalignment of the calcaneal tuberosity, and the severity of the lateral wall blowout and subfibular impingement.
While plain radiographs provide a global overview of the deformity, a fine-cut computed tomography (CT) scan with multiplanar (sagittal, coronal, and axial) reconstructions is the definitive imaging modality and is considered mandatory prior to surgical intervention. Coronal CT reconstructions are essential for precisely quantifying the lateral wall blowout, measuring the distance between the extruded lateral wall and the distal fibula, and evaluating the status of the posterior facet of the subtalar joint. Sagittal CT reconstructions are utilized to evaluate the anterior and middle facets of the subtalar joint, as well as the calcaneocuboid joint, which may also be involved in the malunion or exhibit secondary osteoarthritic changes requiring concurrent arthrodesis. Furthermore, 3D CT reconstructions can be highly beneficial for spatial orientation and preoperative templating, allowing the surgeon to precisely calculate the size and shape of the structural bone graft required to restore calcaneal height and correct the varus deformity.
Preoperative templating involves calculating the exact dimensions of the lateral wall exostectomy and determining how this autologous bone block will be utilized. In Type II and Type III malunions, the resected lateral wall serves as an ideal, dense cortical-cancellous structural autograft. The surgeon must template the anticipated distraction of the subtalar joint required to restore the talocalcaneal angle and correct the varus malalignment, ensuring that the harvested lateral wall fragment will be of sufficient volume to fill the resulting void. If the anticipated defect exceeds the volume of the lateral wall autograft, the surgeon must be prepared to harvest structural iliac crest bone graft (ICBG) or utilize bulk structural allografts (e.g., femoral head or tricortical iliac crest allograft) to supplement the reconstruction.
Optimal patient positioning is critical for adequate surgical exposure, ease of multiplanar fluoroscopic imaging, and the safety of the patient during a prolonged reconstructive procedure. The patient is placed in the strict lateral decubitus position on a radiolucent operating table. A vacuum beanbag is utilized to securely stabilize the torso and pelvis. An axillary roll must be placed to protect the dependent brachial plexus. The normal (contralateral) leg should be positioned down, flexed at the hip and knee, and moved entirely out of the fluoroscopic field, anterior to the injured extremity. All bony prominences, including the dependent fibular head and greater trochanter, must be heavily padded to prevent perioperative neuropraxia or pressure necrosis. A well-padded pneumatic tourniquet is applied to the proximal thigh. The leg is prepped and draped in a standard sterile fashion, ensuring visualization from the proximal third of the tibia down to the toes. Prior to incision, the extremity is exsanguinated using an Esmarch bandage, and the tourniquet is inflated to 350 mm Hg. The surgeon must remain acutely aware of tourniquet time; in the setting of compromised lateral soft tissues, prolonged ischemic time can severely exacerbate postoperative wound healing complications. Tourniquet inflation should ideally be kept under 120 minutes, with a deflation period utilized if the surgery extends beyond this timeframe.
Step-by-Step Surgical Approach and Fixation Technique
Flap Design and Elevation
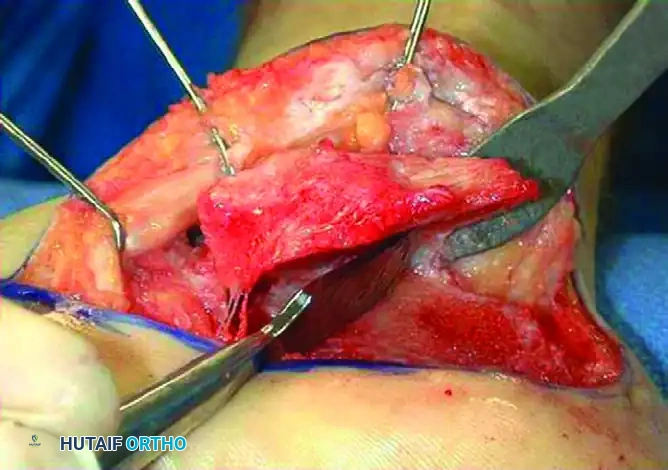
The extensile lateral approach is designed to create a robust, full-thickness fasciocutaneous flap that preserves the delicate vascular supply to the lateral hindfoot. The incision is a classic L-shaped design. The vertical limb is initiated approximately 3 to 5 centimeters proximal to the tip of the lateral malleolus, placed strictly midway between the posterior border of the fibula and the anterior border of the Achilles tendon. This posterior placement is critical, as it allows the sural nerve to be safely elevated within the anterior aspect of the flap. The incision is carried distally to the junction of the glabrous (plantar) and non-glabrous (lateral) skin. At this point, a smooth, sweeping 90-degree turn is made to create the horizontal limb, which extends distally in line with the base of the fifth metatarsal, terminating just proximal to the calcaneocuboid joint.
The incision must be deepened directly and sharply down to the periosteum of the calcaneus in a single, decisive pass. The creation of subcutaneous planes or the use of electrocautery near the skin edges is strictly prohibited, as this will inevitably compromise the subdermal vascular plexus and lead to marginal flap necrosis. Using a sharp periosteal elevator, a full-thickness subperiosteal flap is elevated off the lateral wall of the calcaneus. The elevation proceeds from inferior to superior and from posterior to anterior. The calcaneofibular ligament (CFL) is sharply detached from its insertion on the calcaneus, allowing the peroneal tendons to be elevated superiorly within the flap. The surgeon must exercise extreme caution at the distal extent of the horizontal limb, meticulously identifying and protecting the terminal branches of the sural nerve as they cross the surgical field.
Retraction and Exposure
Traditional self-retaining retractors (e.g., Weitlaner or Gelpi retractors) must be completely avoided, as they exert focal, crushing pressure on the delicate flap edges, leading to ischemia and postoperative wound dehiscence. Instead, the "no-touch" K-wire retraction technique is mandatory. Three 1.6-mm (0.062-inch) Kirschner wires are utilized to retract the full-thickness subperiosteal flap and the peroneal tendons superiorly and anteriorly, completely out of the surgical field.
The first K-wire is driven into the distal tip of the fibula. The second K-wire is driven into the lateral aspect of the talar neck. The third K-wire is driven into the cuboid. Once secure, these wires are carefully bent back upon themselves to gently cradle and hold the flap superiorly. This technique provides unparalleled, panoramic access to the entire lateral calcaneal wall, the posterior facet of the subtalar joint, and the calcaneocuboid joint, all while minimizing mechanical trauma to the soft tissue envelope.
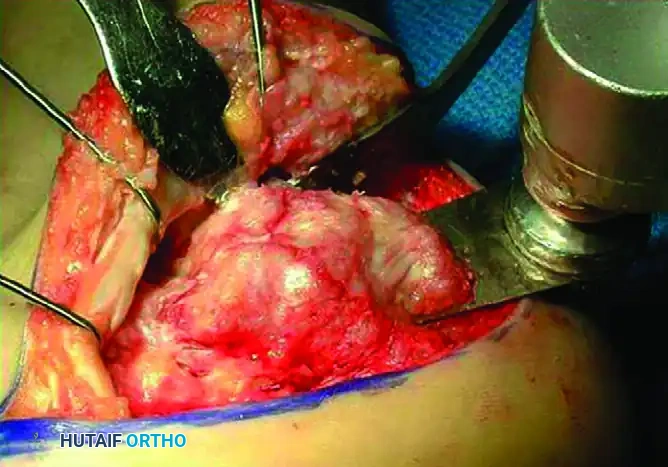
Lateral Wall Exostectomy and Decompression
In all types of calcaneal malunions (Types I, II, and III), the extruded lateral wall exostosis must be radically resected to relieve subfibular impingement and completely decompress the peroneal tendons. The lateral wall is carefully freed of all remaining soft tissue attachments, dissecting as far distally as the calcaneocuboid articulation. To protect the vital plantar neurovascular bundle, a wide Hohmann retractor is carefully placed on the plantar aspect of the calcaneus. A second Hohmann retractor is placed over the anterior process of the calcaneus to protect the dorsal structures.
The exostectomy is initiated using a thin-bladed, oscillating AO osteotomy saw. The osteotomy begins posteriorly, just anterior to the Achilles tendon insertion, and is advanced distally towards the calcaneocuboid joint. The saw blade must be angled slightly medially relative to the longitudinal axis of the calcaneus. This specific trajectory is critical: it leaves more residual bone plantarly to maintain the structural integrity of the calcaneal body, while aggressively resecting the superior aspect of the lateral wall to completely decompress the subfibular space. The surgeon must exercise meticulous control during the superior aspect of the saw cut to avoid inadvertent violation of the talofibular joint or the lateral aspect of the talus.

The distal extension of the malunion frequently involves the calcaneocuboid joint. The residual overhang of the lateral wall in this region often creates a mechanical osseous block to the motion of the transverse tarsal joint. The exostectomy must be continued distally to remove this overhang and the lateral one-fourth of the distal aspect of the calcaneus. To prevent inadvertent saw blade damage to the articular surface of the cuboid, the final distal completion of the exostectomy should be performed manually using a sharp, wide osteotome. The lateral wall fragment is then meticulously removed en bloc.

This excised lateral wall fragment is a highly valuable piece of dense, cortical-cancellous bone. It must be preserved as a single, intact piece on the back table. In Type II and Type III malunions, this fragment will serve as the primary autologous bone block for structural grafting, utilized to restore calcaneal height and correct the varus deformity during the subtalar arthrodesis.

Subtalar Joint Preparation and Arthrodesis
In Type II and Type III calcaneal malunions, the subtalar joint is irreversibly damaged by post-traumatic arthritis and requires a definitive arthrodesis. Attention is directed to the posterior facet of the subtalar joint. A stout lamina spreader is inserted into the posterior facet and gently opened to distract the joint, significantly improving visualization of the articular surfaces.
Meticulous joint preparation is the most critical factor in achieving a successful arthrodesis. All remaining articular cartilage, fibrous scar tissue, and sclerotic subchondral bone must be aggressively debrided from both the talar and calcaneal sides of the joint. This is accomplished using a combination of sharp periosteal elevators, ring curettes, and curved osteotomes. Once the subchondral bone is exposed, it must be aggressively penetrated using a high-speed burr or a 2.0-mm drill bit (subchondral drilling or "feathering"). This process breaks through the sclerotic bone and exposes the underlying vascularized, bleeding cancellous bone, optimizing the biological environment for osteogenesis and fusion.
Deformity Correction and Internal Fixation
Type III malunions present with severe varus malalignment of the hindfoot, which must be anatomically corrected to centralize the mechanical axis and prevent ongoing lateral column overload. This correction is achieved through the strategic placement of the structural bone block. The previously harvested lateral wall autograft is meticulously contoured on the back table to match the dimensions of the distracted subtalar joint.
With the lamina spreader maintaining distraction and correcting the varus deformity, the contoured bone block is impacted into the subtalar joint space. The graft acts as a structural opening-wedge strut, simultaneously lateralizing the calcaneal tuberosity, correcting the varus malalignment, and restoring the critical talocalcaneal height. If the varus deformity is exceptionally rigid or severe, a supplemental laterally based closing wedge osteotomy of the calcaneal tuberosity (Dwyer osteotomy) may be required in addition to the subtalar arthrodesis.
Once the deformity is clinically corrected and the structural graft is perfectly positioned, the subtalar joint is provisionally stabilized with two large-fragment (2.0-mm or 2.5-mm) Kirschner wires or guide pins, driven from the plantar-posterior aspect of the calcaneal tuberosity into the body of the talus. Intraoperative fluoroscopy (AP, lateral, and Harris axial views) is strictly required at this stage to definitively verify the correction of the varus deformity, the restoration of calcaneal height, the anatomic position of the bone block, and the complete decompression of the subfibular space.
Definitive internal fixation of the subtalar arthrodesis is achieved using two or three large-diameter (6.5 mm or 7.3 mm) cannulated, partially threaded cancellous screws. The screws are inserted over the guide pins from the calcaneal tuberosity, directed anteriorly, superiorly, and slightly medially into the dense bone of the talar body and neck. The screws must be advanced with washers to prevent the screw heads from sinking into the osteopenic bone of the tuberosity, ensuring maximal, rigid compression across the arthrodesis site and the structural bone graft.
Wound Closure Techniques
The closure of the extensile lateral approach is arguably as critical as the deep reconstructive exposure. Wound dehiscence, marginal flap necrosis, and deep infection are the most devastating and frequently encountered complications of this procedure. Prior to closure, the surgical site is thoroughly irrigated with copious amounts of sterile saline. The tourniquet is released, and meticulous, exhaustive hemostasis is achieved using electrocautery to prevent postoperative hematoma formation, which can severely compromise flap perfusion by increasing tension on the suture line.
A medium closed-suction drain is placed deep to the fasciocutaneous flap and brought out through a separate stab incision proximally. The flap is then meticulously closed in a layered fashion. The deep subcutaneous tissues and the periosteal layer are reapproximated using interrupted, deep absorbable sutures (e.g., 2-0 or 3-0 Vicryl), ensuring that all tension is removed from the skin edges.
The skin is closed exclusively using the modified Allgöwer-Donati technique with non-absorbable monofilament sutures (e.g., 3-0 or 4-0 Nylon). This specific suturing technique is absolutely mandatory; it acts as a vertical mattress suture on the non-flap (plantar/posterior) side of the incision, but passes strictly through the deep dermis on the flap side, never exiting the epidermis of the flap. This technique provides robust mechanical eversion of the skin edges while completely eliminating strangulation of the delicate dermal capillary plexus on the critical corner and edges of the lateral flap.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, the correction of calcaneal malunions via the extensile lateral approach is associated with a high complication profile. The surgeon must be acutely aware of these risks and possess the reconstructive armamentarium to manage them effectively. Wound healing complications are the most common and feared adverse events. Marginal flap necrosis and superficial dehiscence occur frequently due to the tenuous vascularity of the lateral heel. These are initially managed with aggressive local wound care, strict elevation, and the application of negative pressure wound therapy (NPWT). If the necrosis progresses to full-thickness loss exposing the underlying hardware or structural bone graft, immediate surgical debridement is mandatory. Salvage in these catastrophic scenarios often requires the intervention of a microsurgical team for coverage with a free tissue transfer (e.g., anterolateral thigh or rectus abdominis free flap).
Sural neuritis or frank neuroma formation is another significant complication, resulting from direct intraoperative transection, excessive traction during flap retraction, or postoperative tethering within the dense lateral scar tissue. Prevention through meticulous incision placement and the "no-touch" retraction technique is paramount. If a symptomatic neuroma develops and fails conservative management (gabapentinoids, targeted steroid injections), surgical excision of the neuroma and burying of the proximal nerve stump deep into the muscular belly of the flexor hallucis longus or the soleus is required.
Nonunion of the subtalar arthrodesis is a major concern, particularly in patients with a history of smoking, diabetes, or inadequate preparation of the sclerotic joint surfaces. Nonunion presents as persistent, mechanical hindfoot pain and progressive loss of the achieved deformity correction. Diagnosis is confirmed via a fine-cut CT scan demonstrating failure of trabecular bridging across the arthrodesis site. Salvage management necessitates a revision arthrodesis. This involves removal of the existing hardware, aggressive re-debridement of the nonunion site down to bleeding bone, utilization of orthobiologics (e.g., bone marrow aspirate concentrate, demineralized bone matrix), placement of a new structural graft if height has been lost, and revision internal fixation, often utilizing a robust lateral column plate in addition to large-diameter compression screws to maximize biomechanical stability.
| Complication | Estimated Incidence Rate | Prevention and Salvage Management Strategies |
|---|---|---|
| Wound Dehiscence / Flap Necrosis | 10% - 25% | Prevention: "No-touch" retraction, Allgöwer-Donati closure, strict smoking cessation. Salvage: NPWT, local wound care; Free tissue transfer for exposed hardware/graft. |
| Sural Neuritis / Neuroma | 5% - 15% | Prevention: Posterior placement of vertical incision, meticulous distal dissection. Salvage: Gabapentinoids, targeted injections; Surgical excision and deep muscular burial of the proximal stump. |
| Subtalar Nonunion | 5% - 10% | Prevention: Aggressive joint debridement, rigid compression, strict NWB adherence. Salvage: Revision arthrodesis with structural grafting, orthobiologics, and augmented plate fixation. |
| Inadequate Decompression | 2% - 5% | Prevention: Intraoperative fluoroscopic verification, direct palpation of the subfibular space. Salvage: Revision lateral wall exostectomy and peroneal tendon tenolysis. |
| Deep Infection / Osteomyelitis | 1% - 3% | Prevention: Preoperative antibiotics, meticulous hemostasis, minimization of tourniquet time. Salvage: Hardware removal, aggressive serial debridements, culture-directed IV antibiotics, potential staged reconstruction. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following a calcaneal malunion correction is extensive and requires profound patient compliance. The protocol is strictly phased to protect the fragile soft tissue envelope during the initial healing phase and to ensure absolute mechanical stability of the structural bone graft and subtalar arthrodesis during the consolidation phase.
Phase I: Immediate Post-Operative
