Mastering Calcaneal Malunion Reconstruction: An Intraoperative Guide
Key Takeaway
Join us in the OR for an immersive masterclass on calcaneal malunion reconstruction. We'll meticulously detail the extensile lateral approach, lateral wall exostectomy, and subtalar bone block arthrodesis. This guide covers comprehensive anatomy, precise intraoperative techniques, and critical pearls for correcting hindfoot malalignment and restoring function in complex calcaneal deformities.
Comprehensive Introduction and Patho-Epidemiology
The surgical reconstruction of a calcaneal malunion represents one of the most formidable challenges in foot and ankle orthopedic surgery. This pathology is not merely a static skeletal deformity; it is a dynamic, complex disruption of the hindfoot's intricate biomechanics, leading to profound pain, altered gait kinematics, and severe functional impairment. A calcaneal malunion, fundamentally, represents persistent bony malalignment and its debilitating clinical consequences, stemming from inadequate initial management—whether conservative or operative—of a displaced intra-articular calcaneal fracture. It is a testament to the fact that the initial trauma initiates a cascade of structural failures that, if not meticulously corrected, will culminate in end-stage hindfoot dysfunction.
Epidemiologically, calcaneal fractures account for approximately 60% of all tarsal fractures, with the majority being intra-articular and occurring in the working-age population due to high-energy axial loading mechanisms, such as falls from height or motor vehicle collisions. When these fractures heal in a displaced position, the resulting pathoanatomy is highly predictable. The primary injury vector forces the talus downward into the calcaneus, driving the posterior facet inferiorly into the cancellous body, leading to a catastrophic loss of calcaneal height. Simultaneously, the calcaneal tuberosity is driven into a shortened, varus, and dorsiflexed position, while the lateral wall of the calcaneus "blows out" laterally due to the burst nature of the fracture.

The clinical sequelae of this uncorrected deformity are multifaceted and devastating to the patient's quality of life. The residual articular incongruity of the posterior facet inevitably leads to posttraumatic subtalar arthritis. The loss of calcaneal height results in a relative dorsiflexion of the talus within the ankle mortise, causing anterior ankle impingement and a profound loss of ankle dorsiflexion. Furthermore, the lateral wall expansion creates a massive bony exostosis that impinges upon the fibula—known as lateral subfibular impingement—which directly compresses the peroneal tendons, leading to severe tenosynovitis, stenosis, and frequent subluxation or dislocation. Finally, the varus malalignment of the hindfoot shifts the mechanical axis medially, overloading the lateral column of the foot and creating secondary midfoot and forefoot pathologies.

When evaluating these patients, a meticulous history and physical examination are paramount. The surgeon must ascertain the nature of the initial injury, the primary treatment modality, and the exact timeline of symptom progression. On physical examination, the soft tissue envelope must be scrutinized for previous surgical scars, dystrophic skin changes, and overall pliability, as this will dictate the safety of subsequent surgical incisions. The neurovascular status, particularly the function of the sural nerve, must be documented. Range of motion testing typically reveals a rigid, painful subtalar joint and restricted ankle dorsiflexion. Palpation will localize pain to the sinus tarsi (indicative of subtalar arthritis) or the subfibular region (indicative of lateral wall impingement and peroneal pathology).
Detailed Surgical Anatomy and Biomechanics
Before initiating any reconstructive intervention, a profound understanding of the normal osseous anatomy, articular relationships, and biomechanical function of the calcaneus is mandatory. The calcaneus is the largest tarsal bone, serving as the foundational pillar of the hindfoot. It is an irregularly shaped, robust structure designed to withstand immense ground reaction forces during the heel-strike phase of the gait cycle. Crucially, its posterior tuberosity acts as a vital lever arm for the gastrocnemius-soleus complex via the Achilles tendon, facilitating plantarflexion and forward propulsion. The internal architecture of the calcaneus features distinct trabecular patterns that intersect to support these loads, with a notable area of sparse trabeculae known as the neutral triangle, which is often the epicenter of fracture comminution and subsequent malunion settling.

The calcaneus forms critical articulations that dictate hindfoot motion. Superiorly, it articulates with the talus via three distinct facets—the posterior, middle, and anterior facets—creating the subtalar joint. The posterior facet is the largest and primary weight-bearing surface, while the middle facet is supported by the sustentaculum tali, a dense cortical projection on the medial aspect that often remains anatomically aligned with the talus even in severe fractures. Anteriorly, the calcaneus articulates with the cuboid, forming the calcaneocuboid joint. Together with the talonavicular joint, these articulations constitute the triple joint complex (or transverse tarsal joint). This complex functions as a highly synchronized mechanism; inversion of the subtalar joint locks the transverse tarsal joint to create a rigid lever for push-off, while eversion unlocks it, allowing the foot to become a supple shock absorber. Malunions disrupt this delicate coupling, resulting in a rigid, non-accommodative foot.

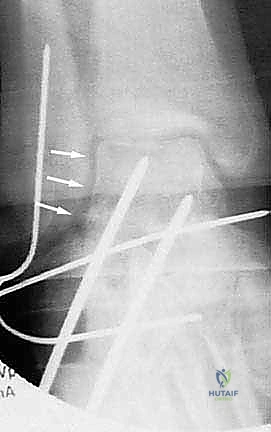
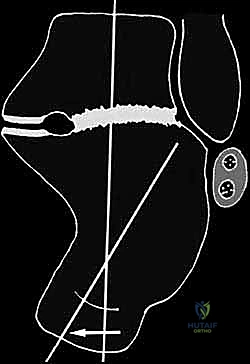
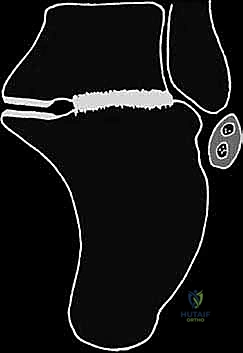
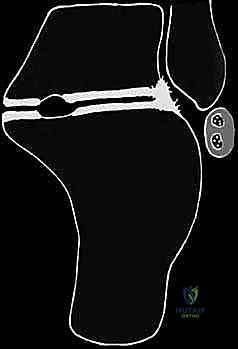
Radiographically, the normal orientation of the calcaneus is defined by several critical angles and measurements. The calcaneal pitch, formed by the intersection of a line along the plantar surface of the calcaneus and the horizontal ground line, normally ranges from 20 to 30 degrees. A decrease in this angle signifies a loss of calcaneal height. Böhler's angle, formed by lines drawn tangent to the anterior and posterior aspects of the superior calcaneal border, normally measures 20 to 40 degrees; flattening or reversal of this angle is a hallmark of severe posterior facet depression. The crucial angle of Gissane, formed by the intersection of the downward slope of the posterior facet and the upward slope of the anterior process, normally measures 100 to 130 degrees. Furthermore, the talocalcaneal height—the vertical distance from the superior dome of the talus to the plantar aspect of the calcaneus—is a critical metric for assessing the degree of vertical collapse.

The soft tissue envelope and neurovascular anatomy surrounding the lateral calcaneus are notoriously unforgiving and demand meticulous surgical respect. The vascular supply to the lateral hindfoot skin is predominantly derived from the lateral calcaneal artery, a terminal branch of the peroneal artery. This vessel supplies the angiosome corresponding to the standard extensile lateral approach flap. Compromise of this artery through poor incision placement or traumatic retraction inevitably leads to catastrophic flap necrosis. The sural nerve courses distally along the posterolateral aspect of the ankle, passing posterior to the peroneal tendons before terminating along the lateral border of the foot. It must be carefully protected within the anteriorly based surgical flap. Deep to the subcutaneous tissues, the peroneal longus and brevis tendons course posterior to the lateral malleolus and are stabilized by the superior and inferior peroneal retinacula. In the setting of a lateral wall blowout, these tendons are displaced laterally, stretched, and subjected to severe mechanical attrition against the fibula.
Exhaustive Indications and Contraindications
The decision to proceed with calcaneal malunion reconstruction is complex and must be highly individualized. Surgical intervention is primarily indicated for patients who have failed an exhaustive trial of conservative management, which typically includes custom orthotics, rigid ankle-foot orthoses (AFOs), activity modification, non-steroidal anti-inflammatory drugs (NSAIDs), and targeted physical therapy. The patient must demonstrate significant, localized pain that correlates directly with the radiographic and advanced imaging findings of the malunion. The Stephens and Sanders classification system for calcaneal malunions provides an excellent framework for determining operative indications based on the specific pathoanatomy present.
| Parameter | Indications for Surgical Reconstruction | Contraindications for Surgical Reconstruction |
|---|---|---|
| Patient Factors | Refractory daily pain, failed >6 months of conservative care, high functional demands, compliant with strict NWB protocols. | Active smoking (absolute or relative depending on surgeon protocol), severe medical comorbidities (ASA IV/V), non-compliance, psychiatric instability. |
| Vascular Status | Palpable pedal pulses, ABI > 0.9, normal capillary refill, healthy skin envelope. | Severe peripheral arterial disease (PAD), ABI < 0.5, lack of palpable pulses, active ischemic ulceration. |
| Soft Tissue | Pliable skin, healed previous surgical incisions, absence of active infection or severe lymphedema. | Active local infection, severe dystrophic changes, active CRPS, history of massive flap necrosis in the region. |
| Pathoanatomy | Type I: Lateral wall exostosis with intact subtalar joint. Type II: Subtalar arthritis + lateral wall exostosis. Type III: Subtalar arthritis + lateral wall exostosis + varus malalignment + loss of height. |
Asymptomatic malunion (radiographic deformity only), isolated forefoot pathology mimicking hindfoot pain. |
| Neurological | Intact protective sensation, capable of participating in postoperative rehabilitation. | Severe peripheral neuropathy (Charcot neuroarthropathy risk), complete paralysis of the lower extremity. |
Surgical indications are heavily influenced by the specific morphological components of the malunion. For isolated lateral subfibular impingement without significant subtalar arthritis or loss of height (Stephens and Sanders Type I), an isolated lateral wall exostectomy and peroneal tendon decompression may suffice. However, if the subtalar joint is arthritic and painful, an in situ subtalar arthrodesis combined with lateral wall exostectomy (Type II) is required. The most complex indication is the Type III malunion, characterized by subtalar arthritis, lateral wall blowout, severe loss of calcaneal height, and varus malalignment. These patients require a comprehensive reconstruction involving lateral wall exostectomy, subtalar arthrodesis, and a distraction bone block osteotomy to restore height, correct the varus deformity, and decompress the anterior ankle.
Contraindications must be strictly adhered to, as the complication profile of this surgery is substantial. Active smoking is a profound contraindication; the vasoconstrictive effects of nicotine drastically increase the risk of flap necrosis, wound dehiscence, and nonunion. Patients must commit to absolute smoking cessation, often verified by preoperative cotinine testing. Severe peripheral vascular disease and poorly controlled diabetes mellitus with peripheral neuropathy are also major contraindications, as the risk of catastrophic limb loss outweighs the potential benefits of pain relief. Furthermore, patients with a history of complex regional pain syndrome (CRPS) in the affected limb should be approached with extreme caution, as surgery can trigger a severe exacerbation.
Diagnostic injections play a critical role in confirming the indications for surgery and isolating the primary pain generators. A fluoroscopically guided injection of local anesthetic into the subtalar joint can differentiate intra-articular pain from extra-articular subfibular impingement. If the patient experiences complete relief of deep sinus tarsi pain following a subtalar injection, but lateral fibular pain persists during ambulation, it confirms the presence of both subtalar arthritis and lateral wall impingement. Conversely, if an injection into the peroneal tendon sheath relieves all lateral symptoms, the subtalar joint may not require arthrodesis, potentially sparing the patient a more extensive procedure.
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of a successful calcaneal malunion reconstruction. Standard weight-bearing radiographs of the foot and ankle, including anteroposterior (AP), lateral, and mortise views, are the initial step. The lateral view is scrutinized to assess the loss of calcaneal height, the talocalcaneal angle, and the presence of anterior ankle impingement. The mortise view is critical for evaluating the lateral wall expansion and its relationship to the fibula, as well as assessing the integrity of the ankle mortise itself. A Harris axial view is essential for visualizing the varus or valgus alignment of the calcaneal tuberosity and quantifying the degree of lateral wall blowout.


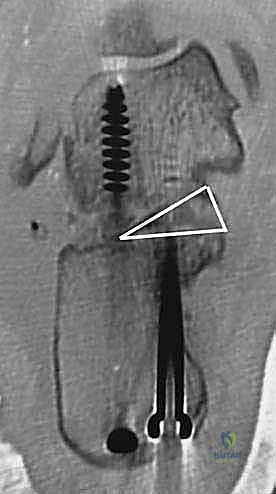
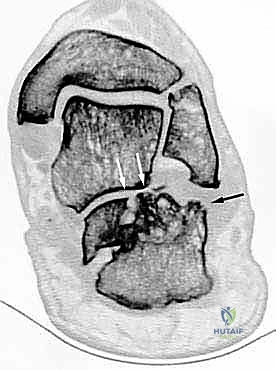
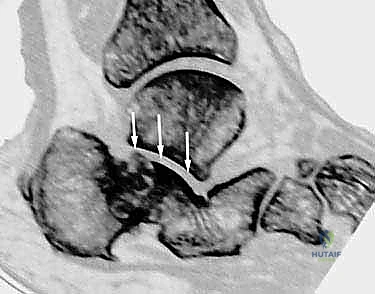
Advanced imaging with a high-resolution Computed Tomography (CT) scan is mandatory for all calcaneal malunions. Axial, sagittal, and coronal reformats provide a three-dimensional understanding of the deformity that plain radiographs cannot offer. Sagittal cuts allow for precise measurement of the posterior facet depression and the exact degree of height loss. Coronal cuts are invaluable for assessing the subtalar joint space, the presence of subchondral cysts or sclerosis, the severity of the lateral wall exostosis, and the status of the peroneal tendon sheath. Axial cuts help evaluate the calcaneocuboid joint, which may also be involved in the malunion and require concomitant arthrodesis.

Digital templating is a critical phase of the preoperative workflow. Using the contralateral, uninjured foot as a template (if available), the surgeon can calculate the exact dimensions of the structural bone graft required to restore calcaneal height and correct the varus deformity. The angle of the corrective wedge for a distraction arthrodesis is measured, ensuring that the talocalcaneal relationship will be restored to anatomical parameters. The trajectory and length of the planned fixation screws (typically 6.5mm or 7.3mm cannulated screws) are also mapped out to ensure adequate purchase in the dense bone of the talar body and neck, avoiding penetration into the ankle joint.
In the operating room, meticulous patient positioning is required to facilitate both the surgical exposure and intraoperative fluoroscopy. The patient is placed in the lateral decubitus position on a radiolucent operating table, with the operative leg facing upward. A vacuum beanbag is utilized to secure the torso, and an axillary roll is placed under the dependent axilla to protect the brachial plexus. All bony prominences are heavily padded. The operative leg is supported on a stack of sterile blankets or a specialized ramp to allow the C-arm to easily swing in for true AP, lateral, and axial views without obstruction from the contralateral limb. A thigh tourniquet is applied but inflated only after exsanguination and precise marking of the planned incision.
Step-by-Step Surgical Approach and Fixation Technique
The Extensile Lateral Approach and Soft Tissue Handling
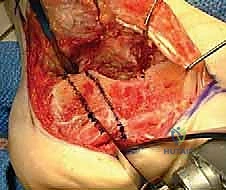
The surgical approach is arguably the most critical aspect of the procedure, as the viability of the lateral soft tissue flap dictates the overall success. An extensile lateral approach is universally utilized. The vertical limb of the incision begins approximately 2 to 3 cm proximal to the tip of the lateral malleolus, positioned just lateral to the Achilles tendon to ensure the sural nerve is safely captured within the anterior flap. The incision courses distally to the junction of the plantar and lateral skin, then curves gently anteriorly, following the glabrous line toward the base of the fifth metatarsal.
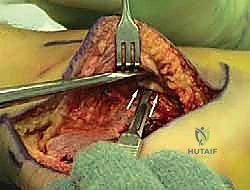
The incision is carried straight down to bone in a single, bold stroke to create a full-thickness subperiosteal flap. Skiving or creating separate subcutaneous planes is strictly prohibited, as it devascularizes the flap. The periosteum is elevated off the lateral wall of the calcaneus using a sharp Cobb elevator. Retraction of the flap must be atraumatic; self-retaining retractors are avoided. Instead, 1.6mm or 2.0mm K-wires are driven into the lateral malleolus, the talar neck, and the cuboid, and the flap is gently retracted using the smooth shafts of the wires. This "no-touch" retraction technique minimizes tension on the microvasculature of the flap, preserving the crucial lateral calcaneal artery.

Lateral Wall Exostectomy and Peroneal Tendon Decompression
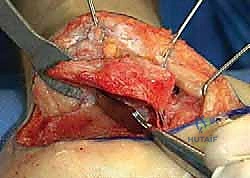
Once the flap is elevated, the massive lateral wall exostosis becomes immediately apparent. The peroneal tendons are carefully identified; they are often splayed, flattened, and encased in dense scar tissue over the exostosis. A meticulous tenolysis is performed, freeing the tendons from the fibula and the calcaneus. The calcaneofibular ligament (CFL) is typically contracted or scarred and is sharply released to allow full mobilization of the peroneal complex anteriorly.

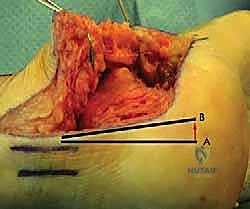
The lateral wall exostectomy is then performed. Using a broad osteotome or an oscillating saw, the prominent lateral wall is resected flush with the lateral border of the subtalar joint and the lateral malleolus. This step is critical for decompressing the subfibular space. The resected bone is carefully preserved on the back table; it is rich in osteoprogenitor cells and will be morselized to serve as high-quality local autograft to supplement the arthrodesis site, reducing the need for extensive iliac crest harvesting.


Subtalar Joint Preparation and Arthrodesis
With the lateral wall removed, the subtalar joint is fully exposed. A lamina spreader is inserted into the posterior facet to distract the joint. The residual articular cartilage, which is typically fibrillated and severely degenerated, is meticulously denuded using a combination of sharp curettes, osteotomes, and a high-speed burr. It is imperative to remove all cartilage down to bleeding subchondral bone to ensure a robust fusion mass. The preparation extends to the middle facet, which is often difficult to visualize but must be thoroughly debrided.

To stimulate osteogenesis, the subchondral bone of both the talus and the calcaneus is "feathered" using a 2.0mm drill bit or a sharp osteotome, creating multiple vascular channels. If a distraction bone block arthrodesis is planned (Type III malunion), a large lamina spreader is placed posteriorly in the joint and opened to restore the talocalcaneal height and pitch. This maneuver simultaneously pulls the talus out of dorsiflexion, decompressing the anterior ankle joint. The varus deformity is corrected by manipulating the calcaneal tuberosity into 5 degrees of valgus.

In Situ Fixation and Structural Grafting
With the deformity corrected and the joint distracted, the resulting void must be filled with a structural bone graft. A tricortical iliac crest autograft is the gold standard, providing both structural support and osteoinductive properties. Alternatively, a fresh-frozen femoral head allograft can be contoured to fit the defect, supplemented with the morselized local autograft obtained from the lateral wall exostectomy. The graft is meticulously shaped into a wedge to match the templated defect and impacted tightly into the subtalar space.
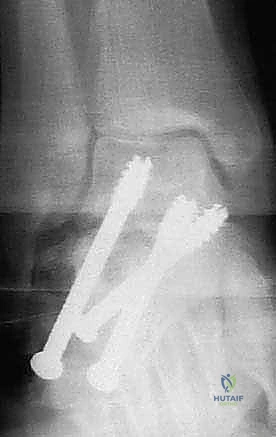
Fixation is achieved using two or three large-diameter (6.5mm or 7.3mm) cannulated, partially threaded screws. Guide pins are inserted from the posterior non-weight-bearing aspect of the calcaneal tuberosity, directed anteriorly, superiorly, and medially into the dense bone of the talar body and neck. Fluoroscopy is utilized extensively during this step to ensure optimal screw trajectory, maximum thread purchase in the talus, and avoidance of penetration into the ankle or talonavicular joints. The screws are advanced sequentially to provide rigid compression across the arthrodesis site and the structural graft.



Following final fluoroscopic confirmation of alignment and hardware placement, the wound is thoroughly irrigated. A closed suction drain is placed deep to the flap to prevent hematoma formation, which can compromise flap viability. The periosteum and subcutaneous tissues are closed meticulously with interrupted absorbable sutures, utilizing a modified Donati technique to evert the skin edges and minimize tension on the epidermis. The skin is closed with non-absorbable nylon sutures, and a bulky, well-padded posterior splint is applied in neutral dorsiflexion.