Mastering Intra-Articular Calcaneal Fracture Repair: An Extensile Lateral Approach
Key Takeaway
This masterclass guides fellows through the intricate repair of intra-articular calcaneal fractures using the extensile lateral approach. We cover comprehensive anatomy, meticulous preoperative planning, and granular, real-time surgical execution. Learn precise reduction techniques, hardware application, and critical intraoperative decision-making. We also delve into common pitfalls, salvage strategies, and detailed postoperative rehabilitation protocols to optimize patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
The management of displaced intra-articular calcaneal fractures remains one of the most formidable challenges in orthopedic traumatology. This injury represents far more than a simple osseous disruption; it is a catastrophic failure of the foundational keystone of the human foot, fundamentally altering hindfoot biomechanics, gait kinematics, and load transmission. For the orthopedic surgeon, the pursuit of meticulous anatomical restoration is not merely an academic exercise, but a critical prerequisite for providing the patient with a functional, pain-free extremity. The extensile lateral approach, when executed with precision and respect for the delicate soft tissue envelope, provides the necessary exposure to reconstruct this complex three-dimensional puzzle.
Historically, the treatment of calcaneal fractures has oscillated between conservative neglect and aggressive surgical intervention. However, modern advancements in advanced cross-sectional imaging, specifically computed tomography (CT), alongside the evolution of low-profile, anatomically contoured locking plate technology, have firmly established open reduction and internal fixation (ORIF) as the gold standard for appropriately selected patients. The primary objectives of surgical intervention are unambiguous: restoration of lateral column length, correction of varus/valgus malalignment of the tuberosity, exact anatomical reduction of the posterior facet of the subtalar joint, and decompression of the subfibular space to prevent peroneal tendon impingement.
Despite our best surgical efforts, the prognosis following a high-energy intra-articular calcaneal fracture is guarded. The initial trauma inflicts significant damage not only to the articular cartilage but also to the intricate soft tissue envelope, including the heel pad, local neurovascular structures, and tendinous complexes. Consequently, the surgeon must approach these injuries with a comprehensive understanding of the pathoanatomy, an appreciation for the limitations of surgical reconstruction, and a highly structured, evidence-based post-operative rehabilitation protocol. Failure to respect the stereotypic fracture patterns or the fragile lateral soft tissues invariably leads to catastrophic complications, including deep soft tissue necrosis, osteomyelitis, and intractable post-traumatic subtalar arthrosis.
Mechanism of Injury and Biomechanical Forces
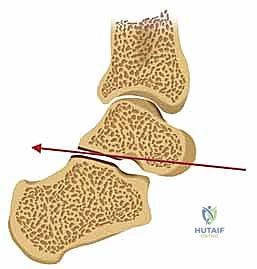
The classic mechanism of injury for an intra-articular calcaneal fracture involves a high-energy axial load, most frequently sustained during a fall from a height or a high-velocity motor vehicle collision. During the impact, the patient's body weight is driven downward through the tibia and into the talus. The talus, functioning essentially as a rigid, wedge-shaped anvil, is driven forcefully into the cancellous body of the calcaneus. The specific position of the foot at the exact moment of impact—specifically the degree of dorsiflexion or plantarflexion, and the presence of varus or valgus alignment—dictates the resulting fracture morphology.
This massive axial load generates a complex combination of shear and compression forces. The primary shear force is directed vertically, splitting the calcaneus into distinct medial and lateral fragments. Simultaneously, compressive forces crush the relatively softer cancellous bone of the calcaneal body beneath the articular facets. This crushing effect is responsible for the characteristic loss of calcaneal height, the flattening of Böhler's angle, and the lateral blow-out of the calcaneal wall. The lateral translation of the tuberosity and the lateral wall blow-out are particularly critical, as they lead to profound heel widening and subsequent impingement of the peroneal tendons against the distal fibula.
Understanding these forces is paramount for surgical reconstruction, as the reduction sequence must effectively reverse the mechanism of injury. The surgeon must employ longitudinal traction to restore length, apply varus or valgus moments to correct tuberosity alignment, and utilize direct elevation to restore the depressed articular fragments of the posterior facet. The energy imparted to the bone is directly proportional to the degree of comminution; thus, a fall from a higher elevation typically results in a more severe Sanders classification, rendering anatomical reconstruction exponentially more difficult.
Epidemiological Considerations and Patient Demographics
Calcaneal fractures account for approximately 2% of all adult fractures and represent roughly 60% of all tarsal bone fractures. The demographic distribution heavily skews toward young to middle-aged adult males, typically occurring in the third to fifth decades of life. This demographic is frequently associated with industrial or occupational hazards, such as construction workers, roofers, or painters, underscoring the significant socioeconomic impact of this injury. The prolonged disability and potential for permanent impairment often result in substantial lost wages and a high rate of failure to return to pre-injury employment levels.
Bilateral calcaneal fractures occur in approximately 5% to 10% of cases and serve as an absolute indicator of a massive axial load. In these high-energy scenarios, the orthopedic surgeon must maintain a high index of suspicion for associated injuries. Concomitant fractures of the lumbar spine (specifically burst fractures or compression fractures at the thoracolumbar junction) are present in up to 10% of patients with calcaneal fractures. Furthermore, associated injuries to the lower extremities, including tibial plateau fractures, pilon fractures, and contralateral foot and ankle trauma, are frequently observed and must be systematically ruled out during the secondary trauma survey.
The presence of patient-specific comorbidities significantly alters the epidemiological risk profile for surgical complications. Diabetes mellitus, peripheral vascular disease, and specifically, tobacco use, drastically increase the incidence of devastating wound complications following an extensile lateral approach. The literature clearly demonstrates that smokers have a multi-fold increased risk of marginal flap necrosis, deep infection, and subsequent need for amputation compared to non-smokers. Consequently, a thorough preoperative assessment of the patient's physiological age, vascular status, and social history is just as critical as analyzing the fracture morphology itself.
Detailed Surgical Anatomy and Biomechanics
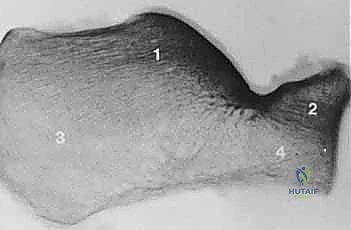
The calcaneus is the largest and most robust of the tarsal bones, serving a dual biomechanical role: it acts as an articulated, shock-absorbing foundation during the heel-strike phase of the gait cycle, and it functions as a powerful lever arm for the Achilles tendon during the push-off phase. Its complex, irregular three-dimensional geometry, coupled with its highly specialized internal trabecular architecture, makes precise surgical reconstruction a demanding endeavor. A profound understanding of both the osseous anatomy and the surrounding neurovascular envelope is non-negotiable for the orthopedic surgeon undertaking an extensile lateral approach.
Osteology and Trabecular Architecture
The internal structure of the calcaneus perfectly reflects its weight-bearing and force-transmitting functions. It is composed of a thin, fragile cortical shell enclosing a highly organized network of cancellous bone. We identify specific, dense trabecular systems within the juxta-articular regions, which are critical for surgical decision-making. The most prominent of these is the thalamic trabecular system, located directly beneath the posterior facet. This dense bone supports the articular surface and is the primary target for subchondral screw purchase during internal fixation.
In addition to the trabecular bone, specific regions of thick cortical bone are vital for achieving stable internal fixation. The medial wall of the calcaneus, particularly in the region of the sustentaculum tali, boasts a cortical thickness of 3 to 4 mm. The sustentaculum tali is firmly tethered to the talus by the robust deltoid and talocalcaneal ligaments, rendering it the "constant" fragment in almost all intra-articular fractures. Our entire reduction strategy hinges on mobilizing the displaced lateral fragments and securing them to this stable, intact medial sustentacular pillar. Another critical cortical strut is located superior-laterally, running between the cuboid facet and the posterior facet within the anterolateral fragment.
The articular anatomy is equally complex. The calcaneus articulates with the talus superiorly via three distinct facets: the anterior, middle, and posterior facets. The posterior facet is the largest and most biomechanically significant, bearing the majority of the axial load. Anteriorly, the calcaneus articulates with the cuboid in a saddle-shaped joint that is essential for preserving lateral column length and allowing multi-planar midfoot motion. Disruption of any of these articular surfaces, particularly the posterior facet, dramatically alters subtalar contact pressures, leading to rapid and progressive post-traumatic arthrosis if left unreduced.
Soft Tissue Envelopes and Neurovascular Structures
The soft tissues enveloping the calcaneus are notoriously unforgiving and are highly susceptible to iatrogenic injury during surgical exposure. The lateral skin and subcutaneous tissue are relatively thin and receive their vascular supply from a delicate network of perforating vessels arising from the peroneal and lateral calcaneal arteries. The trauma of the initial injury frequently results in severe soft tissue contusion, massive edema, and the formation of fracture blisters. Surgical intervention must be strictly delayed until this edema resolves and the skin demonstrates the characteristic "wrinkle sign," indicating that the soft tissue envelope can tolerate the surgical insult.
The sural nerve is a critical sensory structure that runs along the lateral aspect of the hindfoot and is highly vulnerable during the extensile lateral approach. It typically courses distally, posterior to the fibula, crossing the lateral wall of the calcaneus. The traditional L-shaped extensile incision is designed to mobilize this nerve within the full-thickness anterior flap, thereby protecting it from direct trauma or traction injury. However, meticulous dissection and careful retraction are paramount, as sural neuritis or neuroma formation is a common and highly distressing postoperative complication.
Deep to the subcutaneous tissues lie the peroneal tendons (longus and brevis). These tendons course posterior to the lateral malleolus and run along the lateral wall of the calcaneus. In the setting of a displaced intra-articular fracture, the lateral wall of the calcaneus frequently blows out laterally, impinging the peroneal tendons against the fibula. During the surgical approach, these tendons must be carefully elevated and retracted anteriorly within the full-thickness flap. Medially, the posterior tibial neurovascular bundle (comprising the posterior tibial artery, tibial nerve, and accompanying veins) courses posterior to the medial malleolus. While not directly exposed during a standard lateral approach, the surgeon must remain acutely aware of its proximity, particularly when passing drills or screws from lateral to medial into the sustentacular fragment, to avoid catastrophic neurovascular injury.
Fracture Morphology and Classification Systems
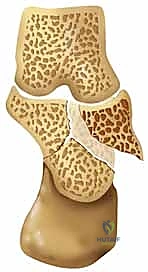
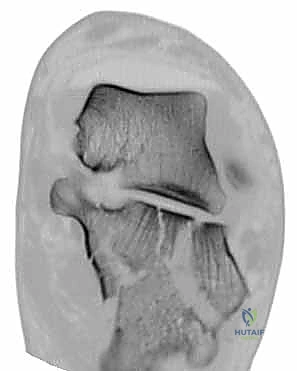
Before making any incision, the surgeon must possess a crystal-clear understanding of the injury's unique pathoanatomical fingerprint. Despite the seemingly infinite variations in comminution, calcaneal fractures exhibit stereotypic fracture lines, fragments, and displacements that dictate our surgical strategy. The talus, acting as a wedge, generates two primary fracture lines.
The First Primary Fracture Line occurs in the sagittal plane, splitting the angle of Gissane and dividing the calcaneus into distinct anterior and posterior fragments. It typically splits either the middle or anterior facet and continues onto the lateral wall in an inverted Y shape. The Second Primary Fracture Line divides the calcaneus into medial and lateral halves, shearing the posterior facet into two or more fragments. As the talus continues its compressive force, the lateral half of the posterior facet is severely impacted into the cancellous body of the calcaneus, creating the characteristic articular step-off.
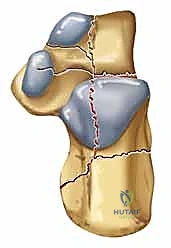
These primary fracture lines yield four major fracture components:
1. Superomedial Fragment (Sustentacular Fragment): This fragment retains its alignment to the talus due to strong ligamentous attachments and serves as the foundation for reconstruction.
2. Anterolateral Fragment: Typically displaces superiorly and extends into the cuboid facet; crucial for restoring lateral column length.
3. Posterior Facet: The most critical articular surface, which breaks into patterns classified by the Sanders system.
4. Tuberosity: Often driven superiorly, tilting into varus or valgus, and translating laterally, causing heel widening.



We rely heavily on the Sanders Classification, based on coronal CT imaging, to categorize the posterior facet disruption.
* Sanders II: Two main articular pieces (one fracture line).
* Sanders III: Three main articular pieces (two fracture lines).
* Sanders IV: Multifragmentary, severely comminuted articular surface.
Furthermore, the Essex-Lopresti classification distinguishes between tongue-type and joint depression patterns based on the lateral radiograph. In a tongue-type fracture, the tuberosity maintains a connection with the posterior facet, often allowing for percutaneous reduction techniques. In a joint depression pattern, the articular surface is completely separated and driven into the cancellous body, almost uniformly necessitating an open reduction.
Exhaustive Indications and Contraindications
The decision to proceed with operative management of a calcaneal fracture requires a complex calculus balancing the mechanical necessity of restoring the articular surface against the profound risks of surgical intervention. Not every displaced fracture warrants an extensile lateral approach, and patient selection is arguably the most critical determinant of a successful outcome. The surgeon must evaluate the fracture characteristics, the integrity of the soft tissue envelope, and the patient's physiological and psychological capacity to adhere to a strict, prolonged rehabilitation protocol.
Operative intervention is generally indicated for displaced intra-articular fractures involving the posterior facet (typically defined as >2 mm of articular step-off), significant loss of calcaneal height (flattening of Böhler's angle), severe varus or valgus malalignment of the tuberosity, and profound heel widening leading to subfibular impingement. Displaced fractures of the anterior process involving >25% of the calcaneocuboid joint also warrant open reduction to restore lateral column length and midfoot kinematics.
Conversely, conservative management (cast immobilization and strict non-weight bearing) is reserved for truly non-displaced or minimally displaced extra-articular fractures, patients with severe baseline immobility, or those with absolute medical contraindications to surgery. The role of primary subtalar arthrodesis is increasingly recognized for highly comminuted Sanders IV fractures, particularly in older patients or those where anatomical reconstruction of the posterior facet is deemed impossible.
Patient Selection Criteria
The ideal candidate for an extensile lateral approach is a young, healthy, non-smoking, compliant patient with an isolated, closed, displaced Sanders Type II or III joint depression fracture. In this optimal scenario, the benefits of restoring normal hindfoot anatomy and biomechanics far outweigh the surgical risks. The patient must possess the cognitive capacity to understand the severity of the injury, the necessity of a strict 10-to-12-week non-weight-bearing period, and the reality that despite a perfect radiographic result, they may still experience long-term stiffness or mild residual pain.
Age alone is not a strict contraindication, but physiological age and baseline activity level must be heavily weighted. An active 65-year-old may benefit greatly from ORIF, whereas a sedentary 50-year-old with multiple medical comorbidities may be better served with non-operative management or a minimally invasive approach. The patient's occupation also plays a role; individuals requiring prolonged standing, walking on uneven surfaces, or heavy lifting (e.g., construction workers) have a much higher functional demand on their hindfoot and are more likely to require anatomical restoration to return to their livelihood, though ironically, literature suggests patients receiving Workers' Compensation often report poorer subjective outcomes regardless of treatment modality.
Absolute and Relative Contraindications
The contraindications to the extensile lateral approach are primarily dictated by the soft tissue envelope and the patient's vascular status. Ignoring these contraindications almost guarantees catastrophic wound complications.
| Contraindication Type | Specific Condition | Clinical Rationale |
|---|---|---|
| Absolute | Severe Peripheral Vascular Disease (PVD) | Inadequate arterial inflow to heal the massive L-shaped surgical flap; extremely high risk of necrosis and amputation. |
| Absolute | Active Local Soft Tissue Infection | Operating through infected tissue will inevitably lead to deep osteomyelitis of the calcaneus. |
| Absolute | Medically Unstable Patient | Polytrauma patients in extremis or those with severe cardiopulmonary disease who cannot tolerate prolonged anesthesia. |
| Relative | Active Tobacco Use (Smoking) | Nicotine causes microvascular vasoconstriction; smokers have a >3x higher rate of wound necrosis and deep infection. Surgery should ideally be delayed or alternative percutaneous methods considered. |
| Relative | Poorly Controlled Diabetes Mellitus | Impaired microcirculation and compromised immune response significantly elevate the risk of wound dehiscence and infection. |
| Relative | Severe Soft Tissue Compromise | Massive fracture blisters, severe edema, or open fractures (depending on Gustilo-Anderson grade) require delay or alternative fixation strategies (e.g., external fixation). |
| Relative | Non-compliant Patient | Inability to adhere to strict non-weight-bearing protocols will result in catastrophic failure of fixation and loss of reduction. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of a successful calcaneal fracture reconstruction. The surgeon must conceptually reduce the fracture and plan the trajectory of every screw before entering the operating theater. This requires a comprehensive radiographic evaluation, meticulous assessment of the soft tissue envelope, and precise patient positioning to facilitate both surgical exposure and intraoperative fluoroscopy.
Advanced Imaging and Pre-Operative Templating
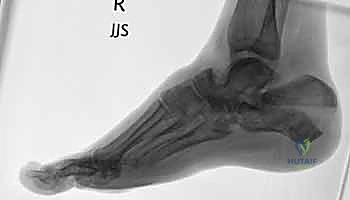
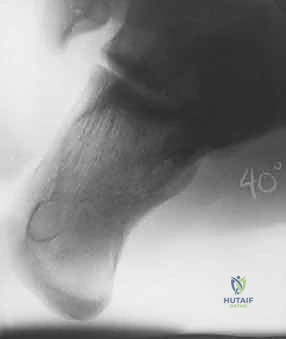
The initial evaluation begins with high-quality orthogonal radiographs of the foot and ankle, including Anteroposterior (AP), Lateral, and Harris Axial views. The lateral view is critical for assessing the loss of calcaneal height, the depression of Böhler's angle, the alteration of the crucial angle of Gissane, and distinguishing between a tongue-type and a joint depression pattern. The Harris axial view provides essential information regarding the varus or valgus alignment of the tuberosity, heel widening, and the integrity of the medial wall.


However, plain radiographs are insufficient for definitive surgical planning. A fine-cut Computed Tomography (CT) scan without contrast is absolutely mandatory for all intra-articular calcaneal fractures. The coronal images are utilized for the Sanders classification, detailing the number and location of fracture lines through the posterior facet. The axial images are invaluable for assessing the calcaneocuboid joint, the anterolateral fragment, and the degree of medial wall comminution. Sagittal reconstructions allow the surgeon to visualize the exact degree of posterior facet impaction and plan the elevation trajectory.

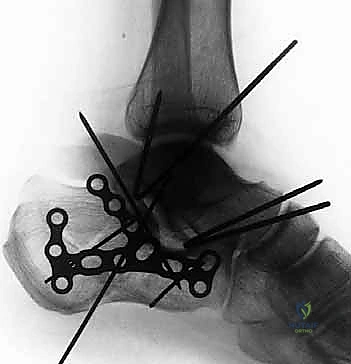
Preoperative templating involves overlaying digital templates of anatomical calcaneal locking plates onto the patient's imaging. The surgeon must determine the appropriate plate size, length, and contour. Furthermore, anticipating the trajectory of the critical "sustentacular screws"—which must pass from the lateral plate, through the reduced posterior facet, and securely into the dense bone of the sustentaculum tali without penetrating the subtalar joint or the medial neurovascular bundle—is a vital component of the templating process.
Soft Tissue Optimization and the Wrinkle Sign
The timing of surgical intervention is dictated entirely by the condition of the soft tissue envelope. Operating through swollen, edematous tissue exponentially increases the risk of wound dehiscence and deep infection. Upon initial presentation, the extremity should be placed in a bulky, well-padded posterior splint, elevated strictly above the level of the heart, and treated with aggressive icing.
The surgeon must monitor the soft tissues meticulously. The resolution of edema is indicated by the appearance of the "wrinkle sign"—the return of normal skin lines and the ability to pinch the skin over the lateral calcaneal wall. This process typically takes anywhere from 10 to 21 days post-injury. The presence of fracture blisters complicates the timing. Clear, fluid-filled blisters represent a superficial epidermal separation and can often be managed by unroofing and applying a non-adherent dressing. Blood-filled blisters, however, indicate a deeper dermal injury and represent a higher risk for necrosis; surgery should ideally be delayed until these have completely epithelialized.
Operating Room Setup and Patient Positioning
The operation is typically performed under general anesthesia, often supplemented with a regional popliteal or sciatic nerve block to provide excellent postoperative analgesia and sympathectomy-induced vasodilation, which aids in soft tissue healing. The patient is positioned in the lateral decubitus position on a radiolucent operating table, with the operative extremity facing upward.
A beanbag or pegboard system is utilized to secure the patient's torso, ensuring that the pelvis is perfectly lateral. The non-operative leg is padded and flexed at the hip and knee, while the operative leg is supported on a ramp or multiple blankets to ensure it remains parallel to the floor. A thigh tourniquet is applied but not inflated until the leg has been exsanguinated.
Crucially, the positioning must allow for unimpeded, multi-planar intraoperative fluoroscopy. The C-arm must be able to easily swing to obtain true lateral, Harris axial, and Broden's views of the subtalar joint. Before prepping and draping, the surgeon must confirm that all necessary fluoroscopic views can be obtained without obstruction from the table pedestal or the contralateral limb. A perfectly positioned patient drastically reduces intraoperative frustration and ensures that radiographic confirmation of the reduction is accurate and reliable.
Step-by-Step Surgical Approach and Fixation Technique
The execution of the extensile lateral approach and the subsequent internal fixation is a highly choreographed sequence. It requires meticulous soft tissue handling, a deep understanding of the three-dimensional fracture morphology, and the ability to sequentially reconstruct the calcaneus from medial to lateral, and anterior to posterior.
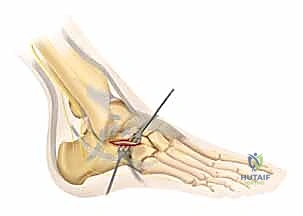
The Extensile Lateral Approach and Full-Thickness Flap
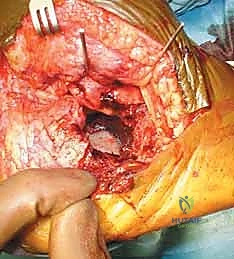
The classic L-shaped extensile lateral incision is designed to provide maximal exposure of the lateral calcaneal wall and subtalar joint while minimizing damage to the delicate vascular supply of the lateral skin flap. The vertical limb of the incision is placed just anterior to the lateral border of the Achilles tendon, extending distally. The horizontal limb begins at the junction of the plantar and lateral skin (the glabrous junction) and extends anteriorly toward the base of the fifth metatarsal. It is imperative that the corner of the 'L' is gently curved, avoiding a sharp 90-degree angle, to minimize the risk of apex necrosis.


The dissection must be carried straight down to the bone in a single, full-thickness layer. The surgeon must avoid creating multiple tissue planes, which devascularizes the flap. Using a scalpel, the incision is taken down through the subcutaneous tissue,
Clinical & Radiographic Imaging Archive