Calcaneus Fractures: Surgical Management & Techniques
Key Takeaway
Intraarticular calcaneus fractures present significant reconstructive challenges. Successful management requires a thorough understanding of hindfoot pathoanatomy, precise CT-based classification, and meticulous soft tissue handling. This guide details the biomechanics of axial load injuries, the Sanders classification system, and step-by-step surgical techniques for open reduction and internal fixation (ORIF) using the extensile lateral approach to restore the Böhler angle and subtalar congruency.
Comprehensive Introduction and Patho-Epidemiology
Intraarticular fractures of the calcaneus represent a formidable challenge in orthopedic traumatology, historically plagued by devastating complications, chronic pain, and profound long-term disability. As the most frequently fractured tarsal bone, accounting for approximately 60% of all tarsal fractures and 2% of all fractures in the human body, the calcaneus plays an indispensable role in hindfoot biomechanics, gait kinematics, and weight-bearing transmission. The management paradigm for these injuries has undergone a paradigm shift over the last three decades. The transition from historical non-operative neglect or primary arthrodesis to sophisticated, anatomically precise open reduction and internal fixation (ORIF) has been driven by the advent of high-resolution computed tomography (CT), a deeper understanding of lateral hindfoot vascularity, and the development of low-profile, anatomically contoured locking plate technology.
Epidemiologically, calcaneus fractures predominantly afflict young, active males in their third to fifth decades of life, representing a significant socioeconomic burden due to prolonged absence from the workforce and the potential for permanent functional impairment. The vast majority of intraarticular calcaneal fractures are the direct consequence of high-energy axial loading mechanisms. Falls from a height—typically greater than six feet—and high-velocity motor vehicle collisions are the most frequently cited etiologies. The magnitude of the force required to shear and compress the dense trabecular bone of the calcaneus dictates that these injuries are rarely isolated. Concomitant injuries are observed in up to 50% of patients, with a classic association existing between calcaneus fractures and compression fractures of the thoracolumbar spine (10% to 15% incidence). Furthermore, bilateral calcaneus fractures occur in approximately 10% of cases, and associated lower extremity trauma, including tibial plateau fractures, pilon fractures, and compartment syndrome of the foot, must be vigilantly excluded during the primary and secondary trauma surveys.


The patho-epidemiology of these fractures is intrinsically linked to the energy absorbed by the soft tissue envelope. The calcaneus is encased in a uniquely specialized, highly septated subcutaneous fat pad on its plantar aspect, designed for shock absorption, and a remarkably thin, vulnerable soft tissue envelope on its lateral aspect. When an axial load is applied, the resultant osseous explosion not only disrupts the articular congruency of the subtalar joint but also inflicts massive barotrauma to the surrounding soft tissues. This localized soft tissue injury leads to profound edema, fracture blistering, and a significantly elevated risk of compartment syndrome of the foot. Consequently, the orthopedic surgeon must view the calcaneus fracture not merely as a bony injury, but as a severe soft tissue injury that happens to contain a fractured bone. The timing of surgical intervention, the choice of surgical approach, and the ultimate functional outcome are all inextricably tethered to the meticulous management of this compromised soft tissue envelope.
Detailed Surgical Anatomy and Biomechanics
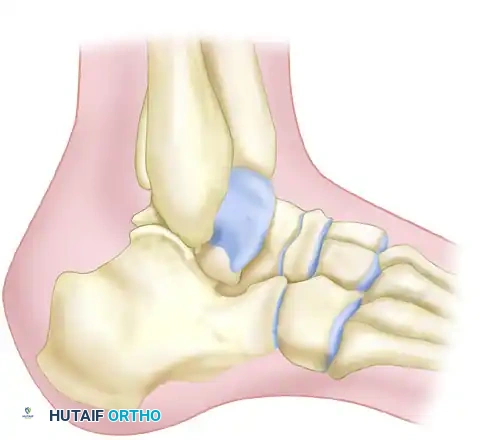
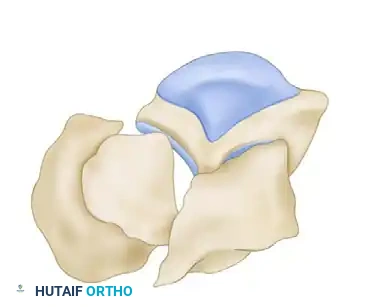
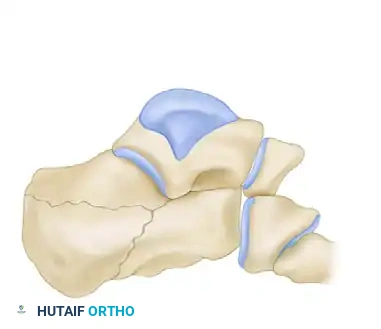
A profound, three-dimensional comprehension of calcaneal anatomy and hindfoot biomechanics is the absolute prerequisite for successful surgical reconstruction. The calcaneus is a complex, irregular bone that articulates with the talus superiorly and the cuboid anteriorly. It features four distinct articular surfaces: the anterior, middle, and posterior facets for the talus, and the distal facet for the cuboid. The posterior facet is the largest and most critical for subtalar joint mechanics, bearing the brunt of the axial load during heel strike. It is convex in the sagittal plane and concave in the coronal plane. The middle facet is supported by the sustentaculum tali, a dense, cortical medial projection that serves as the anatomical cornerstone for reconstruction. The sustentaculum tali is tethered to the talus by the incredibly robust interosseous talocalcaneal ligament, the cervical ligament, and the deltoid ligament complex. Because these ligamentous attachments rarely fail, the sustentaculum tali and its associated articular fragment (the middle facet) remain anatomically aligned with the talus, earning it the moniker of the "constant fragment."
The vascular anatomy of the lateral hindfoot dictates the design of the extensile lateral approach and is critical for minimizing wound complications. The lateral soft tissue envelope is supplied primarily by the lateral calcaneal artery (a terminal branch of the peroneal artery) and the lateral tarsal artery (a branch of the dorsalis pedis artery). These vessels form a delicate anastomotic network. The classic extensile lateral L-shaped incision is specifically designed to respect the angiosome of the lateral calcaneal artery. By creating a full-thickness subperiosteal flap that includes the sural nerve, the peroneal tendons, and the calcaneofibular ligament, the surgeon preserves the microvascular blood supply to the skin edge. Any violation of this full-thickness flap, or the use of self-retaining retractors that crush the skin edges, exponentially increases the risk of ischemic flap necrosis, wound dehiscence, and deep space infection.


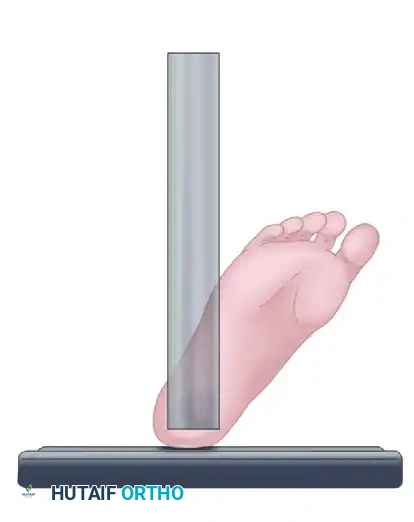
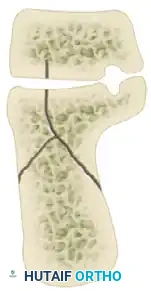
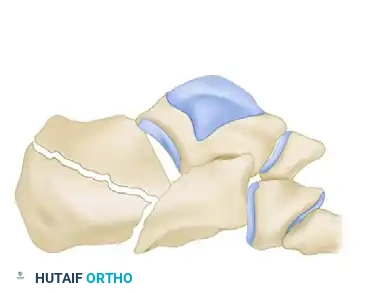
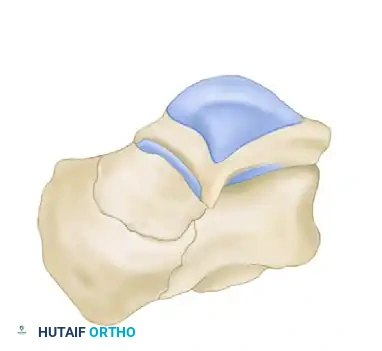
Biomechanically, the fracture pattern is dictated by the position of the foot at the moment of impact and the vector of the axial load. As the force is transmitted through the tibia into the talus, the lateral process of the talus acts as a wedge or an anvil, driving violently into the crucial angle of Gissane. This generates the primary fracture line, a shear force that splits the calcaneus obliquely from posteromedial to anterolateral. This primary line divides the bone into the medial sustentacular fragment (the constant fragment) and the lateral tuberosity fragment. Following the primary shear failure, the continued axial load generates secondary compression fracture lines. The Achilles tendon exerts a massive deforming force on the lateral tuberosity fragment, pulling it superiorly and rotating it into a varus alignment. Simultaneously, the talus drives the posterior facet inferiorly into the cancellous body of the calcaneus, creating a depressed "thalamic" fragment.


This complex sequence of shear and compression forces results in a predictable pathoanatomic deformity: loss of calcaneal height, widening of the heel, varus malalignment of the tuberosity, and profound incongruency of the subtalar joint. The lateral wall of the calcaneus is typically blown out laterally, obliterating the subfibular space. This lateral wall blowout leads to impingement of the peroneal tendons against the distal tip of the fibula, a primary source of chronic lateral hindfoot pain if left unreduced. Furthermore, the medial spike of the tuberosity fragment can be forcefully driven into the medial soft tissues, placing the posterior tibial neurovascular bundle at risk and occasionally resulting in an open fracture on the plantar-medial aspect of the heel.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention in calcaneus fractures is one of the most nuanced and critical determinations in orthopedic traumatology. The goal of surgery is to restore articular congruency, reconstitute calcaneal height and width, correct varus deformity, and decompress the subfibular space. However, the benefits of anatomical restoration must be meticulously weighed against the profound risks of wound complications and deep infection. Patient selection is therefore paramount. The ideal surgical candidate is a physiologically young, active, compliant patient with a displaced intra-articular fracture and a pristine soft tissue envelope. Conversely, the "personality" of the fracture and the host biology may dictate non-operative management even in the face of severe displacement.
Indications for surgical management generally include displaced intra-articular fractures involving the posterior facet (Sanders Types II and III), fractures with significant loss of calcaneal height (flattening of the Böhler angle to less than 15 degrees), widening of the heel with subfibular impingement, and varus malalignment of the tuberosity. Anterior process fractures with greater than 25% involvement of the calcaneocuboid joint or significant displacement also warrant fixation. Tongue-type fractures, particularly those with severe dorsal displacement threatening the posterior skin (the "skin-at-risk" scenario), represent an orthopedic emergency requiring urgent reduction and percutaneous fixation to prevent full-thickness skin necrosis over the Achilles insertion.


Contraindications to open reduction and internal fixation are extensive and must be strictly respected. Absolute contraindications include a non-ambulatory patient, severe peripheral vascular disease (PVD), and an insensate limb (e.g., profound diabetic peripheral neuropathy or a preexisting sciatic/tibial nerve palsy). Operating on an insensate foot carries an unacceptably high risk of postoperative Charcot arthropathy, hardware failure, and ultimate amputation. Active infection or critically compromised soft tissues (unresolved fracture blisters, massive edema without a wrinkle sign) are absolute contraindications to immediate surgery, though delayed intervention may be possible once the soft tissues recover.
Heavy tobacco use is widely considered a strong relative contraindication, and in many major trauma centers, an absolute contraindication to the extensile lateral approach. The vasoconstrictive effects of nicotine and carbon monoxide dramatically increase the risk of ischemic flap necrosis and deep infection (up to a 30-40% complication rate in heavy smokers). Other relative contraindications include advanced age (physiologically older than 65 years), severe medical comorbidities (poorly controlled diabetes mellitus, end-stage renal disease), and highly comminuted Sanders Type IV fractures in patients who are not candidates for primary subtalar arthrodesis. In these challenging scenarios, the surgeon must engage in shared decision-making, clearly articulating that the risks of surgical morbidity may outweigh the potential functional benefits.
| Category | Operative Indications (ORIF / Percutaneous) | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Fracture Pattern | Displaced intra-articular (Sanders II, III) | Non-displaced (Sanders I) | Sanders IV (consider primary fusion) |
| Deformity | Loss of height, varus tuberosity, widened heel | N/A | Severe osteopenia |
| Soft Tissue | "Skin at risk" (Tongue-type) - Urgent | Active local infection, unresolved blisters | Heavily contused soft tissues |
| Host Factors | Young, active, compliant, healthy | Insensate limb, severe PVD, non-ambulatory | Heavy smoking, poorly controlled diabetes, advanced age |
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning for calcaneus fractures requires a multimodal imaging approach to fully define the three-dimensional pathoanatomy. The standard trauma radiographic series is the initial step, comprising a lateral view, an axial (Harris) view, and anteroposterior (AP) and oblique views of the foot. The lateral radiograph is critical for assessing the overall geometry of the calcaneus. The Böhler angle (normally 20 to 40 degrees) is formed by a line drawn from the highest point of the anterior process to the highest point of the posterior facet, intersecting a line drawn from the highest point of the posterior facet to the superior edge of the tuberosity. A depressed Böhler angle indicates loss of calcaneal height and collapse of the posterior facet. The crucial angle of Gissane (normally 120 to 145 degrees) is formed by the downward slope of the posterior facet and the upward slope of the anterior process; widening of this angle indicates impaction of the talus into the calcaneal body.


While plain radiographs provide essential geometric data, high-resolution non-contrast computed tomography (CT) is the definitive gold standard and is absolutely mandatory for surgical planning. CT scans must be reformatted in the axial, sagittal, and semicoronal planes. The semicoronal plane—oriented perpendicular to the normal anatomical position of the posterior facet—is the most critical view. It dictates the Sanders Classification, which is based on the number and location of primary fracture lines traversing the posterior facet at its widest point. The sagittal CT reconstructions are invaluable for defining the exact rotation and depression of the thalamic fragment, while the axial views beautifully delineate the involvement of the calcaneocuboid joint and the integrity of the sustentaculum tali. The surgeon must mentally reconstruct these two-dimensional slices into a three-dimensional surgical strategy, anticipating the location of the constant fragment, the degree of lateral wall blowout, and the trajectory required for sustentacular screw fixation.




Patient positioning in the operating room is a critical component of the procedure, directly impacting the ease of fluoroscopic imaging and surgical access. The patient is typically placed in the lateral decubitus position on a fully radiolucent flat Jackson table or a standard operating table reversed to allow unimpeded C-arm access. A deflatable bean bag is utilized to secure the torso, and an axillary roll is placed. The operative extremity is padded, and a high-thigh tourniquet is applied to ensure a bloodless surgical field, which is essential for identifying the sural nerve and assessing articular reduction. The contralateral leg is flexed at the hip and knee and heavily padded to protect the common peroneal nerve.
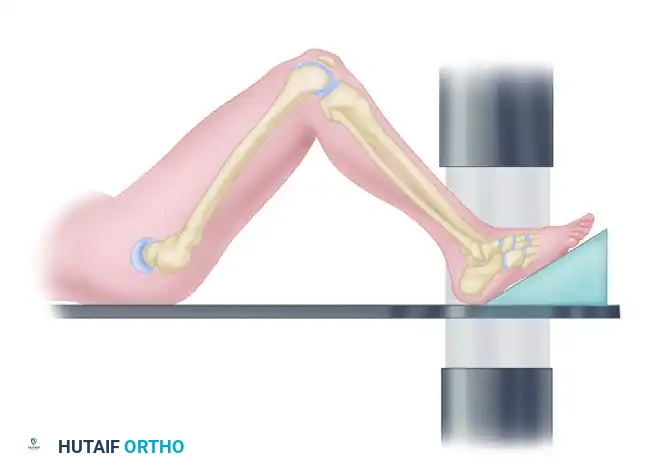
Prior to prepping and draping, the C-arm fluoroscopy unit must be brought into the field to confirm that perfect lateral, axial, and Brodén views can be obtained without moving the patient's leg or breaking the sterile field. The Brodén view is particularly crucial intraoperatively; it is obtained by internally rotating the leg 40 degrees with the ankle in neutral dorsiflexion, and angling the fluoroscopic beam 10, 20, 30, and 40 degrees cephalad. This dynamic sequence provides a tangential view of the posterior facet, allowing the surgeon to confirm absolute anatomic congruency of the articular surface before final fixation is applied.
Step-by-Step Surgical Approach and Fixation Technique
The execution of the extensile lateral approach and subsequent open reduction and internal fixation requires meticulous soft-tissue handling and a highly structured, sequential reduction strategy. Surgery is strictly delayed until the soft tissue envelope permits, indicated by the resolution of massive edema and the appearance of the "wrinkle sign" (typically 10 to 21 days post-injury). Operating through tense, swollen tissue is a guaranteed path to catastrophic wound dehiscence.
The classic extensile lateral L-shaped incision is marked with the horizontal limb positioned exactly at the junction of the glabrous (plantar) and non-glabrous (lateral) skin, extending from the base of the fifth metatarsal posteriorly to the heel cord. The vertical limb ascends just anterior to the lateral border of the Achilles tendon. The incision is made straight down to bone in a single, decisive stroke. To preserve the microvascular supply, a full-thickness subperiosteal flap is elevated off the lateral wall of the calcaneus. This flap must contain the skin, subcutaneous fat, sural nerve, peroneal tendon sheath, and the calcaneofibular ligament. The surgeon uses a periosteal elevator to sharply lift the flap off the lateral wall, working from inferior to superior and posterior to anterior.
A strict "no-touch" technique is mandatory for flap retraction. Self-retaining retractors or forceps must never touch the skin edges. Instead, stout Kirschner wires (1.6mm or 2.0mm) are driven into the lateral malleolus, the talar neck, and the cuboid. The shafts of these K-wires are bent back to gently hold the full-thickness flap superiorly and anteriorly, providing panoramic access to the subtalar joint, the lateral wall, and the calcaneocuboid joint. Once the flap is secured, the hematoma is evacuated, and the lateral wall blowout is identified. The thin cortical shell of the lateral wall is carefully reflected outward, akin to opening the cover of a book, to expose the impacted intracellular cancellous bone and the depressed posterior facet fragments.
The reduction sequence follows a strict, logical progression. First, the primary deformity of the tuberosity fragment must be corrected. A 5.0mm Schanz pin is inserted transversely into the dense bone of the posteroinferior tuberosity. Using this pin as a joystick, the surgeon applies powerful axial traction to restore length, translates the fragment medially to restore width, and pulls plantarly while applying a valgus force to correct the varus and restore calcaneal height. Once the tuberosity is aligned with the medial constant fragment, it is provisionally fixed with heavy K-wires directed from the posteroinferior heel into the sustentaculum tali.


With the overall geometry restored, attention is turned to the articular surface. The depressed fragments of the posterior facet are gently elevated out of the cancellous void using a Freer elevator or a specialized bone tamp. The articular fragments are meticulously pieced together and reduced against the intact articular surface of the talus and the medial sustentacular fragment. This reduction is provisionally held with subchondral K-wires. Intraoperative fluoroscopy, specifically the Brodén views, is utilized to confirm absolute, step-free congruency of the posterior facet. If the calcaneocuboid joint is fractured, it is reduced and pinned at this stage. Finally, the lateral wall is reduced to decompress the subfibular space.
Definitive internal fixation is achieved using a low-profile, anatomically contoured calcaneal locking plate. The plate is slid under the retracted flap and positioned to buttress the lateral wall and support the posterior facet. The most critical screws are the "sustentacular screws." These screws are placed through the plate just inferior to the posterior facet and are directed from lateral to medial, aiming slightly anterior and superior to engage the dense cortical bone of the sustentaculum tali. These screws lock the entire lateral reconstruction to the medial constant fragment. Additional locking and non-locking screws are placed into the anterior process and the posterior tuberosity to create a stable, fixed-angle construct. Bone grafting of the residual cancellous void remains controversial; while historically popular, modern locking plate technology often provides sufficient stability without the need for structural allograft or autograft, reducing operative time and donor site morbidity.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique and stringent patient selection, the surgical management of calcaneus fractures is associated with a formidable complication profile. The most dreaded and frequent complications are related to the vulnerable lateral soft tissue envelope. Wound healing complications—ranging from superficial edge necrosis to catastrophic deep space infection—occur in 10% to 25% of cases following the extensile lateral approach. Superficial dehiscence can often be
Clinical & Radiographic Imaging Archive






