Complex Calcaneal Fracture: Clinical Presentation, Advanced Imaging & Sanders IIIBC Classification Case Study
Key Takeaway
A Sanders Type IIIBC calcaneal fracture is a severe intra-articular heel bone fracture with extensive comminution, often resulting from high-energy axial loads. Diagnosis involves detailed clinical examination for swelling, ecchymosis, and pain, complemented by plain X-rays (evaluating Bohler's/Gissane's angles) and definitive CT scans to classify articular involvement and guide surgical planning.
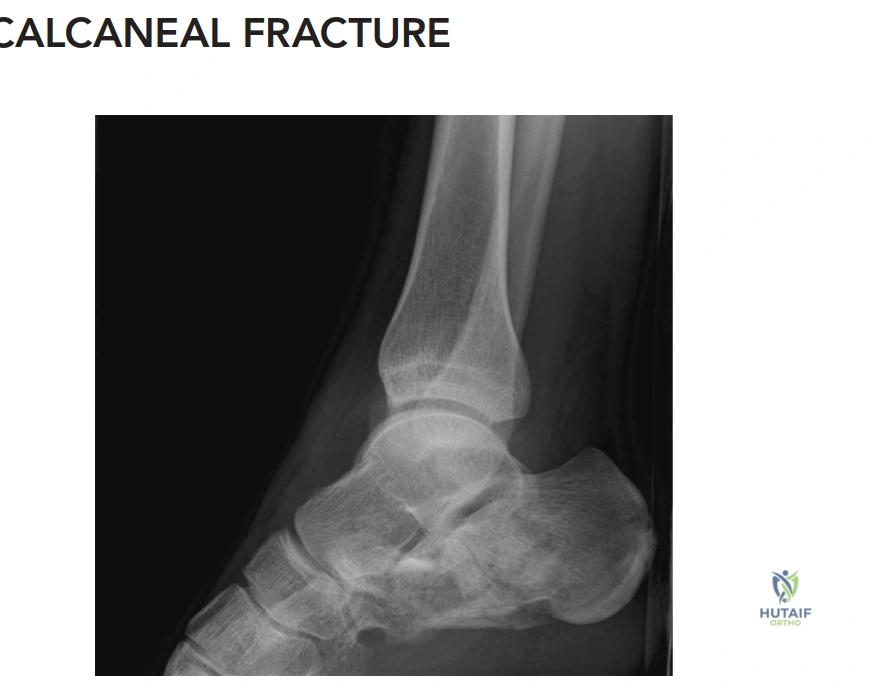
A 38-year-old construction worker presents following a 10-foot fall. He has severe bilateral hindfoot pain and is unable to bear weight. You have reviewed the clinical findings and the following image. What are the key radiographic features present, and how do they influence your initial management?
Candidate: The radiographs show a calcaneal fracture with loss of Bohler’s angle and an increased Gissane’s angle. The CT scan confirms a displaced intra-articular fracture. I would classify this using the Sanders system and plan for ORIF once the soft tissues allow.
Candidates often jump straight to "ORIF" without discussing the soft tissue status or the timing of surgery. Failing to mention the "wrinkle test" or the patient's smoking status (which significantly impacts the risk-benefit ratio of surgery) is a critical omission in a senior-level exam.
A structured answer: 1. Radiographic findings: Describe the loss of Bohler’s angle (<20°) and Gissane’s angle (>120°), indicating sagittal plane collapse. 2. Classification: Identify it as a Sanders Type IIIBC fracture based on coronal CT and note the "tongue-type" variant. 3. Soft Tissue Assessment: Discuss the "wrinkle test" and the necessity of delaying surgery to avoid catastrophic wound breakdown. 4. Risk Stratification: Explicitly address the 15 pack-year smoking history, noting the increased risk of deep infection, and mention that surgery is a nuanced decision to be discussed with the patient regarding potential complications vs. the functional demands of his occupation.
The patient's skin is tense and swollen, and the wrinkle test is negative. How do you manage this in the acute setting, and what specific complications are you looking to prevent?
Candidate: I would keep the foot elevated, apply ice, and monitor the patient. I'd avoid surgery for now because of the risk of wound complications. I am worried about compartment syndrome.
Failing to mention the specific anatomical compartments of the foot (e.g., the calcaneal compartment/quadratus plantae) or missing the importance of monitoring the posterior tibial nerve and FHL function. Simply saying "monitor" is too passive.
The candidate should emphasize: 1. Acute Management: Elevation, immobilization, and strict soft tissue monitoring. 2. Compartment Syndrome: Acknowledge that while rare, it is limb-threatening. Note that the calcaneal compartment (containing the quadratus plantae) is the most relevant. 3. Clinical Thresholds: Maintain a low threshold for intracompartmental pressure monitoring, especially with signs of severe tension or neurological deficit. 4. Patient Counseling: Acknowledge the "wait and see" approach (10-21 days) to reach a "positive wrinkle test," which is the prerequisite for safe extensile surgical intervention.
Assume the soft tissues have settled. You are performing an extensile lateral approach. What are the major dangers to the neurovascular structures, and how do you protect them?
Candidate: I would make a large incision. I'd have to be careful of the sural nerve and the peroneal tendons. I would retract the flap carefully to avoid necrosis.
Vague explanations of "careful retraction." The examiner wants to hear about the specific K-wire retraction technique to avoid point pressure on the flap, which is the leading cause of dehiscence in smokers.
The candidate must articulate: 1. Anatomy: Identify the sural nerve and peroneal tendons within the flap and the lateral calcaneal artery as the blood supply to the flap. 2. Technique: Describe the "no-touch" technique—a single, full-thickness subperiosteal elevation. 3. Retraction: Explain that self-retaining retractors must be avoided. Instead, use 1.6mm K-wires placed into the talus and cuboid, with the flap hooked onto them to distribute tension away from the skin edges. This is the "Gold Standard" for minimizing wound complications in high-risk patients.
