Orthopedic Shoulder 2026 MCQs: Board Review Questions & Answers (Part 3)

Key Takeaway
We review everything you need to understand about Orthopedic Shoulder 2026 MCQs: Board Review Questions & Answers (Part 3). Top-rated Orthopedic Shoulder 2026 MCQs bank. Practice with clinical case questions, orthopedic surgery board review, and evidence-based answers updated for 2026.
Orthopedic Shoulder 2026 MCQs: Board Review Questions & Answers (Part 3)
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Flexion and extension of the elbow occur about an axis of rotation that
Explanation
Question 2
Figure 27 shows the radiograph of a 26-year-old man who sustained a closed head injury and a closed elbow dislocation 6 weeks ago. Examination reveals 65 degrees to 115 degrees of flexion, and intensive physical therapy has resulted in no improvement. A decision regarding the timing of surgical correction of the contracture should be based on
Explanation
Question 3
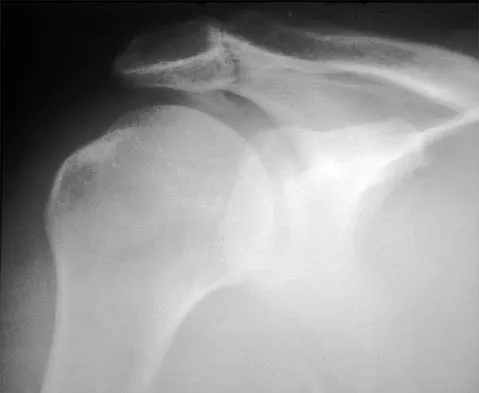
A 70-year-old man who underwent an uncomplicated large rotator cuff repair 6 months ago is now seeking a second opinion regarding persistent pain and weakness in his shoulder. Examination reveals that his incision is well healed and unreactive. The surgical report suggests that the tendons were secured back to bone with sutures through the greater tuberosity. Figure 28 shows a radiograph that was obtained 1 week ago. What is the most likely diagnosis?
Explanation
Question 4
A 29-year-old man who lifts weights states that he injured his left shoulder while performing a bench press 2 days ago. The following morning he noted ecchymosis and swelling in the left chest wall. Examination reveals ecchymosis and tenderness and deformity in the left anterior chest wall and axillary fold that is accentuated with resisted adduction of the arm. Passive range of motion beyond 90 degrees of forward flexion and 45 degrees of external rotation is extremely painful. Glenohumeral stability is difficult to assess because of severe guarding. Figure 29 shows an MRI scan. Management should consist of
Explanation
Question 5
What range of motion parameters are required for a patient with posttraumatic elbow stiffness to accomplish all the normal activities of daily living?
Explanation
Question 6
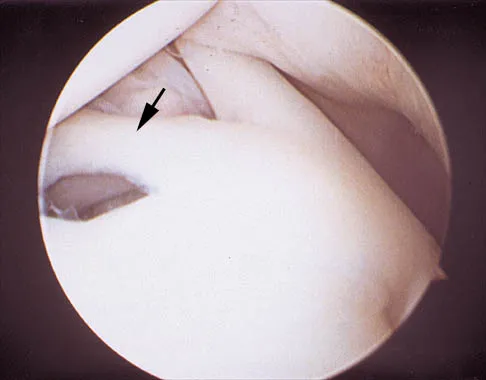
A 24-year-old athlete has a painful right shoulder. Figure 30 shows an intra-articular photograph that was obtained through a posterior portal during arthroscopy; the labrum is indicated by the arrow. Based on these findings, management should consist of
Explanation
Question 7
The use of a screw between the clavicle and the coracoid process to maintain the clavicle and acromioclavicular (AC) joint in a reduced position is a treatment option for AC joint separations. Screw removal is generally recommended after soft-tissue healing. What effect does this rigid coracoclavicular fixation have on shoulder kinematics?
Explanation
Question 8
Figure 31 shows the AP and lateral radiographs of the elbow of a 56-year-old man with chronic polyarticular rheumatoid arthritis. His function continues to be limited by pain with activities of daily living. Examination shows that his total arc of motion is 110 degrees. Nonsurgical management has failed to provide relief. Treatment should now consist of
Explanation
Question 9
A 12-year-old pitcher has had a 2-month history of pain in his right dominant shoulder after throwing. He reports that the pain has gradually progressed to the point where he cannot throw without pain. He also notes that the pain now awakens him at night if he has been active. Anti-inflammatory drugs have failed to provide relief. Examination reveals no abnormalities except for some localized tenderness over the proximal humerus. Figures 32a and 32b show radiographs of both shoulders. What is the most likely diagnosis?
Explanation
Question 10
Which of the following ligaments is the primary static restraint against inferior translation of the arm when the shoulder is in 0 degrees of abduction?
Explanation
Question 11
A 16-year-old high school student undergoes a routine preparticipation physical examination at the beginning of the school year. Examination reveals marked laxity of both shoulders but only mild generalized laxity in other joints. The load and shift test allows for anterior humeral translation to the glenoid rim and posterior humeral translation beyond the glenoid rim. The sulcus sign is present. What is the next most appropriate step in management?
Explanation
Question 12
A 21-year-old professional baseball player has had painful catching and stiffness in his dominant right elbow for the past year. Examination reveals a flexion contracture of 2 degrees and mild pain with full elbow flexion. Radiographs are shown in Figures 33a and 33b. The most effective management should consist of
Explanation
Question 13
A 42-year-old patient has had painful inferior subluxation of the glenohumeral joint following a recent cerebrovascular accident (CVA). Figure 34 shows the AP radiograph of the shoulder. Management should consist of
Explanation
Question 14
A 50-year-old man who underwent an arthroscopic rotator cuff repair 5 days ago now returns for an early postoperative follow-up because of increasing pain in his shoulder. He reports increasing malaise and has a low-grade fever. Examination reveals no redness or swelling, but he has scant serous drainage from the posterior portal. An emergent Gram stain is positive for gram-positive cocci. The next most appropriate step in management should consist of
Explanation
Question 15
A 42-year-old man who is right-hand dominant injured his right shoulder when he fell from a ladder onto his outstretched arm 1 hour ago. Radiographs reveal a two-part greater tuberosity anterior fracture-dislocation. Initial management should consist of
Explanation
Question 16
A 19-year-old man who plays college volleyball undergoes a routine preparticipation physical examination. Figure 35 shows a posterior view of his dominant shoulder. An electromyogram shows that this is a chronic injury, and an MRI scan shows no abnormalities. The best course of action should be
Explanation
Question 17
A 59-year-old construction worker who is right-hand dominant has had right shoulder pain for the past 9 months with no history of injury. Nonsurgical management consisting of two cortisone injections, physical therapy for 3 months, and nonsteroidal anti-inflammatory drugs has failed to provide lasting relief. Examination reveals tenderness over the acromioclavicular (AC) joint and over the subacromial bursa. He has positive Neer and Hawkins impingement signs and AC joint pain with adduction of the shoulder. Radiographs are shown in Figures 36a and 36b. An MRI scan reveals an intact rotator cuff. Management should now consist of
Explanation
Question 18
What three structures are considered the primary constraints necessary for elbow stability?
Explanation
Question 19
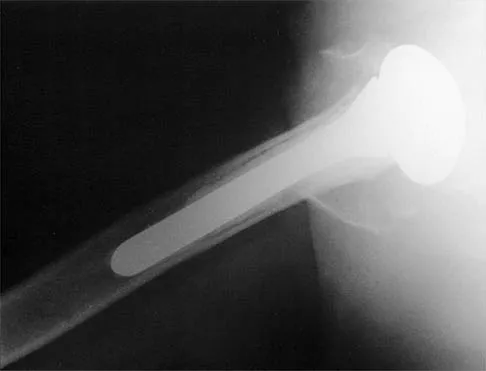
A 68-year-old woman has been progressing slowly after undergoing humeral head replacement for a four-part fracture 3 months ago. She has not regained active elevation, she feels an audible clunk on attempting elevation, and she reports pain and weakness. She used a sling for 2 weeks in the immediate postoperative period. Radiographs are shown in Figure 37a through 37c. Management should consist of
Explanation
Question 20
What is the most important feature in choosing an outcome instrument to assess shoulder disorders?
Explanation
Question 21
Figure 38 shows the radiograph of a 16-year-old wrestler who injured his elbow when he was thrown to the mat by his opponent. To minimize additional trauma to the medial soft tissues, the elbow should be reduced in
Explanation
Question 22
In patients older than age 40 years who sustain a first-time anterior dislocation of the shoulder, prolonged morbidity is most commonly associated with
Explanation
Question 23
Figure 39 shows the AP radiograph of a 62-year-old man with degenerative osteoarthritis secondary to trauma. History reveals that he underwent total elbow arthroplasty 3 years ago. He continues to report instability and constant pain. A complete work-up, including aspiration and cultures, is negative. Treatment should consist of removal of the components and
Explanation
Question 24
A 67-year-old woman undergoes a revision total shoulder arthroplasty for replacement of a loose glenoid component. Examination in the recovery room reveals absent voluntary deltoid and triceps contraction, weakness of wrist and thumb extension, and absent sensation in the palmar aspect of all fingertips and the radial forearm. The next most appropriate step in management should consist of
Explanation
Question 25
Figure 40 shows the radiograph of a 16-year-old wrestler who injured his elbow when he was thrown to the mat by his opponent. Closed reduction is readily accomplished, and the elbow seems stable. Management should now consist of application of a splint for
Explanation
Question 26
During a Latarjet procedure, the coracoid process is transferred to the anterior glenoid. Which nerve is at greatest risk of injury during the coracoid preparation and transfer of the conjoined tendon?
Explanation
Question 27
An 82-year-old woman sustains a displaced 4-part proximal humerus fracture. She has a documented history of severe osteoarthritis and a massive rotator cuff tear prior to the injury. What is the most appropriate surgical treatment?
Explanation
Question 28
In reverse total shoulder arthroplasty (rTSA), which of the following component positioning strategies is most effective in minimizing the risk of scapular notching?
Explanation
Question 29
A 24-year-old rugby player presents with recurrent anterior shoulder instability. A 3D CT scan reveals 27% anterior glenoid bone loss. What is the most appropriate definitive management?
Explanation
Question 30
A 65-year-old man presents with an inability to actively elevate his arm above 60 degrees. Passive elevation is full. An intra-articular injection of local anesthetic completely restores his active elevation to 150 degrees. This clinical finding most likely indicates:
Explanation
Question 31
A 50-year-old man falls on an outstretched arm and experiences acute anterior shoulder pain. Physical examination reveals significantly increased passive external rotation compared to the contralateral side. Which of the following tests is most likely to be positive?
Explanation
Question 32
A 35-year-old man presents to the emergency department after experiencing a grand mal seizure. He holds his right arm internally rotated and is unable to actively or passively externally rotate it. An AP radiograph demonstrates the "lightbulb sign." What is the most appropriate initial management?
Explanation
Question 33
A 28-year-old professional volleyball player complains of vague posterior shoulder pain and weakness. Examination reveals isolated atrophy of the infraspinatus with normal supraspinatus bulk and strength. Where is the most likely site of nerve compression?
Explanation
Question 34
A 55-year-old diabetic woman presents with a 4-month history of severe, diffuse shoulder pain that is progressively worsening, especially at night. Her range of motion is globally decreased but pain is the primary limiting factor. She is currently in which phase of adhesive capsulitis?
Explanation
Question 35
During a diagnostic shoulder arthroscopy on a 22-year-old pitcher, you identify a bucket-handle tear of the superior labrum. However, probing confirms that the biceps anchor remains firmly attached to the superior glenoid tubercle. This corresponds to which classification of SLAP lesion?
Explanation
Question 36
A 30-year-old weightlifter feels a sudden "pop" in his axilla while performing a heavy bench press. He presents with extensive ecchymosis over the anterior axillary fold. He will most likely demonstrate marked weakness in which of the following shoulder motions?
Explanation
Question 37
When evaluating a midshaft clavicle fracture for nonoperative management, which of the following radiographic findings is the most significant risk factor for subsequent nonunion?
Explanation
Question 38
A 25-year-old cyclist falls directly onto his shoulder apex. Radiographs reveal 100% superior displacement of the distal clavicle relative to the acromion. The coracoclavicular distance is increased by 50% compared to the uninjured side. The deltotrapezial fascia remains intact. This represents what type of acromioclavicular (AC) joint injury?
Explanation
Question 39
A 19-year-old football player sustains a posterior sternoclavicular dislocation during a pile-up. He presents with shortness of breath and difficulty swallowing. What is the most immediate life-threatening complication that must be ruled out?
Explanation
Question 40
A 13-year-old elite baseball pitcher presents with worsening right shoulder pain occurring strictly during the cocking phase of throwing. AP radiographs reveal widening and irregularity of the proximal humeral physis. What is the underlying pathophysiology?
Explanation
Question 41
A 32-year-old overhead athlete presents with poorly localized posterior shoulder pain and paresthesias over the lateral deltoid. Angiography demonstrates occlusion of the posterior circumflex humeral artery with the arm in abduction and external rotation. Which nerve is most likely compressed?
Explanation
Question 42
Despite advancements in implant design, what remains the most common complication and cause for late revision surgery following anatomic total shoulder arthroplasty (aTSA)?
Explanation
Question 43
A 26-year-old manual laborer complains of painful crepitus and a loud snapping sensation at the superomedial border of his scapula with movement. Following failure of extensive nonoperative management, surgical intervention is planned. Which structure is most commonly targeted for resection?
Explanation
Question 44
A 21-year-old collegiate tennis player complains of posterior shoulder pain during the late cocking phase of his serve. Arthroscopy reveals undersurface fraying of the posterior supraspinatus and anterior infraspinatus, along with corresponding posterosuperior labral fraying. This triad is characteristic of:
Explanation
Question 45
A 40-year-old man presents with sudden, severe right shoulder pain that lasted unremittingly for 2 weeks. As the pain spontaneously subsided, he noticed profound weakness of the shoulder musculature and pronounced winging of the scapula. EMG demonstrates acute denervation. What is the most likely diagnosis?
Explanation
Question 46
Compared to native shoulder anatomy, a traditional Grammont-style reverse total shoulder arthroplasty alters the biomechanics by doing which of the following?
Explanation
Question 47
A 25-year-old rugby player undergoes an open Latarjet procedure for recurrent anterior shoulder instability with 25% glenoid bone loss. Postoperatively, he presents with inability to flex his elbow and decreased sensation over the lateral forearm. Which nerve was most likely injured during the procedure?
Explanation
Question 48
A 55-year-old manual laborer presents with a massive, irreparable posterosuperior rotator cuff tear. He has intact subscapularis function and no glenohumeral arthritis. He desires to return to heavy labor. Which of the following tendon transfers is most appropriate to restore active external rotation?
Explanation
Question 49
According to the Walch classification, a B2 glenoid is characterized by which of the following?
Explanation
Question 50
A 28-year-old man presents with dull, aching shoulder pain and prominent medial scapular winging that worsens when pushing against a wall. Examination reveals weakness of the serratus anterior. Injury to which nerve is the most likely cause?
Explanation
Question 51
A 32-year-old professional volleyball player presents with poorly localized posterior shoulder pain and paresthesias over the lateral deltoid. An MRI demonstrates isolated atrophy of the teres minor muscle. Which of the following structures is most likely being compressed?
Explanation
Question 52
A 21-year-old collegiate baseball pitcher complains of posterior shoulder pain during the late cocking phase of throwing. Physical exam reveals 15 degrees of internal rotation and 125 degrees of external rotation at 90 degrees of abduction, compared to 60 degrees and 100 degrees respectively on the contralateral side. What is the most appropriate initial management?
Explanation
Question 53
During the surgical approach for a displaced 3-part proximal humerus fracture, preservation of the blood supply to the humeral head is critical. Which artery provides the predominant blood supply to the humeral head?
Explanation
Question 54
A 45-year-old woman presents with acute, severe shoulder pain that awakens her from sleep. Radiographs show a fluffy, ill-defined calcific deposit in the supraspinatus tendon. During which phase of calcific tendinitis does a patient typically experience the most severe pain?
Explanation
Question 55
A 19-year-old male is brought to the emergency department after a motor vehicle accident. He has severe pain over his medial clavicle, shortness of breath, and dysphagia. Radiographs and a CT scan confirm a posterior sternoclavicular dislocation. What is the most appropriate management?
Explanation
Question 56
Which of the following structures is NOT a component of the rotator interval of the shoulder?
Explanation
Question 57
Which of the following is considered an absolute indication for operative fixation of an acute midshaft clavicle fracture?
Explanation
Question 58
A 50-year-old woman with diabetes mellitus presents with worsening shoulder stiffness and pain. Arthroscopy reveals hypervascularity and proliferative synovitis without significant capsular fibrosis. This represents which stage of adhesive capsulitis, and what is the typical duration of this stage?
Explanation
Question 59
A 30-year-old weightlifter feels a "pop" in his anterior axilla while performing a bench press. Examination reveals an ecchymotic swelling and loss of the anterior axillary fold. MRI confirms a complete rupture of the pectoralis major at its humeral insertion. Which of the following is the most appropriate treatment to restore maximum strength?
Explanation
Question 60
A 42-year-old man presents with sudden onset of severe, unrelenting right shoulder pain lasting for two weeks, followed by profound weakness of his deltoid and supraspinatus. There is no history of trauma. MRI of the shoulder is unremarkable. What is the most likely diagnosis?
Explanation
Question 61
A 40-year-old man suffers a first-time seizure and sustains a locked posterior shoulder dislocation. CT scan shows an impaction fracture of the anteromedial humeral head involving 35% of the articular surface. Which of the following is the most appropriate surgical treatment?
Explanation
Question 62
A 24-year-old overhead athlete presents with deep shoulder pain and clicking. MR arthrogram demonstrates detachment of the superior labrum and the origin of the long head of the biceps tendon from the glenoid. What is the standard arthroscopic management for this specific lesion in this patient?
Explanation
Question 63
Which of the following radiographic findings is a widely accepted indication for operative fixation of an extra-articular scapular body/neck fracture?
Explanation
Question 64
A 35-year-old man presents with posterior shoulder pain and weakness in external rotation. Forward elevation strength is normal. Examination reveals atrophy isolated to the infraspinatus fossa. Where is the most likely location of nerve compression?
Explanation
Question 65
A 28-year-old professional volleyball player presents with insidious onset of right shoulder pain and weakness. Clinical examination reveals isolated atrophy of the infraspinatus with normal supraspinatus bulk and strength. MRI demonstrates a paralabral cyst in the spinoglenoid notch. What is the most likely location of the labral tear associated with this condition?
Explanation
Question 66
In reverse total shoulder arthroplasty (RTSA), which of the following glenosphere design modifications or placements is most effective in decreasing the incidence of inferior scapular notching?
Explanation
Question 67
A 22-year-old collegiate rugby player presents with recurrent anterior shoulder instability. A 3D CT scan reveals a 25% anterior glenoid bone loss. What is the most appropriate surgical management to restore stability?
Explanation
Question 68
A 48-year-old recreational tennis player presents with persistent shoulder pain despite 6 months of conservative management. MRI confirms an isolated Type II SLAP tear. What is the most reliable surgical option for this specific patient?
Explanation
Question 69
A 21-year-old collegiate baseball pitcher complains of posterior shoulder pain during the late cocking phase of throwing. Examination shows a 25-degree loss of internal rotation and a 15-degree gain in external rotation compared to the contralateral side. What is the initial treatment of choice?
Explanation
Question 70
A 32-year-old male bodybuilder presents with an acute tearing sensation in his anterior chest and axilla while performing a heavy bench press. Examination reveals an asymmetric chest wall and a palpable defect in the axillary fold. If surgical repair is planned, which anatomical structure represents the most common site of failure in this injury?
Explanation
Question 71
A 65-year-old woman is planning to undergo total shoulder arthroplasty (TSA) for primary osteoarthritis. Preoperative CT imaging reveals a Walch B2 glenoid. What is the recommended strategy to address this specific deformity during primary TSA to prevent early glenoid component loosening?
Explanation
Question 72
A 78-year-old right-hand-dominant woman sustains a 4-part proximal humerus fracture with severe varus collapse and significant comminution of the tuberosities. She lives independently and is medically optimized. What is the most appropriate surgical treatment?
Explanation
Question 73
A 28-year-old male construction worker falls directly onto his right shoulder. Radiographs demonstrate an acromioclavicular (AC) joint injury with the distal clavicle displaced superiorly by 150% of the normal AC joint distance. What is the most appropriate management?
Explanation
Question 74
A 35-year-old man presents with vague posterior shoulder pain and numbness over the lateral aspect of the deltoid. MRI of the shoulder demonstrates isolated atrophy and fatty infiltration of the teres minor muscle. Which of the following structures is most likely compressed?
Explanation
Question 75
A 52-year-old woman with a 10-year history of poorly controlled type 1 diabetes presents with severe, progressive shoulder stiffness and pain for 4 months. She has profound loss of active and passive external rotation. Which of the following best describes the underlying pathophysiology of her condition?
Explanation
Question 76
A 72-year-old woman undergoes a reverse total shoulder arthroplasty (RTSA). At 2-year follow-up, radiographs show inferior scapular notching. Which of the following implant positioning strategies most effectively reduces the risk of this complication?

Explanation
Question 77
A 22-year-old rugby player presents with recurrent anterior shoulder instability. A 3D CT scan reveals 25% anterior glenoid bone loss. What is the most appropriate surgical management?

Explanation
Question 78
A 78-year-old woman sustains a 4-part proximal humerus fracture with head splitting and osteopenia. She lives independently and is a community ambulator. What is the most reliable surgical option to predictably restore forward elevation?
Explanation
Question 79
A 28-year-old elite volleyball player complains of vague posterior shoulder pain and weakness with external rotation. Examination reveals isolated atrophy of the infraspinatus with normal supraspinatus strength. MRI reveals a paralabral cyst. Which nerve is most likely compressed, and at what anatomical location?
Explanation
Question 80
A 32-year-old male bodybuilder felt a pop in his anterior chest while performing a heavy bench press. He has bruising over the anterior axillary fold and weakness in internal rotation and adduction. Which segment of the pectoralis major is most commonly injured in this mechanism?

Explanation
Question 81
A 45-year-old woman presents with shoulder pain and difficulty lifting her arm after a lymph node biopsy in the posterior cervical triangle. On examination, the superior angle of the scapula is displaced laterally, and winging worsens with arm abduction. What is the most likely diagnosis?

Explanation
Question 82
A 60-year-old man with primary glenohumeral osteoarthritis is planned for a total shoulder arthroplasty. A 3D CT scan reveals a Walch B2 glenoid with 20 degrees of retroversion. To prevent early glenoid component loosening, which of the following is the most appropriate management strategy?

Explanation
Question 83
A 40-year-old man presents with acute, excruciating right shoulder pain that started 2 weeks ago following a viral illness. The severe pain has subsided, but he now has profound weakness in forward elevation and external rotation. MRI of the shoulder is unremarkable. What is the most appropriate next step in diagnosis?

Explanation
Question 84
A 25-year-old manual laborer falls directly onto his shoulder. Radiographs show a Rockwood type III acromioclavicular (AC) joint separation. What is the current consensus regarding the initial management of this injury?

Explanation
Question 85
A 65-year-old man presents with an inability to actively elevate his arm above 45 degrees, despite full passive range of motion. MRI reveals a massive, retracted tear of the supraspinatus and infraspinatus with Goutallier stage 4 fatty infiltration. His acromiohumeral distance is 4 mm. What is the most appropriate surgical treatment?

Explanation
Question 86
A 42-year-old man presents with a locked shoulder in internal rotation after a generalized seizure. An axillary lateral radiograph confirms a posterior dislocation with a reverse Hill-Sachs lesion involving 35% of the articular surface. Which of the following is the most appropriate surgical treatment?

Explanation
Question 87
A 72-year-old woman undergoes a reverse total shoulder arthroplasty for cuff tear arthropathy. To minimize the risk of scapular notching, which of the following is the optimal positioning strategy for the glenoid baseplate?
Explanation
Question 88
A 22-year-old rugby player presents with recurrent anterior shoulder instability. CT evaluation reveals 22% anterior glenoid bone loss and an engaging 'off-track' Hill-Sachs lesion. Which of the following is the most appropriate definitive management?
Explanation
Question 89
A 28-year-old man presents with persistent shoulder pain and weakness 4 months after a blunt trauma to his right neck and shoulder region. On examination, forward elevation of the arm against resistance exacerbates the prominence of the medial border of the scapula. Which of the following nerves is most likely injured?
Explanation
Question 90
A 55-year-old man presents with anterior shoulder pain and weakness after attempting to catch a falling heavy object. Physical examination reveals increased passive external rotation compared to the contralateral side, and profound weakness on the belly-press test. MRI confirms an isolated full-thickness tendon tear. The involved tendon normally inserts onto which of the following structures?
Explanation
Question 91
A 68-year-old woman sustains a displaced proximal humerus fracture. According to Hertel's criteria for ischemia, which of the following radiographic findings is the strongest predictor of subsequent avascular necrosis of the humeral head?
Explanation
Question 92
A 45-year-old manual laborer has a massive, irreparable posterosuperior rotator cuff tear. He exhibits severe weakness in external rotation and elevation but has intact subscapularis function. He is considering a latissimus dorsi tendon transfer. Which of the following is considered an absolute contraindication to this procedure?
Explanation
Question 93
A 32-year-old bodybuilder feels a 'pop' and develops severe pain in the anterior axillary fold while performing a heavy bench press. Examination reveals loss of the normal axillary contour. If operative repair is undertaken, the torn tendon should be reattached to which of the following anatomic locations?
Explanation
Question 94
A 40-year-old man presents with a locked, internally rotated shoulder following a generalized seizure. Radiographs confirm a posterior glenohumeral dislocation with an anteromedial humeral head impaction fracture involving 30% of the articular surface. After closed reduction, what is the most appropriate surgical intervention?
Explanation
Question 95
A 35-year-old woman presents with acute, severe, unremitting right shoulder pain of 2 weeks' duration, which started spontaneously. The intense pain has recently subsided, but she has now developed profound weakness in shoulder abduction and external rotation. MRI of the shoulder demonstrates no structural tendon pathology. What is the most likely diagnosis?
Explanation
Question 96
A 50-year-old woman with type 1 diabetes mellitus presents with insidious onset of progressive shoulder stiffness and pain. Passive range of motion is globally restricted, particularly in external rotation with the arm at the side. Thickening and contracture of which of the following structures is most characteristic of this condition?
Explanation
Question 97
A 42-year-old mechanic sustains an acute distal biceps tendon rupture and undergoes repair using a two-incision technique. Compared to a single anterior incision approach, the two-incision technique carries a historically higher risk of which of the following postoperative complications?
Explanation
Question 98
A 26-year-old elite volleyball player complains of vague posterior shoulder pain and selective weakness in external rotation. Forward elevation and internal rotation strength are 5/5. MRI demonstrates an isolated paralabral ganglion cyst at the spinoglenoid notch. Which of the following physical exam findings is most likely present?
Explanation
Question 99
A 29-year-old man requires a glenohumeral arthrodesis due to an irreparable total brachial plexus injury. To optimize postoperative function, allowing his hand to reach his mouth and perineum, what is the generally recommended position for fusing the glenohumeral joint?
Explanation
Question 100
A 24-year-old cyclist falls directly onto his shoulder. Radiographs demonstrate a complete dislocation of the acromioclavicular (AC) joint with the clavicle displaced superiorly by 200% compared to the contralateral side. The deltotrapezial fascia is completely stripped from the distal clavicle. Which Rockwood classification best describes this injury?
Explanation
None
