Orthopedic Shoulder 2026 MCQs: Board Review Questions & Answers (Part 1)

Key Takeaway
Discover the latest medical recommendations for Orthopedic Shoulder 2026 MCQs: Board Review Questions & Answers (Part 1). Top-rated Orthopedic Shoulder 2026 MCQs bank. Practice with clinical case questions, orthopedic surgery board review, and evidence-based answers updated for 2026.
Orthopedic Shoulder 2026 MCQs: Board Review Questions & Answers (Part 1)
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Which of the following statements best describes why the ulnar nerve is most prone to neuropathy at the elbow?
Explanation
Question 2
Figure 1 shows the radiograph of a 71-year-old man who has had increasing pain and weakness in his shoulder for the past 3 years. Nonsurgical management has failed to provide relief. Examination shows 130 degrees of active forward flexion and intact external rotation strength. During surgery, a 1- x 1-cm rotator cuff tear involving the supraspinatus is encountered. Treatment should include
Explanation
Question 3
Which of the following is considered the cause of Milwaukee shoulder, a joint disease similar to rotator cuff arthropathy?
Explanation
Question 4
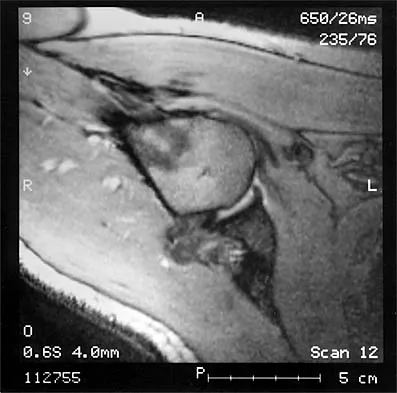
The MRI scan of the shoulder shown in Figure 2 was performed with the arm in abduction and external rotation. The image reveals what condition?
Explanation
Question 5
Figure 3 shows the radiographs of a 32-year-old man who fell 12 feet onto his outstretched arm and sustained a fracture-dislocation of the elbow. Initial management consisted of closed reduction of the dislocation. Surgical treatment should now include repair or reduction and fixation of the
Explanation
Question 6
It is important to avoid which of the following exercises in the immediate postoperative period after humeral head replacement for an acute four-part fracture?
Explanation
Question 7
A 38-year-old man has winging of the ipsilateral scapula after undergoing a transaxillary resection of the first rib 3 weeks ago. What is the most likely cause of this finding?
Explanation
Question 8
A 73-year-old man who underwent repair of the left rotator cuff 6 years ago reports good pain relief but notes residual weakness of the left shoulder, especially with overhead tasks. He denies having pain at night and has minimal discomfort with activities of daily living but is dissatisfied with his shoulder strength. Radiographs show an acromiohumeral interval of 2 mm. Appropriate management should consist of
Explanation
Question 9
A 45-year-old woman has had progressive right shoulder pain for the past 6 months. She notes that the pain disrupts her sleep, she has pain at rest that requires the use of narcotic analgesics, and she has limited use of her left shoulder for most activities of daily living. History reveals the use of corticosteroids for systemic lupus erythematosus. Examination shows diminished range of motion. Radiographs of the right shoulder are shown in Figures 4a and 4b. Treatment should consist of
Explanation
Question 10
The relocation test is most reliable for diagnosing anterior subluxation of the glenohumeral joint when
Explanation
Question 11
A 16-year-old high school pitcher notes acute pain on the medial side of his elbow during a pitch. Examination that day reveals medial elbow tenderness, pain with valgus stress, mild swelling, and loss of extension. Plain radiographs show closed physes and no fracture. Which of the following diagnostic studies will best reveal his injury?
Explanation
Question 12
Figures 5a and 5b show the radiographs of a 45-year-old patient. What is the most likely diagnosis?
Explanation
Question 13
A 14-year-old boy sustains a twisting injury to his right shoulder and recalls feeling a snap during a wrestling match. Examination shows hesitancy to raise the arm away from the side, diffuse tenderness and swelling of the upper arm, and no evidence of neurovascular compromise. Figures 6a and 6b show an AP radiograph and MRI scan. What is the most likely diagnosis?
Explanation
Question 14
Figure 7 shows the radiograph of an otherwise healthy 65-year-old man who injured his right dominant shoulder while skiing 18 months ago. He did not seek treatment at the time of the injury. He now reports intermittent soreness when playing golf but has no other limitations. Examination reveals full range of motion and no tenderness, but he has slight pain with a crossed arm adduction stress test. He is neurologically intact. Initial management should consist of
Explanation
Question 15
Figure 8 shows the AP radiograph of a 33-year-old woman who sustained a midshaft clavicle fracture from a motorcycle accident 15 months ago. She continues to have significant pain with activities of daily living. Management should consist of
Explanation
Question 16
A 62-year-old patient with rheumatoid arthritis has had pain and instability of the elbow following total elbow replacement 2 years ago. A complete work-up, including aspiration and cultures, is negative. Figures 9a and 9b show the AP and lateral radiographs. Treatment should consist of
Explanation
Question 17
A 21-year-old football player reports increasing pain and a deformity involving his chest after colliding with another player during a scrimmage. Imaging studies confirm an anterior sternoclavicular dislocation. Management should consist of
Explanation
Question 18
During total shoulder replacement for rheumatoid arthritis, fracture of the humeral shaft occurs. An intraoperative radiograph shows a displaced short oblique fracture at the tip of the prosthesis. At this point, the surgeon should
Explanation
Question 19
What is the most common contracture deformity of the spastic shoulder secondary to a cerebrovascular accident?
Explanation
Question 20
A 21-year-old collegiate pitcher has had pain in his dominant shoulder for the past 3 months despite management consisting of rest, rehabilitation, and an analysis of throwing mechanics. An arthroscopic photograph from the posterior portal is shown in Figure 10. The biceps anchor to the bone was not detached to probing. Treatment of the lesion to the left of the cannula should consist of arthroscopic
Explanation
Question 21
After humeral head replacement for four-part fractures, what is the most commonly reported difficulty?
Explanation
Question 22
Figures 11a and 11b show the AP and lateral radiographs of a 32-year-old patient on hemodialysis who has increasing elbow pain and a visibly growing mass over the extensor surface. Figure 11c shows the photomicrograph of the biopsy specimen. What is the most likely diagnosis?
Explanation
Question 23
A 52-year-old man who was a former high school pitcher now reports loss of elbow flexion and extension with pain at the extremes of motion. Nonsurgical management has failed to provide relief. Examination reveals movement from 50 degrees to 110 degrees and is painful only at the limits of motion. A radiograph is shown in Figure 12. Treatment should consist of
Explanation
Question 24
A 79-year-old woman with polyarticular rheumatoid arthritis has had progressively increasing right shoulder pain for the past year, and nonsurgical management has failed to provide relief. Her neurologic examination is entirely normal, but she is unable to elevate her arm against gravity. An AP radiograph is shown in Figure 13. Treatment should consist of
Explanation
Question 25
A 22-year-old woman has had progressive upper extremity weakness for the past several years. History reveals no pain in her neck or shoulders. Examination reveals scapular winging of both shoulders and weakness in external rotation. She can abduct to only 120 degrees bilaterally, and there is mild supraspinatus weakness. She is otherwise neurologically intact with normal sensation and reflexes; however, she has difficulty whistling. A clinical photograph is shown in Figure 14. What is the most likely diagnosis?
Explanation
Question 26
A 65-year-old man with primary glenohumeral osteoarthritis is indicated for an anatomic total shoulder arthroplasty. Preoperative CT imaging reveals a biconcave glenoid with 20 degrees of retroversion and asymmetric posterior wear. According to the Walch classification, which type of glenoid morphology is present?
Explanation
Question 27
A 22-year-old rugby player undergoes an open Latarjet procedure for recurrent anterior shoulder instability with 25% glenoid bone loss. Postoperatively, he presents with profound weakness in elbow flexion and decreased sensation over the lateral forearm. Which nerve is most likely injured?
Explanation
Question 28
A 70-year-old man presents with mild, progressive shoulder pain and stiffness 14 months after a reverse total shoulder arthroplasty. His serum ESR and CRP are within normal limits. Joint aspiration is negative for acute inflammation, but tissue cultures taken during revision surgery grow a slow-growing, anaerobic gram-positive bacillus on day 10. What is the most likely causative organism?
Explanation
Question 29
A 68-year-old woman sustains a displaced proximal humerus fracture after a fall. According to the Hertel criteria, which of the following radiographic findings is the most significant predictor of humeral head ischemia and subsequent avascular necrosis?

Explanation
Question 30
A 25-year-old male presents with inability to elevate his right arm past 90 degrees and prominent medial winging of his right scapula, which is exacerbated when he pushes against a wall. He recalls a severe viral illness 3 weeks prior. Which nerve is most likely affected?
Explanation
Question 31
A 45-year-old manual laborer presents with an irreparable, massive posterosuperior rotator cuff tear. He has an intact subscapularis but profoundly weak external rotation and a positive hornblower's sign. What is the most appropriate tendon transfer to restore external rotation?
Explanation
Question 32
Which of the following best describes the biomechanical alteration achieved by a Grammont-style reverse total shoulder arthroplasty compared to the native shoulder joint?
Explanation
Question 33
During the 'freezing' phase of adhesive capsulitis, which of the following is the predominant histologic finding in the glenohumeral joint capsule?
Explanation
Question 34
A 28-year-old cyclist falls directly onto his shoulder. Radiographs demonstrate an acromioclavicular (AC) joint injury with 50% superior displacement of the clavicle relative to the acromion. How is this injury classified according to Rockwood?
Explanation
Question 35
A 40-year-old female presents to the ER with excruciating, acute-onset right shoulder pain with no history of trauma. Radiographs reveal a fluffy, ill-defined calcific deposit in the supraspinatus tendon. The patient's intense pain is most characteristic of which phase of calcific tendinitis?
Explanation
Question 36
A 32-year-old male weightlifter felt a 'pop' in his anterior axilla while performing a heavy bench press. Examination reveals an asymmetric axillary fold and weakness in internal rotation. MRI confirms a pectoralis major rupture. Which portion of the muscle is most commonly torn in this scenario?
Explanation
Question 37
A 21-year-old collegiate baseball pitcher reports posterior shoulder pain during the late cocking phase of throwing. Exam reveals a Glenohumeral Internal Rotation Deficit (GIRD). Which of the following is the primary pathologic mechanism of internal impingement in this athlete?
Explanation
Question 38
A 35-year-old volleyball player presents with painless weakness in external rotation of the dominant shoulder. Examination shows isolated atrophy of the infraspinatus fossa with normal supraspinatus bulk. A paralabral cyst compressing a nerve is suspected. What is the most likely location of the cyst?
Explanation
Question 39
A 42-year-old man presents with a locked shoulder in internal rotation following a generalized seizure. An axillary lateral radiograph reveals a posterior dislocation with a reverse Hill-Sachs lesion involving 35% of the humeral head articular surface. What is the most appropriate surgical management?
Explanation
Question 40
A 13-year-old Little League pitcher presents with gradually worsening lateral shoulder pain. Radiographs demonstrate widening and irregularity of the proximal humeral physis. What is the most appropriate initial management?
Explanation
Question 41
A 50-year-old active construction worker is undergoing surgery for a symptomatic SLAP II tear and degenerative long head of the biceps tendon. He wishes to avoid any cosmetic asymmetry of his arm. Which procedure carries the highest risk of postoperative 'Popeye' deformity?
Explanation
Question 42
A 75-year-old woman presents with severe shoulder pain and inability to actively elevate her arm past 40 degrees (pseudoparalysis). Radiographs reveal severe glenohumeral osteoarthritis, superior migration of the humeral head (Hamada Grade 3), and acetabularization of the coracoacromial arch. What is the gold standard surgical treatment?
Explanation
Question 43
A 21-year-old military recruit has a history of multiple recurrent anterior shoulder dislocations. Preoperative CT imaging shows 26% anterior glenoid bone loss. Which surgical procedure is most indicated to prevent further instability?
Explanation
Question 44
An 18-year-old football player presents to the trauma bay after landing forcefully on his lateral shoulder. He complains of severe chest pain, dyspnea, and dysphagia. On exam, the medial clavicle is not palpable anteriorly. What is the most appropriate next step in management?
Explanation
Question 45
A 45-year-old man develops severe, spontaneous right shoulder pain that lasts continuously for 2 weeks. As the pain finally begins to subside, he notices profound, painless weakness in his shoulder, specifically unable to abduct or externally rotate the arm. Examination reveals deltoid and periscapular atrophy. What is the most likely diagnosis?
Explanation
Question 46
What is the primary biomechanical advantage of the baseplate and glenosphere design in a standard reverse total shoulder arthroplasty?
Explanation
Question 47
A 68-year-old man presents with severe shoulder pain and restricted motion due to primary osteoarthritis. Axial CT imaging reveals a biconcave glenoid with 22 degrees of retroversion and asymmetric posterior wear. The humeral head is subluxated posteriorly. According to the Walch classification, which type of glenoid morphology does this represent?
Explanation
Question 48
Recent quantitative anatomical studies indicate that the primary blood supply to the humeral head, which is highly relevant in determining the risk of avascular necrosis following a 4-part proximal humerus fracture, is derived from which of the following vessels?
Explanation
Question 49
During a Latarjet procedure for anterior shoulder instability, the coracoid process is transferred to the anterior glenoid neck. The dynamic "sling effect" that stabilizes the shoulder during abduction and external rotation is provided primarily by which anatomical structure?
Explanation
Question 50
A 24-year-old elite volleyball attacker complains of persistent posterior shoulder pain. Physical examination reveals isolated weakness in external rotation with intact forward elevation strength. At which anatomical location is the involved nerve most likely being compressed?
Explanation
Question 51
A 32-year-old competitive weightlifter feels a sudden "pop" in his anterior shoulder while performing a heavy bench press. Examination demonstrates an asymmetric chest wall with loss of the anterior axillary fold. If surgical repair is performed to restore function, to which anatomic footprint should the torn tendon be reattached?
Explanation
Question 52
A 28-year-old man sustains a blunt trauma to the posterior triangle of the neck. He presents with an inability to comfortably abduct his arm above 90 degrees and a drooping shoulder. Examination shows prominent lateral scapular winging. Injury to which of the following nerves is the most likely cause?
Explanation
Question 53
A 45-year-old man presents with his shoulder locked in internal rotation following a generalized seizure. Radiographs confirm a posterior shoulder dislocation. A CT scan reveals a reverse Hill-Sachs lesion involving 35% of the anterior articular surface. What is the most appropriate surgical management?
Explanation
Question 54
A 26-year-old cyclist sustains an injury to his shoulder. Radiographs demonstrate an acromioclavicular (AC) joint separation where the distal clavicle is displaced superiorly by 150% relative to the acromion. The coracoclavicular distance is more than doubled compared to the contralateral side. What is the Rockwood classification of this injury?
Explanation
Question 55
During the physical examination of a patient with insidious onset of shoulder pain, which of the following findings is the most reliable clinical indicator to differentiate early "freezing" stage adhesive capsulitis from rotator cuff impingement syndrome?
Explanation
Question 56
A 38-year-old overhead athlete presents with vague posterior shoulder pain and paresthesias over the lateral deltoid. MRI of the shoulder reveals isolated fatty atrophy of the teres minor muscle. Which vascular structure passes through the exact same anatomical space as the compromised nerve?
Explanation
Question 57
In the surgical technique of reverse total shoulder arthroplasty, which of the following glenoid baseplate configurations has been most strongly associated with a decreased incidence of inferior scapular notching?
Explanation
Question 58
A 70-year-old female presents with severe shoulder pain and pseudoparalysis. Radiographs show superior migration of the humeral head and glenohumeral osteoarthritis. She undergoes a reverse total shoulder arthroplasty (RTSA). Postoperatively, she has persistent external rotation weakness and a positive hornblower's sign. Which of the following preoperative factors most likely predicts this specific postoperative deficit?
Explanation
Question 59
A 75-year-old female sustains a comminuted 4-part proximal humerus fracture. Due to her age, poor bone quality, and comminution, she is treated with a reverse total shoulder arthroplasty (RTSA) rather than open reduction and internal fixation. Compared to hemiarthroplasty for this indication, RTSA is associated with:
Explanation
Question 60
A 22-year-old male rugby player presents with recurrent anterior shoulder instability. An MRI shows an anterior glenoid bone loss of 18% and a large Hill-Sachs lesion. Based on the glenoid track concept, if the Hill-Sachs lesion extends medial to the glenoid track, it is considered "off-track." Which of the following is the most appropriate surgical management for an off-track lesion in this high-demand athlete?
Explanation
Question 61
A 28-year-old male weightlifter feels a "pop" in his anterior axilla while bench pressing. Examination reveals ecchymosis, a loss of the anterior axillary fold, and weakness in internal rotation. MRI confirms an acute avulsion of the pectoralis major tendon from its humeral insertion. Which of the following best describes the anatomical arrangement of the native pectoralis major tendon insertion?
Explanation
Question 62
A 68-year-old man presents with insidious onset of shoulder stiffness and mild pain two years after an anatomic total shoulder arthroplasty. Inflammatory markers (ESR, CRP) are normal. Aspiration yields no growth at 3 days. What is the most appropriate next step in diagnosing a potential Cutibacterium acnes infection?
Explanation
Question 63
A 35-year-old elite volleyball player presents with vague posterior shoulder pain and weakness with external rotation. Examination reveals isolated atrophy of the infraspinatus with preserved supraspinatus bulk. Where is the most likely location of nerve compression?
Explanation
Question 64
A 55-year-old manual laborer presents with an irreparable posterosuperior rotator cuff tear. He has significant external rotation weakness and a positive hornblower's sign, but intact forward elevation (pseudoparesis of external rotation). The subscapularis is intact. Which of the following is the most appropriate tendon transfer for this patient?
Explanation
Question 65
A 25-year-old cyclist falls directly onto his shoulder. Clinical exam shows severe prominence of the distal clavicle. Radiographs reveal a Type V acromioclavicular (AC) joint injury with >100% superior displacement. Surgical reconstruction of the coracoclavicular (CC) ligaments is planned. What are the names and typical medial-to-lateral orientation of the native CC ligaments?
Explanation
Question 66
A 52-year-old female with type 1 diabetes presents with progressive shoulder stiffness and pain over 5 months. She has lost significant active and passive range of motion, particularly in external rotation. She is diagnosed with adhesive capsulitis in the "freezing" phase. What is the characteristic histologic finding in the joint capsule of this condition?
Explanation
Question 67
A 40-year-old male presents with acute, severe, unremitting right shoulder pain lasting for 3 weeks, which has recently begun to subside. However, he now notices profound weakness in lifting his arm. Exam shows atrophy of the deltoid and supraspinatus. MRI of the shoulder is unremarkable. EMG shows denervation in the axillary and suprascapular nerve distributions. What is the most likely diagnosis?
Explanation
Question 68
A 30-year-old man sustains a midshaft clavicle fracture with 100% displacement and 2.5 cm of shortening. He undergoes open reduction and internal fixation with a superior plate. Which of the following is the most common complication associated with this specific surgical approach?
Explanation
Question 69
A 45-year-old man falls onto his outstretched hand and presents with anterior shoulder pain. He has increased passive external rotation compared to the contralateral side. The surgeon suspects an acute subscapularis tendon rupture. Which of the following physical examination tests is considered the most sensitive for detecting a partial tear of the upper subscapularis?
Explanation
Question 70
A 19-year-old rugby player sustains a lateral compression injury to his left shoulder. He presents with severe chest pain, shortness of breath, and dysphagia. Examination shows a depression at the left sternoclavicular (SC) joint. Which of the following imaging modalities is the gold standard for diagnosing and assessing the direction of this dislocation?
Explanation
Question 71
A 40-year-old male is involved in a high-speed motorcycle accident and sustains an intra-articular glenoid fracture. Operative intervention is typically indicated for an intra-articular step-off greater than:
Explanation
Question 72
A 48-year-old female presents with sudden, agonizing right shoulder pain over the past 24 hours. She has no history of trauma. Radiographs reveal a large, fluffy, amorphous calcific deposit in the supraspinatus tendon. She is in the resorptive phase of calcific tendinitis. Which of the following biologic environments is responsible for the intense pain during this phase?
Explanation
Question 73
A 72-year-old woman undergoes a reverse total shoulder arthroplasty. At her 2-year follow-up, radiographs show grade 2 scapular notching. Which of the following implant configurations or surgical techniques is most closely associated with a decreased incidence of scapular notching?
Explanation
Question 74
A 24-year-old rugby player presents with recurrent anterior shoulder instability. CT scan reveals 25% anterior glenoid bone loss and an engaging Hill-Sachs lesion. Which of the following procedures is most appropriate?
Explanation
Question 75
A 28-year-old volleyball player presents with insidious onset of posterior shoulder pain and isolated weakness in external rotation. An MRI is obtained, demonstrating a paralabral cyst.
Based on the clinical presentation, where is the cyst most likely located and what labral pathology is associated with it?

Explanation
Question 76
A 65-year-old woman sustains a displaced 3-part proximal humerus fracture. According to Hertel's criteria, which of the following radiographic findings is the strongest predictor for the development of humeral head avascular necrosis?
Explanation
Question 77
A 32-year-old male weightlifter feels a pop in his anterior axilla while performing a heavy bench press. Examination reveals loss of the anterior axillary fold and weakness in internal rotation. Surgical repair is planned. Where does the sternocostal head of the pectoralis major insert in relation to the clavicular head?
Explanation
Question 78
A 21-year-old collegiate pitcher complains of vague posterior shoulder pain. Physical examination shows a 25-degree loss of internal rotation and a 15-degree gain of external rotation compared to the contralateral side. Total arc of motion is decreased by 10 degrees. What is the most appropriate initial management?
Explanation
Question 79
A 45-year-old woman presents with right shoulder weakness following a lymph node biopsy in the posterior triangle of the neck. On examination, the affected scapula is laterally translated and there is a droop of the shoulder. She has difficulty abducting her arm past 90 degrees. Which nerve is injured?
Explanation
Question 80
A 27-year-old cyclist falls directly onto his shoulder. Radiographs demonstrate a displaced acromioclavicular joint injury with 150% superior displacement of the clavicle relative to the acromion. What is the classification of this injury and the standard recommended treatment?
Explanation
Question 81
Which of the following cell types and cytokines are most directly responsible for the capsular fibrosis seen in the proliferative stage of adhesive capsulitis?
Explanation
Question 82
A 55-year-old construction worker presents with insidious onset anterior shoulder pain, positive O'Brien's test, and MRI demonstrating a Type II SLAP tear. There is no significant rotator cuff tearing. What is the most reliable surgical intervention for this patient if conservative management fails?
Explanation
Question 83
A 19-year-old male sustains a severe blow to the medial clavicle during a football game. He presents to the ED with a posterior sternoclavicular dislocation, dyspnea, and dysphagia.
A closed reduction is attempted in the OR. If closed reduction fails, which specialist is most critical to have available during the open reduction?

Explanation
Question 84
A 23-year-old professional baseball pitcher presents with pain in the late cocking phase of throwing. MRI arthrogram reveals a partial articular-sided tear of the supraspinatus and fraying of the posterior superior labrum. What is the underlying pathophysiologic mechanism of this injury?
Explanation
Question 85
A 62-year-old woman with severe rheumatoid arthritis is undergoing total shoulder arthroplasty. Preoperative radiographs and CT show central glenoid wear with medialization of the joint line. The rotator cuff is intact. Which of the following components of the surgical technique is most important to optimize outcomes and component longevity?
Explanation
Question 86
A 70-year-old man undergoes open reduction and internal fixation of a 3-part proximal humerus fracture with a locking plate. Postoperatively, he has profound weakness in shoulder abduction but intact external rotation and normal distal pulses. Radiographs show anatomic reduction.
What is the most likely cause of his deficit?

Explanation
Question 87
A 38-year-old laborer presents with an irreparable subscapularis tendon tear after a massive anterior shoulder injury. He has persistent pain and weakness in internal rotation. To restore internal rotation strength and dynamic anterior stability, a pectoralis major transfer is planned. To optimize the vector of pull, the transfer is typically routed:
Explanation
Question 88
Figure 15 shows the radiograph of a 72-year-old woman with an acute 4-part proximal humerus fracture and significant osteoporosis. She has a history of pseudoparalysis prior to the injury. Which of the following is the most appropriate definitive management?
Explanation
Question 89
A 22-year-old collegiate baseball pitcher presents with posterior shoulder pain during the late cocking phase of throwing. MRI arthrogram reveals a peel-back lesion of the superior labrum. Which physical exam finding is most closely associated with this specific pathology?
Explanation
Question 90
Figure 9 shows the AP radiograph of a 74-year-old male with chronic right shoulder pain, pseudoparalysis, and limited active forward elevation to 45 degrees. The radiograph reveals superior migration of the humeral head and acetabularization of the acromion. What is the most appropriate surgical intervention?
Explanation
Question 91
A 26-year-old male sustains an acute, traumatic anterior shoulder dislocation. After successful closed reduction in the emergency department, he notes persistent numbness over the lateral aspect of his shoulder. Which muscle's function is most likely to be impaired?
Explanation
Question 92
A 35-year-old female presents with aching shoulder pain and fatigue when working overhead. Physical examination demonstrates medial winging of the scapula that is accentuated when she pushes against a wall. Which nerve and corresponding muscle are primarily affected?
Explanation
Question 93
A 28-year-old cyclist falls directly onto his shoulder point. Clinical exam shows a highly prominent clavicle. Radiographs reveal 150% superior displacement of the distal clavicle relative to the acromion. Which type of acromioclavicular (AC) joint separation has occurred and what is the standard primary recommendation?
Explanation
Question 94
A 30-year-old male volleyball player presents with isolated weakness in external rotation of his dominant shoulder. Forward elevation and internal rotation strength are normal. MRI reveals a paralabral cyst. At what anatomical location is this cyst most likely compressing the affected nerve?
Explanation
Question 95
A 19-year-old male is brought to the trauma bay after a rugby tackle. He complains of severe pain over the medial clavicle, dysphagia, and a sensation of choking. Which of the following is the most appropriate immediate diagnostic imaging step to guide management?
Explanation
Question 96
Latissimus dorsi tendon transfer is occasionally considered for patients with massive, irreparable posterosuperior rotator cuff tears. Which of the following is generally considered an absolute contraindication for this procedure?
Explanation
Question 97
Figure 51 demonstrates a physical exam finding in a 55-year-old male laborer complaining of acute, sharp anterior shoulder pain and bruising after lifting heavy equipment. A noticeable 'Popeye' deformity is present. He is highly active and reports severe persistent cramping in the arm. What is the most appropriate definitive management?
Explanation
Question 98
A 52-year-old female presents with progressive, severe shoulder stiffness and diffuse pain over the past 4 months. Examination shows significant loss of both active and passive range of motion, particularly external rotation. Which of the following systemic conditions is most strongly associated with the development of this pathology?
Explanation
Question 99
Figure 10 shows the axillary radiograph of a 68-year-old male 7 years post-anatomic total shoulder arthroplasty, who presents with increasing pain. The radiograph demonstrates radiolucent lines >2 mm around the entirely of the glenoid component. Which underlying factor is most predictive of early glenoid component loosening?
Explanation
Question 100
A 21-year-old collegiate linebacker undergoes arthroscopic stabilization for recurrent anterior shoulder instability. During diagnostic arthroscopy, the surgeon notes an avulsion of the anteroinferior capsulolabral complex from the glenoid rim. What is the classic eponym for this lesion?
Explanation
None
