Surgical Management of Peroneal Tendon Subluxation: Retinaculum Repair and Fibular Groove Deepening
Key Takeaway
Recurrent peroneal tendon subluxation often requires surgical intervention to restore the superior peroneal retinaculum (SPR) and deepen the fibular retromalleolar groove. This comprehensive surgical guide details the anatomical repair of the SPR and the Zoellner and Clancy osteoperiosteal flap technique for groove deepening. Emphasizing precise tissue handling, biomechanical restoration, and structured postoperative rehabilitation, these procedures ensure optimal tendon stability and a safe return to high-demand athletic activities.
Comprehensive Introduction and Patho-Epidemiology
Historical Context and Evolution of Management
The recognition and surgical management of peroneal tendon subluxation and dislocation have evolved significantly since the initial descriptions in the late 19th and early 20th centuries. Historically, these injuries were frequently misdiagnosed as simple lateral ankle sprains, leading to chronic pain, persistent instability, and eventual tendinopathic degeneration. Early surgical interventions primarily focused on non-anatomical soft tissue slings or aggressive bone block procedures, which often resulted in severe peritendinous adhesions, restricted subtalar kinematics, and high failure rates. The paradigm shifted dramatically with the seminal work of Eckert and Davis in 1976, who provided the foundational anatomical classification of superior peroneal retinaculum (SPR) avulsions. Subsequently, Zoellner and Clancy introduced the vascularized osteoperiosteal flap technique for fibular groove deepening, fundamentally altering the operative approach by respecting the anatomical gliding surface of the tendons while restoring osseous stability. Today, the gold standard of care mandates a highly individualized, pathoanatomy-driven approach combining retinacular reconstruction with osseous morphological correction when indicated.
Epidemiology and Patient Demographics
Peroneal tendon instability is predominantly observed in the young, active, and athletic population, though it can occur across a broad demographic spectrum. The true incidence remains underreported due to the high rate of initial misdiagnosis in emergency departments and primary care settings. Epidemiological data indicate a strong predilection for sports involving sudden, explosive changes in direction, forced dorsiflexion, and rapid inversion-to-eversion transitions. Consequently, alpine skiers, basketball players, soccer athletes, and gymnasts represent the highest-risk cohorts. In alpine skiing, the mechanism frequently involves the tip of the ski catching the snow, forcing the ankle into violent dorsiflexion while the peroneal musculature is maximally contracted. While acute dislocations are relatively rare, accounting for approximately 0.3% to 0.5% of all acute ankle injuries, chronic recurrent subluxation is a frequently encountered pathology in specialized foot and ankle surgical practices, often presenting alongside chronic lateral ankle instability (CLAI).
Pathophysiology of Subluxation and Dislocation
The pathophysiological cascade leading to peroneal tendon subluxation is fundamentally a failure of the static restraints to withstand the dynamic forces exerted by the peroneal musculature. The primary mechanism of injury is a sudden, forceful reflex contraction of the peroneus longus and brevis muscles in an attempt to stabilize the ankle during a sudden inversion or dorsiflexion stress. This immense isovolumetric contraction creates a massive anteriorly directed vector force against the Superior Peroneal Retinaculum. If the force exceeds the tensile strength of the SPR or its periosteal attachment, the retinaculum fails. Eckert and Davis classified these failures into four distinct grades: Grade I involves the SPR stripping the periosteum from the fibula; Grade II involves an avulsion of the fibrocartilaginous ridge; Grade III is a cortical avulsion fracture (the "fleck sign"); and Grade IV involves the SPR tearing off its posterior calcaneal insertion. Once the primary restraint is compromised, the tendons are free to translate anteriorly over the lateral malleolus. Repeated subluxation events lead to progressive attenuation of the soft tissues, chronic tenosynovitis, and mechanical attrition of the peroneus brevis tendon as it is compressed between the fibula and the overlying peroneus longus.
Detailed Surgical Anatomy and Biomechanics
Osteology of the Distal Fibula and Retromalleolar Groove
A profound understanding of the osseous morphology of the distal fibula is paramount for successful surgical intervention. The retromalleolar groove, located on the posterior aspect of the lateral malleolus, serves as the primary osseous conduit for the peroneal tendons. Cadaveric and advanced imaging studies have demonstrated significant anatomical variance in the morphology of this groove. Approximately 82% of the population possesses a concave groove, 11% exhibit a flat groove, and 7% present with a convex morphology. The presence of a flat or convex groove drastically reduces the intrinsic osseous stability of the tendons, rendering the individual highly susceptible to dislocation even with relatively minor trauma. The lateral border of this groove is bordered by a distinct fibrocartilaginous ridge, which effectively deepens the sulcus by an additional 2 to 3 millimeters. Preservation or reconstruction of this ridge and the smooth cortical floor of the groove is a critical objective during any deepening procedure to prevent postoperative tendon attrition.
The Superior Peroneal Retinaculum Complex
The Superior Peroneal Retinaculum (SPR) is the paramount static stabilizer of the peroneal tendons. It is a distinct, thickened band of the crural fascia, originating from the periosteum of the posterolateral distal fibula and extending posteroinferiorly to insert onto the lateral wall of the calcaneus and the Achilles tendon sheath. Histologically, the SPR is composed of dense, organized type I collagen fibers designed to resist immense transverse tension. The SPR forms the posterior and lateral boundaries of the fibro-osseous tunnel housing the tendons. It is crucial to recognize that the SPR is not an isolated structure; it is intimately contiguous with the superficial fascia of the leg proximally and the inferior peroneal retinaculum (IPR) distally. The anatomical tension and integrity of the SPR must be meticulously restored during surgery. Furthermore, the sural nerve, providing sensation to the lateral aspect of the foot, courses superficially in the posterolateral ankle, typically crossing the operative field 1 to 2 centimeters posterior to the fibula, making it highly vulnerable during surgical exposure and retinacular repair.
Biomechanics of the Peroneal Tendons
The peroneus longus and brevis are the primary evertors of the foot and play a critical role in dynamic lateral ankle stabilization and the regulation of the first ray during the stance phase of gait. Within the retromalleolar groove, the peroneus brevis is situated anteriorly and medially, directly abutting the fibular cortex, while the peroneus longus lies posteriorly and laterally. During active dorsiflexion and eversion, the tendons undergo significant longitudinal excursion. The lateral malleolus acts as an anatomical pulley, altering the line of pull of the tendons. This pulley mechanism generates a substantial anteriorly directed resultant force vector. In a healthy ankle, the depth of the groove and the integrity of the SPR counteract this vector. However, in the setting of SPR incompetence, active dorsiflexion causes the peroneus longus to compress the peroneus brevis against the sharp posterior edge of the fibula, leading to the classic longitudinal split tears of the brevis tendon—a hallmark consequence of chronic instability that must be addressed concurrently during surgical reconstruction.
Exhaustive Indications and Contraindications
Clinical Presentation and Diagnostic Criteria
Patients suffering from peroneal tendon instability present with a distinct constellation of symptoms and clinical signs. In the acute setting, patients report a history of forced dorsiflexion with an audible "pop" or snapping sensation posterolateral to the ankle, followed by severe pain, ecchymosis, and edema localized over the retromalleolar region. Chronic presentations are characterized by recurrent, painful snapping or a subjective sensation of the ankle "giving way," particularly when walking on uneven terrain or pivoting. The hallmark of physical examination is the provocation test: the patient is instructed to actively dorsiflex and evert the foot against manual resistance. In a positive test, the tendons can be palpated or visually observed subluxating anteriorly over the lateral malleolus. Furthermore, exquisite tenderness along the peroneal tendon sheath and pain with passive inversion (stretching the tendons) are common. Diagnostic imaging is critical; weight-bearing radiographs may reveal the pathognomonic "fleck sign," while dynamic ultrasound provides real-time visualization of the subluxation. High-resolution MRI is the definitive modality for assessing groove morphology, SPR integrity, and concomitant intrasubstance tendon tears.
Definitive Indications for Operative Intervention
Surgical management is dictated by the chronicity of the injury, the morphological characteristics of the fibula, and the functional demands of the patient. Operative intervention is definitively indicated in the following scenarios:
1. Acute, traumatic peroneal tendon dislocation in high-demand elite athletes or active individuals where conservative management (cast immobilization in plantarflexion and inversion) carries an unacceptably high risk of recurrence and prolonged absence from sport.
2. Chronic, recurrent peroneal tendon subluxation or dislocation that has proven refractory to a comprehensive non-operative regimen, including aggressive physical therapy, proprioceptive training, and functional bracing for a minimum of 3 to 6 months.
3. Subluxation accompanied by MRI-confirmed high-grade longitudinal split tears of the peroneus brevis or longus tendons that necessitate open debridement, synovectomy, and tubularization.
4. Symptomatic instability in the presence of a demonstrably convex or severely flattened retromalleolar groove, where isolated soft tissue repair is biomechanically doomed to fail.
Absolute and Relative Contraindications
While surgical correction is highly successful, careful patient selection is imperative to avoid catastrophic complications. Absolute contraindications include active local or systemic infection, severe peripheral arterial disease compromising the vascularity of the posterolateral ankle, and medically unstable patients unfit for general or regional anesthesia. A critical relative contraindication—and a frequent cause of primary surgical failure—is an unaddressed, rigid cavovarus foot deformity. A cavovarus morphotype places immense, continuous eccentric stress on the lateral compartment and the peroneal retinaculum. The surgeon must perform a Coleman block test preoperatively to determine if the hindfoot varus is flexible and forefoot-driven. Failure to concurrently correct a rigid hindfoot varus (e.g., via a lateralizing calcaneal osteotomy or dorsiflexion first metatarsal osteotomy) will inevitably lead to massive mechanical overload and catastrophic failure of the SPR repair and groove deepening.
| Category | Specific Indications / Contraindications | Clinical Rationale |
|---|---|---|
| Indications | Acute dislocation in elite athletes | Minimizes time away from sport; prevents chronic tendon attrition. |
| Indications | Chronic refractory subluxation | Restores biomechanical stability and eliminates pain/snapping. |
| Indications | Concomitant peroneus brevis split tears | Prevents progressive tendon rupture; requires open tubularization. |
| Contraindications | Unaddressed rigid cavovarus foot deformity | CRITICAL: Will cause mechanical failure of the repair due to extreme varus stress. |
| Contraindications | Severe peripheral vascular disease | High risk of wound dehiscence and flap necrosis. |
| Contraindications | Active local soft tissue infection | Absolute contraindication to elective orthopedic hardware/repair. |
Pre-Operative Planning, Templating, and Patient Positioning
Advanced Imaging and Pre-Operative Templating
Meticulous preoperative planning begins with a comprehensive review of advanced imaging. Axial MRI cuts are the most critical sequences for the operating surgeon. These images allow for precise quantification of the retromalleolar groove depth and the identification of a flat or convex fibular morphology. The surgeon must template the expected depth of the excavation required (typically 6 to 9 millimeters) to achieve a stable concavity. Furthermore, the MRI must be scrutinized for the "magic angle" artifact, which can mimic tendinosis, and true longitudinal split tears of the peroneus brevis, which dictate the need for extensive tendon debridement. If a bony avulsion (Eckert-Davis Grade III) is present on radiographs, the surgeon must plan for either excision of the fragment with soft tissue repair or internal fixation using miniature screws or suture anchors, depending on the fragment's size and structural integrity.
Anesthesia and Operating Room Setup
The procedure is typically performed under general anesthesia or a highly effective regional anesthetic block (e.g., popliteal sciatic nerve block combined with a saphenous nerve block). Regional anesthesia provides excellent intraoperative muscle relaxation and profound postoperative analgesia, facilitating early discharge in an ambulatory surgery setting. The operating room should be equipped with a high-speed pneumatic or electric burr system (e.g., a 3-mm or 4-mm cutting burr) for precise cancellous bone removal. Fine, sharp osteotomes (1/4 inch and 1/2 inch) are mandatory for elevating the delicate osteoperiosteal flap without fracturing the cortical shell. Micro-suture anchors (typically 2.4mm to 3.0mm, double-loaded with high-strength non-absorbable suture) should be available for retinacular reconstruction.
Optimal Patient Positioning and Tourniquet Application
Optimal patient positioning is crucial for unhindered access to the posterolateral ankle. The preferred position is the true lateral decubitus position with the operative extremity facing upward. All bony prominences must be meticulously padded, and an axillary roll placed to protect the brachial plexus. Alternatively, some surgeons prefer a supine position with a massive bump placed under the ipsilateral hip. This internally rotates the lower extremity, bringing the lateral malleolus into the superior surgical field. While supine positioning allows easier access to the anterior ankle if concomitant procedures are required, the lateral decubitus position provides superior, direct orthogonal visualization of the retromalleolar groove. A well-padded pneumatic tourniquet is applied to the proximal thigh. Following strict exsanguination of the limb using an Esmarch bandage, the tourniquet is inflated to 250-300 mmHg to ensure a completely bloodless surgical field, which is critical for identifying the sural nerve and assessing the microvascularity of the osteoperiosteal hinge.
Step-by-Step Surgical Approach and Fixation Technique
Superficial Dissection and Sural Nerve Protection
The surgical approach begins with a 7 to 8-centimeter J-shaped or curvilinear incision centered over the posterior border of the distal third of the fibula, extending distally and curving gently toward the base of the fifth metatarsal. The incision must be placed slightly posterior to the fibula to avoid placing the surgical scar directly over the bony prominence, which can lead to painful postoperative footwear impingement. Deepening the incision through the subcutaneous fat must be performed with extreme caution using blunt dissection techniques. The sural nerve and the lesser saphenous vein are highly variable in their course but generally traverse the operative field 1 to 2 centimeters posterior to the lateral malleolus. Once identified, the nerve should be gently mobilized and protected with a vessel loop, retracting it posteriorly. Aggressive retraction or devascularization of the sural nerve must be avoided to prevent debilitating postoperative complex regional pain syndrome (CRPS) or painful neuromas.
Tendon Inspection and Pathology Management
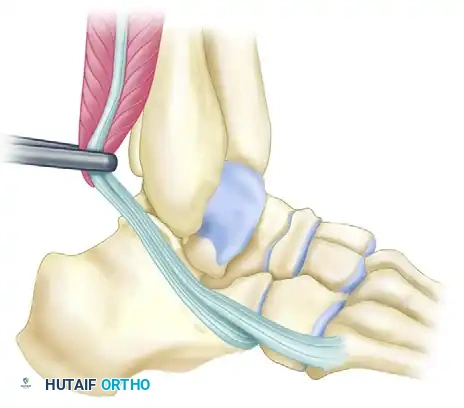
Following superficial dissection, the deep crural fascia and the remnants of the Superior Peroneal Retinaculum are identified. The SPR is incised longitudinally, slightly posterior to its fibular attachment, to open the peroneal tendon sheath.
Figure A: With the tendons freed from their sheath, retract them anteriorly over the lateral malleolus to expose the retromalleolar groove.
The peroneus longus and brevis tendons are systematically delivered from the wound and inspected circumferentially. Pathological alterations are nearly universal in chronic cases. The peroneus brevis, due to its vulnerable position against the fibula, frequently exhibits longitudinal split tears or severe tenosynovitis. Degenerative, non-viable tissue must be sharply debrided. If a longitudinal split is identified, the tendon is repaired via a running locked tubularization technique using 4-0 non-absorbable monofilament suture. If the brevis tendon is severely degenerated (greater than 50% cross-sectional area loss), a tenodesis of the proximal and distal stumps of the brevis to the adjacent, intact peroneus longus tendon may be required. Once the tendons are addressed, they are retracted anteriorly over the lateral malleolus to fully expose the retromalleolar groove.
Direct Repair of the Superior Peroneal Retinaculum
In the minority of cases where the retromalleolar groove demonstrates adequate, anatomical concavity, an isolated direct repair of the SPR may be sufficient. The posterior aspect of the lateral malleolus is meticulously decorticated using a rongeur or a high-speed burr to create a bleeding, osteogenic bed. The redundant or avulsed SPR is mobilized. Using 2.4mm or 3.0mm suture anchors placed along the posterolateral ridge of the fibula, the SPR is advanced and securely tied down, effectively plicating the retinaculum and eliminating any redundant capsular volume. The repair must be tensioned with the ankle in neutral dorsiflexion and slight eversion. Over-tensioning must be avoided, as it can lead to stenosing tenosynovitis within the newly reconstructed fibro-osseous tunnel.
Fibular Groove Deepening via Osteoperiosteal Flap
For the vast majority of chronic instability cases presenting with a shallow or convex groove, the Zoellner and Clancy groove deepening technique is the definitive procedure. With the tendons retracted, a rectangular osteoperiosteal flap is mapped out on the posterolateral aspect of the distal fibula. The flap typically measures 3 to 4 centimeters in length and 1 to 1.5 centimeters in width. Using a sharp scalpel, the periosteum is incised along the proximal, distal, and lateral borders. Crucially, the posteromedial border is left completely intact.
Using a highly sharp, thin 1/4-inch osteotome, a cortical bone flap (approximately 2 to 3 millimeters thick) is carefully elevated from lateral to medial. The intact posteromedial periosteum acts as a "living hinge," ensuring the cortical flap retains its vital blood supply and does not become an avascular piece of free bone graft. Once elevated, the flap is swung posteriorly on its hinge, exposing the underlying cancellous bone of the distal fibular metaphysis.
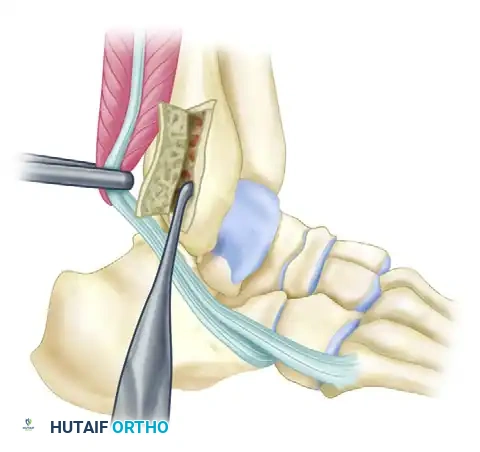
Figure B: The cortical flap is hinged posteriorly. Cancellous bone is systematically removed from the posterior aspect of the fibula to deepen the groove.
A high-speed motorized burr or a sharp curette is then utilized to systematically excavate the cancellous bone. The goal is to create a uniform, concave trough approximately 6 to 9 millimeters deep. The surgeon must exercise extreme caution not to violate the anterior or medial cortices of the fibula, which could precipitate an iatrogenic fracture. Once adequate depth is achieved, the osteoperiosteal flap is gently tamped back into the newly created defect. Because the smooth, native cortical surface of the flap is preserved, it provides an anatomically perfect, frictionless gliding surface for the peroneal tendons, drastically reducing the risk of postoperative adhesions compared to techniques that leave raw cancellous bone exposed.
Retinaculum Augmentation and Final Closure
With the groove deepened and the flap impacted into place, the peroneal tendons are relocated into their anatomical position. The ankle is taken through a rigorous range of motion, specifically forced active-simulated dorsiflexion and eversion, to confirm absolute stability of the tendons within the deepened sulcus. Attention is then turned to the SPR. If the native SPR is robust, it is directly repaired over the tendons using suture anchors or transosseous drill holes.
However, in many chronic cases, the SPR is severely attenuated, friable, or completely incompetent. In these scenarios, a retinacular augmentation is mandated. A secondary periosteal flap, measuring approximately 1 to 1.5 square centimeters, is raised from the lateral surface of the lateral malleolus, leaving its posterior edge hinged.
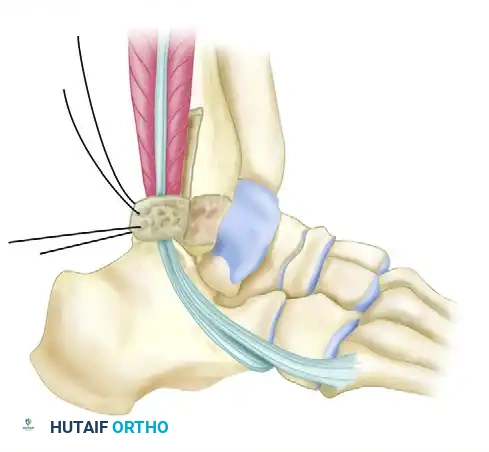
Figure C: The secondary periosteal flap is swung posteriorly over the tendons in the deepened groove and sutured to the medial part of the peroneal retinaculum to reinforce the repair.
This secondary flap is reflected posteriorly, draped over the relocated tendons, and sutured securely to the medial remnants of the native SPR or the adjacent Achilles fascia using 2-0 non-absorbable sutures. This effectively creates a robust, vascularized neo-retinaculum. The tourniquet is then deflated, and meticulous hemostasis is achieved. The subcutaneous tissues are approximated with 2-0 or 3-0 absorbable sutures, and the skin is closed with a non-absorbable monofilament in a vertical mattress fashion to minimize wound edge necrosis. A sterile, bulky compressive dressing and a rigid short-leg splint are applied in the operating room with the ankle locked in neutral dorsiflexion and slight eversion.
Complications, Incidence Rates, and Salvage Management
Intraoperative Complications and Mitigation
Intraoperative complications, while relatively rare in experienced hands, require immediate recognition and skilled management. The most catastrophic intraoperative error during the groove deepening procedure is the iatrogenic fracture of the lateral malleolus. This occurs if the surgeon aggressively burrs the cancellous bone and inadvertently breaches the anterior or medial cortex, creating a massive stress riser. If a fibular fracture occurs, the procedure must immediately pivot to formal Open Reduction and Internal Fixation (ORIF) using a lateral neutralization plate and screws to restore fibular stability before proceeding with the tendon relocation. Another significant intraoperative complication is the complete avulsion of the osteoperiosteal flap from its medial hinge, converting a vascularized flap into a free bone graft. If this occurs, the free cortical shell should still be utilized, but it must be meticulously impacted and potentially secured with a bioabsorbable pin to prevent migration, acknowledging that the risk of non-union or resorption is significantly increased.
Postoperative Complications and Recurrence
The most common postoperative complication is sural neuritis, with an incidence ranging from 5% to 10% in the literature. This can result from direct intraoperative nerve laceration, aggressive traction leading to neuropraxia, or entrapment in postoperative scar tissue. Initial management involves aggressive desensitization therapy, gabapentinoids, and targeted ultrasound-guided corticosteroid injections. Refractory cases may necessitate surgical neurolysis or neurectomy with proximal burying of the nerve stump into muscle.
Recurrent subluxation is the most feared complication, occurring in less than 5% of patients who undergo a combined groove deepening and SPR repair. Recurrence is almost universally attributed to technical errors (inadequate groove depth, loose SPR repair) or, most critically, the failure to recognize and surgically address a concomitant hindfoot cavovarus deformity. Postoperative stiffness and peritendinous adhesions are also potential issues, highlighting the delicate balance required in postoperative immobilization. Prolonged casting beyond 3 to 4 weeks significantly increases the risk of symptomatic adhesions, necessitating early, controlled sagittal plane mobilization.
Salvage Procedures for the Failed Primary Repair
Management of a failed primary peroneal tendon stabilization is a complex surgical challenge. When revision surgery is indicated, the surgeon must reassess the entire biomechanical axis of the lower extremity. If a cavovarus deformity was missed, a lateralizing calcaneal osteotomy (e.g., Dwyer or sliding osteotomy) is an absolute necessity to correct the mechanical axis. For the local soft tissue and osseous failure, salvage options include massive bone block procedures (e.g., the Kelly or DuVries techniques), which involve sliding a large cortical block of the lateral fibula posteriorly to act as a physical barrier. Alternatively, tendon rerouting techniques can be employed. The most robust salvage soft tissue procedure involves incising the calcaneofibular ligament (CFL), routing the peroneal tendons deep to the CFL, and subsequently repairing the ligament. The CFL then acts as an unyielding, massive anatomical restraint against anterior tendon translation, though this alters normal subtalar kinematics and is strictly reserved for complex revision scenarios.
| Complication | Estimated Incidence | Primary Etiology | Salvage / Management Strategy |
|---|---|---|---|
| Sural Neuritis / Neuroma | 5% - 10% | Traction injury, scar entrapment, direct laceration. | Gabapentinoids, targeted blocks, surgical neurolysis/neurectomy. |
| Recurrent Subluxation | < 5% (with combined repair) | Missed cavovarus deformity, inadequate groove depth. | Calcaneal osteotomy, CFL tendon rerouting, bone block procedures. |
| Peroneal Tendon Adhesions | 10% - 15% | Prolonged immobilization, excessive surgical trauma. | Aggressive physical therapy, surgical tenolysis if refractory. |
| Iatrogenic Fibular Fracture | < 1% | Excessive cancellous burring breaching anterior cortex. | Immediate intraoperative ORIF with lateral plate and screws. |
Phased Post-Operative Rehabilitation Protocols
Phase I Maximum Protection Phase (Weeks 0 to 3)
The immediate postoperative period prioritizes the protection of the delicate retinacular repair and the integration of the osteoperiosteal flap. Upon leaving the operating room, the patient is placed in a rigid, well-padded short-leg splint. The ankle must be strictly immobilized in neutral dorsiflexion (90 degrees to the tibial shaft) and slight eversion. This specific positioning minimizes tension on the reconstructed Superior Peroneal Retinaculum and prevents the tendons from engaging in the pulley mechanism that drives them anteriorly. The patient is instructed to maintain strict non-weight-bearing (NWB) status using crutches or a knee scooter. Aggressive edema control is paramount; the limb must be elevated above the level of the heart for the majority of the day to promote optimal wound healing and prevent wound dehiscence, a critical concern in the relatively hypovascular posterolateral ankle.
Phase II Controlled Mobilization Phase (Weeks 3 to 6)
At the three-week postoperative mark, the initial splint or cast is removed, and the surgical incisions are inspected. Assuming uncomplicated wound healing, the patient is transitioned into a controlled ankle motion (CAM) walker boot equipped with a hinged mechanism. The rehabilitation focus shifts to preventing peritendinous adhesions while continuing to protect the lateral repair. The hinge is unlocked to allow active and active-assisted range of motion exclusively in the sagittal plane (dorsiflexion and plantar flexion). Active and passive inversion are strictly prohibited during this phase, as inversion places immense tensile stress on the healing SPR. Weight-bearing is progressively advanced. Depending on the surgeon's assessment of repair security and patient compliance, the patient may progress from partial weight-bearing to full weight-bearing as
