Deciding to Remove Hip Arthroplasty with Well-Fixed Components

Key Takeaway
This topic focuses on Deciding to Remove Hip Arthroplasty with Well-Fixed Components, In hip arthroplasty, well-fixed implants might require removal for several reasons. For instance, a hip arthroplasty with wellfixed components may necessitate revision due to infection, recurrent dislocations, limb-length discrepancy, severe osteolysis, or polyethylene wear. Other causes include locking mechanism failure or a femoral stem fracture. Determining specific components to remove is crucial.
Introduction and Epidemiology
The extraction of well-fixed femoral and acetabular implants during revision total hip arthroplasty represents a formidable technical challenge requiring meticulous preoperative planning, advanced surgical techniques, and an intimate understanding of periprosthetic anatomy. Revision total hip arthroplasty is performed with increasing frequency due to the expanding volume of primary arthroplasties and the extended life expectancy of patients. While the primary goal of revision surgery is to address the mode of failure, surgeons frequently encounter scenarios where a component is clinically failing (e.g., malposition, infection, or osteolysis) yet remains rigidly fixed to the host bone.

The decision to remove a well-fixed component must balance the necessity of extraction against the inevitable morbidity associated with the procedure. Removing well-fixed implants carries a significant risk of iatrogenic bone loss, periprosthetic fracture, and extended operative times. Consequently, the key intraoperative determination is identifying which components strictly necessitate removal and which are sufficiently well-fixed and appropriately positioned to be retained.

Epidemiological data suggests that instability, aseptic loosening, and periprosthetic joint infection are the leading causes of revision total hip arthroplasty. In cases of periprosthetic joint infection, the standard of care typically mandates the complete explantation of all foreign bodies, regardless of fixation status, to eradicate biofilm. Conversely, in cases of isolated polyethylene wear or modular component failure, retention of a well-fixed, optimally positioned shell or stem is preferred to preserve host bone stock.
The burden of revision total hip arthroplasty continues to grow exponentially. Joint replacement registries worldwide, including the National Joint Registry (NJR) and the American Joint Replacement Registry (AJRR), indicate that revisions account for approximately 10% to 15% of all hip arthroplasty procedures performed annually. The complexity of these cases is magnified by the evolution of implant technology. Modern highly porous titanium and trabecular metal components are designed to achieve rapid, robust osteointegration. While this is highly desirable in the primary setting, it transforms the revision of a well-fixed component into an arduous surgical endeavor.
When evaluating the epidemiology of component extraction, it is critical to stratify by the mode of primary failure. Instability often requires the revision of one or both components to correct version, offset, or center of rotation. If a well-fixed acetabular shell is malpositioned (e.g., excessive retroversion or vertical inclination), retention with a face-changing liner may be considered, but severe malposition mandates extraction. Adverse local tissue reactions (ALTR) secondary to trunnionosis or metal-on-metal articulation present another distinct epidemiological subset. In these scenarios, the femoral stem may be rigidly fixed, but severe corrosion at the head-neck taper may necessitate stem extraction if a new modular head cannot be safely or securely engaged.

Ultimately, the epidemiology of well-fixed component extraction highlights a shift in revision arthroplasty. Historically, surgeons revised loose, cemented implants where extraction was relatively straightforward. Today, the contemporary revision surgeon must be equipped to dismantle fully porous-coated, extensively ingrown implants without compromising the structural integrity of the remaining host bone.

Surgical Anatomy and Biomechanics
A profound understanding of pelvic and femoral anatomy is paramount when navigating the distorted tissue planes typical of revision hip surgery. Important anatomic considerations include the pelvic osteological landmarks, the proximal femoral architecture, and the surrounding neurovascular structures.

Pelvic Osteology and Landmarks
The pelvic landmarks that assist in component removal and subsequent revision positioning include the ischium, pubis, anterior and posterior acetabular columns, anterior inferior iliac spines, transverse acetabular ligament, sciatic notch, and acetabular walls.

Preservation of the anterior and posterior columns during acetabular explantation is critical, as these structures provide the mechanical foundation for reimplantation. The transverse acetabular ligament serves as a reliable landmark for establishing the inferior margin and version of the reconstructed acetabulum. The ischium and pubis must be carefully identified, particularly when placing revision hardware such as cages or multi-hole hemispherical shells, to ensure safe screw trajectory away from intrapelvic structures.

When extracting a well-fixed acetabular shell, the surgeon must be acutely aware of the vascular anatomy divided into the four Wasielewski quadrants. The anterior-superior quadrant risks injury to the external iliac vessels, while the anterior-inferior quadrant contains the obturator neurovascular bundle. The posterior-superior quadrant is generally considered the "safe zone" for screw placement, though over-penetration can still endanger the superior gluteal vessels and sciatic nerve. The posterior-inferior quadrant carries a risk to the internal pudendal and inferior gluteal vessels. Aggressive use of extraction osteotomes or explant blades that breach the medial wall or quadrilateral plate can result in catastrophic vascular injury.

Proximal Femoral and Diaphyseal Anatomy
The proximal femoral anatomy includes the greater and lesser trochanters and the vastus ridge. The vastus ridge frequently represents a point of relatively weak bone in revision scenarios due to osteolysis, previous trochanteric osteotomies, or stress shielding from the primary implant.

The femoral diaphyseal anatomy is defined by the attachments of the vastus musculature at the vastus ridge anteriorly and at the linea aspera posteriorly. These muscular attachments often must be elevated or reflected during an extended trochanteric osteotomy to mobilize the osteotomized fragment and aid in the extraction of well-fixed femoral stems.

Biomechanically, the extraction of a well-fixed stem requires disrupting the bone-implant interface. In cemented stems, the interface consists of bone-cement and cement-implant boundaries. Cemented stems can often be extracted by disrupting the cement-implant interface, followed by piecemeal removal of the cement mantle. In cementless stems, fixation relies on biological ingrowth (porous coatings) or ongrowth (grit-blasted surfaces).
The biomechanics of extraction dictate that shear forces must be applied to break these biological bonds. However, the shear strength of bone ingrowth into modern highly porous metals often exceeds the ultimate tensile strength of the surrounding cancellous and cortical bone. Consequently, applying raw extraction force via a slap hammer to a well-fixed porous stem without adequately disrupting the interface with flexible osteotomes or an extended trochanteric osteotomy will inevitably result in a periprosthetic fracture.

Stress shielding further complicates femoral anatomy in the revision setting. Proximal stress shielding, commonly seen with extensively porous-coated cylindrical stems, leads to severe calcar resorption and cortical thinning. This fragile proximal bone tube is highly susceptible to fragmentation during stem extraction. Surgeons must recognize that the diaphyseal bone providing the robust distal fixation is often the only reliable bone stock remaining, making controlled extraction imperative to preserve the isthmus for the subsequent revision stem.

Indications and Contraindications
The decision to extract or retain a well-fixed component is one of the most consequential judgments in revision hip arthroplasty. The overarching principle is to minimize surgical morbidity while ensuring the mechanical and biological success of the revision reconstruction.

Absolute indications for the removal of well-fixed components include chronic periprosthetic joint infection (PJI). In the setting of a two-stage exchange for PJI, eradication of the biofilm requires the explantation of all foreign materials, including well-fixed stems, cups, and cement mantles. Retention of hardware in the face of chronic infection almost universally leads to recurrent sepsis.

Severe component malposition causing recurrent instability or impingement is another strong indication for extraction. For example, an acetabular component placed in 30 degrees of retroversion cannot typically be salvaged with a face-changing liner without compromising impingement-free range of motion. Similarly, a femoral stem placed in severe retroversion causing anterior instability must be extracted and revised to correct the version.

Adverse local tissue reactions (ALTR) and severe metallosis, often associated with metal-on-metal articulations or mechanically assisted crevice corrosion (trunnionosis), may dictate component removal. If the femoral trunnion is severely damaged, corroded, or deformed, placing a new modular head carries an unacceptably high risk of catastrophic dissociation or recurrent corrosion. In such cases, despite rigid diaphyseal fixation, the stem must be extracted. Alternatively, if the trunnion damage is mild to moderate, a titanium adapter sleeve may be utilized to salvage the well-fixed stem.

Conversely, there are strong indications for component retention. If the primary mode of failure is isolated polyethylene wear with secondary osteolysis, and the acetabular shell remains well-fixed and appropriately positioned, the preferred strategy is liner exchange and bone grafting of the osteolytic lesions. Removing a well-fixed, well-positioned shell in this scenario inflicts unnecessary bone loss and operative morbidity.
Table of Indications for Component Extraction vs Retention
| Clinical Scenario | Recommendation | Rationale and Considerations |
|---|---|---|
| Chronic Periprosthetic Joint Infection | Extraction (All components) | Eradication of biofilm is impossible with retained hardware. |
| Acute PJI (within 4 weeks of index) | Retention (Selective) | Debridement, Antibiotics, and Implant Retention (DAIR) with modular exchange may be attempted. |
| Severe Acetabular Malposition | Extraction | Cannot be adequately corrected with offset/face-changing liners; high risk of recurrent instability. |
| Isolated Polyethylene Wear | Retention | If shell is well-fixed and well-positioned, liner exchange and lesion grafting preserve bone stock. |
| Severe Trunnionosis / Corroded Taper | Extraction | A damaged trunnion cannot securely hold a new head, risking dissociation or ongoing ALTR. |
| Mild Trunnionosis | Retention | Can often be salvaged using a titanium taper adapter sleeve if the stem is rigidly fixed. |
| Recurrent Instability (Stem Retroversion) | Extraction | Version correction is required to restore appropriate hip biomechanics and stability. |
| Massive Osteolysis threatening fixation | Extraction | Even if clinically stable, impending catastrophic failure or fracture warrants revision before massive bone loss occurs. |
Contraindications to extracting a well-fixed component are largely relative and center on patient frailty and the risk of catastrophic bone loss. In a medically fragile, elderly patient with a well-fixed but slightly malpositioned component causing infrequent subluxation, the physiological insult of a massive extraction and reconstruction may outweigh the benefits. In such cases, utilizing constrained liners or dual-mobility articulations within the existing well-fixed shell may provide a safer, albeit compromised, salvage solution.

Furthermore, the lack of appropriate extraction equipment or surgical expertise is an absolute contraindication to attempting the removal of extensively porous-coated implants. These procedures should be referred to tertiary centers equipped with specialized extraction instrumentation, ultrasonic cement removal tools, and a comprehensive inventory of revision implants, including custom triflange components or structural allografts.

Pre Operative Planning and Patient Positioning
Thorough preoperative planning is the cornerstone of successful component extraction. The surgeon must anticipate the structural deficits that will remain after the well-fixed implants are removed. This requires a comprehensive radiographic and clinical evaluation.
Standard preoperative imaging must include an anteroposterior (AP) radiograph of the pelvis, an AP of the affected hip, and a cross-table lateral view. Judet views (iliac and obturator obliques) are essential if acetabular component extraction is planned, as they allow for the evaluation of the anterior and posterior columns.

Advanced imaging is increasingly utilized in complex revisions. Computed Tomography (CT) with Metal Artifact Reduction Sequence (MARS) provides invaluable three-dimensional data regarding the extent of periprosthetic osteolysis, the integrity of the cortical bone, and the exact position and version of the components. MARS CT is particularly useful in differentiating between a well-fixed component and one with subtle fibrous encapsulation that may not be apparent on plain radiographs.
Digital templating is mandatory. The surgeon must template not only the anticipated revision components but also the existing components to understand their geometry. Knowing the exact make, model, and dimensions of the well-fixed implants is critical. This information dictates the specific extraction tools required. For example, knowing the core diameter of a cylindrical fully porous-coated stem allows the surgeon to select the appropriately sized trephine. Knowing the locking mechanism of an acetabular liner ensures the correct tools are available to disengage it without damaging the shell, should retention be an option.
Preoperative medical optimization is crucial. Revision arthroplasty involving component extraction is associated with significant blood loss. Patient blood management strategies, including preoperative optimization of hemoglobin, the use of intraoperative tranexamic acid (TXA), and the availability of cell salvage systems, must be coordinated.

Patient Positioning and Operating Room Setup
Patient positioning depends on the surgeon's preferred approach, though the lateral decubitus position is most commonly employed for revision total hip arthroplasty. Rigid pelvic fixation using peg boards or a specialized bean bag is essential, as significant force and manipulation are required during component extraction. The pelvis must be strictly perpendicular to the floor to ensure accurate assessment of version and inclination during the subsequent reconstruction.
The operating room setup must include a comprehensive array of extraction instrumentation. This includes:
* Flexible osteotomes of various lengths and geometries.
* Acetabular explant systems (e.g., Zimmer Explant, Explant blades of varying radii).
* Femoral trephines matching the diameter of the retained stem.
* High-speed metal-cutting burrs (e.g., Midas Rex) for sectioning components.
* Ultrasonic cement removal devices (e.g., OSCAR) if a cemented component is being revised.
* Slap hammers, vice grips, and universal extraction devices.
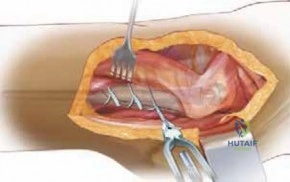
* Extended trochanteric osteotomy (ETO) instrumentation, including oscillating saws, Gigli saws, and cerclage cable systems.

Ensuring all necessary equipment is sterilized and available in the operating room prior to incision prevents catastrophic intraoperative delays and compromises in surgical technique.
Detailed Surgical Approach and Technique
The surgical approach must provide extensile exposure to both the acetabulum and the femur. The posterior approach is the workhorse of revision hip arthroplasty, offering excellent visualization of the posterior column, proximal femur, and diaphyseal bone.
Acetabular Component Extraction Techniques
Extracting a well-fixed cementless acetabular shell is a delicate procedure aimed at preserving the cavitary and segmental bone of the acetabulum. The first step is the removal of the modular liner. If the liner is polyethylene, it can often be levered out or drilled and engaged with a screw to pull it free. If it is a ceramic or metal liner, specialized suction or extraction tools provided by the manufacturer may be required.

Once the shell is exposed, any retaining screws must be removed. Stripped screw heads are a common complication; high-speed burrs or specialized screw extraction kits must be available to core out or reverse stripped screws. Attempting to extract a shell with retained screws will result in massive avulsion of the pelvic bone.
The interface between the metal shell and the host bone must then be disrupted. The use of specialized acetabular explant systems is the gold standard. These systems utilize a centering head that articulates with the inner diameter of the shell, guiding a curved, hemispherical blade along the bone-implant interface.
The surgeon must carefully select the blade size to match the outer diameter of the shell. The blade is driven sequentially around the periphery of the component. It is critical to avoid allowing the blade to drift into the host bone, particularly medially through the quadrilateral plate or superiorly into the weight-bearing dome. If the explant blade binds, it must be reversed and a smaller blade or a different starting point utilized.

In cases of highly porous trabecular metal cups, bone ingrowth can be so profound that conventional explant blades cannot penetrate the interface without risking pelvic fracture. In these extreme scenarios, the surgeon may need to use a high-speed metal-cutting burr to section the titanium shell into quadrants. The individual quadrants can then be carefully collapsed inward and peeled away from the bone, minimizing peripheral bone loss.
Femoral Component Extraction Techniques
The extraction of a well-fixed femoral stem is highly dependent on the stem's design and fixation philosophy.
For well-fixed cemented stems, the interface of choice for disruption is the cement-implant interface. Flexible osteotomes are driven down the proximal interface to break the bond. Vice grips and a slap hammer are then applied to the trunnion. Once the stem is removed, the retained cement mantle must be extracted. This is best accomplished using ultrasonic cement removal tools, which melt the cement without damaging the surrounding cortical bone, allowing it to be removed in segments.
For well-fixed proximally porous-coated tapered wedge stems, the ingrowth is limited to the metaphyseal region. Flexible osteotomes, carefully directed along the anterior, posterior, medial, and lateral borders of the proximal sleeve, can often disrupt the fixation sufficiently to allow extraction with a slap hammer. Care must be taken to protect the greater trochanter, which is highly susceptible to fracture during this maneuver.
The most challenging scenario is the extraction of a well-fixed, extensively porous-coated cylindrical stem. These stems achieve rigid diaphyseal fixation over a large surface area. Attempting to extract these stems from a superior approach using osteotomes alone is nearly impossible and carries an unacceptably high risk of shattering the proximal femur.
Trephines (hollow reamers) can be used to core out the bone around the cylindrical stem. The trephine is passed over the trunnion and driven distally. However, the surgeon must be perfectly co-axial with the stem; any deviation will result in the trephine cutting through the femoral cortex, creating a catastrophic stress riser or complete perforation.

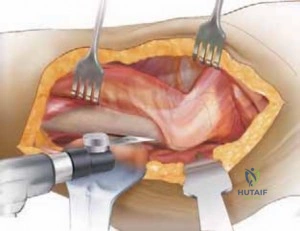
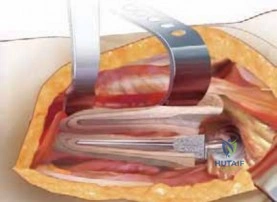
The Extended Trochanteric Osteotomy (ETO)
The Extended Trochanteric Osteotomy (ETO) is the most powerful and reliable technique for extracting well-fixed cementless stems, particularly extensively
Clinical & Radiographic Imaging