Total Hip Arthroplasty: Preparation, Approaches, and Surgical Techniques
Key Takeaway
Total hip arthroplasty requires meticulous preoperative templating, precise patient positioning, and a thorough understanding of surgical anatomy. The choice of surgical approach—whether anterolateral, direct lateral, or posterolateral—dictates the exposure and postoperative stability. This guide provides an evidence-based, step-by-step masterclass on the posterolateral approach, emphasizing biomechanical restoration, soft-tissue preservation, and optimal component positioning to ensure long-term survivorship and functional recovery in orthopedic patients.
Comprehensive Introduction and Patho-Epidemiology
Total Hip Arthroplasty (THA) is universally recognized as one of the most successful and cost-effective surgical interventions in modern medicine, often heralded as the "operation of the century." Originally pioneered by Sir John Charnley in the 1960s, the procedure revolutionized the management of end-stage hip pathology through the introduction of the low-friction arthroplasty concept. Charnley’s fundamental principles—utilizing a small-diameter metallic femoral head articulating with a polymeric acetabular component fixed with polymethylmethacrylate (PMMA) bone cement—laid the groundwork for decades of iterative biomechanical and biomaterial advancements. Today, THA reliably relieves pain, restores functional mobility, and significantly improves the quality of life for millions of patients worldwide, with modern implant survivorship routinely exceeding 90% at two decades of follow-up.
The patho-epidemiology driving the demand for THA is predominantly anchored by primary osteoarthritis (OA), a progressive degenerative joint disease characterized by articular cartilage degradation, subchondral bone sclerosis, osteophyte formation, and joint space narrowing. Primary OA accounts for approximately 70% to 80% of all primary THA indications. However, secondary causes of hip arthritis represent a critical subset of patients who often present with complex anatomical deformities. These include developmental dysplasia of the hip (DDH), osteonecrosis (avascular necrosis) secondary to corticosteroid use, trauma, or coagulopathies, post-traumatic arthritis following acetabular or femoral neck fractures, and inflammatory arthropathies such as rheumatoid arthritis and ankylosing spondylitis. As the global population ages and the prevalence of obesity increases, the demographic profile of the THA patient is simultaneously expanding at both ends of the age spectrum, with younger, highly active patients demanding durable solutions and elderly patients requiring interventions to maintain independent ambulation.
The economic and societal burden of hip osteoarthritis is staggering, necessitating a continuous evolution in surgical efficiency and perioperative care. The advent of Enhanced Recovery After Surgery (ERAS) protocols has drastically shifted the paradigm of THA from a prolonged inpatient admission to a short-stay or even outpatient procedure. This transition is facilitated by multimodal pain management strategies, blood conservation techniques (such as the routine use of tranexamic acid), and minimally invasive surgical approaches that spare soft tissue envelopes. Consequently, the cost-per-Quality-Adjusted Life Year (QALY) gained from THA remains exceptionally favorable, making it a cornerstone procedure not only for orthopedic surgeons but for global healthcare systems managing musculoskeletal disease burdens.
Furthermore, the evolution of bearing surfaces has profoundly altered the epidemiological landscape of THA failures. Historically, the primary mode of mid-to-long-term failure was aseptic loosening driven by particulate debris-induced osteolysis—often termed "polyethylene disease." The introduction of highly cross-linked polyethylene (HXLPE) in the late 1990s, achieved through gamma irradiation and subsequent thermal remodeling (melting or annealing) to eliminate free radicals, has virtually eradicated catastrophic catastrophic wear and subsequent osteolysis. Concurrently, advancements in ceramic-on-ceramic and ceramic-on-polyethylene articulations provide alternative bearing options with exceptionally low wear rates, specifically tailored for the young, high-demand patient demographic. Understanding these epidemiological shifts is paramount for the operating surgeon when selecting the optimal implant construct for an individual patient's specific pathology and life expectancy.
Detailed Surgical Anatomy and Biomechanics
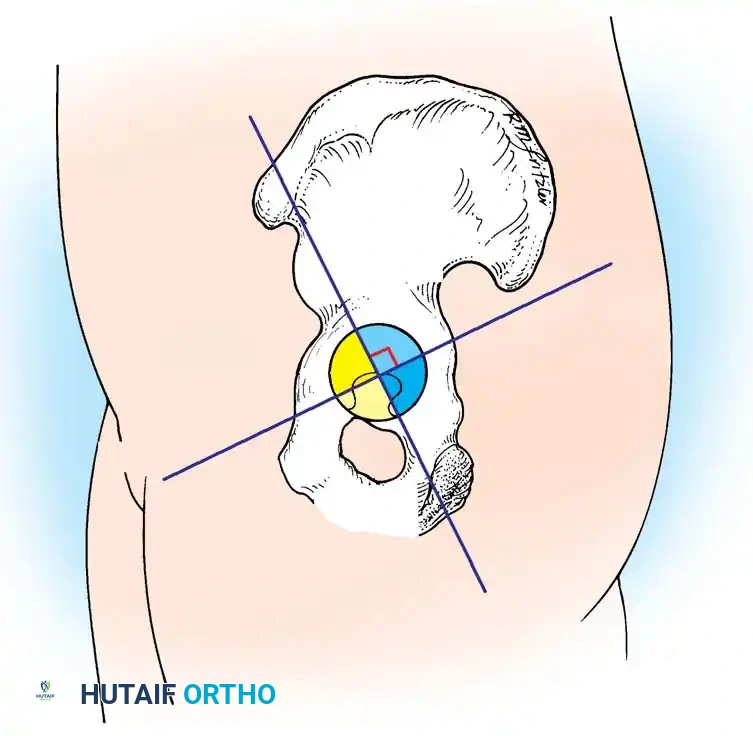
A profound, three-dimensional understanding of hip joint anatomy and its inherent biomechanics is the absolute prerequisite for executing a successful THA. The hip is a highly constrained, multiaxial ball-and-socket (enarthrodial) joint formed by the articulation of the hemispherical femoral head and the cup-shaped acetabulum. The acetabulum itself is a composite structure embryologically derived from the confluence of the ilium, ischium, and pubis at the triradiate cartilage. Surgically, the acetabulum is oriented in approximately 15 to 20 degrees of anteversion and 40 to 45 degrees of abduction (inclination) relative to the coronal and sagittal planes of the pelvis. The true medial wall of the acetabulum is defined radiographically by the ilioischial line and surgically by the cotyloid fossa, which houses the pulvinar and the ligamentum teres. The transverse acetabular ligament (TAL) spans the inferior acetabular notch and serves as a critical intraoperative landmark for determining the native version and inferior seating depth of the acetabular component.
The soft-tissue envelope surrounding the hip joint is robust and compartmentalized, dictating the various surgical intervals utilized during arthroplasty. The abductor complex, comprising the gluteus medius and minimus, originates from the external surface of the ilium and inserts onto the greater trochanter. This musculature is the primary dynamic stabilizer of the pelvis during the single-leg stance phase of gait. Posteriorly, the short external rotators (piriformis, superior gemellus, obturator internus, inferior gemellus, and quadratus femoris) provide dynamic external rotation and posterior stability. Anteriorly, the iliopsoas tendon crosses the joint capsule to insert on the lesser trochanter, acting as the primary hip flexor. The joint capsule itself is reinforced by three powerful ligaments—the iliofemoral (Y ligament of Bigelow), pubofemoral, and ischiofemoral ligaments—which dictate the terminal ranges of motion and must be meticulously managed or repaired depending on the chosen surgical approach.
Neurovascular proximity demands meticulous surgical technique to prevent catastrophic iatrogenic injury. The sciatic nerve, derived from the lumbosacral plexus (L4-S3), exits the greater sciatic foramen typically inferior to the piriformis muscle. It lies in close proximity to the posterior acetabular column and can be injured by excessive retractor pressure, limb lengthening, or direct laceration during the posterolateral approach. The superior gluteal nerve, which innervates the critical abductor musculature, exits the pelvis superior to the piriformis and courses anteriorly between the gluteus medius and minimus. It is at significant risk during direct lateral (Hardinge) or anterolateral approaches if the proximal splitting of the abductors extends beyond the "safe zone" of 3 to 5 centimeters proximal to the tip of the greater trochanter. Anteriorly, the femoral nerve and artery lie within the femoral triangle, separated from the hip capsule by the iliopsoas muscle belly, making them vulnerable during anterior approaches or via errant anterior retractor placement.
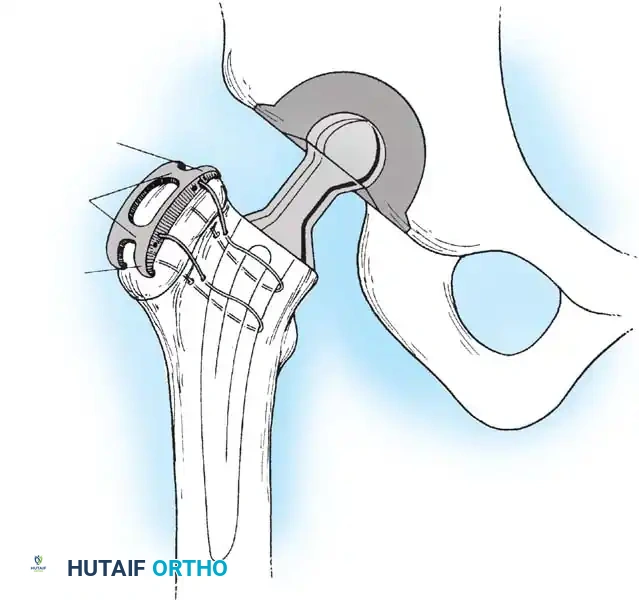
Biomechanically, the hip joint operates as a class I lever system where the fulcrum is the center of rotation (COR) of the femoral head. The body weight acts on a long moment arm extending from the center of gravity to the COR, while the abductor musculature acts on a much shorter moment arm extending from the greater trochanter to the COR. To maintain a level pelvis during single-leg stance, the abductor force must be approximately three times body weight, resulting in a joint reaction force (JRF) across the hip that can exceed four to five times body weight during normal ambulation. The primary biomechanical goal of THA is to medialise the acetabular COR to the true anatomic floor (reducing the body weight moment arm) and to restore or slightly increase femoral offset (increasing the abductor moment arm). This optimization drastically reduces the required abductor force, thereby minimizing the overall JRF, decreasing interfacial stresses at the implant-bone junction, and mitigating the risk of accelerated bearing wear or component loosening.
Exhaustive Indications and Contraindications
The decision to proceed with Total Hip Arthroplasty is predicated on a careful synthesis of the patient's clinical presentation, radiographic findings, and functional limitations. The primary indication for THA is debilitating, end-stage degenerative joint disease—most commonly primary osteoarthritis—that has proven refractory to a comprehensive regimen of non-operative management. This conservative paradigm must include activity modification, weight loss (if applicable), targeted physical therapy focusing on abductor and core strengthening, the judicious use of non-steroidal anti-inflammatory drugs (NSAIDs), and potentially intra-articular corticosteroid injections. Clinically, patients typically present with deep, aching groin pain that exacerbates with weight-bearing and transitions into rest pain or night pain, severely disrupting sleep architecture. Functional impairment is often profound, characterized by a progressive inability to perform activities of daily living (ADLs), such as donning shoes and socks, negotiating stairs, or ambulating beyond household distances.
Secondary indications encompass a broad spectrum of structural and systemic pathologies that culminate in articular destruction. Osteonecrosis (avascular necrosis) of the femoral head, often secondary to high-dose corticosteroid therapy, chronic alcohol abuse, or trauma, is a frequent indication in younger demographics, particularly when the disease has progressed to subchondral collapse (Ficat Stage III or IV). Developmental dysplasia of the hip (DDH) presents unique reconstructive challenges, often requiring concomitant structural bone grafting of the acetabulum or subtrochanteric shortening osteotomies of the femur. Inflammatory arthropathies, including rheumatoid arthritis and ankylosing spondylitis, frequently necessitate bilateral interventions and are complicated by systemic immunosuppression and poor bone stock. Furthermore, displaced femoral neck fractures in the physiologically active, independently ambulating elderly patient are increasingly treated with THA rather than hemiarthroplasty, as robust literature demonstrates superior functional outcomes and lower long-term revision rates.
Despite its high success rate, THA is not universally applicable, and strict adherence to established contraindications is vital for preventing catastrophic failures. Absolute contraindications are non-negotiable barriers to surgery. The presence of an active local or systemic infection (e.g., bacteremia, active urinary tract infection, or overlying cellulitis) absolutely precludes the implantation of hardware due to the extreme risk of periprosthetic joint infection (PJI). Severe, unoptimized medical comorbidities, such as unstable angina, recent myocardial infarction (within 6 months), or severe medically refractory heart failure, pose prohibitive anesthetic risks. Additionally, a completely neuropathic joint (Charcot arthropathy) or a profound absence of functional abductor musculature (without the possibility of utilizing constrained or dual-mobility components) are absolute contraindications due to the near certainty of postoperative instability and dislocation.
Relative contraindications require nuanced clinical judgment and extensive preoperative optimization. Morbid obesity (BMI > 40, and particularly > 50) is strongly correlated with increased rates of infection, wound complications, and early implant failure; many surgeons mandate weight loss prior to elective intervention. Severe osteoporosis does not preclude THA but heavily dictates the choice of fixation, mandating cemented femoral stems to prevent intraoperative periprosthetic fractures or postoperative subsidence. Active smoking and poor dentition are significant modifiable risk factors for wound healing complications and hematogenous seeding, respectively, and should be aggressively managed with cessation programs and dental clearance prior to surgical scheduling.
| Category | Specific Condition | Rationale / Surgical Implication |
|---|---|---|
| Absolute Indications | End-stage OA with failed conservative tx | Restoration of function and pain relief. |
| Absolute Indications | Ficat Stage III/IV Avascular Necrosis | Subchondral collapse cannot be salvaged natively. |
| Absolute Contraindications | Active local or systemic infection | Extreme risk of Periprosthetic Joint Infection (PJI). |
| Absolute Contraindications | Severe, unstable medical comorbidities | Prohibitive intraoperative mortality risk. |
| Absolute Contraindications | Neuropathic (Charcot) joint | Guaranteed early mechanical failure and dislocation. |
| Relative Contraindications | Morbid Obesity (BMI > 40) | Elevated risk of infection, DVT, and mechanical failure. |
| Relative Contraindications | Active Tobacco Use | Impaired wound healing and compromised osseointegration. |
| Relative Contraindications | Severe Osteoporosis | Dictates the necessity of cemented femoral fixation. |
Pre-Operative Planning, Templating, and Patient Positioning
The foundation of a successful Total Hip Arthroplasty (THA) is laid long before the first incision. Meticulous preoperative templating is mandatory to anticipate the optimal size of the components, restore the anatomic center of rotation, equalize leg lengths, and re-establish femoral offset. Failure to accurately template can lead to intraoperative compromises, resulting in altered biomechanics, instability, or accelerated polyethylene wear. Modern templating has largely transitioned from acetate overlays to sophisticated digital software, but the underlying biomechanical principles remain identical. The surgeon must synthesize the patient's clinical examination—specifically the apparent and true leg length discrepancy (LLD)—with high-quality radiographic imaging to formulate a precise, reproducible surgical blueprint.
Clinical Pearl: Always template both the affected and the contralateral normal hip. The contralateral hip often provides a more accurate representation of the patient’s native center of rotation and offset, especially in cases of severe degenerative dysplasia or protrusio acetabuli.
Radiographic Assessment
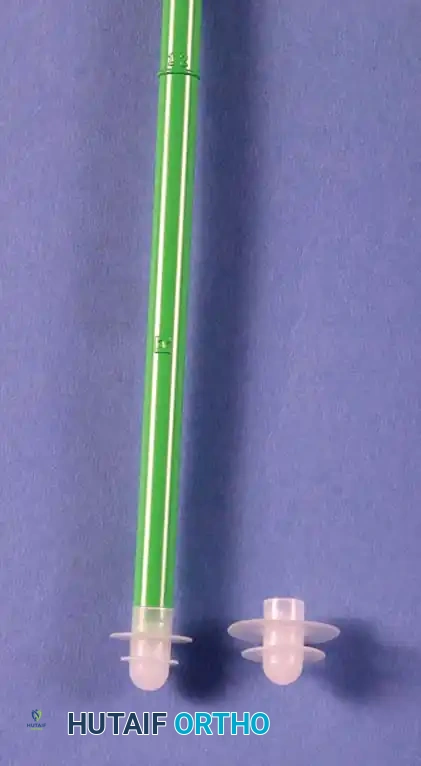
Standard preoperative radiographs must include an anteroposterior (AP) view of the pelvis centered over the pubic symphysis (with the hips internally rotated 15 degrees to profile the femoral neck) and a lateral view of the affected hip. A magnification marker, typically a 25mm metallic sphere, must be positioned at the level of the greater trochanter to allow digital software to calibrate the image accurately, usually adjusting for the standard 15% to 20% magnification inherent in pelvic radiography.
Step-by-Step Templating Process:
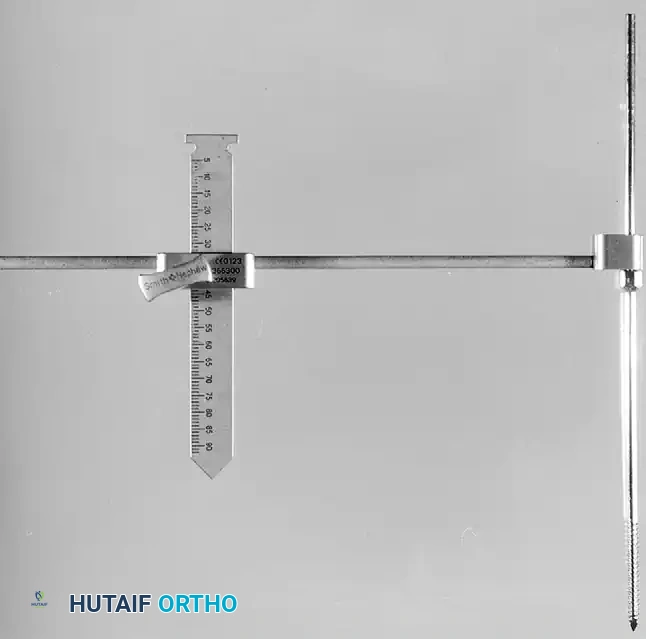
1. Determine Leg Length Discrepancy: A horizontal reference line is drawn across the bottom of the radiographic teardrops or the ischial tuberosities. The difference in the perpendicular distance from this line to a reproducible landmark on the proximal femur (usually the lesser trochanter) approximates the amount of limb shortening.
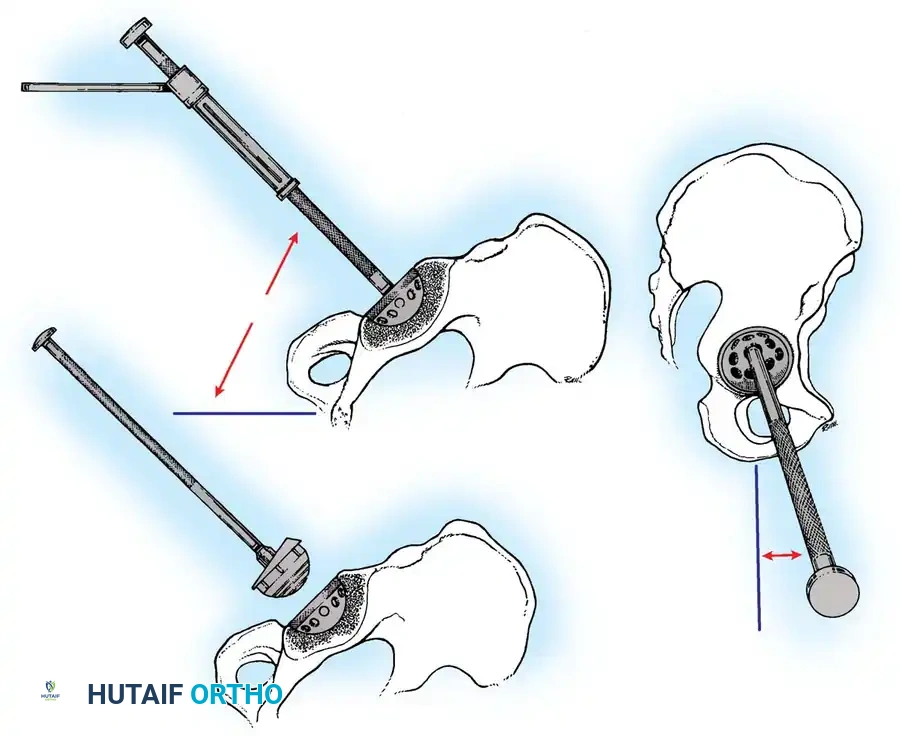
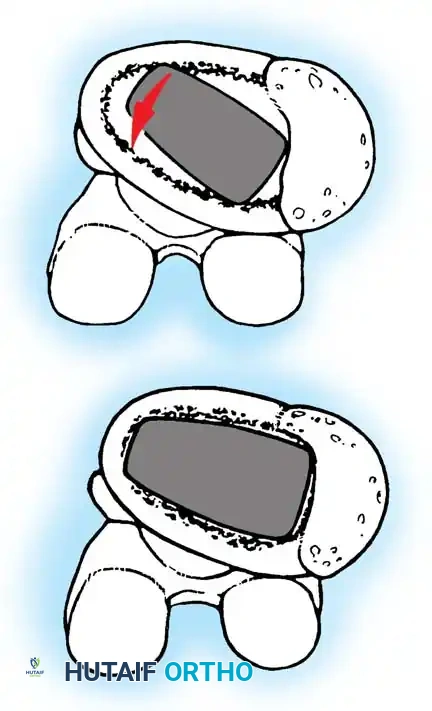
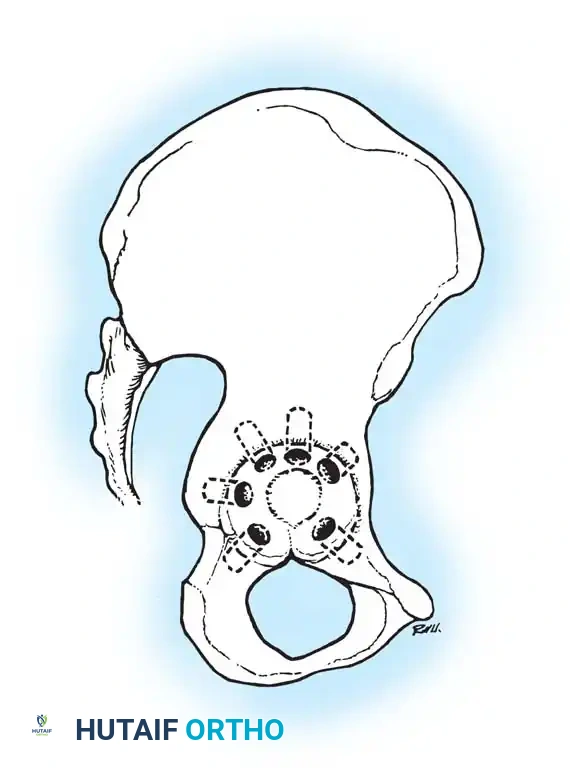
2. Acetabular Templating: The acetabular template is positioned at a 40- to 45-degree angle of inclination. It should correspond closely to the subchondral bone plate, ensuring adequate lateral coverage and medialization to the true floor (ilioischial line). The new center of rotation is marked.
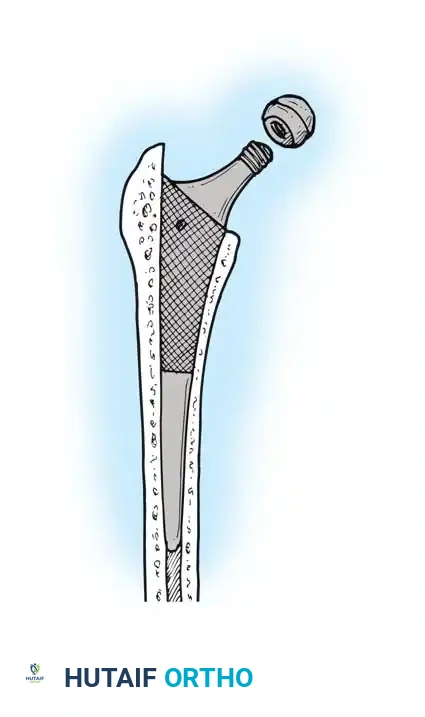
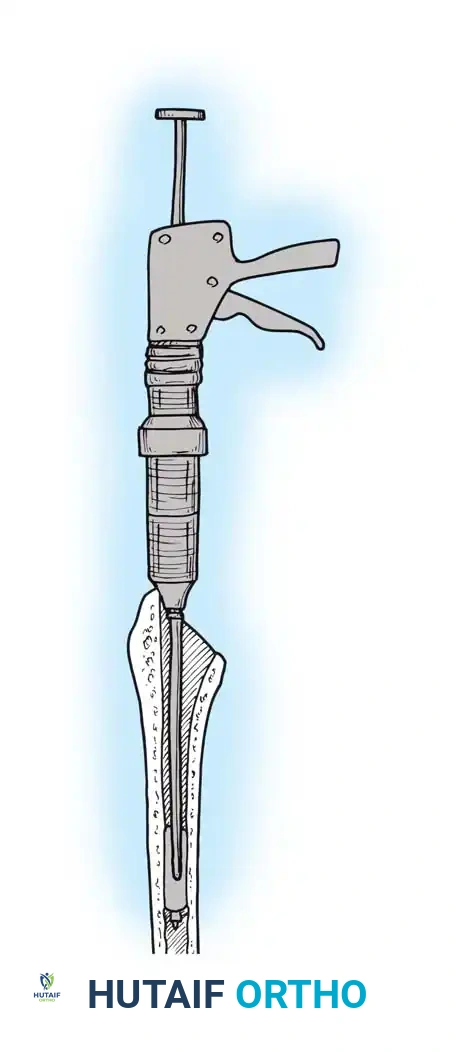
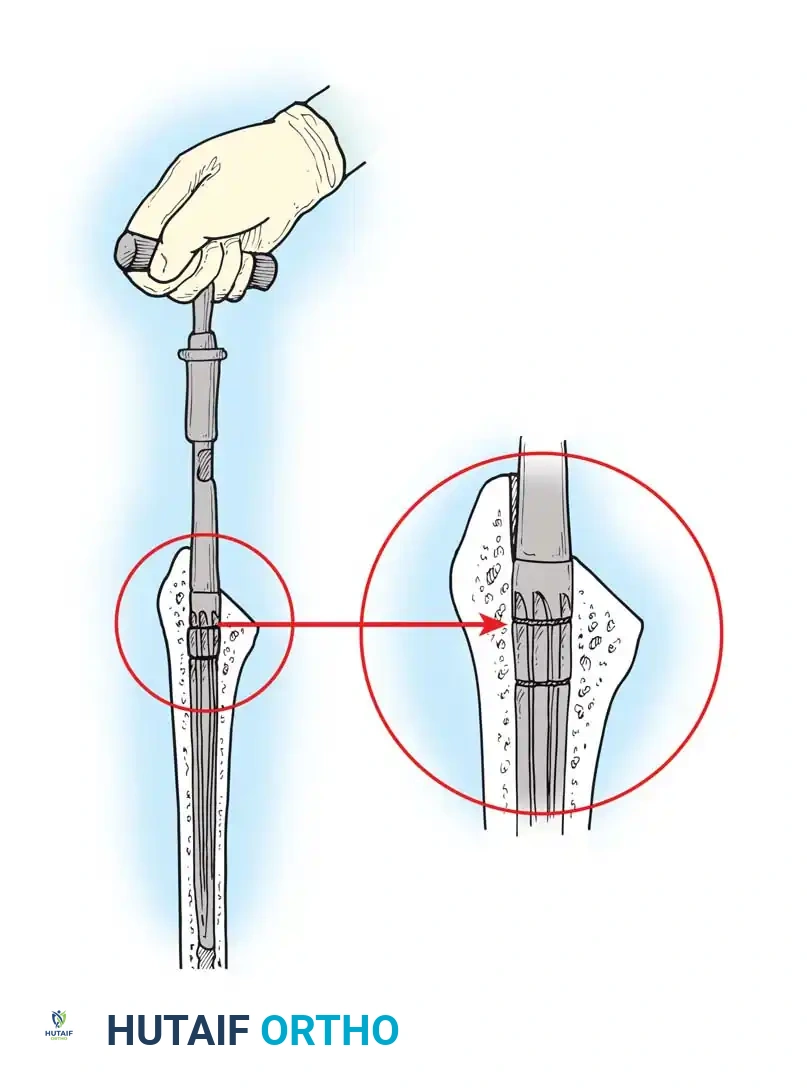
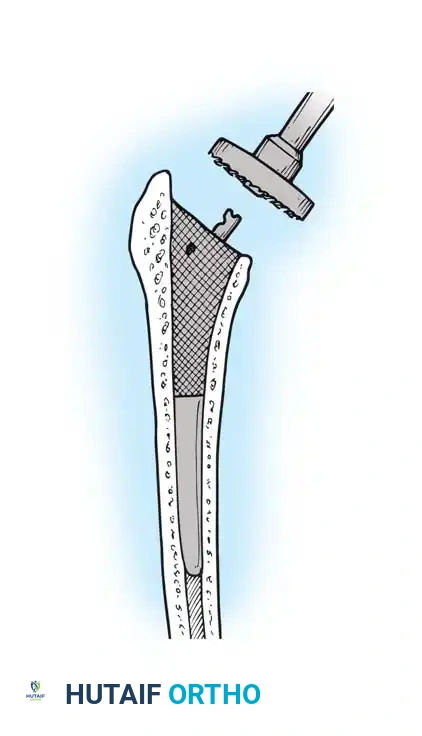
3. Femoral Templating: The femoral template that most closely matches the proximal and distal size and contour of the femoral metaphysis and diaphysis is selected. The surgeon must decide between a standard or high-offset stem to optimize abductor tension without inadvertently lengthening the limb.
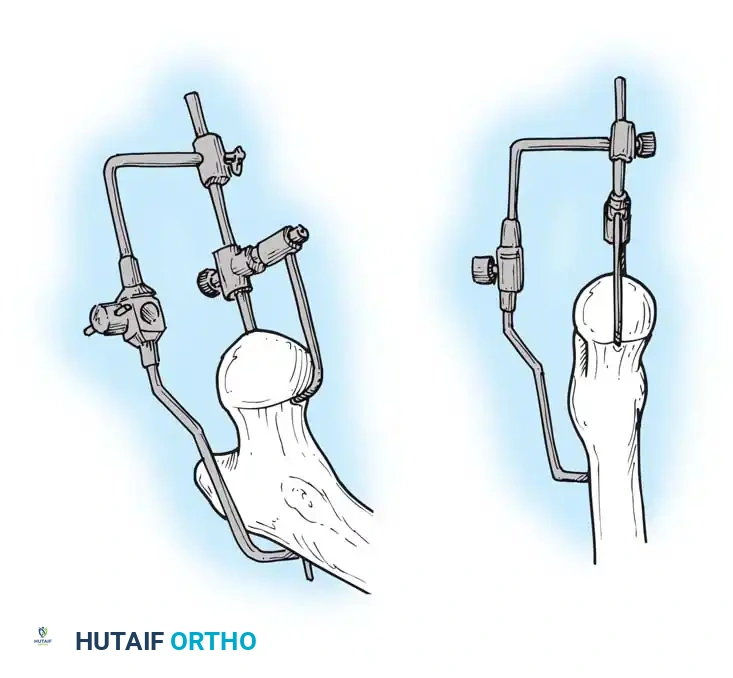
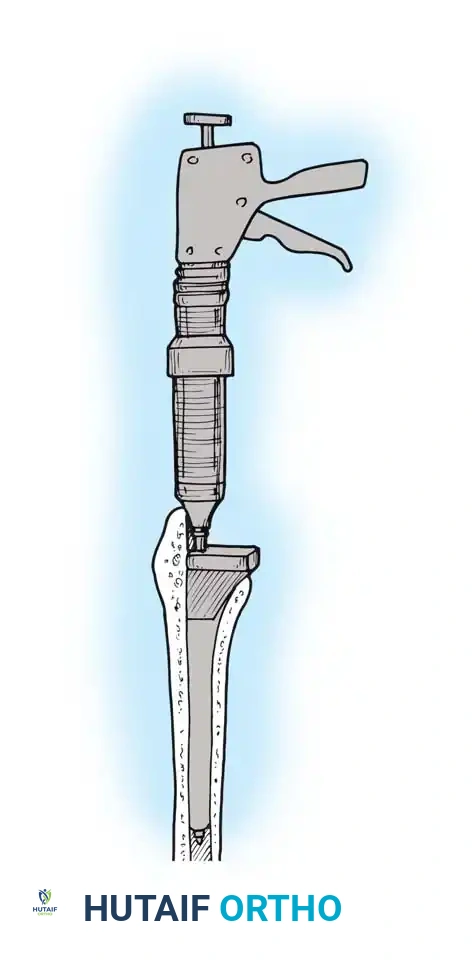
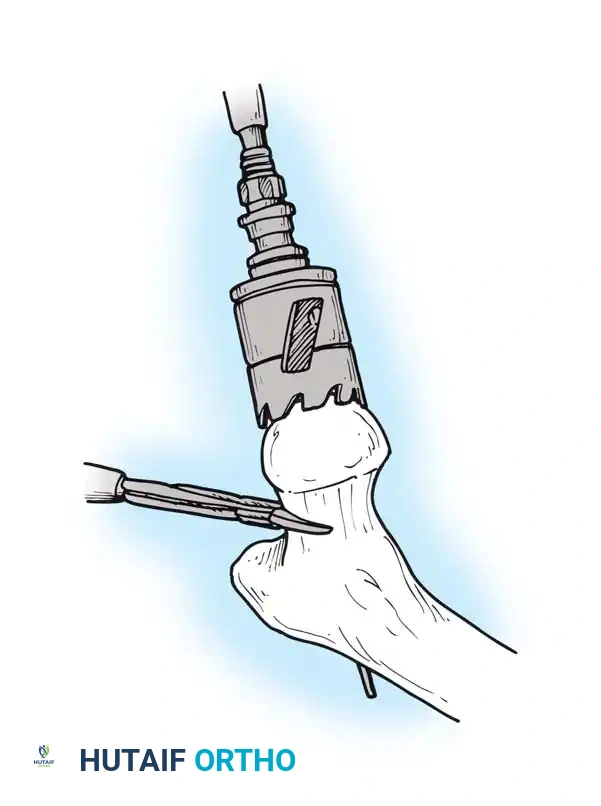
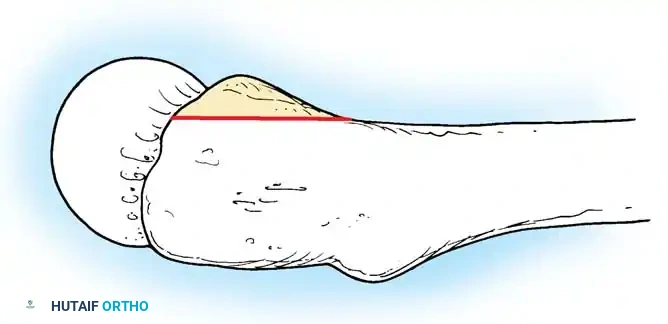
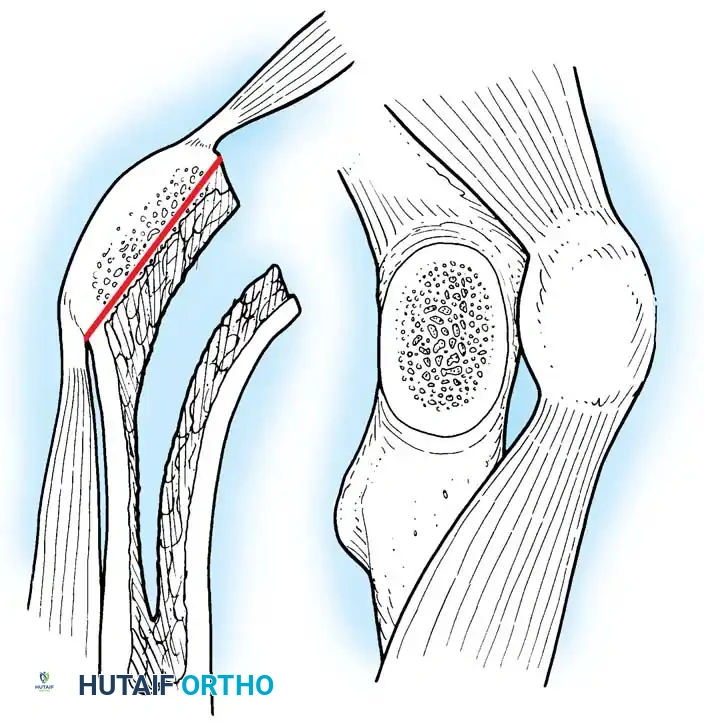
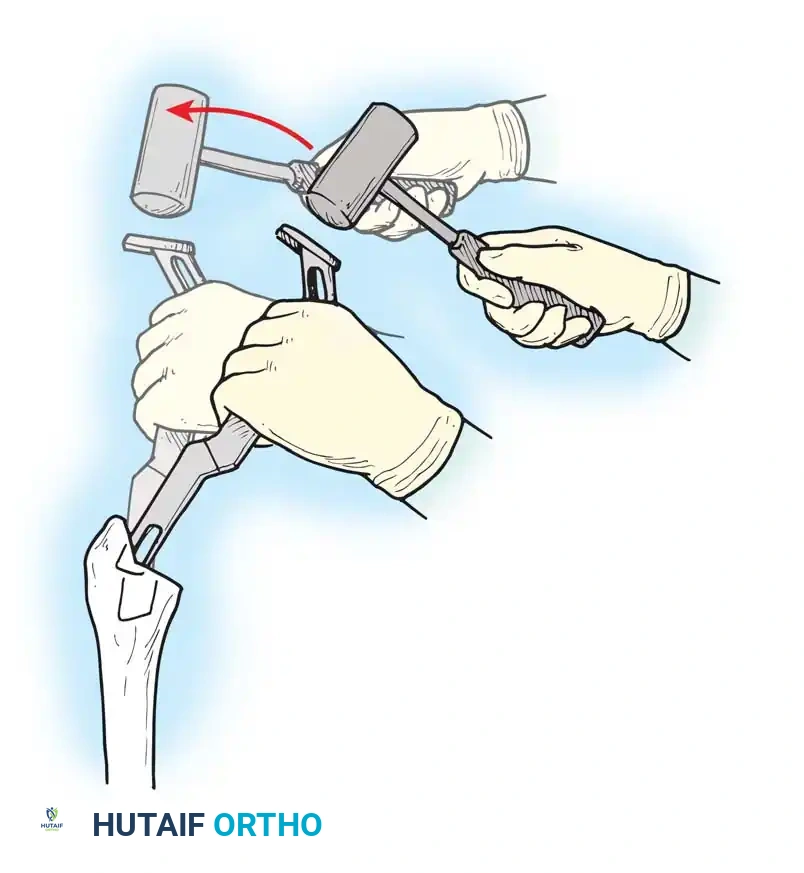
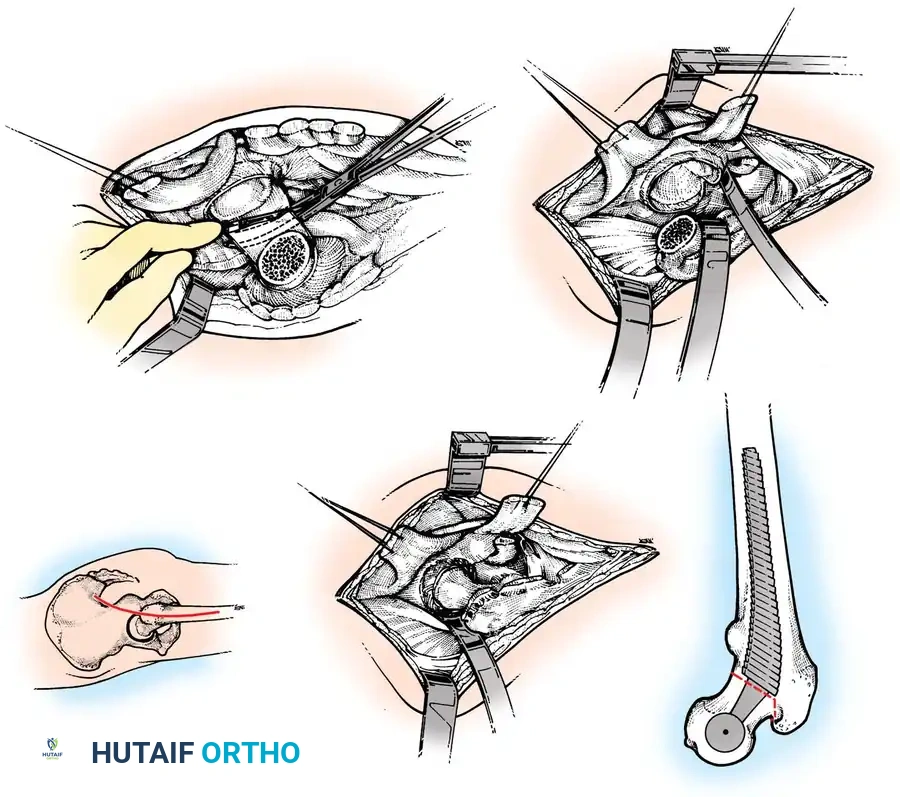
4. Neck Length and Offset: The neck length and offset are estimated to restore the abductor moment arm. The anticipated level of the femoral neck resection is marked relative to the lesser trochanter, providing a critical intraoperative landmark for the initial osteotomy.

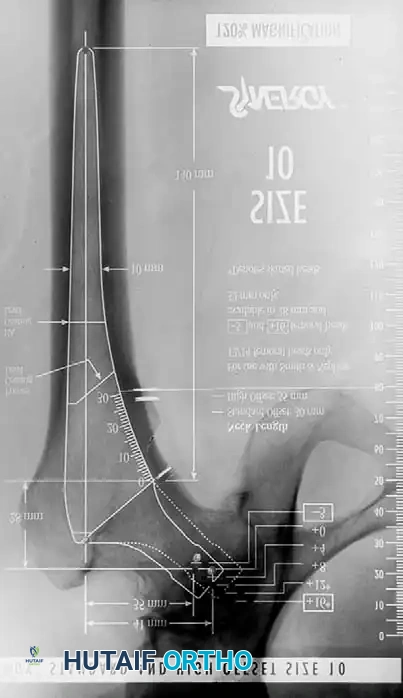


Advanced templating systems, such as the Synergy system, allow for precise calculation of standard versus high-offset stems to fine-tune soft-tissue tension. Intraoperative and postoperative radiographs should confirm that the completed arthroplasty corresponds to the preoperative plan, with implants properly sized and leg length/offset correctly restored.



Positioning Devices and Padding
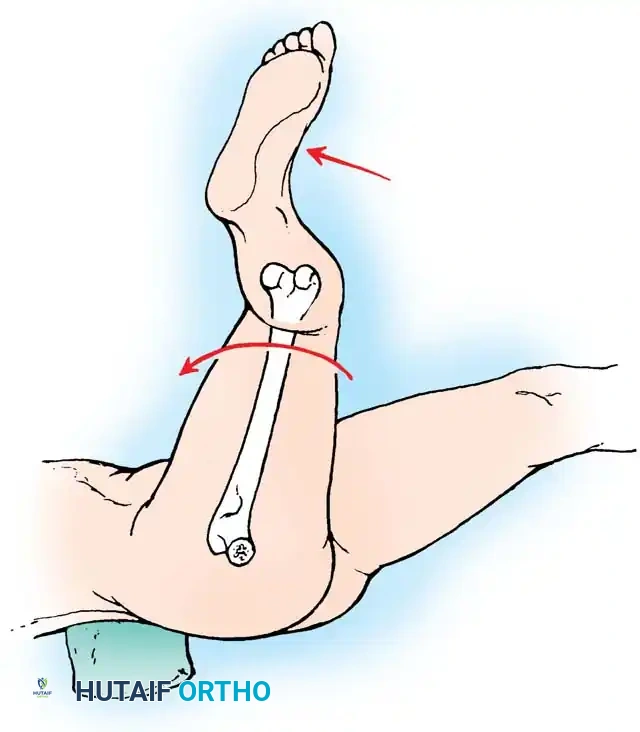
Proper patient positioning is critical. An operating table that tilts easily is highly recommended, especially when the patient is placed in the lateral decubitus position for a posterolateral or direct lateral approach. If the patient is not anchored securely, the pelvis may roll during the procedure, making the proper determination of acetabular component version and inclination exceedingly difficult, leading to malpositioning and subsequent instability.
A variety of pelvic positioning devices (peg boards, clamp positioners) are commercially available. Positioning devices must be placed securely against the pubic symphysis anteriorly and the sacrum posteriorly. They must not impede the motion of the hip intraoperatively, or assessing stability and impingement will be compromised. Anterior supports should be placed against the anterior superior iliac spines (ASIS) or pubic symphysis so that no pressure is applied over the femoral triangles. Compression here can result in catastrophic limb ischemia or femoral nerve neuropathy. Suction-deflated beanbags can be used, though dedicated rigid hip positioning devices are generally more secure for heavy or obese patients. All bony prominences and the dependent peroneal nerve (at the fibular head) must be meticulously padded, especially if a lengthy primary or revision procedure is expected.
If the patient is to be operated on in the supine position (e.g., for a direct anterior approach), a small pad is placed beneath the buttock of the affected hip. This is especially helpful in obese patients, as it allows loose adipose tissue to drop away from the incision site, facilitating exposure. A specialized fracture table or a standard table with a sterile leg-holder can be utilized to facilitate femoral elevation and exposure during the anterior approach.
Draping Protocol
Strict aseptic technique is paramount to mitigate the devastating complication of periprosthetic joint infection. The adhesive edges of a U-shaped plastic drape are applied to the skin to seal off the perineal and gluteal areas. The hip and entire limb are prepared with a suitable bactericidal solution (e.g., Chlorhexidine-alcohol), ensuring adequate drying time to maximize antimicrobial efficacy and prevent operating room fires. The foot is preferably covered with an impervious stockinette and secured with self-adherent wrap.
Final drapes must be of an impervious material to allow abundant pulsatile irrigation without fear of strike-through contamination. If anterior dislocation of the hip is anticipated while the patient is in the lateral position, utilize a draping system that incorporates a sterile pocket suspended across the anterior side of the operating table. This allows the leg to be placed safely in the bag while the femur is being prepared, preventing contamination from non-sterile table components.
Step-by-Step Surgical Approach and Fixation Technique
Many variations have evolved in the surgical approaches used for THA. The choice of a specific surgical approach is largely a matter of the surgeon's personal preference, training, and the specific anatomical challenges of the patient. Virtually all modern total hip femoral and acetabular components can be properly implanted through numerous approaches, provided adequate exposure is obtained without compromising the neurovascular structures or irreparably damaging the dynamic muscular stabilizers.
1. Anterolateral and Direct Lateral Approaches
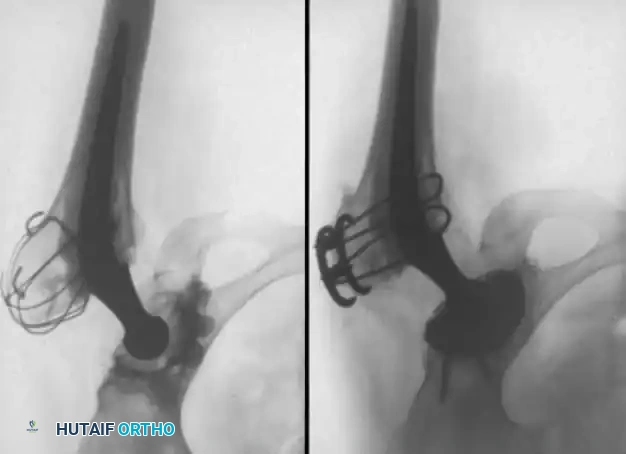
The Anterolateral Approach (e.g., Watson-Jones) exploits the internervous plane between the tensor fasciae latae (superior gluteal nerve) and the gluteus medius (superior gluteal nerve)—though technically an intermuscular rather than true internervous plane, it provides excellent access to the anterior capsule. Historically, Charnley utilized a variation of this with a routine trochanteric osteotomy, which is now largely abandoned due to high rates of trochanteric nonunion and wire breakage.
The Direct Lateral Approach (Hardinge) is performed supine or lateral. It is a muscle-splitting incision through the anterior third of the gluteus medius and minimus, allowing anterior dislocation and affording excellent acetabular exposure. The primary drawback is residual abductor weakness and a postoperative Trendelenburg limp, which can occur due to avulsion of the repaired anterior abductors or direct iatrogenic injury to the superior gluteal nerve if the split extends greater than 5 cm proximal to the greater trochanter. The Dall variation involves removal of the anterior portion of the abductors with an attached thin wafer of bone from the anterior edge of the greater trochanter, yielding superior bony healing and abductor function compared to soft-tissue repair alone.
2. The Posterolateral Approach: Soft Tissue Dissection
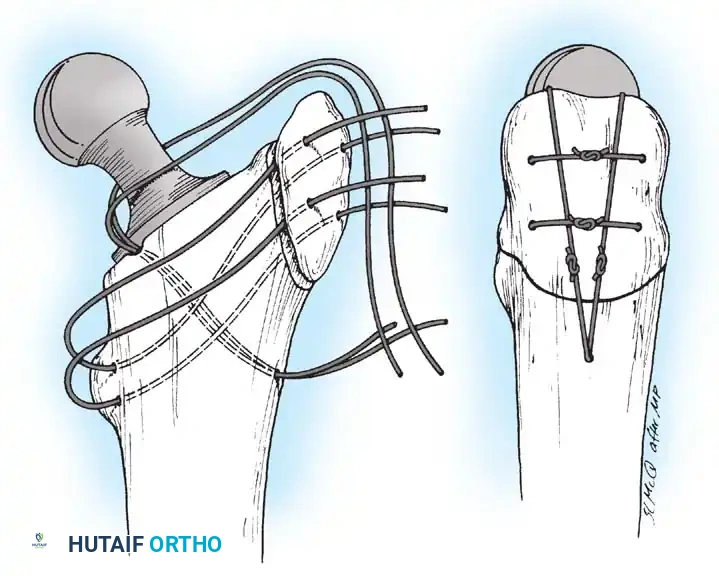
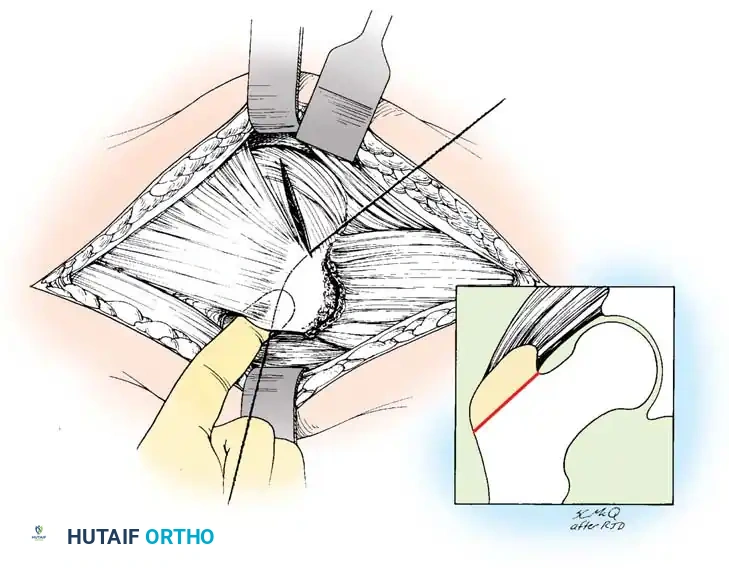
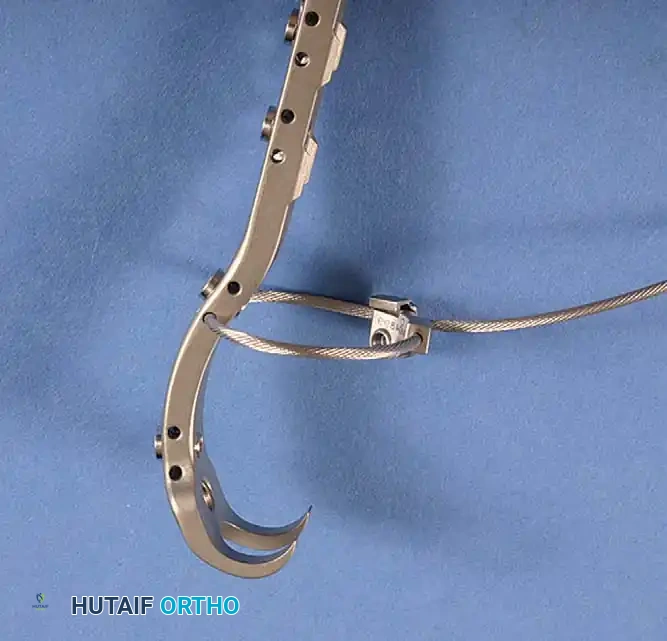
The posterolateral approach, with posterior dislocation of the hip, requires the lateral decubitus position. It is the most commonly utilized approach globally. It does not require routine osteotomy of the greater trochanter, thereby preserving the abductor mechanism entirely. While historically associated with a higher postoperative dislocation rate, modern enhanced posterior soft-tissue repair techniques (repairing the capsule and short external rotators back to the greater trochanter via transosseous tunnels) have reduced this risk to levels comparable with anterior and lateral approaches.
With the patient firmly anchored in the straight lateral position, make a slightly curved incision centered over the greater trochanter. Begin proximally at a point level with the ASIS along a line parallel to the posterior edge of the greater trochanter. Extend distally to the center of the trochanter and along the femoral shaft for approximately 10 cm. Adequate proximal extension is required for straight-line reaming of the femoral canal; distal extension is needed for unhindered acetabular preparation.
Divide the subcutaneous tissues in a single plane down to the fascia lata and the thin fascia covering the gluteus maximus. Dissect the subcutaneous tissues from the fascial plane for ~1 cm anteriorly and posteriorly to facilitate closure. Divide the fascia lata in line with the skin wound over the center of the greater trochanter. Bluntly split the gluteus maximus proximally in the direction of its fibers. Coagulate
Clinical & Radiographic Imaging Archive