Primary Uncemented Total Hip Arthroplasty: A Case Study Title

Key Takeaway
This topic focuses on Primary Uncemented Total Hip Arthroplasty: A Case Study Title, The **case title uncemented** primary total hip arthroplasty addresses severe right hip osteoarthritis in a 61-year-old female. This procedure utilizes an extensively porous-coated femoral stem to achieve immediate diaphyseal cortical fixation without cement. This implant choice offers high long-term survivorship, providing a durable solution for debilitating hip pain when non-surgical treatments are exhausted.
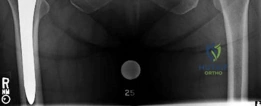
A 61-year-old female presents with a one-year history of worsening right groin pain, limiting ADLs. BMI is 34.1. Clinical examination shows a flexion contracture, limited internal rotation, and an abductor lurch. Here are her pelvic radiographs:

Describe your radiographic findings and explain the pathophysiology behind the groin pain in the context of this presentation.
Candidate: The X-ray shows end-stage osteoarthritis with loss of joint space, sclerosis, and osteophytes. The groin pain is due to the cartilage wear, and the limited ROM is caused by the bone spurs and capsule tightness.
Failure to use formal terminology (e.g., Kellgren-Lawrence grade). Missing the mechanical causes of pain like subchondral cysts (geodes) or the specific clinical link to the obturator/femoral nerve referral patterns. Candidates often describe findings randomly without a systematic approach (e.g., bone, joint, soft tissue).
Systematically address: 1. Radiographic findings: Kellgren-Lawrence Grade IV change; superior/axial joint space obliteration, subchondral sclerosis, large marginal osteophytes (femoral head-neck and acetabular rim), and subchondral geodes. 2. Pathophysiology: The pain is intra-articular, referred via the obturator and femoral nerves. 3. Clinical correlation: Loss of internal rotation is the earliest and most sensitive sign of capsular contracture and anterior osteophytic impingement. The abductor lurch is a biomechanical compensation to decrease the joint reactive force (JRF) by shifting the center of gravity closer to the hip's center of rotation.
You decide to proceed with a Total Hip Arthroplasty (THA). You have templated for an extensively porous-coated AML stem. What are the biomechanical principles and potential long-term complications of using this specific implant design?
Candidate: The AML stem uses an interference fit at the diaphysis for fixation. It's good for long-term hold, but it can cause stress shielding because the stem is stiff and doesn't load the proximal bone.
Missing the mention of the modulus of elasticity mismatch and the technical prerequisite of "cylindrical reaming." Failing to define the biologic process—that the "scratch fit" achieves initial mechanical stability required for secondary osteointegration.
Principles: Emphasize achieving rigid initial mechanical stability (micromotion < 150 microns) via diaphyseal "scratch fit" to allow for osteointegration into the porous coating. Complications: 1. Stress Shielding: Due to the high modulus of elasticity of the CoCr stem, the load is bypassed from the proximal femur (Wolff’s Law), leading to calcar resorption. 2. Thigh Pain: Caused by the stiffness mismatch and distal stress transfer. 3. Intraoperative Fracture: Risk of longitudinal split during impaction due to hoop stresses in the diaphysis.
Postoperatively, you are assessing the patient's recovery. Look at the follow-up radiograph below. What specific radiographic sign suggests that biological fixation is occurring, and what are the associated surgical risks during this specific implantation phase?

Candidate: I see bone bridging to the stem. This is called a spot weld. The risk is that if the surgeon reams too little, they might fracture the bone when putting the stem in.
Not clearly distinguishing between "initial mechanical stability" and "secondary biologic fixation." Failing to mention the concept of "hoop stress" and how surgeons mitigate this (e.g., cerclage wiring).
The sign is the "Spot Weld," where endosteal bone bridges directly to the porous coating, confirming osseointegration. Risk Mitigation: The primary intraoperative risk is a longitudinal femoral shaft fracture during stem impaction. This is caused by excessive hoop stress when the canal is under-reamed. Strategies to mitigate this include meticulous sequential reaming to the planned diameter and the use of prophylactic cerclage cabling in patients with Dorr Type A (narrow) femoral canals.
