Surgical Management of Specific Hip Disorders in Total Hip Arthroplasty
Key Takeaway
Total hip arthroplasty (THA) requires meticulous surgical modifications when addressing specific hip disorders. Osteoarthritis demands careful osteophyte resection and acetabular medialization. Rheumatoid arthritis presents challenges like osteopenia, cervical instability, and altered anatomy. Osteonecrosis requires complete removal of prior grafts, while protrusio acetabuli necessitates anatomic hip center restoration and medial wall grafting. Mastering these condition-specific nuances ensures optimal biomechanics, implant survivorship, and clinical outcomes in complex arthroplasty cases.
Comprehensive Introduction and Patho-Epidemiology
Extensive clinical data and biomechanical research have accumulated since the 1970s concerning the diverse pathologies for which total hip arthroplasty (THA) is indicated. While the fundamental principles of THA remain consistent—namely, the relief of pain and the restoration of a stable, functional articulation—routine surgical techniques must frequently be modified to address the unique pathoanatomy and biomechanical deficits associated with specific conditions. A nuanced understanding of these entities is mandatory for the reconstructive arthroplasty surgeon to optimize implant survivorship, restore joint kinematics, and minimize perioperative complications. The transition from a "one-size-fits-all" approach to a pathology-specific surgical strategy represents a hallmark of advanced arthroplasty practice.
Osteoarthritis (OA), whether primary (idiopathic) or secondary to previous trauma, dysplasia, or childhood hip disorders (e.g., Legg-Calvé-Perthes disease, Slipped Capital Femoral Epiphysis), remains the most common indication for total hip arthroplasty. The patho-epidemiology of primary OA involves a complex cascade of mechanical wear and biochemical degradation of articular cartilage, leading to subchondral sclerosis, eburnation, and the formation of massive marginal osteophytes. Secondary OA often presents with profound anatomic distortion; for instance, developmental dysplasia of the hip (DDH) results in a shallow, lateralized acetabulum and excessive femoral anteversion, requiring complex reconstructive strategies that deviate significantly from standard primary THA.

Inflammatory arthropathies, including rheumatoid arthritis (RA), juvenile idiopathic arthritis (JIA), psoriatic arthritis, and systemic lupus erythematosus (SLE), present a systemic patho-epidemiology characterized by aggressive synovial hypertrophy and enzymatic cartilage destruction. Unlike the hypertrophic bone formation seen in OA, inflammatory conditions are characterized by severe osteopenia, bony resorption, and profound soft tissue attenuation. The chronic use of corticosteroids and disease-modifying antirheumatic drugs (DMARDs) further compromises bone density and soft tissue healing capacity. The epidemiology of these conditions often dictates earlier surgical intervention, frequently in patients with bilateral disease and multi-joint involvement.
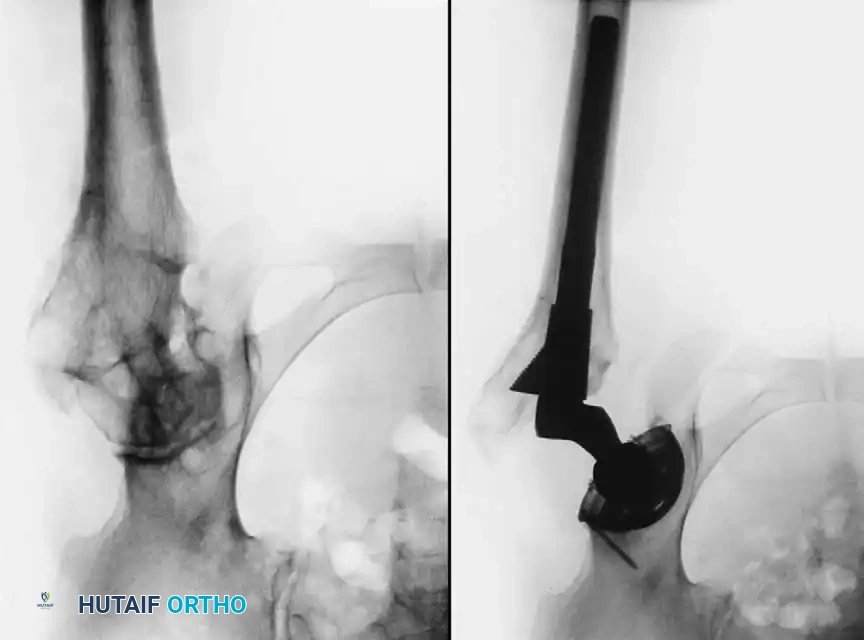
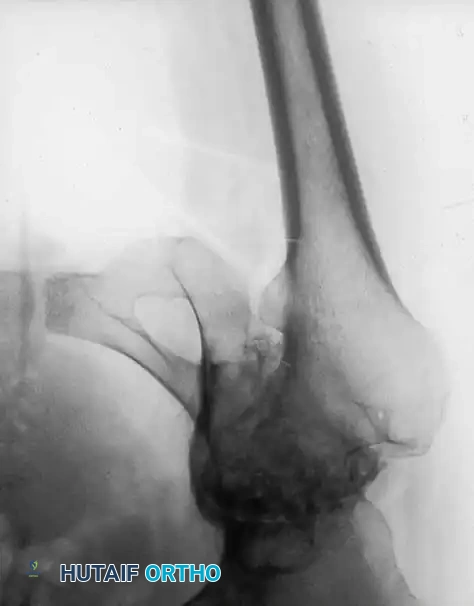
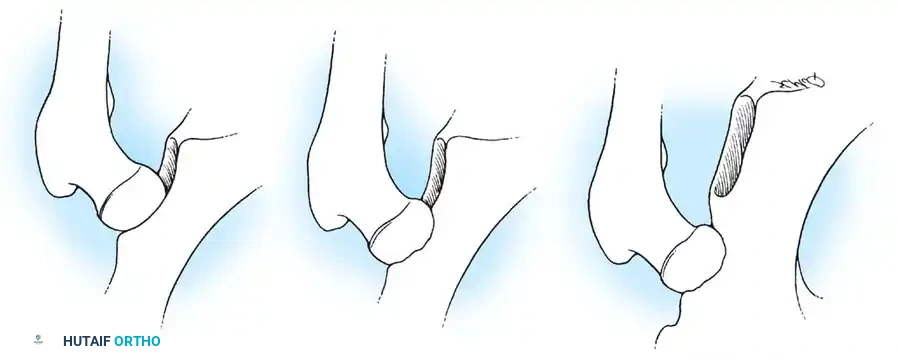
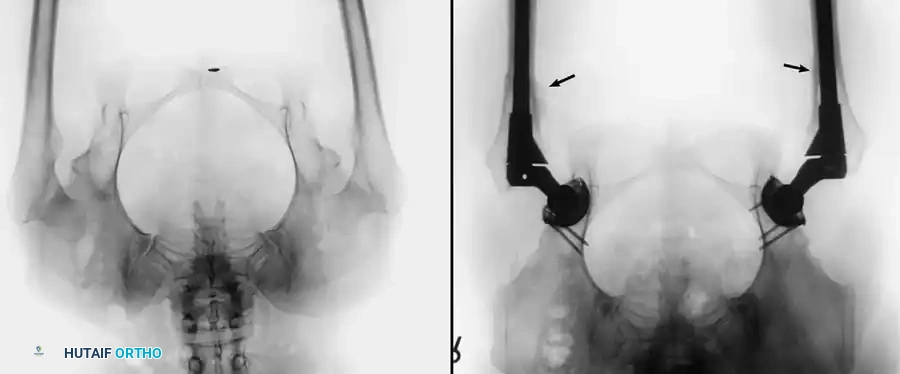
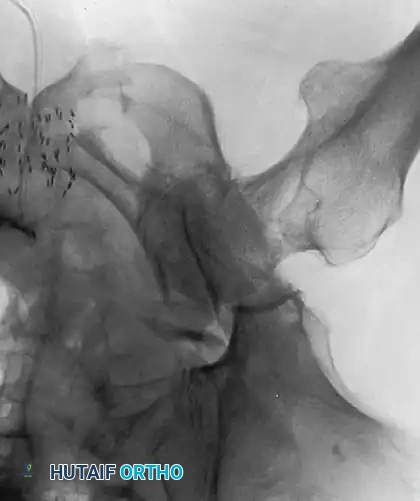
Osteonecrosis (avascular necrosis, AVN) and protrusio acetabuli represent distinct pathological entities with unique epidemiological profiles. Osteonecrosis predominantly affects younger patients and is frequently associated with systemic risk factors such as high-dose corticosteroid administration, alcohol abuse, sickle cell hemoglobinopathies, and coagulation disorders. The pathology is driven by an ischemic insult to the femoral head, leading to a necrotic wedge, subchondral collapse, and rapid secondary joint degeneration. Protrusio acetabuli, defined radiographically by the medial migration of the femoral head beyond the ilioischial (Kohler) line, can be primary (Otto pelvis) or secondary to inflammatory diseases, metabolic bone disorders, or trauma. The progressive medialization of the joint center severely alters pelvic biomechanics, demanding meticulous preoperative planning and specialized reconstructive techniques to prevent catastrophic medial wall failure.

Detailed Surgical Anatomy and Biomechanics
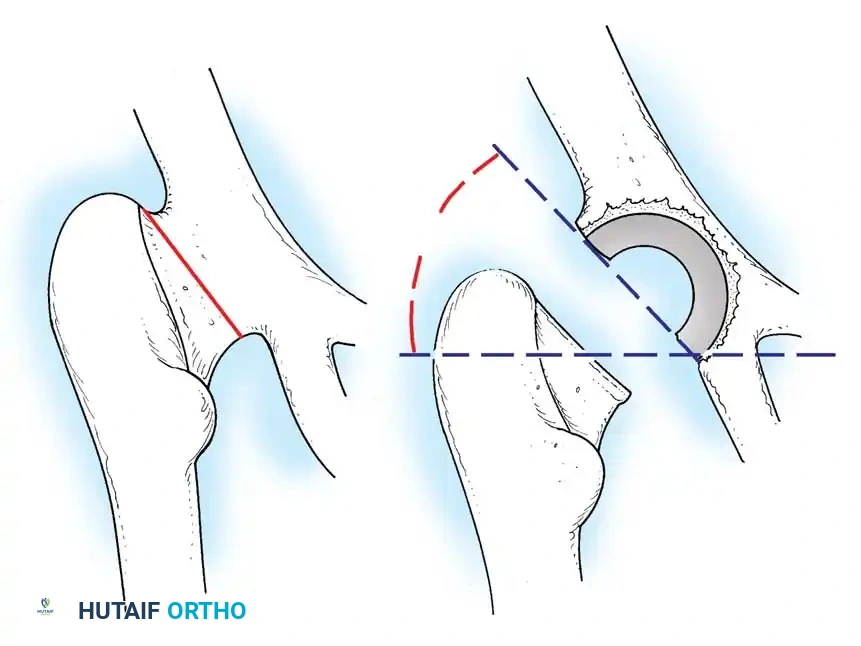
The successful execution of a total hip arthroplasty relies on the precise restoration of normal hip biomechanics, which requires an intimate understanding of the altered surgical anatomy presented by specific disease states. In a normal hip, the center of rotation (COR) is positioned to optimize the abductor moment arm while minimizing the joint reactive forces across the articulation. The femoral offset—the perpendicular distance from the center of the femoral head to the anatomical axis of the femur—must be restored to appropriately tension the abductor musculature (gluteus medius and minimus). Failure to restore offset results in abductor weakness, a positive Trendelenburg sign, and increased impingement risk.
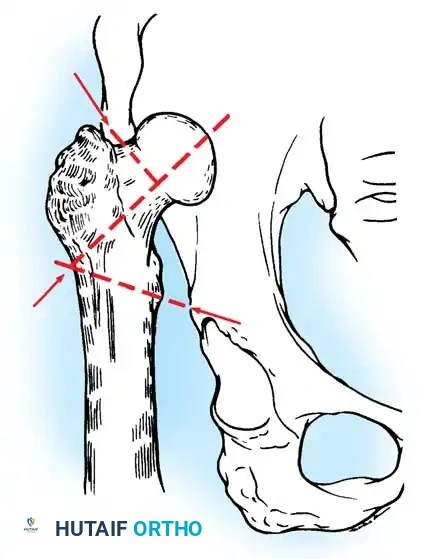
In the setting of advanced osteoarthritis, the surgical anatomy is frequently distorted by massive osteophytosis. Marginal osteophytes can completely tether the femur within the acetabulum, effectively locking the joint and increasing the risk of iatrogenic fracture during dislocation. Within the acetabulum, medial and inferior osteophytes may obliterate the cotyloid fossa (pulvinar), lateralizing the femoral head and creating a "false bottom." If the surgeon fails to recognize this altered anatomy and reams only to the false bottom, the acetabular component will be placed in an excessively lateralized and superior position. This lateralization shortens the abductor lever arm, exponentially increasing the joint reactive forces and predisposing the reconstruction to early mechanical failure and superior migration.
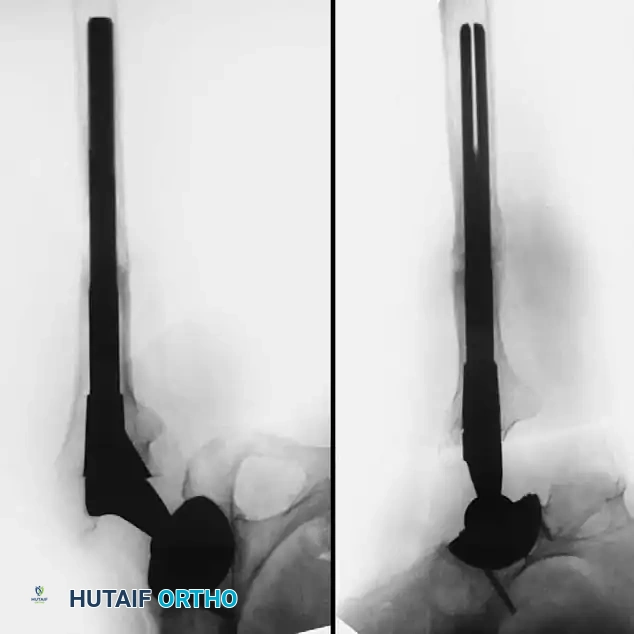
Conversely, inflammatory arthropathies and protrusio acetabuli present with a medialized center of rotation. In severe protrusio, the medial wall of the acetabulum is paper-thin or frankly deficient, and the femoral head may migrate deep into the true pelvis. Biomechanically, this medialization reduces the femoral offset and allows the greater trochanter to impinge against the ilium, severely restricting range of motion. The proximal femoral anatomy in inflammatory conditions is often categorized as Dorr Type C, characterized by a widened "stovepipe" medullary canal with extremely thin cortices. This lack of diaphyseal isthmus complicates the achievement of stable initial press-fit fixation with standard tapered wedge stems, often necessitating the use of fully porous-coated cylindrical stems or cemented fixation.

Osteonecrosis presents a unique anatomical challenge, particularly when patients have undergone prior joint-preserving procedures such as core decompression or vascularized fibular grafting. The femoral head anatomy is distorted by subchondral collapse, but more critically, the intramedullary canal may be obstructed by dense, sclerotic bone tracts or retained cortical grafts. The biomechanical integrity of the proximal femur is compromised by the necrotic segment, yet the surrounding bone may be highly reactive and sclerotic. Navigating this juxtaposition of necrotic, osteopenic, and sclerotic bone requires meticulous preparation to ensure that the femoral component achieves appropriate alignment and cortical contact without inducing a varus deformity or intraoperative fracture.
Exhaustive Indications and Contraindications
The decision to proceed with total hip arthroplasty must be carefully individualized, weighing the severity of the specific hip disorder against the patient's physiological age, functional demands, and medical comorbidities. In primary and secondary osteoarthritis, the primary indication remains intractable pain that is refractory to comprehensive non-operative management, including weight loss, activity modification, physical therapy, non-steroidal anti-inflammatory drugs (NSAIDs), and intra-articular injections. Radiographic evidence of joint space narrowing, subchondral sclerosis, and osteophytosis must correlate with the patient's clinical symptoms.
In inflammatory arthropathies, the indications for THA often arise earlier in the patient's life due to the aggressive nature of the disease. Pain, profound loss of mobility, and progressive deformity are the primary drivers for surgical intervention. However, the timing of surgery must be coordinated with the patient's rheumatologist to manage perioperative immunosuppression. In osteonecrosis, THA is indicated for Ficat Stage III (subchondral collapse/crescent sign) and Stage IV (secondary degenerative changes). While joint-preserving procedures may be attempted in Ficat Stages I and II, the presence of structural collapse invariably necessitates arthroplasty. For protrusio acetabuli, progressive medial migration threatening the integrity of the medial wall is an absolute indication for reconstruction before catastrophic intrapelvic visceral compromise occurs.
| Pathology | Primary Indications for THA | Specific Contraindications / Cautions |
|---|---|---|
| Osteoarthritis (OA) | Intractable pain, severe functional limitation, radiographic joint space exhaustion, failure of conservative therapy. | Active joint infection, severe neurotrophic arthropathy (Charcot joint), medically unstable patient. |
| Inflammatory Arthropathy (RA/JIA) | Progressive destructive arthropathy, profound loss of ROM, impending protrusio, unremitting pain. | Unstable cervical spine (absolute caution), active systemic flare, active untreated vasculitic ulcers. |
| Osteonecrosis (AVN) | Ficat Stage III (collapse) and IV (secondary OA), failure of core decompression or grafting. | Ficat Stage I/II in young patients (consider joint preservation first), active substance abuse compromising rehab. |
| Protrusio Acetabuli | Progressive medial migration past Kohler line, severe impingement, impending medial wall blowout. | Inadequate bone stock for rim fixation without appropriate structural allograft/cage availability. |
Absolute contraindications for THA across all specific hip disorders include active local or systemic infection, severe medical comorbidities precluding anesthesia (e.g., recent myocardial infarction, unstable angina), and neuropathic arthropathy, which carries an unacceptably high risk of early catastrophic loosening and instability. Relative contraindications include morbid obesity, severe peripheral vascular disease, and profound psychiatric or cognitive disorders that would prevent adherence to postoperative rehabilitation protocols. The surgeon must also carefully evaluate the patient's soft tissue envelope; poor skin quality, active vasculitic ulcers (common in RA), or previous massive irradiation to the pelvis significantly elevate the risk of postoperative infection and wound dehiscence.
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning and digital templating are non-negotiable steps in the surgical management of complex hip disorders. Accurate templating allows the surgeon to anticipate implant size, restore the center of rotation, correct leg length discrepancies (LLD), and identify potential intraoperative pitfalls. A standardized anteroposterior (AP) radiograph of the pelvis, centered over the pubic symphysis with the hips internally rotated 15 degrees (to profile the femoral neck), is mandatory. A lateral radiograph of the affected hip is also required to assess femoral version and anterior bowing, which is particularly relevant in juvenile idiopathic arthritis and post-traumatic deformities.

When templating for osteoarthritis, the surgeon must identify the true medial wall of the acetabulum, often obscured by medial osteophytes. The acetabular template should be positioned at the level of the radiographic teardrop, ensuring that the component will be medialized appropriately to restore the anatomic hip center. On the femoral side, the template is used to determine the level of the neck resection, the required stem size to achieve diaphyseal fit, and the appropriate offset option (standard vs. high offset) to restore the abductor lever arm. The surgeon must also anticipate the need to resect massive overhanging trochanteric osteophytes to prevent extra-articular impingement.
In patients with rheumatoid arthritis and protrusio acetabuli, templating focuses heavily on managing bone deficiency. For RA, the templating process must account for the Dorr Type C femoral canal, often requiring a larger, fully coated stem to achieve stability in osteopenic bone. For protrusio, the template must demonstrate how the hip center will be lateralized and inferiorized. The surgeon must plan for the use of a multi-hole acetabular shell to allow for supplementary screw fixation in the peripheral rim, and calculate the volume of cancellous bone graft required to reconstitute the medial wall defect. Furthermore, in RA patients, preoperative flexion and extension cervical radiographs are mandatory to rule out atlantoaxial subluxation or subaxial instability, which could lead to catastrophic spinal cord injury during intubation.
Patient positioning depends on the surgeon's preferred approach (e.g., posterior, direct anterior, anterolateral), but meticulous execution is critical regardless of the technique. In the lateral decubitus position, rigid pelvic fixation utilizing anterior and posterior supports is essential to prevent pelvic roll during the procedure. Unrecognized changes in pelvic tilt or rotation during surgery will lead to inaccurate assessment of acetabular version and inclination, predisposing the patient to instability and impingement. The operative leg must be draped free to allow for full assessment of range of motion, stability, and leg length comparison against the contralateral limb.
Step-by-Step Surgical Approach and Fixation Technique
The surgical approach to specific hip disorders requires a highly adaptable technique, prioritizing safe exposure, meticulous bone preparation, and rigid implant fixation. The following subsections detail the technical modifications required for distinct pathologies.
Osteoarthritis and Hypertrophic Degeneration
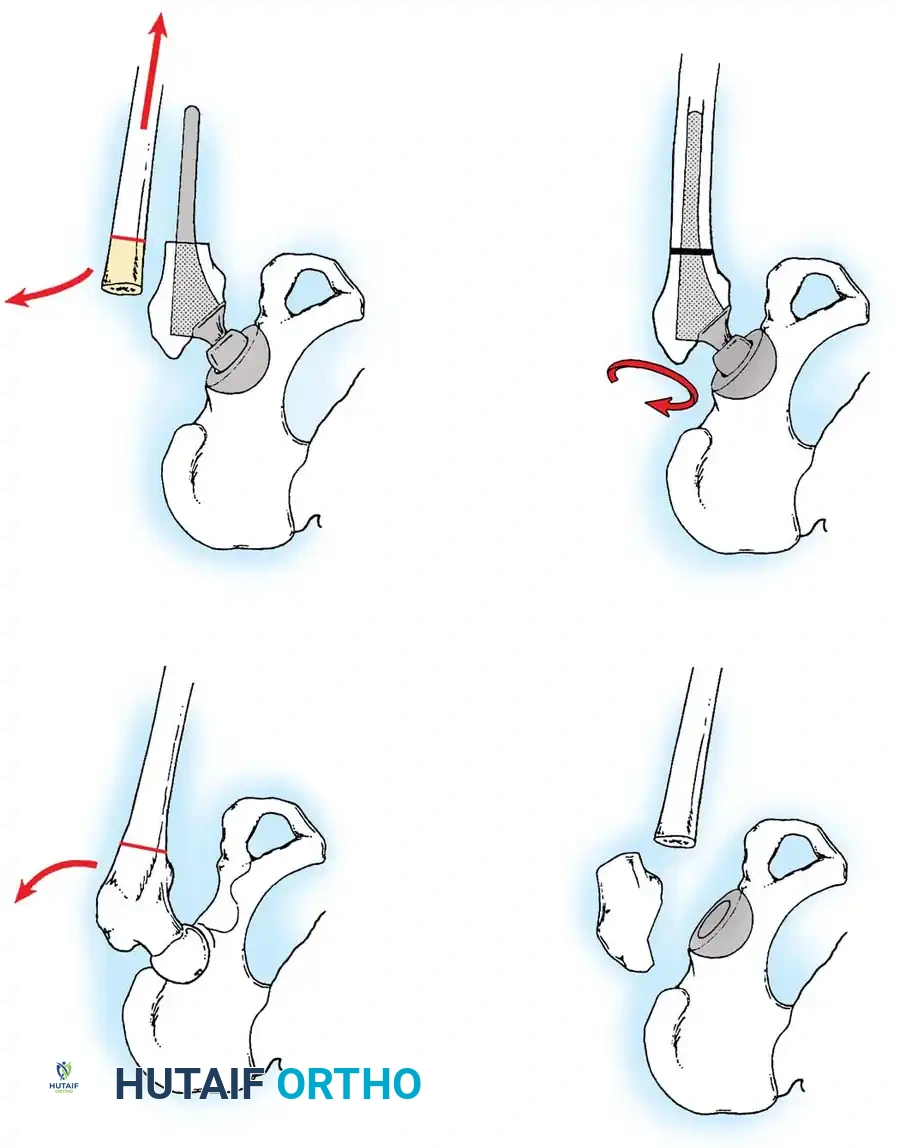
In advanced OA, safe dislocation of the hip is the first critical step. Massive marginal osteophytes often tether the femur within the acetabulum. The surgeon must never forcefully lever the femur to achieve dislocation, as this places the patient at high risk for iatrogenic femoral neck or shaft fractures. Instead, perform a meticulous in situ resection of the anterior and posterior acetabular osteophytes prior to attempting dislocation. In severe cases, an in situ femoral neck osteotomy—making the neck cut before dislocating the head—is the safest approach. Once the head is removed, acetabular preparation begins. The subchondral bone is characteristically thick, sclerotic, and eburnated. Considerable reaming with sharp, hemispherical reamers is required to bypass this sclerotic layer and reach a bleeding cancellous bed satisfactory for biologic bone ingrowth.

Osteophytes may completely obliterate the cotyloid fossa, creating a "false bottom." The surgeon must deepen the acetabulum to its true anatomic medial wall to fully contain the cup. Failure to medialize the acetabulum leaves the superior portion of the cup unsupported or resting on structurally inferior osteophytic bone. Furthermore, careful excision of all peripheral acetabular osteophytes is mandatory to prevent postoperative bony impingement. On the femoral side, the greater trochanter is often hypertrophied. Trimming the anterior or posterior overhang of the trochanter may be required to prevent extra-articular impingement during internal and external rotation, ensuring a stable, impingement-free range of motion.
Rheumatoid Arthritis and Osteopenic Bone
The surgical management of RA demands extreme caution due to profound osteopenia and soft tissue fragility. Special handling of the limb is paramount; the osteopenic bone is highly susceptible to iatrogenic fracture. Retractors must be placed with extreme care. Levering the femur anteriorly with a Hohmann retractor can easily fracture the anterior acetabular margin or the femoral neck. Acetabular preparation must be performed with gentle, sequential reaming, often stopping 1-2 mm short of the templated size to achieve a press-fit without blowing out the fragile medial wall. The use of a multi-hole acetabular shell is frequently indicated to allow for the placement of multiple supplementary screws, ensuring rigid initial fixation in poor bone stock.
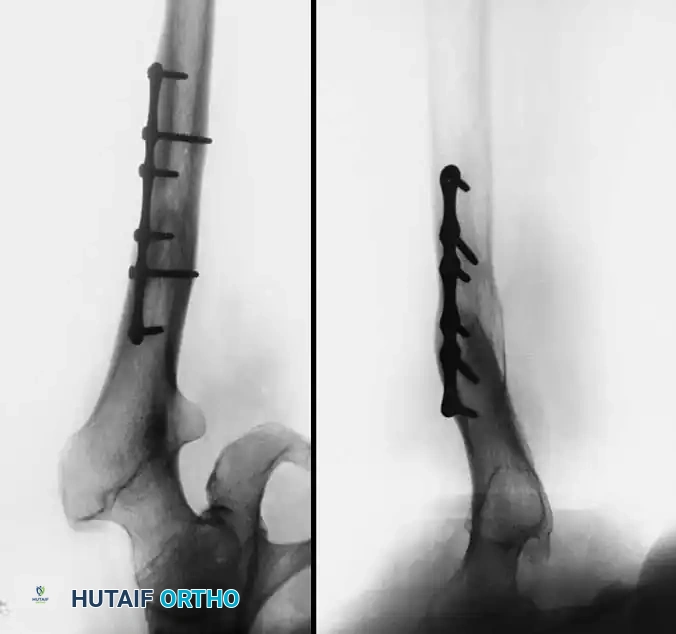
Femoral preparation in RA is usually straightforward due to the widened medullary canal, but the cortices are paper-thin and easily penetrated. The surgeon must maintain strict axial alignment during broaching to avoid cortical perforation or varus malalignment. While severe osteopenia historically favored cemented fixation, contemporary highly porous cementless components have shown excellent survivorship in RA patients, provided initial press-fit stability is achieved. In patients with JIA, excessive femoral anteversion and anterior bowing of the proximal femur are common, occasionally requiring a concomitant subtrochanteric derotational osteotomy or the use of modular, custom, or ultra-small components.

Osteonecrosis and Retained Hardware
Upon capsulotomy in a patient with osteonecrosis, the surgeon will often encounter a highly hyperemic capsule and profound synovial proliferation. Meticulous hemostasis using electrocautery is required to maintain visualization. A large synovial effusion is common and should not immediately be mistaken for infection, though routine intraoperative cultures are a prudent medicolegal and clinical step. The primary technical challenge arises if the patient has previously undergone a cortical bone grafting procedure (e.g., free or vascularized fibular graft).
The intramedullary portion of any retained graft must be completely excised. Conventional broaches will deflect off the hard cortical graft, leading to varus malpositioning, undersizing of the femoral component, or catastrophic proximal femur fracture. To safely remove prior grafts, the surgeon should utilize a high-speed burr and flexible reamers to clear the canal. Intraoperative fluoroscopy with the broach or reamer in place is highly recommended to ensure complete graft removal, proper axial alignment, and optimal cortical contact before final stem impaction.

Protrusio Acetabuli and Medial Wall Reconstruction
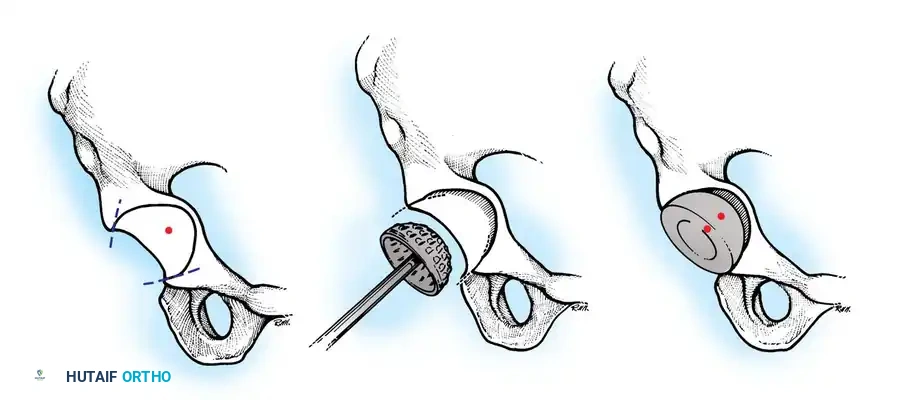
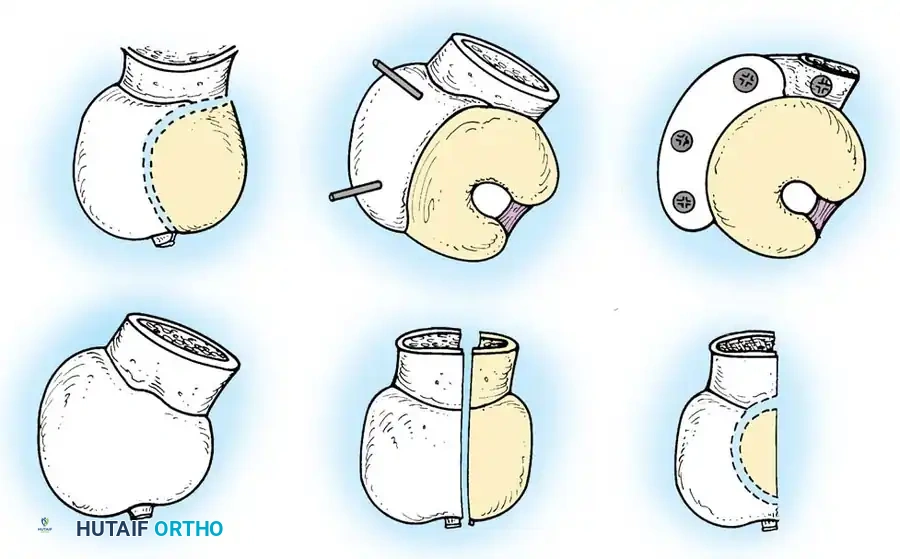
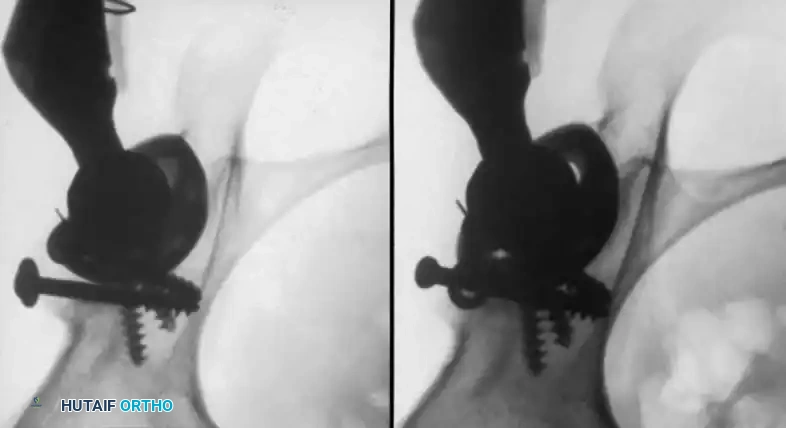
The surgical management of protrusio acetabuli relies on three non-negotiable biomechanical principles: restoration of the anatomic hip center, peripheral rim fixation, and medial wall reconstruction. The hip center of rotation must be lateralized and brought inferiorly to its true anatomic position to restore abductor mechanics. To achieve this, the acetabular implant must be supported by the intact, structurally sound peripheral rim of the acetabulum, completely bypassing the deficient medial wall.
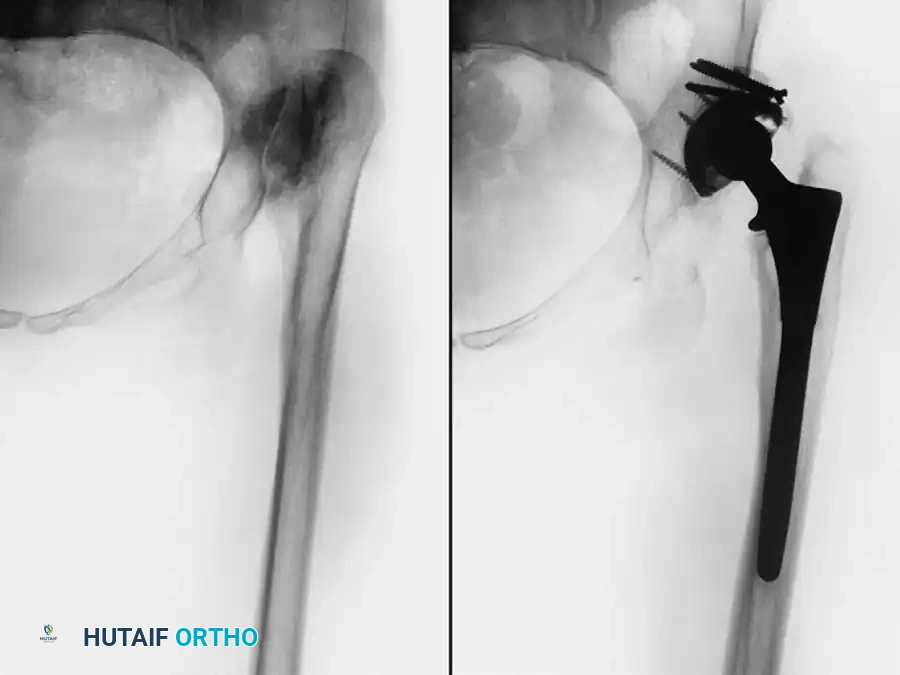
Cavitary and segmental defects of the medial wall must be reconstituted to prevent progressive medial migration of the new implant. This is typically achieved utilizing impaction bone grafting. The resected femoral head is meticulously morselized into cancellous chips. These chips are then densely impacted into the medial defect using reverse reamers or specialized impaction instruments. A highly porous, multi-hole hemispherical cup is then impacted into the peripheral rim, compressing the graft medially. Multiple screws are placed into the safe zones (posterosuperior quadrant) to ensure absolute stability of the shell while the medial graft incorporates.

Complications, Incidence Rates, and Salvage Management
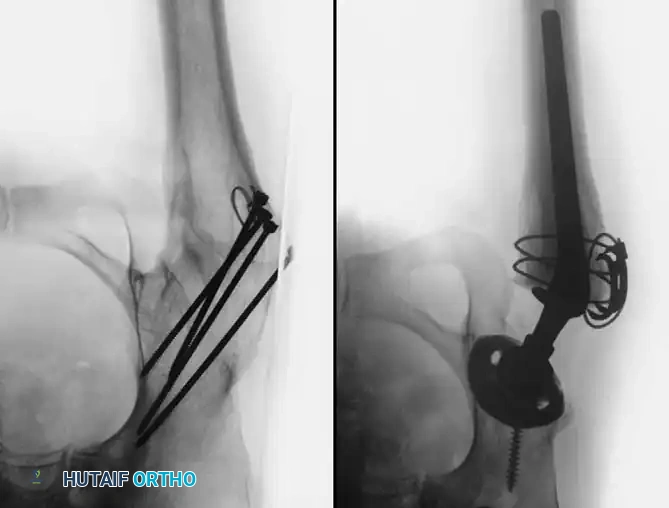
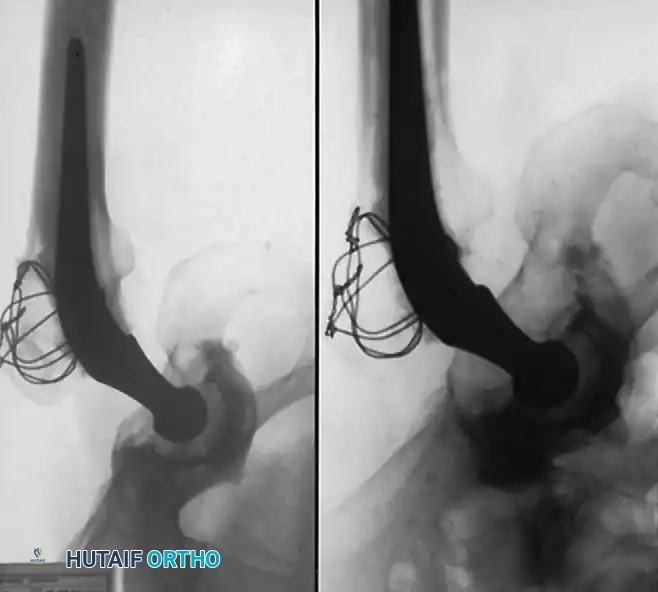
Despite meticulous surgical technique, total hip arthroplasty for specific complex disorders carries an inherently higher complication profile than routine primary THA. Intraoperative fractures are a significant risk, particularly in patients with RA (due to severe osteopenia) and advanced OA (due to massive osteophytes and altered anatomy). The incidence of intraoperative calcar fractures during cementless stem impaction can approach 3-5% in osteopenic cohorts. Salvage management requires immediate recognition; non-displaced calcar fissures can be managed with prophylactic cerclage wiring, while displaced fractures may necessitate the use of a diaphyseal-engaging long stem to bypass the defect.
Instability and dislocation remain critical concerns, particularly when the pathoanatomy has led to significant soft tissue contractures or when the center of rotation is inadequately restored. Failure to excise peripheral osteophytes in OA can cause bony impingement, levering the head out of the socket. In protrusio, failure to lateralize the hip center results in a lax abductor mechanism, dramatically increasing dislocation risk. Management of recurrent instability involves a thorough diagnostic workup to identify component malposition, followed by revision surgery to correct version, increase offset, or utilize dual-mobility bearings or constrained liners as salvage options.
Infection and wound healing complications are disproportionately higher in patients with inflammatory arthropathies. The chronic use of corticosteroids and DMARDs blunts the immune response and impairs fibroblast proliferation. The incidence of periprosthetic joint infection (PJI) in RA patients is reported to be 1.5 to 2 times higher than in the OA population. Salvage management of acute PJI involves aggressive debridement, antibiotics, and implant retention (DAIR) with modular exchange, whereas chronic infections mandate a two-stage revision protocol utilizing an antibiotic-eluting cement spacer.
| Complication | Incidence / High-Risk Cohort | Salvage Management Strategy |
|---|---|---|
| Intraoperative Fracture | 3-5% (RA, severe osteopenia, retained hardware in AVN). | Prophylactic/therapeutic cerclage wiring; bypass with diaphyseal-engaging long stem. |
| Instability / Dislocation | 2-4% (Altered offset, un-resected osteophytes, protrusio). | Revision for component malposition; utilize dual-mobility or constrained liners. |
| Periprosthetic Infection | 1.5-2.5% (RA, SLE, chronic steroid/DMARD use). | DAIR for acute (<4 weeks); Two-stage revision with antibiotic spacer for chronic. |
| Medial Wall Blowout | <1% (Severe Protrusio, over-reaming in RA). | Structural allograft, impaction bone grafting, anti-protrusio cage, or custom triflange. |
Aseptic loosening and accelerated polyethylene wear were historically common in young, active patients with osteonecrosis. However, the advent of highly cross-linked polyethylene and ceramic-on-ceramic bearings has drastically reduced this complication. When aseptic loosening does occur, often presenting with progressive radiolucent lines and osteolysis, salvage requires revision arthroplasty utilizing extended trochanteric osteotomies (ETO) for stem removal and the use of porous-coated revision components to bridge bone defects.
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol following THA must be tailored to the specific surgical interventions performed to address the underlying hip disorder. Phase I (Immediate Post-Operative, Days 0-14) focuses on early mobilization, deep vein thrombosis (DVT) prophylaxis, and protection of the reconstruction. For standard OA and AVN cases with rigid cementless fixation, immediate weight-bearing as tolerated (WBAT) is encouraged to promote bone ingrowth and prevent deconditioning. However, in cases of severe protrusio acetabuli where extensive medial wall impaction grafting was performed, weight-bearing may be restricted to toe-touch or partial weight-bearing for 6 to 8 weeks to prevent graft subsidence and medial migration of the shell before biologic incorporation occurs.
Phase II (Weeks 2-6) emphasizes the restoration of active range of motion and the initiation of abductor strengthening. In patients with long-standing OA or inflammatory arthropathies, significant preoperative soft tissue contractures (e.g., flexion, external rotation, and adduction contractures) are common. Physical therapy must aggressively target these contractures through sustained stretching and capsular mobilization. Aquatic therapy can be highly beneficial during this phase, providing buoyancy to assist with range of motion while minimizing joint reactive forces.
Phase III (Weeks 6-12) involves advanced proprioceptive training, gait normalization, and the transition to closed-kinetic-chain exercises. Patients with RA often require a more prolonged and modified Phase III protocol due to multi-joint involvement; the use of assistive devices (e.g., platform walkers) may be necessary to protect the upper extremities and contralateral joints. Strengthening of the core and lumbopelvic stabilizers is critical to eliminate the Trendelenburg gait, particularly in patients whose abductor musculature was chronically attenuated by preoperative lateralization or medialization of the hip center.
Long-term surveillance is the final, ongoing phase of rehabilitation. Routine radiographic follow-up at 6 weeks, 1 year, and every 3-5 years thereafter is mandatory. The surgeon must carefully evaluate the radiographs for signs of graft incorporation (in protrusio and AVN), stable bone ingrowth (absence of progressive radiolucent lines), and restoration of the anatomic hip center. Patients must be educated on lifetime activity modifications, avoiding high-impact activities that could accelerate bearing wear or compromise the fixation interface, particularly in the younger osteonecrosis demographic.

Summary of Landmark Literature and Clinical Guidelines
The surgical management of specific hip disorders has been heavily shaped by decades of rigorous clinical research and evolving guidelines. In the realm of inflammatory arthropathies, landmark studies have definitively shifted the paradigm from cemented to cementless fixation. Long-term registry data and retrospective cohorts have demonstrated that highly porous titanium components achieve excellent survivorship in RA patients, rivaling that of OA cohorts, provided initial press-fit stability is obtained. Furthermore, clinical guidelines published jointly by the American College of Rheumatology (ACR) and the American Association of Hip and Knee Surgeons (AAHKS) dictate the precise perioperative management of DMARDs and biologics, balancing the risk of disease flare against the risk of periprosthetic joint infection.
For protrusio acetabuli, the technique of impaction bone grafting remains the gold standard, heavily supported by the foundational literature of Slooff and colleagues, who demonstrated excellent long-term incorporation of morselized allograft and autograft in cavitary defects. Subsequent studies by Ranawat et al. reinforced the necessity of placing the acetabular component at the anatomic hip center and achieving peripheral rim fixation, showing that failure to do so invariably leads to recurrent protrusio and catastrophic failure.