Conservative Hip Surgery: Relief for Bilateral Dysplasia

Key Takeaway
Learn more about Conservative Hip Surgery: Relief for Bilateral Dysplasia and how to manage it. Conservative hip surgery addresses conditions like Developmental Dysplasia of the Hip (DDH) in patients such as a 47-year-old female experiencing severe bilateral groin pain and activity limitations. This joint-preserving approach targets underlying anatomical abnormalities, evident from positive impingement tests, to reduce pain, improve hip function, and potentially avoid or postpone total hip replacement, considering the patient's specific health profile.
You are reviewing a 22-year-old female patient who presents with insidious onset of bilateral groin pain. She has no history of trauma. On physical examination, she demonstrates a waddling gait and increased lumbar lordosis. The AP Pelvis radiograph is shown below. What are the key radiographic features of the condition, and how would you quantify them?
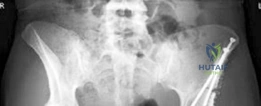
Candidate: This looks like bilateral developmental dysplasia of the hip (DDH). The radiographic features include a shallow acetabulum with reduced coverage of the femoral head. To quantify this, I would measure the lateral center-edge angle of Wiberg, the Tönnis angle, and check the Shenton line. I would also order a false profile view to assess anterior coverage.
Candidates often just describe the hip as "shallow" or "out of the socket" without using standardized, objective terminology. Failing to mention specific normal values (e.g., LCE >25°, Tönnis <10°) suggests a lack of systematic clinical approach. Missing the importance of the Tönnis grade for joint-preservation decision-making is a critical failure.
Start with a structured description: "The AP pelvis reveals bilateral acetabular dysplasia characterized by lateral and superior migration of the femoral head with deficient lateral coverage." Proceed to list the parameters: 1) LCE angle of Wiberg (<20° diagnostic for dysplasia), 2) Tönnis angle (>10° indicating excessive obliquity), 3) ACE angle via false profile (<20°), and 4) Tönnis grade for OA assessment. Emphasize that the primary biomechanical issue is a reduced weight-bearing surface area leading to edge-loading, cartilage delamination, and labral pathology.
The patient is confirmed to have symptomatic bilateral DDH with Tönnis Grade 1 changes. She is requesting surgical management. Discuss your approach to surgical planning, specifically regarding the timing and the potential pitfalls of the Bernese periacetabular osteotomy (PAO).

Candidate: I would recommend staged PAO procedures separated by 3 to 6 months. Simultaneous bilateral surgery has a higher risk of complications like blood loss and recovery difficulty. Regarding the technique, the main risk is an intra-articular fracture during the retroacetabular cut. I would ensure I use the obturator oblique view to stay extra-articular.
Ignoring the "steep learning curve" of the procedure. Failing to mention the importance of blood management (cell salvage) or the need for neurovascular protection (LFCN, obturator nerve) during the approach. Overlooking the importance of checking hip ROM intraoperatively for impingement after fragment reorientation.
Structure the answer by: 1) **Decision Making:** Support staging over simultaneous procedures citing the higher risk of transfusion and morbidity in simultaneous cases. 2) **Technical Execution:** Describe the four cuts (Ischial, Pubic, Iliac, Retroacetabular) emphasizing the preservation of the posterior column and the use of the obturator oblique view to navigate safely. 3) **Complication Mitigation:** Highlight the risk of LFCN injury, intra-articular fracture, and the need for dynamic ROM testing before hardware fixation to avoid pincer-type impingement.
During your follow-up of a patient 8 weeks post-PAO, they complain of persistent numbness over the lateral aspect of the thigh and some difficulty with abduction. What is your differential diagnosis for this presentation, and how do you manage it?
Candidate: The lateral thigh numbness is likely due to a neuropraxia of the Lateral Femoral Cutaneous Nerve (LFCN). The weakness in abduction could be due to pain, deconditioning, or potentially an injury to the superior gluteal nerve or just the healing process of the abductor muscles after the Smith-Petersen approach.
Failing to distinguish between sensory and motor deficits. Suggesting invasive diagnostics immediately rather than observation. Missing the mention of Heterotopic Ossification (HO) as a cause for restricted motion/pain, or not discussing the need for formal physical therapy to address the abductor weakness.
Systematically address the findings: 1) **Sensory:** LFCN neuropraxia is common (up to 30%); reassure the patient, as it is usually self-limiting, and prescribe gabapentinoids if painful. 2) **Motor:** Differentiate between nerve injury (superior gluteal nerve) and mechanical/muscular factors. Abductor weakness is expected in the early post-op phase due to the surgical approach and the need for strengthening. 3) **Red Flags:** Rule out complications like HO (X-ray), hardware failure (X-ray), or deep infection. Emphasize a structured rehabilitation program focusing on gait re-education and progressive abductor strengthening.
