Operative Management of Foot and Ankle Tendon Disorders
Key Takeaway
The operative management of foot and ankle tendon disorders requires a profound understanding of hindfoot biomechanics and soft-tissue balancing. This guide provides an evidence-based framework for treating posterior tibial tendon dysfunction, peroneal tendon tears, flexor hallucis longus impingement, and anterior tibialis ruptures. Surgical strategies range from primary tubularization and retinacular reconstruction to complex tendon transfers and corrective osteotomies, ensuring optimal functional restoration for both athletic and non-athletic patients.
Comprehensive Introduction and Patho-Epidemiology
The operative management of tendon disorders in the foot and ankle represents a complex, highly nuanced intersection of soft-tissue reconstruction and biomechanical realignment. Foundational literature by pioneers such as Johnson, Myerson, Mann, and Sobel has established beyond reproach that isolated soft-tissue procedures are rarely sufficient for chronic tendinopathies associated with structural deformity. Successful outcomes dictate a comprehensive, multi-planar approach: addressing the primary tendon pathology while simultaneously correcting underlying osseous malalignment to protect the reconstruction and restore the mechanical axis of the lower extremity. The paradigm has shifted definitively from simple tenosynovectomies to complex, joint-sparing biomechanical reconstructions that demand a profound understanding of foot and ankle kinematics.
Epidemiologically, foot and ankle tendinopathies exhibit distinct demographic distributions dictated by their unique pathomechanical etiologies. Posterior tibial tendon dysfunction (PTTD), the primary driver of adult acquired flatfoot deformity (AAFD) or progressive collapsing foot deformity (PCFD), predominantly afflicts females in their fifth to seventh decades, often exacerbated by systemic comorbidities such as obesity, hypertension, and diabetes mellitus. Conversely, peroneal tendon disorders are typically observed in a younger, more active demographic, frequently presenting as a sequela of chronic lateral ankle instability, repetitive inversion injuries, or underlying cavovarus foot morphology. Flexor hallucis longus (FHL) pathology, classically termed "dancer's tendinitis," is overwhelmingly prevalent in ballet dancers, gymnasts, and athletes whose disciplines demand extreme, repetitive plantarflexion, leading to mechanical impingement at the fibro-osseous tunnel. Finally, anterior tibialis tendon (ATT) ruptures present as a rare but debilitating entity, most commonly occurring in males over the age of fifty following an unexpected eccentric load applied to a plantarflexed foot.
The pathophysiology underlying these disorders is rarely an acute inflammatory event; rather, it is a chronic degenerative process characterized by mucoid degeneration, neovascularization, and disorganized collagen architecture—a true tendinosis. This degeneration is frequently localized to specific hypovascular "watershed" zones within the tendons, rendering them highly susceptible to mechanical attrition and microtrauma. As the tendon's structural integrity is compromised, it undergoes plastic deformation, elongating beyond its physiological resting length. This elongation leads to a critical loss of mechanical advantage, transferring immense eccentric loads to the secondary static ligamentous restraints, which inevitably attenuate and fail, resulting in progressive, multi-planar osseous deformity.
Detailed Surgical Anatomy and Biomechanics
Posterior Tibial Tendon Anatomy and Biomechanics
The posterior tibial tendon (PTT) is the primary dynamic stabilizer of the medial longitudinal arch and the principal invertor of the midfoot. Originating from the posterior aspects of the tibia, fibula, and interosseous membrane, the muscle belly transitions into a tendon in the distal third of the leg. As it courses posterior to the medial malleolus, it undergoes a sharp 90-degree turn, creating an area of significant mechanical stress and a well-documented hypovascular zone approximately 1 to 1.5 cm distal to the medial malleolus. The PTT boasts a broad, complex insertion, primarily anchoring to the navicular tuberosity and the plantar aspect of the medial cuneiform, with secondary slips extending to the bases of the second, third, and fourth metatarsals, the cuboid, and the sustentaculum tali. Biomechanically, the PTT functions during the stance phase of gait to invert the subtalar joint, which consequently locks the transverse tarsal joint (talonavicular and calcaneocuboid joints). This locking mechanism transforms the midfoot into a rigid lever arm, an absolute prerequisite for efficient forward propulsion during toe-off.
Peroneal Tendon Anatomy and Biomechanics
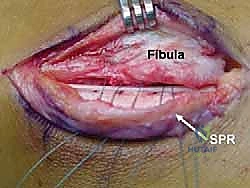
The peroneus longus (PL) and peroneus brevis (PB) tendons occupy the lateral compartment of the leg, serving as the primary evertors of the foot and dynamic stabilizers against lateral ankle inversion. The PB originates from the distal two-thirds of the lateral fibula and inserts onto the tuberosity of the fifth metatarsal. The PL originates more proximally, coursing posterior to the PB within the retromalleolar groove, then diving plantarward through the cuboid tunnel to insert onto the plantar-lateral aspect of the medial cuneiform and the base of the first metatarsal. The superior peroneal retinaculum (SPR) is the primary static restraint preventing subluxation of these tendons from the shallow fibular groove. The PB is particularly vulnerable to longitudinal split tears due to the "bowstringing" effect; during forced dorsiflexion and inversion, the PL compresses the PB against the sharp posterior margin of the fibula, leading to mechanical attrition. Furthermore, the PB possesses a watershed zone at the tip of the lateral malleolus, predisposing it to degenerative tearing.
Flexor Hallucis Longus Anatomy and Biomechanics
The flexor hallucis longus (FHL) originates from the posterior surface of the fibula and the interosseous membrane. Uniquely, its muscle belly extends far distally, often reaching the level of the tibiotalar joint. The tendon courses through a fibro-osseous tunnel bounded anteriorly by the posterior surface of the talus (between the medial and lateral tubercles) and the undersurface of the sustentaculum tali, and posteriorly by the flexor retinaculum. It then traverses the plantar midfoot, crossing superior to the flexor digitorum longus (FDL) at the Knot of Henry, before inserting at the base of the distal phalanx of the hallux. The FHL acts as a powerful plantarflexor of the hallux and ankle. Pathology typically arises at the posterior fibro-osseous tunnel, where a low-lying muscle belly or an accessory os trigonum can cause severe mechanical impingement during extreme ankle plantarflexion, leading to tenosynovitis, nodule formation, and painful triggering.
Anterior Tibialis Tendon Anatomy and Biomechanics
The anterior tibialis tendon (ATT) is the largest and most medial tendon of the anterior compartment, responsible for 80% of ankle dorsiflexion power. Originating from the lateral condyle and proximal half of the tibia, the tendon courses beneath the superior and inferior extensor retinacula to insert onto the medial and plantar surfaces of the medial cuneiform and the base of the first metatarsal. An avascular zone exists between 4.5 cm and 6.5 cm proximal to its insertion, which correlates directly with the most frequent site of spontaneous rupture. Biomechanically, the ATT functions concentrically to clear the foot during the swing phase of gait and eccentrically to control plantarflexion (preventing "foot slap") immediately following heel strike. Rupture of this tendon profoundly disrupts the gait cycle, leading to a steppage gait and secondary contractures of the Achilles tendon.
Exhaustive Indications and Contraindications
The decision-making process for operative intervention in foot and ankle tendinopathies requires a meticulous assessment of the patient's physiological age, functional demands, soft-tissue envelope, and the presence of fixed versus flexible osseous deformity. Non-operative management, including aggressive physical therapy, non-steroidal anti-inflammatory medications, and rigid orthotic bracing (e.g., Arizona brace for PTTD), must be exhaustively trialed for a minimum of 3 to 6 months before considering surgical reconstruction, except in cases of acute tendon ruptures in active individuals.
Surgical intervention for PTTD is heavily dictated by the Johnson and Strom classification, as modified by Myerson. Stage I disease (tenosynovitis without deformity) is treated with tenosynovectomy only if recalcitrant to prolonged conservative care. Stage II disease (tendinosis with flexible flatfoot deformity) is the classic indication for combined soft-tissue reconstruction (FDL transfer) and osseous realignment (medializing calcaneal osteotomy). Once the deformity becomes rigid (Stage III), joint-sparing procedures are absolutely contraindicated, and the surgeon must proceed to definitive arthrodesis (subtalar or triple). For peroneal pathology, isolated tenosynovectomy is indicated for persistent pain without tearing. However, if a longitudinal split tear is identified, tubularization or tenodesis is required, combined with fibular groove deepening if the retromalleolar sulcus is anatomically shallow or convex.
| Pathology / Condition | Primary Surgical Indication | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| PTTD Stage II (Flexible) | Painful flexible flatfoot failing 6 months of bracing; progressive arch collapse. | Rigid deformity (Stage III); Active infection; Charcot neuroarthropathy. | Severe obesity (BMI > 40); Uncontrolled diabetes; Advanced peripheral vascular disease. |
| PTTD Stage III (Rigid) | Painful, rigid hindfoot valgus and forefoot abduction. | Active infection; Medically unfit for major surgery. | Severe osteopenia compromising hardware fixation. |
| Peroneal Split Tear | Persistent lateral retromalleolar pain; MRI-confirmed tear > 3 months duration. | Asymptomatic incidental MRI finding; Active local skin infection. | Sedentary patient with minimal pain; Heavy smoker. |
| FHL Impingement | Posterior ankle pain with extreme plantarflexion; Hallux triggering failing injections. | Generalized ankle osteoarthritis causing the primary pain. | Unrealistic postoperative expectations (e.g., immediate return to elite ballet). |
| ATT Rupture (Acute) | Acute rupture (< 6 weeks) in active, ambulating patient. | Non-ambulatory patient; Severe dementia. | Elderly patient with low functional demands (braceable). |
| ATT Rupture (Chronic) | Chronic rupture with gait dysfunction and flexible hindfoot. | Fixed equinus contracture that cannot be released. | Severe peripheral neuropathy. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning begins with a rigorous clinical examination. For PTTD, the surgeon must evaluate the "too-many-toes" sign, the inability to perform a single-limb heel rise, and the flexibility of the hindfoot and midfoot. The Silfverskiöld test is mandatory to assess for isolated gastrocnemius contracture versus global Achilles tightness, which will dictate the need for a concomitant gastrocnemius recession or Achilles tendon lengthening. For peroneal pathology, provocative testing including resisted eversion and the peroneal subluxation test must be documented. FHL pathology is assessed via the FHL stretch test, noting pain posterior to the medial malleolus during combined ankle and hallux dorsiflexion.
Imaging protocols must be standardized. Weight-bearing anteroposterior, lateral, and mortise radiographs of the foot and ankle are non-negotiable. On the lateral view, the surgeon must measure Meary's angle (talo-first metatarsal angle), calcaneal pitch, and talonavicular coverage angle to quantify the extent of the flatfoot deformity. Magnetic Resonance Imaging (MRI) is highly sensitive for evaluating tendon integrity, utilizing T1-weighted images for anatomical detail and T2/STIR sequences for fluid and edema. The surgeon must be acutely aware of the "magic angle" phenomenon, an artifact occurring when the tendon is oriented at 55 degrees to the main magnetic field, which can falsely simulate tendinosis or tearing on short TE sequences. Computed Tomography (CT) is invaluable for assessing subtalar joint arthritis in advanced PTTD or defining the bony anatomy of an os trigonum in FHL impingement.
Patient positioning is critical for optimal surgical exposure and efficiency. For PTTD reconstruction (FDL transfer and MDCO), the patient is placed supine. A substantial bump is placed beneath the ipsilateral hip to internally rotate the lower extremity, bringing the medial malleolus directly anterior and allowing simultaneous access to the lateral calcaneus for the osteotomy and the medial midfoot for the tendon transfer. For peroneal tendon reconstruction, the patient is placed in the lateral decubitus position, heavily padded, with a beanbag for stabilization. FHL releases can be performed supine (for medial approaches) or prone (for posterior endoscopic approaches). In all cases, a well-padded thigh tourniquet is applied, and the extremity is prepped and draped to above the knee to allow for intraoperative assessment of alignment. Fluoroscopy must be positioned on the contralateral side of the table, entering perpendicular to the operative field.
Step-by-Step Surgical Approach and Fixation Technique
Stage II PTTD Reconstruction: FDL Transfer and MDCO
The gold standard for Stage II PTTD is the FDL tendon transfer combined with a medializing calcaneal osteotomy (MDCO). Correcting the hindfoot valgus is the most critical step; it shifts the mechanical axis of the Achilles tendon medially, converting it from a deforming evertor into a corrective invertor, thereby decreasing the excursion and mechanical demand on the transferred FDL tendon.
The procedure begins with the lateral approach for the MDCO. An oblique incision is made posterior to the peroneal tendons and sural nerve, directly over the lateral calcaneal tuberosity. Dissection is carried down to the periosteum. A sagittal saw is utilized to perform a through-and-through oblique osteotomy, originating just posterior to the posterior facet of the subtalar joint and exiting plantarly. The cut is angled at approximately 45 degrees to the plantar surface of the foot. Using a lamina spreader and a specialized calcaneal shift elevator, the posterior tuberosity is translated medially by 10 to 15 mm. The osteotomy is provisionally pinned with a Kirschner wire. Fluoroscopy confirms the translation and ensures the subtalar joint has not been penetrated. Rigid fixation is achieved using one or two 6.5 mm or 7.0 mm cannulated headless compression screws, placed from the posterior heel pad, traversing the osteotomy, and anchoring solidly into the dense bone of the anterior calcaneal body.
Attention is then directed medially. A longitudinal incision is made extending from the distal medial malleolus to the navicular tuberosity. The flexor retinaculum is incised, and the diseased PTT is exposed. The PTT is typically found to be hypertrophic, flattened, and severely degenerated. It is excised, leaving a small 1 cm distal stump at the navicular. The FDL tendon is identified plantar to the navicular and traced distally to the Knot of Henry. It is transected as distally as possible. To prevent iatrogenic lesser toe clawing, the distal stump of the FDL is tenodesed to the adjacent FHL tendon using a running 2-0 non-absorbable suture.
A 4.5 mm to 5.5 mm drill hole is created dorsal-to-plantar through the center of the navicular tuberosity. The proximal FDL tendon is whipstitched with a #2 high-strength suture (e.g., FiberWire) and passed through the navicular tunnel from plantar to dorsal. Tensioning the transfer is the most technically demanding aspect of the procedure. The foot is held in maximal equinovarus, and the ankle is positioned in slight plantarflexion. While maintaining this position, the FDL is pulled taut, sutured to itself, and secured to the adjacent periosteum and the remaining stump of the PTT using multiple interrupted braided non-absorbable sutures. Finally, the superomedial calcaneonavicular (spring) ligament is inspected; if attenuated, it is imbricated and repaired with suture anchors placed into the sustentaculum tali.
Peroneal Tendon Repair and Fibular Groove Deepening
Surgical management of peroneal tendon disorders requires meticulous soft-tissue handling and a critical assessment of the retromalleolar groove. The patient is positioned laterally, and a longitudinal incision is made along the posterior border of the fibula, extending distally to the base of the fifth metatarsal. The sural nerve, which crosses the operative field distally, must be identified and protected.
The superior peroneal retinaculum (SPR) is incised longitudinally. Crucially, a 2 to 3 mm cuff of retinaculum must be left attached to the posterior fibula to facilitate robust repair during closure. The PL and PB tendons are delivered from the wound and inspected. The PB is meticulously examined for the classic longitudinal split tear, which often spans from the tip of the fibula to the musculotendinous junction.
If the PB exhibits less than 50% cross-sectional degeneration, the degenerative edges of the split are sharply excised. The tendon is then tubularized using a running locked 4-0 non-absorbable suture, restoring its cylindrical contour to allow smooth gliding. If the PB is severely degenerated (>50% non-viable), attempting tubularization will result in a structurally incompetent tendon. In this scenario, the diseased segment is excised entirely. The proximal and distal viable stumps of the PB are then tenodesed to the intact PL tendon using a side-to-side weave technique with heavy non-absorbable suture.
Following tendon repair, the retromalleolar groove is palpated. A flat or convex fibular groove is a primary risk factor for recurrent pathology. To perform a groove deepening procedure, a rectangular cortical flap is created on the posterior aspect of the distal fibula using a sharp 1/4-inch osteotome. The flap is hinged laterally. Cancellous bone is aggressively curetted or burred from beneath the flap to create a deep concavity. The cortical flap is then tamped down into the newly created recess, effectively deepening the sulcus while preserving the smooth fibrocartilaginous gliding surface. The tendons are reduced into the deepened groove, and the SPR is repaired tightly over the tendons using drill holes or small suture anchors placed into the posterolateral fibula, ensuring no residual subluxation occurs with ankle dorsiflexion and eversion.
Flexor Hallucis Longus Release and Endoscopy
Operative intervention for FHL tenosynovitis and posterior impingement can be performed via an open posteromedial approach or a posterior endoscopic approach. For the open approach, an incision is made posterior to the medial malleolus. The deep fascia is incised, and the posterior tibial neurovascular bundle (PTNVB) is carefully identified and retracted anteriorly. The FHL is identified by its characteristic low-lying muscle belly. The fibro-osseous sheath is released completely from the posterior talus down to the level of the sustentaculum tali. The tendon is delivered into the wound, and any nodular thickening or low-lying muscle belly causing impingement is sharply debrided.
Increasingly, the posterior endoscopic approach (popularized by van Dijk) is utilized for its lower morbidity and superior visualization of the posterior ankle anatomy. The patient is placed prone. Two portals are established: a posterolateral portal located just lateral to the Achilles tendon at the level of the joint line, and a posteromedial portal located just medial to the Achilles tendon. A 4.0 mm, 30-degree arthroscope is introduced. The crucial anatomical landmark is the FHL tendon itself. The neurovascular bundle lies immediately medial to the FHL tendon. Therefore, the absolute rule of posterior ankle endoscopy is that the surgeon must keep the camera and all working instruments lateral to the FHL tendon at all times. The flexor retinaculum over the FHL is released endoscopically using a retrograde blade. If an os trigonum or a prominent posterior talar process is present and contributing to impingement, it is excised using an arthroscopic burr and grasping forceps.
Anterior Tibialis Tendon Reconstruction
Surgical management of ATT ruptures depends heavily on the chronicity of the injury. For acute ruptures (<6 weeks) with minimal retraction, primary repair is indicated. An anterior longitudinal incision is made over the ankle joint, slightly lateral to the palpable crest of the tibia to avoid placing the incision directly over the tendon repair. The extensor retinaculum is incised in a step-cut or Z-lengthening fashion; this is vital to allow for anatomic repair during closure and prevent postoperative bowstringing of the tendon. The degenerative tendon ends are debrided back to healthy, parallel collagen fibers. A Krackow or grasping whipstitch technique utilizing a heavy, non-absorbable suture (e.g., #2 FiberWire or Orthocord) is placed in both the proximal and distal stumps. The repair is tied with the ankle held in 10 to 15 degrees of dorsiflexion to restore appropriate resting tension.
In chronic or neglected ruptures, the tendon ends are often retracted, leaving a gap exceeding 3 to 4 cm, rendering primary repair impossible. In these cases, an Extensor Hallucis Longus (EHL) tendon transfer is the procedure of choice. The EHL is harvested distally at the level of the first metatarsophalangeal joint. It is routed proximally and passed through the native ATT sheath. The EHL is then anchored into the medial cuneiform or navicular using a biotenodesis screw or bone anchors. To maintain active hallux extension and prevent a drop-toe deformity, the distal stump of the EHL is tenodesed to the adjacent Extensor Digitorum Longus (EDL) tendon. Alternatively, if the surgeon wishes to preserve native EHL function, an intercalary allograft (such as a semitendinosus or peroneus longus allograft) can be utilized to bridge the ATT defect, woven into the native stumps using a Pulvertaft weave technique.
Complications, Incidence Rates, and Salvage Management
The surgical management of foot and ankle tendon disorders carries a distinct complication profile, largely driven by the complex interplay of soft-tissue healing and osseous union. Neurovascular injury remains a significant concern. The sural nerve is at high risk during the lateral approach for the MDCO and peroneal tendon exploration, while the saphenous nerve and posterior tibial neurovascular bundle are at risk during medial and posterior approaches, respectively.
Nonunion or delayed union of the calcaneal osteotomy occurs in a small percentage of patients, particularly those with a history of tobacco use or poorly controlled diabetes. Over-tensioning of tendon transfers (e.g., FDL for PTTD) can lead to a rigid, iatrogenic equinovarus deformity, which is exceptionally difficult for the patient to tolerate. Conversely, under-tensioning or failure to adequately correct the underlying osseous deformity will result in recurrent flatfoot and early clinical failure of the transfer.
| Complication | Associated Procedure | Estimated Incidence | Prevention Strategy | Salvage Management |
|---|---|---|---|---|
| Sural Nerve Neuritis/Neuroma | MDCO; Peroneal Exploration | 5 - 8% | Meticulous blunt dissection; avoid aggressive retraction; identify nerve early. | Gabapentinoids; targeted nerve blocks; surgical excision of neuroma and burying stump in muscle. |
| Calcaneal Osteotomy Nonunion | MDCO | 2 - 4% | Rigid compression screw fixation; strict NWB protocol; smoking cessation. | Revision internal fixation with autologous bone grafting; prolonged immobilization. |
| Under-correction / Recurrent Deformity | PTTD Reconstruction | 10 - 15% | Ensure adequate (10-15mm) medial translation of MDCO; consider adding lateral column lengthening. | Revision surgery with Triple Arthrodesis to definitively stabilize the hindfoot. |
| Iatrogenic Equinovarus Deformity | FDL Transfer (Over-tensioning) | < 3% | Tension FDL with ankle in neutral/slight plantarflexion, NOT maximal dorsiflexion. | Aggressive physical therapy; if rigid, surgical release or lengthening of the transfer. |
| Deep Vein Thrombosis (DVT) | All Foot/Ankle procedures | 1 - 3% | Early mobilization of toes; chemical prophylaxis in high-risk patients (Caprini score). | Therapeutic anticoagulation (DOACs or LMWH) per hematology guidelines. |
| Wound Dehiscence / Infection | Achilles/ATT/Peroneal approaches | 3 - 6% | Gentle soft-tissue handling; layered closure; avoid operating through compromised skin. | Local wound care; oral/IV antibiotics; surgical debridement; rotational flaps for large defects. |
Phased Post-Operative Rehabilitation Protocols
Successful tendon surgery relies as heavily on strict adherence to a scientifically structured post-operative rehabilitation protocol as it does on the surgical execution itself. Tendon healing undergoes three overlapping biological phases: the inflammatory phase (days 1-7), the proliferative phase (weeks 1-6), and the remodeling phase (weeks 6-12+). The rehabilitation protocol must respect these biological timelines to prevent catastrophic failure of the repair while mitigating the risks of arthrofibrosis and muscle atrophy.
Phase I: Maximum Protection (Weeks 0-6)
The primary goal during the inflammatory and early proliferative phases is the absolute protection of the surgical repair and osseous osteotomies. Immediately post-operatively, the patient is placed in a bulky, well-padded posterior splint. At the 10-to-14-day mark, sutures are removed, and the patient is transitioned to a rigid short leg cast or a locked controlled ankle motion (CAM) boot.
* Weight-Bearing: The patient remains strictly non-weight-bearing (NWB) for a minimum of 4 to 6 weeks.
* Positioning: Immobilization positioning is procedure-specific. For PTTD/FDL transfers, the foot is casted in slight equinovarus to remove tension from the medial repair. For peroneal repairs, the foot is casted in slight eversion. For ATT repairs, the foot is immobilized in slight dorsiflexion.
Phase II: Progressive Loading and Remodeling (Weeks 6-12)
As the tendon enters the remodeling phase, controlled mechanical stress is introduced to promote collagen realignment along the lines of tension.
* Transition: The cast is removed, and the patient is transitioned permanently to a CAM boot.
* Weight-Bearing: Progressive partial weight-bearing is initiated, advancing by 25% of body weight weekly, with the goal of achieving full weight-bearing in the boot by week 8 to 10.
* Physical Therapy: Formal physical therapy commences. The focus is on active range of motion (AROM) and active-assisted range of motion (AAROM). Passive stretching of the repaired tendon is strictly avoided; however, passive stretching of the antagonist muscles is critical (e.g., aggressive Achilles stretching for PTTD patients). Water therapy and stationary cycling in the boot are excellent low-impact modalities.
Phase III: Strengthening and Return to Sport (Weeks 12+)
The final phase focuses on restoring muscular strength, endurance, and proprioception.
* Footwear: The patient is weaned from the CAM boot into supportive athletic footwear. For PTTD reconstructive patients, custom orthotics with medial longitudinal arch support and a medial heel post are prescribed to provide lifelong protection to the reconstruction.
* Therapy: Isotonic and isokinetic strengthening exercises are advanced. Proprioceptive training utilizing a BAPS board or Bosu ball is essential to retrain the neuromuscular pathways disrupted by surgery.
* Milestones: Return to high-impact sports, running, or heavy manual labor is typically restricted until 6 to 9 months post-operatively. Clearance is contingent upon the patient demonstrating greater than 80% symmetric strength compared to the contralateral limb and the ability to perform pain-free dynamic loading (e.g., single-leg hopping).
Summary of Landmark Literature and Clinical Guidelines
The evidence-based practice of foot and ankle tendon surgery is anchored in several landmark publications that have shaped modern clinical guidelines. The classification system proposed by Johnson and Strom in 1989 remains the foundational diagnostic algorithm for PTT
