Simple & Safe Posterior Approach to the Sacroiliac: Key Techniques

Key Takeaway
Here are the crucial details you must know about Simple & Safe Posterior Approach to the Sacroiliac: Key Techniques. The posterior approach to the sacroiliac joint is a simple, safe surgical method used for open reduction and internal fixation of joint disruptions, ilium fractures, and treating infections. While its popularity has diminished, this approach to the sacroiliac joint remains invaluable when adequate imaging is not possible or alternative techniques like plating are used, though reduction and fixation can be technically demanding.
Introduction and Epidemiology
The sacroiliac (SI) joint, a critical component of the pelvic ring, plays a pivotal role in transferring axial loads from the spine to the lower extremities, ensuring the stability and integrity of the entire lumbopelvic complex. Disruptions of the SI joint, often secondary to high-energy trauma such as motor vehicle collisions or falls from height, can lead to significant pelvic instability, neurological deficits, and long-term functional impairment. Epidemiologically, SI joint disruptions represent a substantial portion of posterior pelvic ring injuries, frequently associated with complex fracture patterns of the sacrum and ilium.
While percutaneous screw fixation techniques have gained widespread popularity for their minimally invasive nature, the posterior open approach to the sacroiliac joint remains an indispensable tool in the armamentarium of the orthopedic trauma surgeon. Its enduring value lies in providing direct visualization for complex anatomical reductions, effective debridement for infections, and the versatility to apply various fixation constructs, including plates, which may offer superior biomechanical stability in certain fracture types or patient demographics. This approach is particularly invaluable when fluoroscopic imaging is suboptimal, anatomical reduction cannot be achieved percutaneously, or when infection necessitates aggressive debridement. Despite the technical demands of achieving precise reduction and safe fixation through this approach, its inherent safety profile, meticulously applied, minimizes the risk of vital structure compromise.
Surgical Anatomy and Biomechanics
A thorough understanding of the surgical anatomy and biomechanics of the sacroiliac joint is paramount for safe and effective surgical intervention.
Bony Anatomy
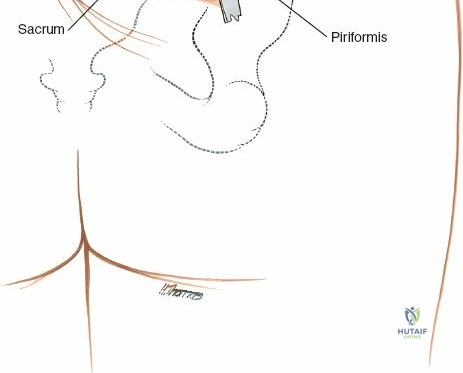
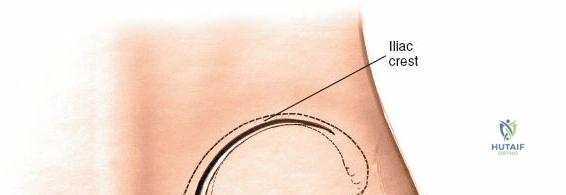
The SI joint is formed by the auricular surfaces of the sacrum and the ilium. The sacrum, a keystone bone, articulates with the two iliac bones. Key bony landmarks relevant to the posterior approach include the posterior superior iliac spine (PSIS), the posterior inferior iliac spine (PIIS), the iliac crest, and the sacral ala and foramina. The PSIS is a consistently palpable landmark, serving as a reliable starting point for incision planning and deeper dissection. The joint itself is hybrid, partly syndesmotic (ligamentous) and partly diarthrodial (synovial), allowing limited motion (typically 2-4 degrees of rotation and 1-2 mm of translation), crucial for shock absorption.
Ligamentous Structures
The stability of the SI joint is predominantly conferred by an exceptionally strong ligamentous complex:
* Posterior Sacroiliac Ligaments: Superficial and deep layers connecting the ilium to the sacrum, particularly robust near the PSIS.
* Interosseous Sacroiliac Ligaments: The strongest ligaments, located deep to the posterior ligaments, filling the space between the sacral and iliac tuberosities.
* Sacrotuberous and Sacrospinous Ligaments: These robust accessory ligaments provide significant stability by connecting the sacrum to the ischial tuberosity and ischial spine, respectively, preventing rotation and superior migration of the hemipelvis.
Disruption of these ligaments is directly correlated with pelvic instability, with successive failure leading to increasingly unstable fracture patterns.
Neurovascular Structures
The proximity of vital neurovascular structures mandates meticulous attention during the posterior approach and fixation.
* Lumbosacral Plexus: The sacral nerve roots (S1-S4) exit the sacrum through the anterior and posterior sacral foramina. The S1 nerve root exits superiorly, and subsequent roots exit progressively caudally. Iatrogenic injury to these nerve roots, particularly S1, is a recognized complication of errant screw placement, leading to motor and sensory deficits.
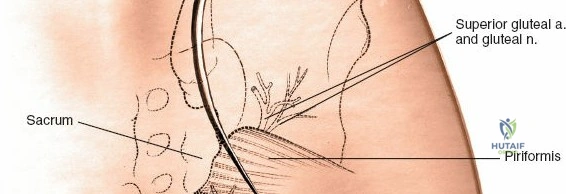
* Superior Gluteal Artery and Nerve: These structures emerge from the greater sciatic notch, superior to the piriformis muscle. Excessive lateral dissection or retraction beyond the iliac crest can endanger this bundle, leading to hemorrhage or gluteal muscle weakness.
* Iliac Vessels: The common and internal iliac vessels lie anterior to the sacrum. Overpenetration of fixation devices through the anterior sacral cortex risks catastrophic hemorrhage.
Muscular Layers
The posterior approach involves traversing several muscle layers:
* Gluteus Maximus: The largest superficial muscle, often split longitudinally in line with its fibers.
* Erector Spinae and Multifidus: Deep muscles that may require partial detachment or retraction from the posterior iliac crest and sacrum.
* Piriformis: Located deep to the gluteus maximus, it crosses the greater sciatic notch.
Biomechanics
The SI joint functions as a dynamic interface for load transfer. Its stability relies on both "form closure" (intrinsic stability from bone and ligamentous architecture) and "force closure" (extrinsic stability from muscle contractions). Traumatic disruptions compromise this biomechanical equilibrium, necessitating surgical stabilization to restore mechanical competence and functional outcomes. Understanding the vectors of instability (e.g., vertical shear, rotational instability) dictates the choice and configuration of fixation.
Indications and Contraindications
The decision to proceed with a posterior open approach to the sacroiliac joint is based on a careful assessment of injury pattern, patient comorbidities, and the specific advantages offered by direct visualization and plating.
Operative Indications
- Unstable Sacroiliac Joint Disruptions: Particularly those classified as Young-Burgess LC-II, LC-III, APC-II, APC-III, and vertical shear (VS) injuries (Tile B and C), where significant displacement or instability exists.
- Fractures of the Ilium Near the Sacroiliac Joint: This includes crescent fractures or complex iliac wing fractures extending into the SI joint, which may require direct reduction and buttressing.
- Sacral Fractures Extending into the SI Joint: Especially those with significant displacement, neurological compromise, or involvement of the sacral foramen that may necessitate direct decompression or plating.
- Sacroiliac Joint Infections: Septic arthritis or osteomyelitis requiring open debridement, washout, and targeted antibiotic delivery.
- Failed Percutaneous Fixation: Cases where closed reduction and percutaneous screw placement fail to achieve or maintain adequate reduction, or where imaging limitations preclude safe percutaneous intervention.
- Need for Direct Anatomical Reduction: When gross displacement, rotation, or comminution prevents accurate closed reduction, requiring direct visualization and manipulation with reduction clamps or pointed reduction forceps.
- Contralateral Pelvic Ring Injuries: In polytrauma patients requiring extensive pelvic stabilization where a comprehensive posterior approach may be beneficial.
- Fusion for Chronic Sacroiliac Pain/Instability: Though less common as a primary approach for isolated fusion, it may be used in conjunction with other procedures or for revision.
Non Operative Indications
- Stable Sacroiliac Joint Disruptions: For example, some APC-I type injuries with minimal displacement and intact posterior ligamentous complex. These are typically managed with protected weight-bearing and pain control.
- Isolated Sacral Fractures: Without significant displacement, neurological deficits, or pelvic instability.
- Medically Unfit Patients: Individuals with severe comorbidities that contraindicate general anesthesia or extensive surgery.
- Symptomatic SI Joint Dysfunction: Without traumatic instability, amenable to conservative measures such as physical therapy, anti-inflammatory medications, and corticosteroid injections.
Contraindications
- Absolute Contraindications:
- Active local soft tissue infection (relative, but requires careful consideration).
- Severe, uncorrectable coagulopathy.
- Patient instability precluding safe anesthesia and surgery.
- Relative Contraindications:
- Severe osteoporosis rendering fixation tenuous.
- Extensive local soft tissue compromise or devitalization, increasing infection risk.
- Lack of surgeon experience with the specific approach and fixation techniques.
Operative Versus Non Operative Indications
| Indication Type | Operative Management | Non Operative Management |
|---|---|---|
| Fracture Pattern | Unstable pelvic ring injuries (Tile B/C, Young-Burgess LC-II/III, APC-II/III, VS) | Stable pelvic ring injuries (e.g., APC-I, minimal displacement) |
| Displacement | Gross displacement, rotational instability, vertical shear | Minimal displacement, intact posterior ligamentous complex |
| Associated Factors | Sacral fractures with neurological deficits, complex iliac fractures | No neurological deficits, isolated sacral ala fractures without displacement |
| Special Cases | Sacroiliac joint infection, failed percutaneous fixation, non-union/malunion | Chronic SI pain without instability (conservative treatment, injections) |
| Patient Status | Medically stable, able to tolerate surgery | Medically unstable, severe comorbidities (unless life-threatening instability) |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is crucial for optimizing outcomes and minimizing complications in posterior sacroiliac surgery.
Imaging Acquisition and Review
- Standard Radiographs: Anteroposterior (AP) pelvic, inlet, and outlet views are essential for initial assessment of pelvic ring integrity and fracture patterns.
- Computed Tomography (CT) Scan: Mandatory for detailed assessment of fracture morphology, comminution, sacral anatomy, and foramen integrity. Multiplanar reconstructions (axial, coronal, sagittal) and 3D reconstructions are invaluable for visualizing fragment orientation, assessing articular involvement, and precisely planning screw trajectories to avoid the sacral nerve roots and anterior vascular structures.
- Magnetic Resonance Imaging (MRI): Useful in cases of suspected ligamentous injury not apparent on CT, evaluation of infection, or to assess for direct nerve root compression.
Templating and Surgical Simulation
- Preoperative templating of screw length, diameter, and trajectory on CT images is highly recommended. Identifying safe zones for screw insertion into the S1 and S2 vertebral bodies, avoiding the sacral foramina, is critical.
- Practice on anatomical bone models or virtual reality simulators can enhance surgeon familiarity with optimal screw paths and reduction maneuvers.
- Confirming C-arm accessibility for inlet, outlet, and lateral sacral views during draping is non-negotiable.
Patient Positioning
The patient is positioned prone on the operating table. This position allows direct posterior access to the SI joint and sacrum.
- Chest and Pelvic Bolsters: Longitudinal bolsters should be carefully placed under the chest wall (from clavicle to iliac crest) and the anterior superior iliac spines (ASIS). Crucially, the abdomen must be free to hang dependent, preventing compression of the inferior vena cava. This maneuver reduces intra-abdominal pressure, thereby decreasing epidural venous bleeding and improving visibility in the operative field.
- Upper Extremities: Arms are typically abducted on arm boards, padded to prevent nerve compression (e.g., ulnar nerve at the elbow, brachial plexus). Abduction should not exceed 90 degrees.
- Lower Extremities: The knees are usually slightly flexed and padded, with pillows placed under the shins to prevent pressure on the knees and toes.
- Head: Positioned in neutral alignment, with appropriate padding to prevent pressure injuries to the face or eyes.
- C-arm Accessibility: Prior to draping, the C-arm must be brought into the field to confirm that unobstructed AP, lateral, inlet, and outlet views of the pelvis and sacrum can be obtained without repositioning the patient or the table during surgery. This is paramount for real-time intraoperative imaging control of reduction and fixation.
Sterile Preparation and Draping
Meticulous sterile preparation and draping are essential to minimize the risk of surgical site infection, particularly given the proximity to the perianal region.
* The entire posterior aspect of the pelvis, including the lower back, buttocks, and perineum, should be meticulously prepped with an antiseptic solution (e.g., iodophor or chlorhexidine-based prep).
* A strict U-drape technique is employed to completely isolate the contaminated anal region from the surgical field. Adhesive drapes are often used for secure exclusion.
* Standard intravenous antibiotic prophylaxis should be administered prior to incision.
Detailed Surgical Approach and Technique
The posterior approach to the sacroiliac joint, while seemingly straightforward, requires precise anatomical knowledge and meticulous technique to ensure both effective fixation and patient safety.
Incision and Initial Dissection
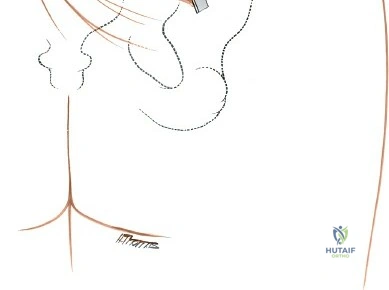
The primary landmark for the posterior approach is the posterior superior iliac spine (PSIS).
* Incision: A longitudinal incision, approximately 10-15 cm in length, is made over the posterior aspect of the ilium, centered over the PSIS and extending inferomedially towards the sacrum. Alternatively, a "hockey stick" incision curving along the iliac crest can be used if wider exposure of the iliac wing is required.
- Subcutaneous Dissection: The skin and subcutaneous tissues are incised. Care is taken to identify and coagulate any perforating vessels.
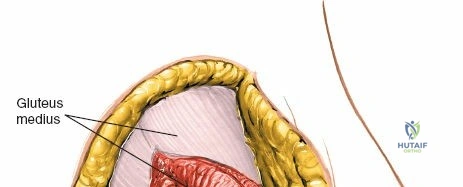
- Fascial Layer: The thoracolumbar fascia is incised longitudinally. The gluteus maximus muscle fibers are then identified.
Muscle Dissection and Exposure
- Gluteus Maximus Split: The gluteus maximus muscle is typically split longitudinally in line with its fibers, rather than transected, to minimize muscle damage. This split begins inferior to the PSIS and extends distally.
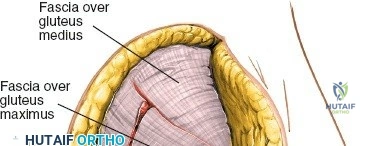
- Subperiosteal Elevation: Using an electrocautery and periosteal elevators, the muscle attachments (primarily gluteus maximus, and potentially portions of the erector spinae and multifidus originating from the iliac crest and sacrum) are elevated subperiosteally from the posterior aspect of the iliac crest, the PSIS, and the adjacent sacrum.
- Exposure of Bony Landmarks: This exposes the posterior aspect of the ilium and sacrum, along with the robust posterior sacroiliac ligaments. The PSIS serves as a key orientation point.



- Retraction: Self-retaining retractors (e.g., Gelpi or Weitlaner) or malleable retractors are carefully placed to maintain exposure, ensuring not to place excessive pressure on soft tissues or neurovascular structures. Lateral retraction should be judicious to avoid injury to the superior gluteal neurovascular bundle exiting the greater sciatic notch.
Visualization of the Sacroiliac Joint and Ligaments
- Deepening the Exposure: Further subperiosteal elevation deep to the posterior sacroiliac ligaments allows direct visualization of the SI joint line and any associated fractures or dislocations. The strong interosseous sacroiliac ligaments are encountered at this stage.



Reduction Techniques
Achieving anatomical reduction is the cornerstone of successful fixation, particularly for unstable SI joint disruptions.
* Preoperative Traction: For vertical displacement, longitudinal traction, preferably applied preoperatively through a distal femoral or tibial pin, is often effective. This should be maintained during the initial phases of the approach.
* Direct Manipulation: With direct visualization, various instruments can be employed:
* Reduction Clamps: Pointed reduction forceps, Jungbluth clamps, or Weber clamps can be applied across the iliac crest and sacrum to compress or distract fragments.
* Bone Hooks/Levers: Hohmann retractors or similar levers can be used to manipulate fragments.
* K-wire Fixation: Temporary K-wires are invaluable for holding reduction once achieved, allowing for definitive fixation.
Fixation Strategies
The choice between screws, plates, or a combination depends on the specific injury pattern, bone quality, and surgeon preference.
Sacroiliac Screw Fixation
- Technique: Typically, one or two large diameter (7.0 or 7.3 mm) cannulated, partially threaded screws are inserted from the ilium across the SI joint into the S1 and/or S2 vertebral bodies.
- Trajectory Planning: Preoperative CT templating is critical. The optimal trajectory generally runs from the posterior ilium, just anterior to the PSIS, aiming into the anterior aspect of the S1 or S2 body.
- S1 Screws: Aim slightly anterior and inferior towards the S1 body, avoiding the S1 nerve root exiting the superior aspect of the S1 foramen.
- S2 Screws: May offer a slightly larger bony target, but still require careful trajectory to avoid the S2 nerve root.
- Fluoroscopic Control: Strict intraoperative C-arm fluoroscopy is mandatory at every step:
- Inlet View: Confirms the screw is not breaching the anterior sacral cortex.
- Outlet View: Shows the relationship to the sacral foramina and helps ensure the screw is within the sacral body.
- Lateral View: Confirms appropriate depth and trajectory within the sacrum.
- Drilling and Tapping: A guide wire is advanced under fluoroscopic control. The trajectory is confirmed in all three planes (inlet, outlet, lateral) before drilling. A cannulated drill bit is used, followed by tapping if using non-self-tapping screws. The screw length is measured, and the appropriate screw is inserted.
- Computer-Assisted Navigation: If available, this technology can significantly enhance the accuracy and safety of screw placement, particularly in complex cases or distorted anatomy.
Dorsal Sacroiliac Plating
- Indications: Plating is often preferred for highly unstable injuries, vertical shear injuries, crescent fractures, or when additional rotational stability is required. It can also be used in conjunction with sacroiliac screws.
- Plate Placement: Specialized dorsal SI plates are contoured to fit the posterior aspect of the ilium and sacrum. The plate is positioned lateral to the sacral foramina, typically spanning the SI joint.
- Screw Fixation for Plates: Cortical or locking screws are used to secure the plate to both the ilium and the sacrum. Similar to SI screws, all screw trajectories into the sacrum must be meticulously checked with fluoroscopy to avoid neurovascular structures. The screws should engage at least two cortices in both the ilium and sacrum.




Wound Closure
- Irrigation and Hemostasis: The wound is thoroughly irrigated with saline solution, and meticulous hemostasis is achieved.
- Drainage: A suction drain may be placed in the deep wound space to manage anticipated postoperative bleeding and reduce hematoma formation.
- Layered Closure: The deep fascia is closed with absorbable sutures to re-approximate the gluteus maximus. The subcutaneous tissues are closed, followed by skin closure using sutures, staples, or adhesive strips.
Complications and Management
Despite the "simple and safe" nature of the posterior approach to the sacroiliac joint compared to anterior approaches, a distinct set of potential complications exists. Meticulous surgical technique, thorough preoperative planning, and vigilant postoperative monitoring are essential for their prevention and management.
| Complication Type | Incidence (Approximate) | Salvage Strategies |
|---|---|---|
| Neurovascular Injury | 2-15% | Immediate screw revision/removal (if malpositioned); nerve exploration and neurolysis; vascular repair (if anterior cortical breach); compartment syndrome fasciotomy (rare). Prophylactic measures include strict fluoroscopic control, pre-op CT. |
| Surgical Site Infection | 1-5% (deep); 5-10% (superficial) | Debridement and irrigation, targeted intravenous antibiotics; hardware removal if infection persists after union or chronic non-union. Rigorous sterile technique, prophylactic antibiotics. |
| Malunion / Non-union | 5-20% | Revision surgery with osteotomy, bone grafting, and enhanced fixation (e.g., combined plate/screws); physical therapy for functional deficits; pain management. Achieved by anatomical reduction, stable fixation, appropriate weight-bearing. |
| Hardware Failure / Prominence | 5-10% | Hardware removal after union; revision with stronger or different fixation if fixation is primary failure; padding over prominent hardware. |
| Persistent Pain | 10-30% | Conservative management (PT, injections, medication); hardware removal (if irritating); diagnostic nerve blocks; SI joint fusion (if instability persists or degenerative etiology). |
| Hematoma Formation | 5-10% | Observation, pain management; surgical evacuation if large or symptomatic; drain placement during surgery. |
| Deep Vein Thrombosis (DVT) | 1-5% | Anticoagulation; placement of inferior vena cava filter (if contraindicated for anticoagulation). Prophylactic anticoagulation, early mobilization. |
| Superior Gluteal Nerve/Artery Injury | Rare | Careful dissection, limited lateral retraction. If identified, nerve repair/vascular repair. |
Neurovascular Injury
The most critical potential complications are iatrogenic injuries to the sacral nerve roots (S1, S2, S3) or the major iliac vessels.
* Sacral Nerve Roots: Malpositioned screws, particularly those directed too far posterolaterally or penetrating the sacral foramen, can directly injure the exiting nerve roots. This can manifest as motor weakness (e.g., foot drop, gluteal weakness), sensory deficits, or intractable neuropathic pain. Vigilant fluoroscopic control (inlet, outlet, lateral views) during guide wire and screw placement is paramount. Electromyography (EMG) or somatosensory evoked potential (SSEP) monitoring may be considered in high-risk cases.
* Iliac Vessels: Anterior cortical breach of the sacrum by a screw can lead to catastrophic hemorrhage due to injury to the common iliac, internal iliac, or external iliac vessels. This is generally avoided by confirming screw tip position on the inlet view and ensuring the screw does not violate the anterior cortex.
* Superior Gluteal Nerve/Artery: Excessive or uncontrolled lateral retraction of the gluteal musculature can injure the superior gluteal neurovascular bundle as it exits the greater sciatic notch. This can cause significant bleeding or gluteal muscle weakness.
Management: Immediate recognition is key. If a malpositioned screw is suspected or confirmed (e.g., by intraoperative neurological change, excessive bleeding, or post-operative imaging), the screw should be promptly removed or revised. Neurological symptoms may require formal nerve exploration and neurolysis. Vascular injuries necessitate immediate vascular surgery consultation and repair.
Surgical Site Infection (SSI)
Despite stringent aseptic techniques, SSIs can occur, ranging from superficial cellulitis to deep osteomyelitis. The proximity to the perianal region warrants extra caution during draping.
Management: Superficial infections typically respond to oral antibiotics. Deep infections often require surgical debridement, thorough irrigation, collection of cultures for targeted antibiotic therapy, and potentially prolonged intravenous antibiotics. Hardware removal may be necessary if infection persists, though generally not before bony union is achieved.
Malunion or Non-union
Inadequate reduction or insufficient fixation can lead to malunion (healing in a deformed position) or non-union (failure of healing). This results in persistent pain, gait disturbance, and long-term functional deficits.
Management: Revision surgery may be indicated, involving osteotomies to correct malalignment, débridement of non-union sites, bone grafting, and more robust fixation. Physical therapy and pain management are also critical components of long-term care.
Hardware Failure or Prominence
Screws or plates can loosen, break, or become prominent under the skin, causing irritation.
Management: Symptomatic hardware typically warrants removal once bony union is confirmed. If hardware failure leads to loss of reduction or non-union, revision surgery with new fixation is required.
Persistent Pain
Even after anatomically successful fixation, some patients may experience chronic pain localized to the SI joint or referred to the lower back or leg. This can be multifactorial, including residual joint damage, nerve irritation, or muscle imbalance.
Management: A multidisciplinary approach involving physical therapy, pain management specialists, diagnostic injections (e.g., SI joint blocks), and sometimes hardware removal. In select cases, if instability or degenerative changes persist, SI joint fusion may be considered.
Post Operative Rehabilitation Protocols
A structured and progressive rehabilitation protocol is integral to achieving optimal functional outcomes following posterior SI joint fixation. The specific protocol must be tailored to the individual patient, considering the severity of the injury, the stability of fixation, bone quality, and concomitant injuries.
Immediate Postoperative Phase (Weeks 0-6)
- Pain Management: Aggressive pain control with a multimodal approach (opioids, NSAIDs, neuropathic agents) to facilitate early mobilization.
- Deep Vein Thrombosis (DVT) Prophylaxis: Pharmacological prophylaxis (e.g., low molecular weight heparin) and mechanical prophylaxis (e.g., sequential compression devices) are initiated immediately.
- Weight Bearing Status:
- For most unstable SI joint injuries, touch-down weight bearing (TDWB) or non-weight bearing (NWB) on the affected side is prescribed for 6-8 weeks to protect the repair.
- In cases of highly stable fixation or for sacral fractures with minimal SI joint involvement, protected weight bearing (e.g., 25-50% weight bearing with crutches/walker) may be considered, but strict surgeon discretion is advised.
- Physical Therapy Focus:
- Bed Mobility and Transfers: Education on safe log-rolling, bed mobility, and transfers to avoid unwanted stress on the pelvis.
- Range of Motion (ROM): Gentle active and passive range of motion exercises for hips, knees, and ankles. Avoidance of hip flexion beyond 90 degrees or extreme rotation, which can stress the SI joint.
- Core Activation: Isometric abdominal and gluteal muscle contractions, without stressing the pelvis, to initiate core stability.
- Upper Extremity Strengthening: Important for ambulation with crutches/walker.
- Wound Care: Daily wound checks, dressing changes, and monitoring for signs of infection.
Intermediate Phase (Weeks 6-12)
- Radiographic Assessment: Follow-up radiographs (AP pelvis, inlet, outlet views) are obtained around 6-8 weeks to assess for early signs of healing and to confirm hardware integrity and position.
- Progression of Weight Bearing: Based on radiographic evidence of healing and clinical stability, weight-bearing status is gradually advanced. This typically progresses from TDWB/NWB to partial weight bearing (PWB) and then to full weight bearing (FWB) as tolerated.
- Physical Therapy Focus:
- Gait Training: Progression from assistive devices to independent ambulation. Emphasis on normal gait mechanics.
- Strengthening: Gradual introduction of progressive resistance exercises for hip abductors, extensors, and core musculature. Avoidance of direct impact loading or ballistic movements.
- Balance and Proprioception: Incorporate exercises to improve balance and proprioception.
- Soft Tissue Mobilization: Gentle scar massage and stretching to improve tissue extensibility.
Advanced Phase (Weeks 12-24 and Beyond)
- Full Weight Bearing: Most patients are able to fully weight bear and discontinue assistive devices, provided adequate radiographic healing.
- Physical Therapy Focus:
- Functional Training: Activities that simulate daily life tasks, incorporating multi-joint movements.
- High-Level Strengthening: Advanced resistance training, including eccentric exercises.
- Sport-Specific Training (if applicable): Gradual return to recreational or athletic activities, with emphasis on proper body mechanics and injury prevention.
- Endurance Training: Cardiovascular exercises (e.g., swimming, cycling) to improve overall fitness.
- Long-Term Monitoring: Periodic clinical and radiographic follow-up to monitor for complications, assess long-term outcomes, and address any residual pain or functional limitations. Hardware removal may be considered after 12-18 months if symptomatic or requested by the patient and if union is complete.
Summary of Key Literature and Guidelines
The literature concerning the posterior open approach to the sacroiliac joint, while evolving with the advent of percutaneous techniques, remains robust for specific indications. Current orthopedic trauma guidelines emphasize anatomical reduction and stable fixation for displaced unstable pelvic ring injuries, including those involving the SI joint.
Key Principles from Literature:
* Anatomical Reduction: Multiple studies underscore the importance of anatomical reduction, particularly for vertically unstable injuries, to achieve optimal long-term functional outcomes and minimize the risk of post-traumatic arthrosis and chronic pain. The direct visualization afforded by the open posterior approach can be critical in achieving this in complex cases where closed reduction is inadequate.
* Stable Fixation: The choice of fixation (screws, plates, or combined) depends on the injury pattern. Dorsal plating, often used with the posterior approach, has been shown to provide robust biomechanical stability, particularly against rotational and vertical shear forces, making it suitable for severely unstable SI joint disruptions or associated iliac fractures.
* Role of Percutaneous vs. Open: While percutaneous sacroiliac screw fixation is the preferred method for many SI joint disruptions due to its reduced soft tissue dissection and lower infection rates, the open posterior approach retains its role when:
* Direct visualization is required for complex anatomical reduction.
* Infection necessitates debridement.
* Plating provides superior stability for specific fracture patterns (e.g., crescent fractures, highly comminuted sacral fractures).
* Image guidance is inadequate or unavailable.
* Revision surgery is required.
* Neurovascular Safety: The importance of meticulous preoperative planning using CT scans and strict intraoperative fluoroscopic control for screw placement cannot be overstated. Computer-assisted navigation has shown promise in improving screw placement accuracy and reducing complications.
* Infection Management: The open approach allows for thorough debridement and washout in cases of septic SI joint arthritis or osteomyelitis, which is difficult to achieve with percutaneous methods.
* Multidisciplinary Approach: The management of complex pelvic ring injuries, including those of the SI joint, often benefits from a multidisciplinary team involving orthopedic trauma surgeons, neurosurgeons, vascular surgeons, and rehabilitation specialists.
Guidelines and Resources:
* The Orthopaedic Trauma Association (OTA) and American Academy of Orthopaedic Surgeons (AAOS) regularly publish clinical practice guidelines and educational materials that inform the management of pelvic and acetabular fractures. These resources consistently advocate for stable anatomical fixation of unstable pelvic ring injuries.
* Classic texts by Tile, Rockwood and Green, and Bucholz and Heckman provide foundational knowledge and detailed descriptions of surgical approaches and fixation strategies for pelvic trauma. These resources highlight the posterior approach as a time-tested method for achieving direct access to the SI joint.
In conclusion, the posterior approach to the sacroiliac joint, while perhaps less frequently utilized than its percutaneous counterpart for simple dislocations, remains an essential and effective surgical technique. Its "simple and safe" attributes, when applied with a profound understanding of surgical anatomy, meticulous technique, and rigorous adherence to fluoroscopic control, enable surgeons to achieve anatomical reduction and stable fixation, especially in challenging situations where direct visualization and robust plating are paramount. Continual advancements in imaging, navigation, and fixation devices further refine its application, ensuring its place as a critical option in pelvic trauma surgery.
Clinical & Radiographic Imaging

