Deepen Skills: Anterolateral & Lateral Surgical Approaches

Key Takeaway
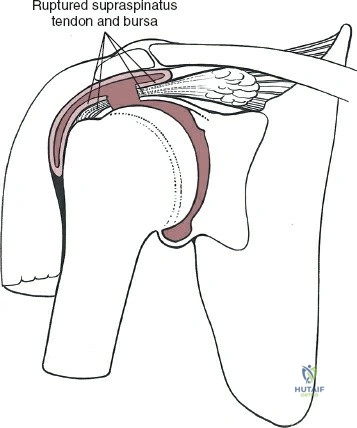
Discover the latest medical recommendations for Deepen Skills: Anterolateral & Lateral Surgical Approaches. The anterolateral and lateral approaches to the shoulder involve dissecting the outer muscular sleeve, primarily splitting the lateral deltoid muscle fibers. This surgical technique leverages the deltoid's multipennate arrangement, which allows for longitudinal splitting despite its strength. These approaches facilitate access to underlying structures, including the supraspinatus tendon, for orthopedic procedures.
Introduction and Epidemiology
As Academic Orthopedic Surgeons and Medical Educators, our commitment lies in fostering a deep understanding of surgical principles and techniques. This discourse aims to meticulously dissect the anterolateral and lateral surgical approaches to the shoulder, providing a high-yield reference for orthopaedic surgeons, residents, and medical students. Mastery of these approaches is fundamental for addressing a spectrum of pathologies, from complex rotator cuff tears to intricate proximal humerus fractures and demanding shoulder arthroplasty.
The anterolateral and lateral approaches to the shoulder are workhorse incisions in orthopaedic surgery, providing excellent access to the subacromial space, rotator cuff, greater tuberosity, and proximal humeral shaft. Historically, open shoulder surgery relied heavily on extensive deltoid detachment, often leading to significant morbidity. Over time, refinements in surgical technique, driven by a deeper understanding of deltoid anatomy and vascular supply, have evolved towards deltoid-splitting or deltoid-sparing approaches, minimizing iatrogenic injury and improving functional outcomes.

Epidemiologically, conditions managed via these approaches are prevalent. Rotator cuff tears, particularly large to massive tears requiring open repair or superior capsule reconstruction, are common, with incidence increasing with age. Proximal humerus fractures constitute approximately 4-5% of all fractures, frequently necessitating open reduction and internal fixation (ORIF) or arthroplasty, often utilizing these lateral exposures. Additionally, open acromioplasty, glenohumeral arthrodesis, and certain shoulder arthroplasty procedures, such as reverse total shoulder arthroplasty, may employ modifications of these approaches. The utility of these exposures underscores their critical importance in the orthopaedic surgeon's armamentarium.
Surgical Anatomy and Biomechanics
A profound understanding of the surgical anatomy underpinning the anterolateral and lateral approaches is paramount for minimizing complications and optimizing surgical outcomes. This involves meticulous knowledge of osteology, musculature, neurovascular structures, and capsuloligamentous complexes.
Osteological Considerations
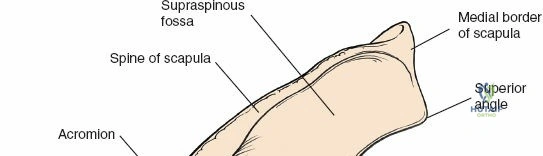
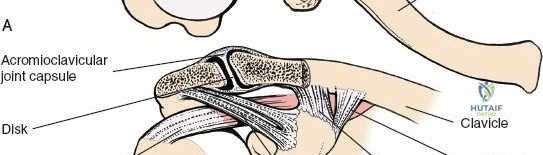
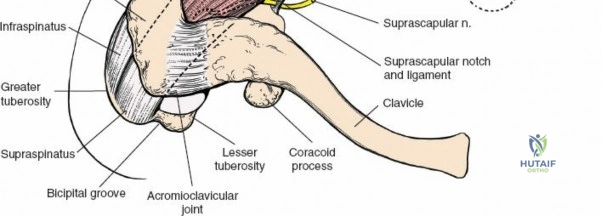
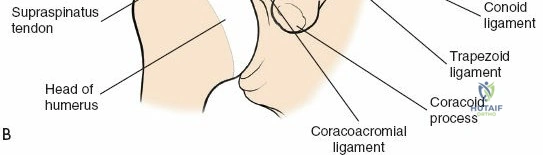
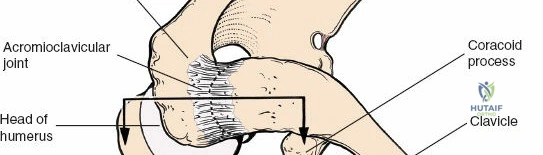
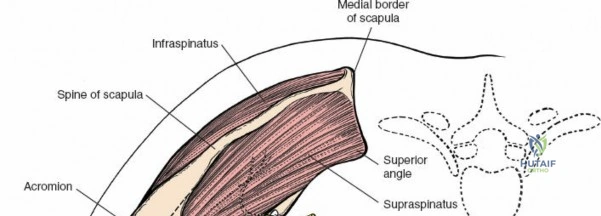
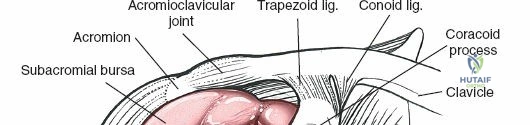
The acromion serves as a crucial landmark and the superior boundary of the subacromial space. As noted in the foundational text, the acromion exhibits considerable morphological variation. These variations, particularly Hooked (Type III) or Curved (Type II) acromial types, have been associated with an increased incidence of impingement syndrome and rotator cuff tears. Early anatomical studies classified acromial morphology, correlating specific shapes with disease processes. Surgical decompression, or acromioplasty, aims to recontour the undersurface of the acromion to alleviate impingement. The greater tuberosity of the humerus is the insertion site for the supraspinatus, infraspinatus, and teres minor tendons, making its anatomical restoration critical in fracture management and rotator cuff repair. The humeral head and proximal humerus are the primary targets for fracture fixation and arthroplasty.
Musculature and Internervous Planes
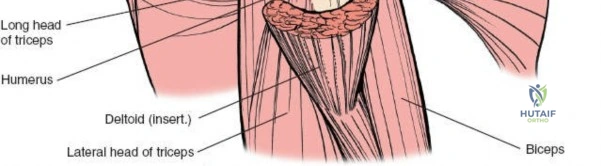
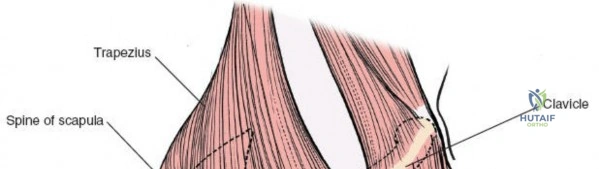
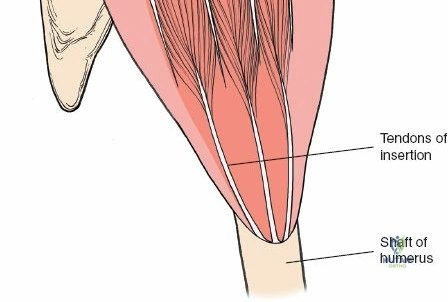
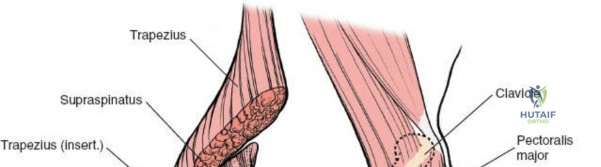
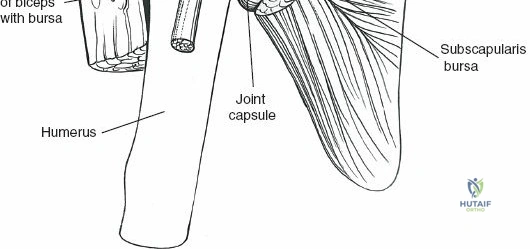
The deltoid muscle is the principal muscle encountered. Its tri-part nature—anterior, middle (lateral), and posterior—is critical. The lateral approach affects the portion of the deltoid muscle that arises from the lateral border of the acromion. The lateral deltoid consists of oblique fibers arising in a multipennate fashion from tough tendinous bands that originate from the acromion. These bands actually mark the bone with a series of notches. Similar bands arise from the insertion of the muscle onto the humerus halfway down the lateral humeral shaft at the deltoid tuberosity.

Unlike the deltopectoral approach, which exploits a true internervous plane between the deltoid (axillary nerve) and pectoralis major (medial and lateral pectoral nerves), the anterolateral and lateral approaches do not utilize a true internervous plane. Instead, they rely on a blunt split of the deltoid muscle fibers. The anterolateral approach typically splits the interval between the anterior and middle thirds of the deltoid, while the direct lateral approach splits the middle third. Because the entire deltoid is innervated by the axillary nerve, splitting the muscle fibers carries an inherent risk of denervating the anterior or lateral portions of the muscle if the split extends too far distally.
Neurovascular Structures
The axillary nerve is the most critical structure at risk during these approaches. After exiting the quadrangular space, the axillary nerve courses anteriorly around the surgical neck of the humerus, deep to the deltoid muscle, supplying it and the overlying skin. The nerve typically lies approximately 5 to 7 centimeters distal to the lateral edge of the acromion. However, this distance is variable and depends heavily on the patient's arm length and the anterior-to-posterior position of the split.
The "safe zone" for splitting the deltoid is generally considered to be within 5 cm of the acromion. Extending the split beyond this point risks transecting the anterior branches of the axillary nerve, leading to devastating anterior deltoid paralysis. Accompanying the axillary nerve is the posterior circumflex humeral artery (PCHA), which provides significant vascularity to the proximal humerus and must be protected during deep dissection and retractor placement.
Indications and Contraindications
The selection of the anterolateral or lateral approach depends on the precise location of the pathology, the required distal extension, and the surgeon's familiarity with the regional anatomy. These approaches are highly versatile but must be applied judiciously based on strict clinical criteria.
Operative Versus Non Operative Management
The decision to proceed with surgical intervention utilizing these approaches requires a careful analysis of patient factors, biomechanical demands, and fracture or tear morphology.
| Pathology | Operative Indications (Anterolateral or Lateral Approach) | Non-Operative Indications |
|---|---|---|
| Proximal Humerus Fractures | Displaced 2-part, 3-part, or 4-part fractures; greater tuberosity displacement > 5mm; head-split fractures. | Minimally displaced fractures; non-ambulatory patients with low functional demands; prohibitive surgical risk. |
| Rotator Cuff Tears | Acute massive tears; chronic tears with significant weakness failing conservative therapy; superior capsular reconstruction. | Partial-thickness tears; asymptomatic full-thickness tears in elderly; advanced fatty infiltration (Goutallier stage 3-4) without arthroplasty plan. |
| Shoulder Arthroplasty | Cuff tear arthropathy (RTSA); complex fracture sequelae requiring arthroplasty where lateral exposure is optimal. | Active joint infection; neuropathic joint (Charcot); severe deltoid dysfunction (axillary nerve palsy). |
| Subacromial Impingement | Refractory impingement failing > 6 months of structured physical therapy and corticosteroid injections. | First-line presentation; concurrent adhesive capsulitis (requires resolution prior to acromioplasty). |
Specific Contraindications
Absolute contraindications to the lateral and anterolateral approaches include active overlying soft tissue infection and pre-existing severe axillary nerve palsy (unless the procedure is a nerve graft or transfer). Relative contraindications include previous extensive surgical approaches in the same region that may have distorted the axillary nerve anatomy, necessitating a more extensile or alternative exposure such as the deltopectoral approach to safely identify and protect the neurovascular bundle.

Pre Operative Planning and Patient Positioning
Meticulous preoperative planning and optimal patient positioning are foundational for a successful procedure. The spatial orientation of the glenohumeral joint requires specific intraoperative setups to maximize visualization and allow for dynamic assessment of the shoulder.
Imaging Modalities
Standard preoperative imaging includes a complete shoulder trauma series: true anteroposterior (Grashey), scapular Y, and axillary lateral radiographs. For proximal humerus fractures, a non-contrast computed tomography (CT) scan with 3D reconstruction is highly recommended to assess articular surface involvement, tuberosity displacement, and bone stock. For rotator cuff pathology, magnetic resonance imaging (MRI) without contrast is the gold standard for evaluating tendon retraction, muscle atrophy, and fatty infiltration.

Patient Positioning Techniques
The Beach Chair Position is the most commonly utilized setup for anterolateral and lateral approaches. The patient is placed supine, and the back of the operating table is elevated to approximately 45 to 60 degrees. The patient's head must be securely stabilized in a neutral position to prevent cervical spine hyperextension or lateral flexion, which can cause brachial plexus traction injuries.
The operative arm must be completely free-draped to allow for unrestricted manipulation. A mechanical arm holder (e.g., Spider arm or Trimano) is frequently employed to maintain the arm in desired degrees of abduction and rotation, facilitating access to different aspects of the rotator cuff and proximal humerus.
Alternatively, the Lateral Decubitus Position can be utilized, particularly for arthroscopic-assisted procedures that may transition to a mini-open lateral approach. The arm is placed in balanced suspension with 10 to 15 pounds of traction. While this provides excellent visualization of the glenohumeral joint, orientation can be more challenging for open fracture fixation compared to the beach chair position.

Detailed Surgical Approach and Technique
The execution of the anterolateral and lateral approaches demands precise soft tissue handling and a rigorous adherence to anatomic boundaries to prevent iatrogenic morbidity.
Skin Incision and Subcutaneous Dissection
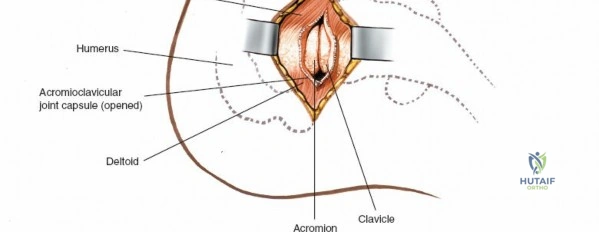
For the Anterolateral Approach, the skin incision begins at the anterior aspect of the acromion, just lateral to the acromioclavicular joint, and extends distally for approximately 3 to 5 centimeters in line with the humeral shaft.

For the Direct Lateral Approach, the incision is centered over the lateral border of the acromion and extends distally. Subcutaneous tissues are bluntly dissected to expose the underlying deep fascia of the deltoid muscle. Hemostasis is achieved using electrocautery, taking care to identify and coagulate branches of the acromial rete.
Deltoid Splitting and Axillary Nerve Protection
Once the deltoid fascia is exposed, the raphe between the anterior and middle thirds of the deltoid (for the anterolateral approach) or the central fibers of the middle deltoid (for the lateral approach) is identified. The muscle fibers are bluntly separated using a periosteal elevator or the surgeon's finger.

It is absolutely critical to limit the distal extent of this split to 4 to 5 centimeters from the lateral edge of the acromion. To prevent inadvertent distal propagation of the split during retraction, a heavy non-absorbable stay suture (e.g., #1 or #2 Ethibond) is routinely placed at the distal apex of the split.
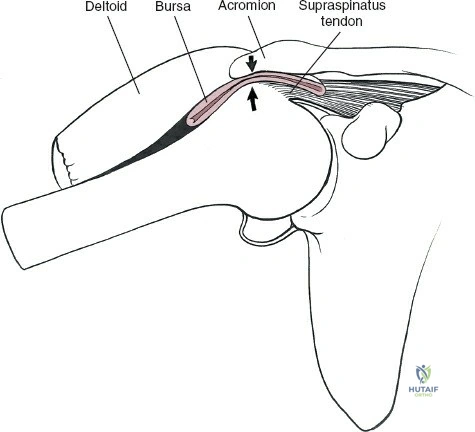
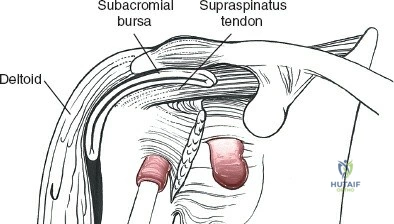
Deep to the deltoid, the subacromial bursa is encountered. This is often thickened and inflamed in the setting of rotator cuff disease or filled with hematoma in the setting of trauma. A thorough bursectomy is performed to expose the underlying rotator cuff insertions and the greater tuberosity.
Extended Lateral Approach and Minimally Invasive Plate Osteosynthesis
For proximal humerus fractures with diaphyseal extension, the Extended Lateral Approach is highly advantageous, allowing for Minimally Invasive Plate Osteosynthesis (MIPO). This technique involves a proximal deltoid-splitting window and a separate distal window.

In the extended lateral approach, the axillary nerve must be definitively identified and protected. After the initial proximal deltoid split, blunt dissection is carried distally deep to the deltoid. The axillary nerve can be palpated as a distinct cord traversing horizontally across the humeral neck.
A distal incision is made along the lateral aspect of the arm, identifying the lateral border of the biceps and the brachialis. The brachialis is split longitudinally to expose the humeral shaft.
A locking compression plate is then slid submuscularly from the proximal window to the distal window. Crucially, the plate must pass deep to the axillary nerve to avoid compressing or tethering the nerve against the hardware.
Reduction and Fixation Strategies
Once exposure is achieved, fracture reduction or rotator cuff repair commences. For proximal humerus fractures, heavy non-absorbable sutures are passed through the insertions of the supraspinatus, infraspinatus, and subscapularis. These traction sutures allow for indirect manipulation and reduction of the tuberosity fragments.
The humeral head is reduced to the shaft, and provisional fixation is achieved with Kirschner wires. The lateral locking plate is applied, ensuring it is positioned posterior to the bicipital groove to avoid impingement on the long head of the biceps tendon, and distal enough to clear the acromion during shoulder abduction.

For rotator cuff repairs, the footprint on the greater tuberosity is decorticated to a bleeding bone bed. Suture anchors are placed in a single-row or double-row configuration, and the tendon is mobilized and repaired under appropriate tension.
Complications and Management
While the anterolateral and lateral approaches provide excellent exposure, they are associated with specific complications that require vigilant intraoperative technique and prompt postoperative management.
Neurological Injury
The most feared complication is injury to the axillary nerve. This can occur via direct laceration if the deltoid split extends too far distally, or via traction neuropraxia from aggressive retraction.

Iatrogenic injury to the axillary nerve results in paralysis of the deltoid muscle and loss of sensation over the lateral shoulder (the "regimental badge" area). If a complete transection is recognized intraoperatively, immediate primary microsurgical repair or nerve grafting is indicated. For postoperatively identified neuropraxia, observation and electromyography (EMG) at 6 to 12 weeks are standard, with nerve transfers (e.g., radial nerve branch to triceps transferred to axillary nerve) considered if no recovery is evident by 3 to 6 months.

Biomechanical Failure and Soft Tissue Complications
Deltoid avulsion from the acromion is a catastrophic complication, historically associated with extensive open approaches but still possible if the proximal origin is aggressively undermined. Repair requires transosseous sutures through the acromion and yields unpredictable functional results.

In fracture management, hardware complications such as intra-articular screw penetration (cut-out) due to osteoporotic bone settling, or varus collapse of the humeral head, are significant risks.
Avascular necrosis (AVN) of the humeral head can occur following complex proximal humerus fractures due to disruption of the anterior and posterior circumflex humeral arteries. The risk of AVN is highly correlated with the integrity of the medial calcar hinge and the length of the metaphyseal extension attached to the head fragment (Hertel's criteria).
Summary of Common Complications
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Strategy / Management |
|---|---|---|---|
| Axillary Nerve Palsy | 1% - 5% | Distal deltoid split >5cm; aggressive retraction; plate compression. | Observation (neuropraxia); EMG at 6-12 weeks; Nerve transfer (radial to axillary) for chronic deficits. |
| Deltoid Dehiscence | < 1% | Excessive proximal soft tissue stripping; failure to repair fascia. | Transosseous repair to acromion; structured immobilization. |
| Hardware Penetration | 5% - 15% (Fractures) | Osteoporotic bone; varus collapse; incorrect initial screw length. | Hardware removal; revision ORIF with bone grafting; conversion to Arthroplasty (RTSA). |
| Avascular Necrosis | 10% - 30% (Complex Fractures) | Disruption of PCHA/ACHA; short metaphyseal head extension; medial hinge disruption. |
Clinical & Radiographic Imaging