Masterclass in Orthopaedic Surgical Techniques & Approaches
Key Takeaway
Mastering foundational orthopaedic surgical techniques is paramount for optimizing patient outcomes and minimizing perioperative complications. This comprehensive guide details evidence-based protocols for tourniquet application, intraoperative fluoroscopy, and precise patient positioning. By adhering to strict biomechanical principles and safety guidelines, orthopaedic surgeons can effectively mitigate risks such as post-tourniquet syndrome, radiation exposure, and positioning-related neuropathies, ensuring the highest standards of surgical excellence and patient care.
Comprehensive Introduction and Patho-Epidemiology
The mastery of orthopaedic surgery extends far beyond the mere mechanical execution of osteotomies or the deployment of internal fixation devices. It is fundamentally rooted in a profound biological respect for the soft tissue envelope, the meticulous preparation of the surgical environment, the strategic utilization of intraoperative adjuncts, and the uncompromising adherence to patient safety protocols. The modern orthopaedic surgeon must operate not merely as a carpenter of bone, but as a sophisticated architect of the musculoskeletal system, understanding that the biological environment dictates the ultimate success or failure of any mechanical construct. This masterclass delineates the critical surgical techniques that form the bedrock of operative orthopaedics, specifically focusing on the biomechanics of tourniquet application, the optimization of intraoperative imaging, the nuances of patient positioning, and the foundational principles of soft tissue and bone handling.
The patho-epidemiology of surgical complications in orthopaedics frequently underscores failures in these foundational principles rather than errors in definitive implant placement. Iatrogenic peripheral nerve injuries related to improper patient positioning or excessive tourniquet pressures account for a significant percentage of perioperative morbidity, with ulnar neuropathy at the cubital tunnel and common peroneal nerve palsy being the most frequently litigated positioning-related injuries. Furthermore, surgical site infections (SSIs), which carry an incidence of 1% to 2% in primary arthroplasties and up to 30% in severe open trauma, are heavily influenced by intraoperative soft tissue handling, hemostasis, and the duration of tourniquet-induced ischemia. Prolonged ischemia dramatically alters the local immune response, impairing macrophage function and decreasing tissue oxygen tension, which is a critical substrate for oxidative microbial killing by neutrophils.
Creating the optimal surgical environment requires a delicate balance between achieving a bloodless field for anatomical visualization and minimizing ischemic damage to the extremity. The historical evolution of orthopaedic surgery has been inextricably linked to the development of techniques that mitigate these risks. From the rudimentary and often catastrophic use of uncontrolled constrictive bands in the 19th century to the highly sophisticated, microprocessor-controlled pneumatic tourniquets of the modern era, the trajectory has always been toward maximizing efficacy while minimizing physiological insult. Similarly, the integration of intraoperative fluoroscopy has revolutionized minimally invasive techniques, yet it has introduced the insidious risk of cumulative radiation exposure, demanding rigorous adherence to safety protocols.
Ultimately, the foundational techniques discussed herein are not merely preliminary steps to the "main event" of the surgery; they are integral, continuous components of the procedure itself. A meticulously planned internervous approach, a perfectly calibrated tourniquet, and a flawlessly positioned patient collectively reduce operative time, minimize blood loss, lower the risk of infection, and accelerate postoperative rehabilitation. Mastery of these elements distinguishes the competent technician from the truly exceptional orthopaedic surgeon, ensuring that the intervention restores function without inflicting iatrogenic harm.
Detailed Surgical Anatomy and Biomechanics
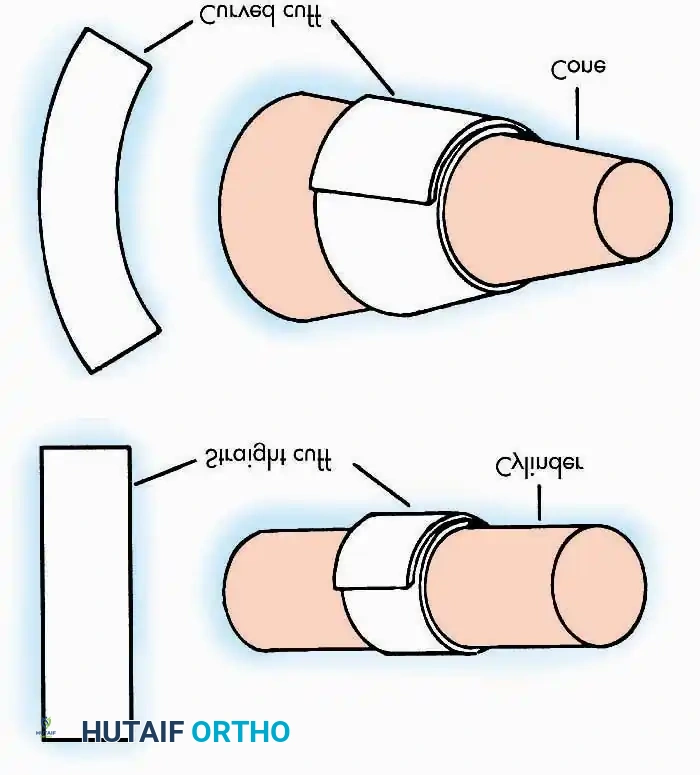
Operations on the extremities are profoundly facilitated by the use of a tourniquet, which provides a bloodless surgical field, enhances anatomical visualization, and expedites the procedure. However, the tourniquet is a potentially dangerous instrument that demands profound physiological understanding and meticulous care. The biomechanics of tourniquet application dictate that efficacy is a function of the relationship between cuff design, limb morphology, and applied pressure. Pedowitz et al. demonstrated that curved tourniquets applied to conical extremities require significantly lower arterial occlusion pressures compared to straight (rectangular) tourniquets. When a straight tourniquet is applied to a conical thigh, the pressure is unevenly distributed, concentrating dangerously on the proximal edge, which necessitates excessively high inflation pressures to achieve hemostasis, thereby exponentially increasing the risk of neurapraxia and skin sloughing.
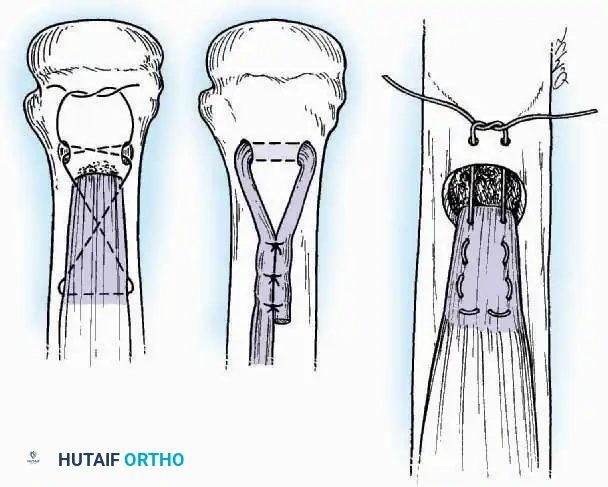
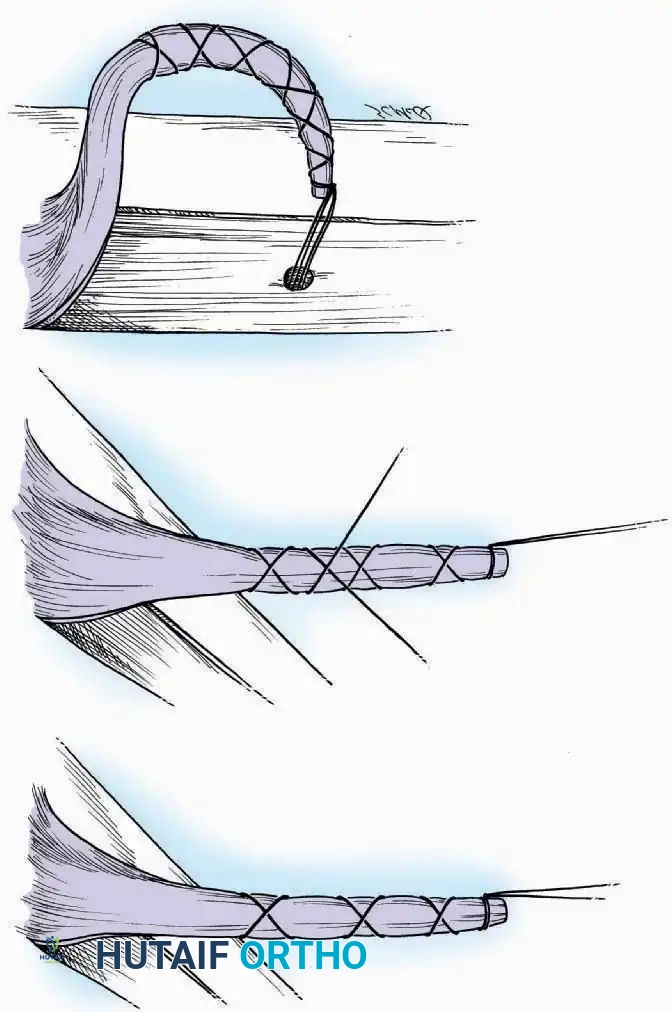
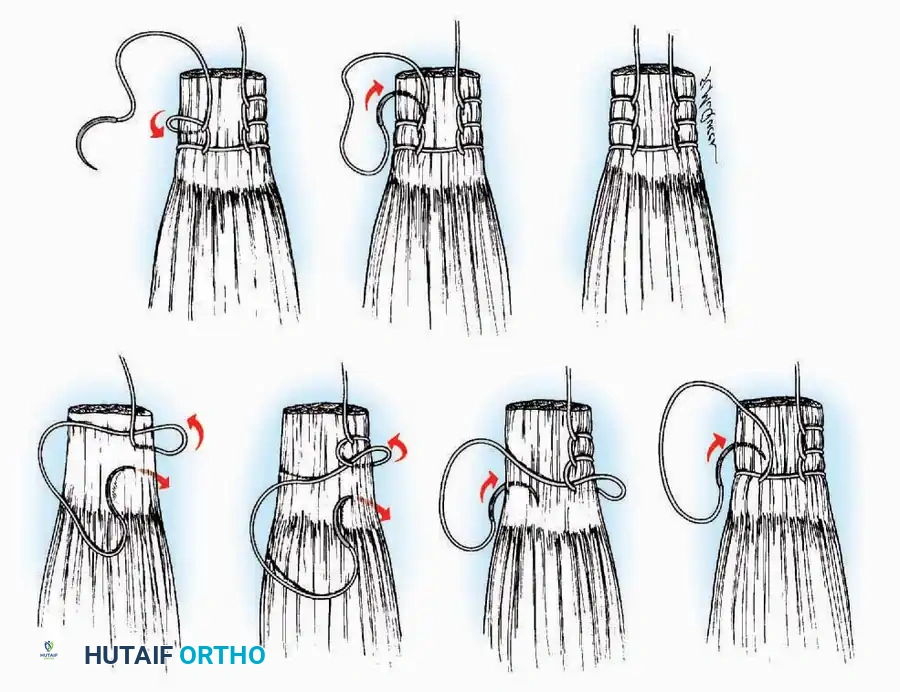
The biomechanics of soft tissue reconstruction and tendon repair rely heavily on the configuration of the suture within the collagenous matrix of the tendon. High-tensile, non-absorbable sutures are the standard, but the holding power is dictated by the suture's interaction with the longitudinal fibers. The Krackow suture, a continuous locking technique, provides exceptional grip by creating a series of interlocking loops that distribute tension across a broad surface area of the tendon, preventing the suture from pulling through the parallel collagen bundles under physiological loads. Conversely, the Bunnell and Kessler core sutures, utilized primarily in flexor tendon repairs of the hand, are biomechanically designed to bury the knot within the tendon interface, allowing smooth gliding through critical pulleys and synovial sheaths while maintaining sufficient tensile strength to permit early active mobilization.
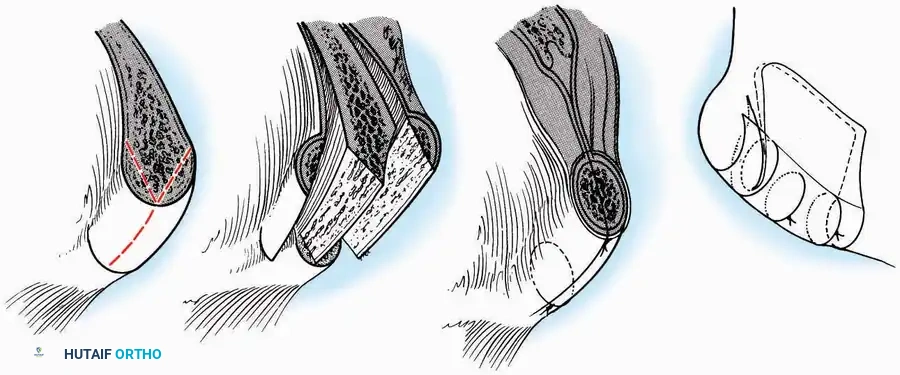
Bone grafting, a cornerstone of orthopaedic reconstruction, relies on three distinct biological and biomechanical properties: osteogenesis (the transfer of living osteoblasts and osteoprogenitor cells), osteoinduction (the provision of growth factors like Bone Morphogenetic Proteins that stimulate mesenchymal stem cell differentiation), and osteoconduction (the provision of a structural, porous scaffold for vascular and cellular ingrowth). Autogenous cancellous bone, harvested from the iliac crest or tibial metaphysis, remains the gold standard because it inherently possesses all three properties. The trabecular architecture of cancellous bone provides an immense surface area for rapid revascularization, which is critical for the survival of the transplanted osteocytes and the subsequent creeping substitution that integrates the graft into the host bed.
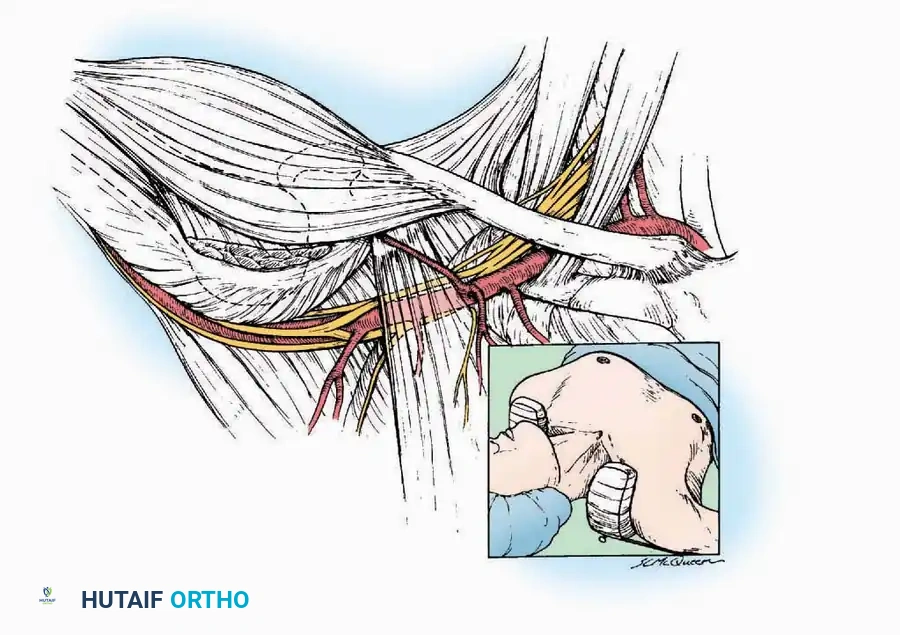
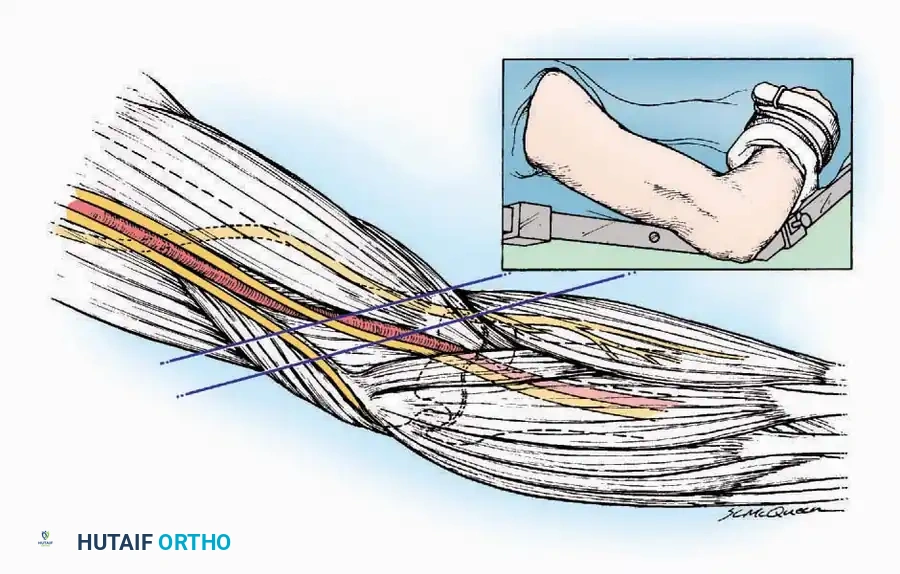
The fundamental philosophy of any orthopaedic approach is to reach the target pathology via the most direct route while inflicting minimal collateral damage to the surrounding soft tissue envelope. This is achieved by exploiting internervous planes—the avascular and areolar boundaries between muscles supplied by different peripheral nerves. By dissecting strictly within these planes, the surgeon ensures that neither adjacent muscle is denervated. For example, the anterior approach to the hip (Smith-Petersen) utilizes the true internervous plane between the sartorius (innervated by the femoral nerve) and the tensor fasciae latae (innervated by the superior gluteal nerve). Understanding the deep fascial compartments and the precise arborization of neurovascular bundles within these planes is the hallmark of anatomical mastery in orthopaedic surgery.
Exhaustive Indications and Contraindications
The decision to utilize specific foundational techniques, such as tourniquet application, specific patient positioning, or autologous bone grafting, must be individualized based on the patient's physiological status, the anatomical region, and the goals of the procedure. Pneumatic tourniquets are overwhelmingly indicated for procedures distal to the mid-thigh or mid-brachium where a bloodless field is critical for identifying microscopic neurovascular structures (e.g., hand surgery, nerve repairs) or where cement interdigitation requires a perfectly dry cancellous bone bed (e.g., total knee arthroplasty). However, their use is fraught with risks in patients with compromised vascular compliance or hypercoagulable states.
Bone graft selection similarly requires a rigorous assessment of indications. Autologous Iliac Crest Bone Graft (ICBG) is indicated for non-unions, massive cavitary defects, and complex arthrodeses where maximal biological activity (osteogenesis and osteoinduction) is required. However, the significant donor site morbidity associated with ICBG makes it relatively contraindicated in elderly patients with severe osteoporosis, where the harvest may precipitate an iliac wing fracture, or in patients with a history of chronic pelvic pain. In such scenarios, synthetic osteoconductive scaffolds combined with bone marrow aspirate concentrate (BMAC) or allograft may serve as appropriate alternatives.
Patient positioning is dictated by the surgical approach, but physiological contraindications often force the surgeon to adapt. Prone positioning, while essential for posterior spinal instrumentation and certain posterior approaches to the pelvis and lower extremity, severely alters pulmonary compliance and venous return. It is relatively contraindicated in patients with severe restrictive airway disease, massive obesity, or unstable cervical spines, necessitating alternative approaches such as the lateral decubitus position or specialized turning frames.
| Technique / Adjunct | Primary Indications | Relative Contraindications | Absolute Contraindications |
|---|---|---|---|
| Pneumatic Tourniquet | TKA, Hand/Foot surgery, Nerve/Tendon repair, Complex intra-articular fractures. | Severe obesity (conical limb), Mild peripheral vascular disease (PVD), History of DVT. | Sickle cell disease, Severe calcific PVD, Compartment syndrome, AV fistulas. |
| Autologous ICBG | Atrophic non-unions, Spinal fusion, Large cavitary defects, Joint arthrodesis. | Osteoporosis, Chronic pelvic pain, Previous harvest from the same site. | Active local infection at the donor site, Severe coagulopathy. |
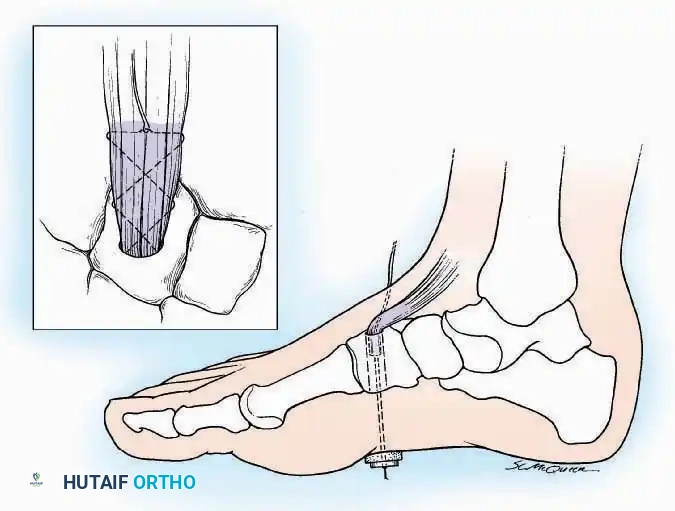
| Prone Positioning | Posterior spine surgery, Posterior acetabular approaches, Achilles tendon repair. | Morbid obesity, Moderate pulmonary disease, Advanced pregnancy. | Unstable cervical spine fracture, Severe restrictive airway disease, Increased ICP. |
| Lateral Decubitus | Total hip arthroplasty (posterior approach), Shoulder arthroscopy, Lateral pelvic approaches. | Severe scoliosis (makes pelvic registration difficult), Contralateral shoulder pathology. | Unstable pelvic ring injuries (if not stabilized), Severe cardiopulmonary instability. |
Pre-Operative Planning, Templating, and Patient Positioning
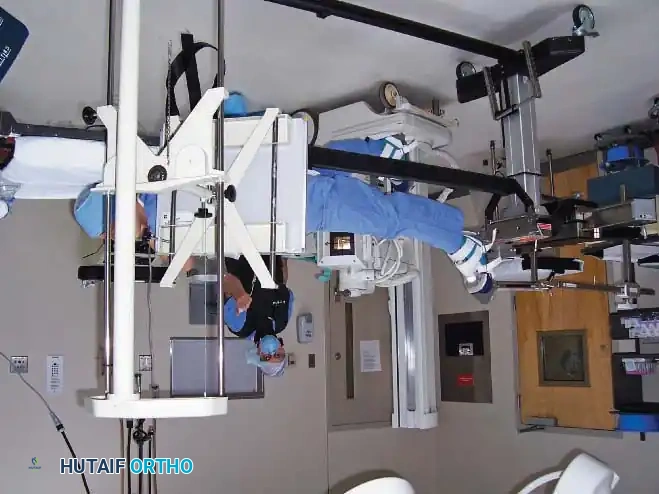
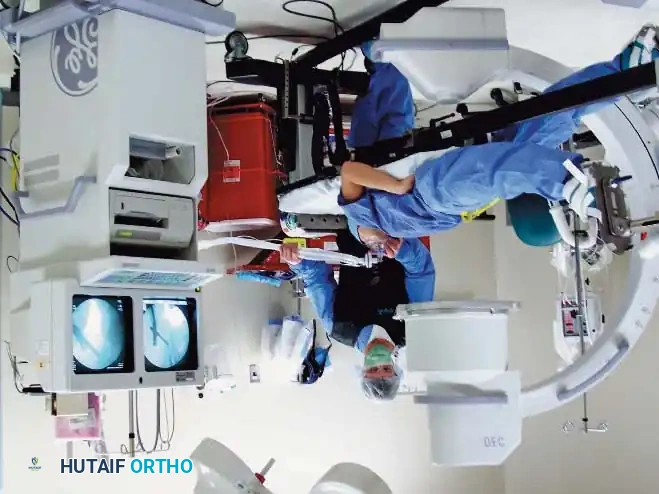
Pre-operative planning is the cognitive rehearsal of the surgical procedure, encompassing digital templating, equipment optimization, and the meticulous orchestration of the operating room layout. Orthopaedic surgery relies heavily on real-time intraoperative imaging to assess fracture reduction, implant trajectory, and joint congruency. The integration of portable radiographs and C-arm image intensifiers requires strict adherence to aseptic technique and radiation safety. When planning for continuous fluoroscopy, the C-arm must be meticulously draped, and the room must be configured to allow free rotation of the C-arm from anteroposterior (AP) to lateral planes without compromising the sterile field. The surgeon and scrub nurse must coordinate the movement of the machine, ensuring the unsterile base never breaches the sterile boundaries.


Patient positioning is a critical, highly vulnerable phase of the operation. Before the patient is anesthetized, the surgeon must verify and mark the surgical site to prevent "wrong-site" surgery. In the supine position, which is utilized for anterior approaches to the hip, knee, and upper extremity, the sacrum, heels, and occiput must be well padded to prevent decubitus ulcers. The arms should be abducted no more than 90 degrees to prevent traction injuries to the brachial plexus. A common pitfall is the compression of the ulnar nerve at the cubital tunnel; if the arm is hyperflexed or rests against the hard edge of the armboard, severe neurapraxia can occur. The forearm must be supinated or maintained in a neutral position to offload the ulnar nerve.

Prone positioning requires meticulous attention to respiratory mechanics and ocular pressure. Firm chest rolls extending from the clavicles to the iliac crests are essential to allow free abdominal excursion during ventilation and to decrease inferior vena cava compression. This offloading of the abdomen is critical, as increased intra-abdominal pressure translates to epidural venous engorgement, leading to profuse bleeding during spine surgery. The head must be supported in a neutral position using a specialized foam face block or Mayfield tongs, ensuring absolutely no pressure is placed on the globes of the eyes to prevent devastating ischemic optic neuropathy.
When the patient is placed in the lateral decubitus position, an axillary roll must be placed just caudal to the dependent axilla—not directly in it—to protect the dependent brachial plexus and allow adequate chest excursion. The common peroneal nerve is particularly vulnerable as it wraps superficially around the fibular neck of the dependent leg. Copious padding must be placed between the knees and under the lateral aspect of the dependent fibula to prevent compression neuropathy. The pelvis must be rigidly secured with anterior and posterior positioners to prevent shifting during reaming or impaction, which could alter the surgeon's perception of version and inclination.

Step-by-Step Surgical Approach and Fixation Technique
The execution of the surgical procedure begins with the precise application of the tourniquet, if indicated. In obese patients, achieving a stable tourniquet position is challenging due to the conical shape of the adipose tissue. The Krackow maneuver is employed: an assistant manually grasps the soft tissue distal to the tourniquet site and pulls it distally while the padding and cuff are applied. Upon release, the bulky subcutaneous tissue retracts proximally, acting as a mechanical buttress that prevents the tourniquet from slipping distally during inflation. Prior to inflation, the limb must be exsanguinated by elevating the extremity for 2 minutes or applying a sterile Esmarch bandage from the digits proximally. The pressure is then set using the Limb Occlusion Pressure (LOP) protocol, adding a safety margin (+40 to +80 mm Hg depending on the baseline LOP) to ensure complete arterial occlusion without excessive crushing force.
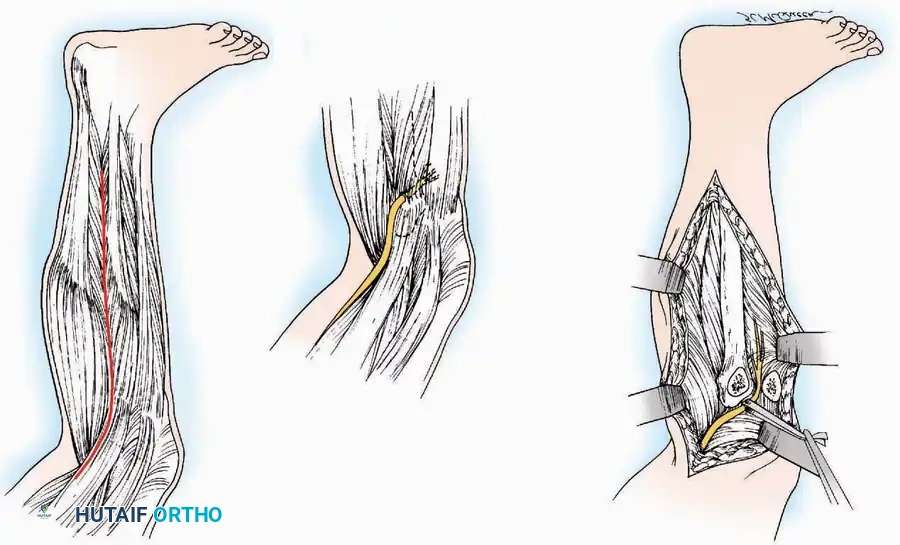
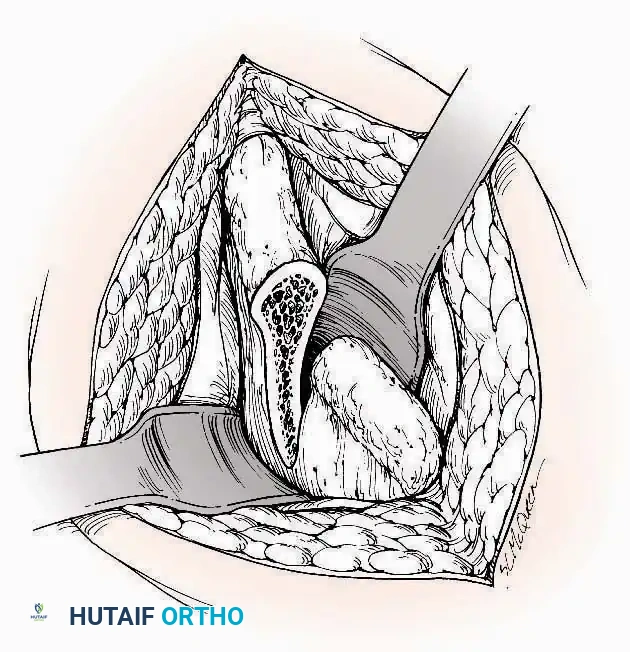
The surgical approach must rigorously respect internervous planes and local vascular angiosomes. Following the skin incision, full-thickness fasciocutaneous flaps are developed to preserve the subdermal vascular plexus. As the deep fascia is incised, the surgeon identifies the areolar tissue marking the internervous plane. Blunt dissection, aided by precise electrocautery, separates the muscle bellies. Retractors must be placed carefully, ensuring they rest on bone rather than crushing muscle tissue or tethering neurovascular bundles. For example, during an anterior hip approach, the ascending branches of the lateral circumflex femoral artery must be identified and meticulously ligated as they cross the operative field between the sartorius and tensor fasciae latae.
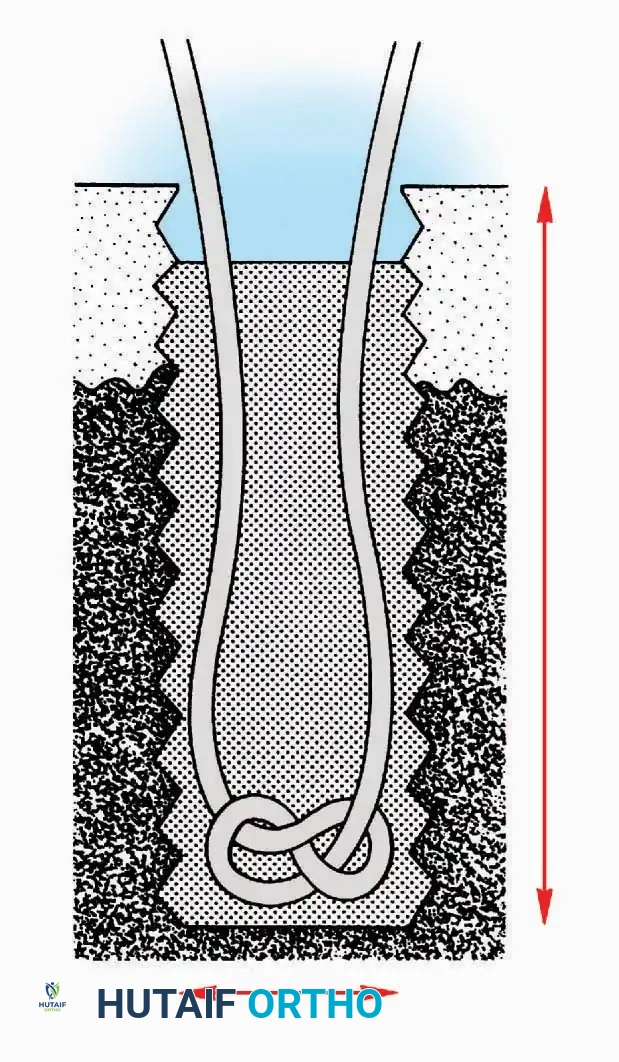
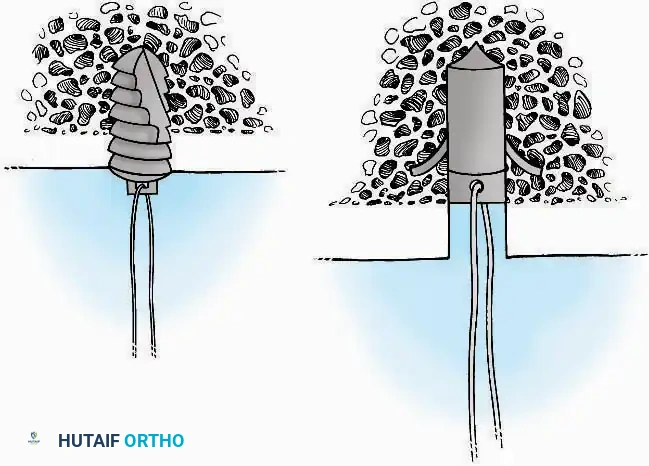
When soft tissue or tendon fixation is required, the bone surface must be meticulously prepared. The cortex is decorticated using a burr or osteotome to expose a bleeding cancellous bed, which provides the necessary pluripotential cells for osteointegration. If utilizing staple or anchor fixation, the hardware must be deployed perpendicular to the bone surface. Barbed staples must be driven symmetrically to ensure uniform compression of the tendon footprint against the bone, while suture anchors must be seated deep enough to prevent articular impingement but shallow enough to maintain optimal pull-out strength in the subchondral bone.
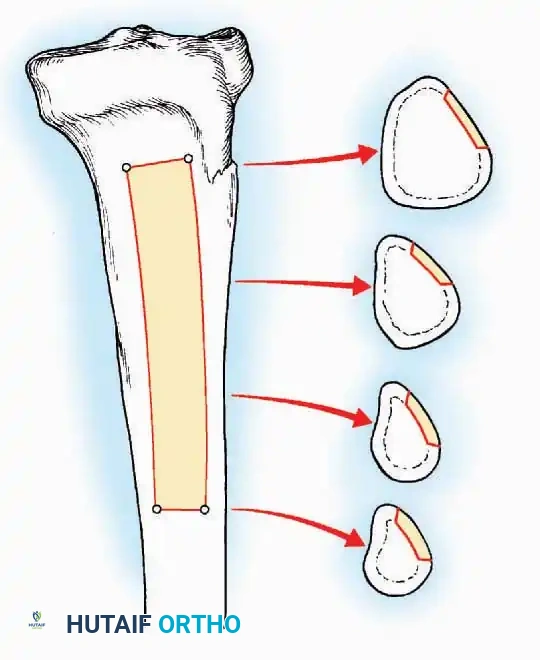
Autogenous bone grafting requires precise harvesting techniques to maximize yield while minimizing morbidity. For tibial bone grafting, a cortical window is created in the proximal or distal metaphysis. Curettes are sequentially utilized to harvest the underlying cancellous matrix, taking extreme care to avoid compromising the structural integrity of the subchondral bone supporting the tibial plateau or the ankle mortise.
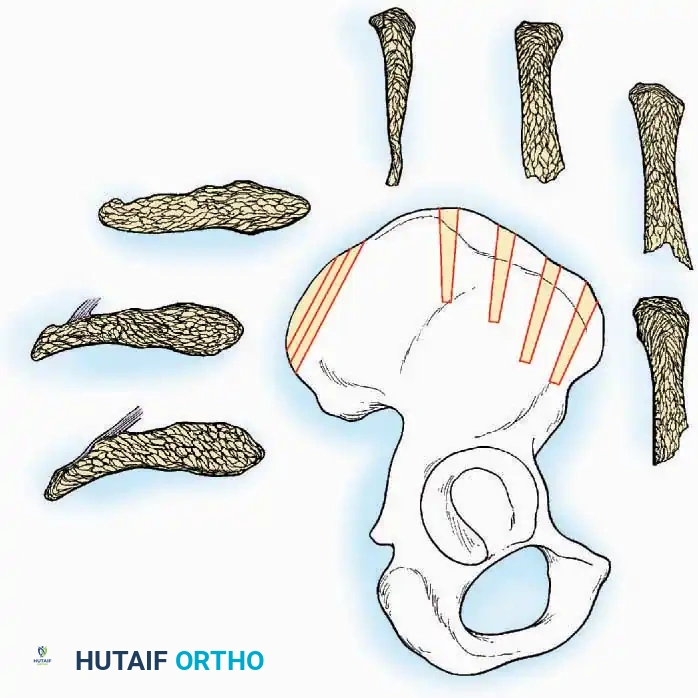
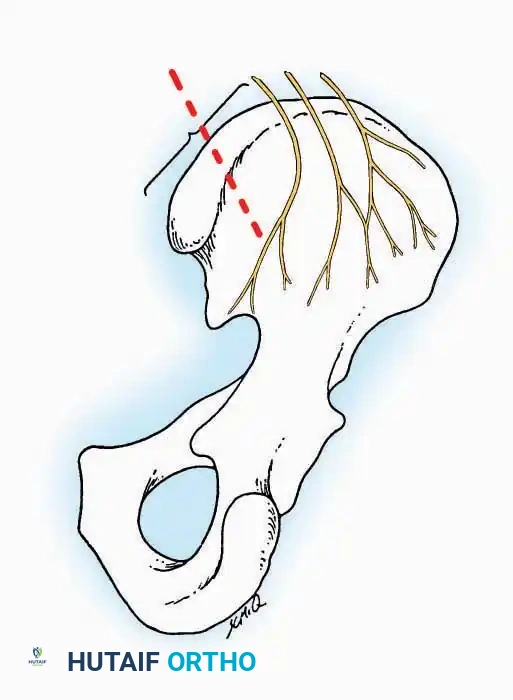
When harvesting from the anterior iliac crest, the incision is made parallel to the crest, staying at least 2 cm posterior to the Anterior Superior Iliac Spine (ASIS) to prevent avulsion fractures of the sartorius origin and to protect the Lateral Femoral Cutaneous Nerve (LFCN). For posterior harvests, dissection is limited to within 8 cm of the Posterior Superior Iliac Spine (PSIS) to avoid devastating injury to the superior cluneal nerves and the sacroiliac joint.



During deep dissection, neurovascular structures must be identified, mobilized, and protected. Vessel loops should be used to gently retract nerves. Excessive traction must be avoided, as peripheral nerves are highly sensitive to ischemic stretch injuries. The vasa nervorum can be disrupted by as little as 8% elongation, leading to transient or permanent neurapraxia. Meticulous hemostasis is paramount before closure to prevent postoperative hematoma formation, which serves as a nidus for infection and increases tension on the incision.

Complications, Incidence Rates, and Salvage Management
Despite meticulous adherence to surgical principles, complications inherent to these foundational techniques can occur. Tourniquet-related complications are primarily driven by the duration of ischemia and the magnitude of applied pressure. Post-Tourniquet Syndrome, characterized by profound edema, pallor, joint stiffness, motor weakness, and subjective numbness, occurs in up to 10% of cases where ischemia exceeds 2 hours. This is a manifestation of ischemia-reperfusion injury, where the sudden reintroduction of oxygenated blood triggers a massive release of reactive oxygen species (ROS), leading to lipid peroxidation, increased capillary permeability, and microvascular congestion. Salvage management involves aggressive elevation, cryotherapy, and in severe cases, fasciotomy if compartment syndrome ensues.
Positioning neuropathies represent a devastating and highly litigious complication. Ulnar neuropathy at the elbow occurs in approximately 0.5% of all general anesthetics, while common peroneal nerve palsy in the lateral decubitus position occurs in up to 1% of cases if padding is inadequate. These injuries are typically neurapraxic, resulting from focal demyelination due to mechanical compression and local ischemia of the vasa nervorum. Management is initially expectant, utilizing orthotics (e.g., AFO for foot drop) and physical therapy to prevent contractures. Electromyography (EMG) is indicated at 6 weeks if no clinical improvement is observed, and surgical neurolysis may be required for refractory cases demonstrating severe axonal loss.
Bone graft harvest morbidity is a significant deterrent to the use of autograft. Iliac crest harvests carry a complication rate of up to 15%, including chronic donor site pain, hematoma, pelvic fractures, and nerve injuries. Injury to the Lateral Femoral Cutaneous Nerve (LFCN) during anterior harvests results in meralgia paresthetica, a painful dysesthesia over the anterolateral thigh. Herniation of abdominal contents through a full-thickness iliac crest defect is a rare but catastrophic complication requiring urgent general surgical repair. Salvage management for chronic donor site pain often involves prolonged pain management, localized corticosteroid injections, and occasionally, surgical denervation.
Radiation exposure to the orthopaedic surgeon is a cumulative, lifelong occupational hazard. Failure to adhere to the ALARA (As Low As Reasonably Achievable) principle can lead to radiation-induced cataracts, thyroid dysfunction, and radiodermatitis. The incidence of cataracts among orthopaedic surgeons is significantly higher than in the general population. Management is strictly preventative: utilizing lead shielding (minimum 0.35 mm lead equivalence), maximizing distance from the source (inverse square law), and positioning the x-ray tube under the operating table to minimize scatter radiation to the surgeon's upper body and eyes.
| Complication | Incidence Rate | Primary Etiology | Salvage / Management Protocol |
|---|---|---|---|
| Post-Tourniquet Syndrome | 5% - 10% (Ischemia > 2 hrs) | Ischemia-reperfusion injury, ROS release, microvascular congestion. | Elevation, cryotherapy, NSAIDs, monitor for compartment syndrome. |
| Ulnar Neurapraxia | ~0.5% of supine cases | Direct compression at cubital tunnel, arm hyperflexion. | Expectant observation, night splinting, EMG at 6 weeks, neurolysis if refractory. |
| Meralgia Paresthetica | 2% - 5% of Anterior ICBG | Iatrogenic injury/traction to the Lateral Femoral Cutaneous Nerve. | Gabapentinoids, local anesthetic/steroid blocks, surgical neurectomy for severe cases. |
