Mastering Interfascicular Nerve Grafting and Perineurial Neurorrhaphy
Key Takeaway
Interfascicular nerve grafting is a microsurgical technique utilized to bridge segmental peripheral nerve defects without tension. By utilizing multiple cutaneous nerve grafts, surgeons can precisely align proximal and distal fascicles, mitigating intraneural fibrosis. This technique is indicated for massive nerve gaps, brachial plexus reconstruction, and free functional muscle transfers, requiring meticulous fascicular mapping and tension-free coaptation to optimize motor and sensory recovery.
Comprehensive Introduction and Patho-Epidemiology
The reconstruction of peripheral nerve injuries with significant segmental defects remains one of the most technically demanding and biologically complex challenges in operative orthopaedics, hand surgery, and microsurgery. While primary end-to-end repair (epiperineurial neurorrhaphy) is universally recognized as the gold standard for acute, sharp nerve transections presenting with minimal gap, the reality of major trauma dictates that secondary repair is frequently required. These secondary reconstructions are invariably complicated by longitudinal nerve retraction, extensive neuroma-in-continuity formation, and significant segmental soft tissue and neural defects resulting from the initial high-energy trauma or subsequent surgical debridement.
The pathophysiology of a transected peripheral nerve initiates a profound cascade of cellular and biochemical events. Distal to the injury site, the nerve undergoes Wallerian degeneration, a process characterized by the axonal cytoskeleton's breakdown, myelin sheath clearance by recruited macrophages, and the proliferation of Schwann cells that form the bands of Büngner. These bands serve as the critical biological conduits for future regenerating axons. Proximally, the neuron's cell body undergoes chromatolysis, shifting its metabolic machinery from neurotransmitter production to the synthesis of structural proteins required for axonal elongation. The race against time in nerve reconstruction is fundamentally a race against the irreversible fibrosis of the distal motor endplates and sensory receptors, which typically occurs within 18 to 24 months post-injury.
Experimental and clinical evidence unequivocally demonstrates that tension across a nerve repair site is the single most detrimental biomechanical and physiological factor affecting functional outcomes. Tension induces intraneural ischemia by stretching and obliterating the longitudinal microvascular networks within the epineurium and perineurium. Furthermore, tension disrupts the delicate microvascular blood-nerve barrier, leading to intraneural edema, and stimulates aggressive intraneural fibrosis. This fibrotic response effectively creates an impenetrable physical barrier, blocking axonal regeneration and resulting in a painful, non-functional neuroma.
To circumvent the catastrophic effects of tension at the coaptation site, Hanno Millesi pioneered the paradigm-shifting technique of interfascicular nerve grafting in the early 1970s. By abandoning the historical practice of extreme joint flexion to achieve primary approximation—a practice doomed to failure upon subsequent joint mobilization—Millesi introduced the concept of utilizing multiple cutaneous nerve grafts. This technique allows for the precise, absolutely tension-free alignment of corresponding fascicles between the proximal and distal nerve stumps. When executed with rigorous microsurgical principles, interfascicular grafting has been utilized successfully to bridge massive nerve gaps exceeding 20 cm, restoring critical motor and sensory function in otherwise devastating limb injuries.
Detailed Surgical Anatomy and Biomechanics
Understanding the intricate internal topography and microanatomy of peripheral nerves is paramount for any surgeon undertaking interfascicular grafting. A peripheral nerve is not a homogenous, static cable but rather a highly complex, dynamic, and metabolically active structure composed of distinct neural and connective tissue compartments. The functional unit of the nerve is the axon, which is individually enveloped by the endoneurium, a delicate layer of connective tissue matrix and Schwann cells. Multiple axons are bundled together to form fascicles, which are tightly bound by the perineurium.
The perineurium is a remarkably strong, multilayered structure composed of specialized perineurial cells and dense collagen fibrils. It serves two critical functions: it provides the primary tensile strength of the peripheral nerve, and it forms the selectively permeable blood-nerve barrier, maintaining the specialized endoneurial fluid environment required for action potential propagation. Fascicles are subsequently grouped together and protected by the internal epineurium, a loose connective tissue that acts as a gliding layer and shock absorber. The entire nerve trunk is then ensheathed by the external epineurium, which condenses from the surrounding mesoneurium and carries the extrinsic segmental blood supply.
The internal topography of fascicles changes dramatically along the longitudinal course of the nerve. In the proximal segments of major mixed nerves (such as the sciatic nerve in the thigh or the proximal median nerve in the arm), fascicular topography is highly plexiform. In these regions, fascicles frequently divide, merge, and intertwine, making the isolation of specific motor or sensory groups exceedingly difficult. Distally, as the nerve approaches its target end-organs, the topography becomes parallel and distinct, segregating into specific, identifiable motor and sensory fascicular groups. The fundamental goal of interfascicular grafting is to accurately map these groups and bridge them with corresponding grafts, thereby minimizing axonal misdirection—often termed cross-innervation—which leads to poor functional recovery and debilitating synkinesis.
Biomechanically, peripheral nerves are designed to accommodate the substantial excursions required during normal joint movement. This is facilitated by the redundancy of the axons within the endoneurium (the bands of Fontana) and the gliding planes provided by the mesoneurium. However, the tolerance for longitudinal strain is remarkably low. Classic microvascular studies by Lundborg and others have demonstrated that elongation of a peripheral nerve by a mere 8% to 10% results in complete cessation of intraneural venular flow, while elongation beyond 15% causes complete arterial ischemia and structural failure of the perineurial tubes. These biomechanical absolutes underscore why interfascicular grafting, which restores continuity without exceeding these critical strain thresholds, remains the definitive solution for segmental defects.
Exhaustive Indications and Contraindications
The decision to proceed with interfascicular nerve grafting requires advanced microsurgical experience, specialized instrumentation, and meticulous preoperative planning. The procedure is not a panacea for all nerve injuries and must be applied judiciously based on the specific characteristics of the injury, the patient's physiological status, and the anticipated timeline for reinnervation. The primary indication remains the reconstruction of nerve gaps following segmental injury, delayed presentation, or neuroma resection where a primary epiperineurial neurorrhaphy cannot be performed without inducing tension.
Beyond traumatic segmental defects, interfascicular grafting is frequently employed in the complex arena of nerve transfer surgery (neurotization). In severe brachial plexus avulsion injuries, where proximal nerve roots are unavailable, grafts are utilized to bridge the distance between a healthy donor nerve (e.g., routing an intercostal nerve or the spinal accessory nerve) and a critical recipient nerve (e.g., the musculocutaneous nerve for elbow flexion). Furthermore, nerve grafts are essential components in free functional muscle transfers (FFMT). For example, in a gracilis transfer for long-standing facial palsy or global brachial plexus reconstruction, a cross-facial nerve graft or a supraclavicular graft is often required to provide the necessary neural input to the transferred muscle's obturator nerve.
Contraindications to interfascicular nerve grafting are primarily dictated by the biological environment of the recipient bed and the temporal limits of motor endplate viability. A heavily scarred, avascular, or actively infected soft tissue bed is an absolute contraindication, as the non-vascularized nerve graft relies entirely on plasmatic imbibition from the surrounding tissues for the first 3 to 5 days prior to neovascularization. Placing a graft in a fibrotic bed guarantees central graft necrosis and failure. Additionally, attempting to graft a motor nerve when the anticipated time for regenerating axons (growing at approximately 1 mm/day) to reach the target muscle exceeds 18 to 24 months is generally futile due to irreversible motor endplate fibrosis and muscle atrophy.
| Clinical Parameter | Primary Indications for Interfascicular Grafting | Absolute or Relative Contraindications |
|---|---|---|
| Defect Size | Segmental gaps > 2.0 - 2.5 cm after adequate neuroma resection. | Gaps < 2.0 cm that can be mobilized for tension-free primary repair. |
| Injury Timing | Delayed presentations (weeks to months) with nerve retraction. | Massive delay (>18-24 months) for motor targets (irreversible atrophy). |
| Soft Tissue Bed | Well-vascularized, healthy muscle or subcutaneous tissue bed. | Heavily irradiated, fibrotic, avascular, or actively infected beds. |
| Reconstructive Type | Bridging nerve transfers, Free Functional Muscle Transfers (FFMT). | Severe, uncorrectable joint contractures distal to the nerve injury. |
| Patient Factors | Compliant patient capable of adhering to strict post-op protocols. | Severe malnutrition, active smoking (relative), uncontrolled diabetes. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative evaluation and meticulous planning are the cornerstones of successful interfascicular nerve grafting. The clinical examination must precisely document the extent of motor and sensory deficits, utilizing the Medical Research Council (MRC) grading system for motor power and standardized sensory testing (e.g., static and moving two-point discrimination, Semmes-Weinstein monofilaments). The advancement of a Tinel sign should be carefully mapped, as an arrested Tinel sign over several months is highly indicative of a dense neuroma-in-continuity that will require resection and grafting.
Electrodiagnostic studies, including Electromyography (EMG) and Nerve Conduction Studies (NCS), are critical adjuncts. These studies should ideally be obtained no earlier than 3 to 4 weeks post-injury to allow for complete Wallerian degeneration, ensuring accurate assessment of the injury's severity (axonotmesis vs. neurotmesis). Advanced neuroimaging, specifically High-Resolution Ultrasound (HRUS) and Magnetic Resonance Neurography (MRN), has revolutionized preoperative templating. These modalities allow the surgeon to visualize the exact length of the neuroma, the degree of fascicular disruption, and the longitudinal extent of the segmental defect before the first incision is made, facilitating precise planning for donor nerve harvest.
Donor nerve selection is a critical preoperative decision. The sural nerve remains the workhorse donor for interfascicular grafting, capable of providing up to 30 to 40 cm of graft material. It possesses an excellent fascicular architecture that closely mimics the fascicular groups of major mixed nerves in the upper extremity. Alternative donor sites include the medial antebrachial cutaneous (MABC) nerve, the lateral antebrachial cutaneous (LABC) nerve, and the terminal branch of the posterior interosseous nerve (PIN). The choice of donor depends on the required length, the necessary cross-sectional area to match the recipient fascicles, and the patient's tolerance for the specific donor site morbidity (e.g., lateral foot numbness for the sural nerve).
Patient positioning and operating room setup must be optimized for microsurgery. The patient is typically positioned supine with the affected limb extended on a radiolucent hand table. A pneumatic tourniquet is applied to ensure a strictly bloodless field during the initial dissection and neuroma resection. The operative microscope (e.g., Zeiss or Leica models) must be balanced and positioned to allow ergonomic, high-magnification viewing for both the primary surgeon and the assistant. Microsurgical instrumentation—including jeweler's forceps, microscissors, diamond knives, and specialized nerve approximators—must be meticulously inspected and prepared prior to the commencement of the procedure.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of the modified Millesi approach for interfascicular nerve grafting demands absolute precision, patience, and adherence to atraumatic microsurgical principles. The procedure is typically performed under general anesthesia or regional blockade, depending on the necessity for intraoperative awake nerve stimulation.
Exposure and Preparation of the Nerve Stumps
The initial approach requires extensile exposure. Brunner-type zigzag or generous longitudinal incisions that cross flexion creases obliquely are utilized. This prevents postoperative scar contracture directly over the delicate repair site. The fundamental principle of nerve dissection is to identify the nerve trunk in virgin, unscarred tissue both proximally and distally before tracing it toward the dense zone of injury. Dissection is performed under loupe magnification initially, utilizing a bloodless field achieved with a pneumatic tourniquet.
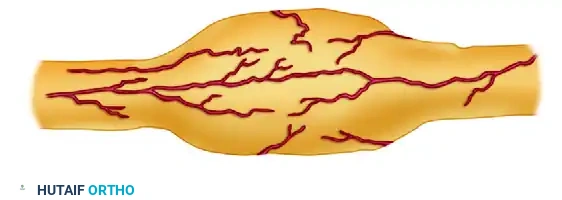
Figure 1: External appearance of the neuroma-in-continuity or end-bulb neuroma prior to resection.
Epineurectomy and Neuroma Resection
Once the zone of injury is isolated, the external epineurium is incised proximal to the neuroma in normal-appearing tissue. The epineurium is carefully peeled back, reflecting it toward the scarred stump to expose the underlying fascicular bundles. This process is repeated on the distal stump, which often presents as a glioma—a disorganized, fibrotic mass of Schwann cells lacking viable axonal conduits. The neuroma and glioma are then sequentially resected using a fresh neurosurgical blade or a diamond knife. Resection continues millimeter by millimeter until healthy, pouting fascicles—demonstrating the classic "mushrooming" effect—are visualized under the high-power operating microscope.

Figure 2: Neuroma and epineurium excised to expose fascicles of different lengths, depending on the extent of their involvement in the scar tissue.
Fascicular Mapping and Step-Cutting
Under the operating microscope, the major fascicle groups are identified and followed longitudinally to the point where they become obscured by intraneural scarring. These groups are then transected at different levels depending on the extent of scar involvement, creating a "step-cutting" geometry. This differential transection is critical; it prevents the multiple nerve grafts from clumping together, distributes the bulk of the coaptation sites over a wider area, and minimizes cross-scarring between adjacent grafts. Topographical matching is then performed. The distal stump is explored to identify its terminal branches (e.g., motor vs. sensory), and these groups are traced proximally to map the corresponding fascicles accurately.
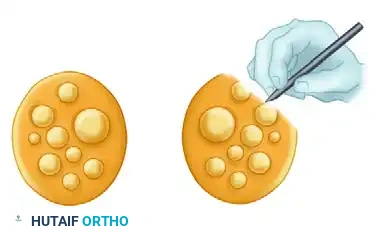
Figure 3: After dissection of the scar, the cut ends of the nerve are held in alignment, demonstrating the matching of corresponding proximal and distal fascicles prior to graft interposition.
Graft Harvesting and Preparation
Once the exact length of the required nerve graft is measured, the tourniquet must be deflated. Absolute hemostasis is mandatory before graft inset; even a microscopic hematoma will act as a physical barrier to regenerating axons and promote aggressive fibrosis. The chosen donor nerve (typically the sural nerve) is harvested using a minimally invasive step-incision technique or an endoscopic harvester to minimize scarring. The harvested nerve is then sectioned into segments approximately 10% to 15% longer than the measured defect. This excess length accounts for inevitable graft shrinkage and ensures absolute tension-free coaptation, even during full joint excursion.
Microsurgical Coaptation
The final and most delicate phase is the microsurgical inset of the grafts. The nerve grafts are placed between the corresponding proximal and distal fascicular groups. Crucially, the grafts must be reversed in orientation (the distal end of the graft is sutured to the proximal nerve stump). This reversal minimizes axonal escape through small cutaneous branching points inherent to the donor nerve. Coaptation is performed using 9-0 or 10-0 monofilament nylon sutures on a spatulated micro-needle. Sutures are placed strictly through the perineurium or the robust interfascicular epineurium. Typically, only one to three sutures per graft are required to maintain perfect alignment. Fibrin tissue adhesive may be applied judiciously to the periphery of the repair to augment stability, provided extreme care is taken to ensure the glue does not interpose between the axonal interfaces.
Complications, Incidence Rates, and Salvage Management
Despite meticulous microsurgical technique, interfascicular nerve grafting carries a significant risk profile. The long distances that regenerating axons must traverse, combined with the biological hurdles of two coaptation sites (proximal and distal), make complications a reality that the reconstructive surgeon must anticipate and manage effectively.
The most devastating complication is central graft necrosis and subsequent failure of regeneration. This typically occurs when the graft is placed into a poorly vascularized, heavily scarred bed. Because the free nerve graft relies on plasmatic imbibition for survival prior to neovascularization, an ischemic bed leads to rapid fibrotic replacement of the endoneurial tubes. Neuroma-in-continuity at the proximal coaptation site is another frequent complication, occurring in up to 10-15% of cases. This is usually the result of inadequate initial neuroma resection (leaving scarred fascicles), excessive tension on the repair, or hematoma formation. Clinically, this presents as a halted Tinel sign, localized neuropathic pain, and a failure of distal motor or sensory recovery.
Donor site morbidity, while often downplayed, can be a significant source of patient dissatisfaction. Harvest of the sural nerve universally results in numbness over the lateral aspect of the foot and ankle. More problematically, up to 5-8% of patients may develop a painful, hypersensitive neuroma at the proximal transection site of the donor nerve. Joint stiffness and capsular contracture represent a major secondary complication, arising from the delicate balance required between protecting the nerve repair with immobilization and initiating early movement to preserve joint mechanics.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Graft Necrosis / Failure | 5% - 15% | Avascular bed, hematoma, infection, graft too thick. | Debridement, vascularized nerve graft, tendon transfers, or FFMT. |
| Neuroma-in-Continuity | 10% - 20% | Inadequate resection, tension, poor fascicular matching. | Re-exploration, intraoperative nerve monitoring, revision grafting. |
| Donor Site Neuroma | 5% - 8% | Superficial placement of the proximal donor nerve stump. | Excision and transposition of the stump deep into adjacent muscle belly. |
| Joint Stiffness / Contracture | 15% - 25% | Prolonged immobilization (>3-4 weeks), lack of therapy. | Aggressive hand therapy, dynamic splinting, surgical capsulotomy. |
| Synkinesis (Cross-Innervation) | Variable | Inaccurate fascicular mapping, plexiform nerve topography. | Targeted motor re-education, biofeedback, selective botulinum toxin. |
When interfascicular grafting fails, or when the patient presents too late for nerve reconstruction (beyond the 18-24 month window for motor endplate viability), salvage procedures must be employed. Tendon transfers remain the primary salvage modality, utilizing expendable, innervated muscle-tendon units to restore critical functions (e.g., the classic Boyes or Jones transfers for radial nerve palsy). In cases where local tendon transfers are unavailable due to global deficits, Free Functional Muscle Transfers (such as a gracilis innervated by an intercostal nerve or spinal accessory nerve) are utilized to restore gross limb function.
Phased Post-Operative Rehabilitation Protocols
The postoperative management of an interfascicular nerve graft is as critical to the ultimate functional outcome as the microsurgical execution itself. The rehabilitation protocol must be meticulously phased to protect the delicate coaptation sites during the initial healing phase, while progressively restoring joint mobility, preventing contractures, and facilitating the complex process of sensory and motor cortical reeducation.
Phase 1: Strict Immobilization (Weeks 0 to 3)
Immediately following wound closure, a bulky, non-compressive plaster splint is applied in the operating room. For nerve repairs in the hand, wrist, or forearm, the splint is strategically placed to immobilize the involved joints in a neutral, absolutely tension-free position. This initial postoperative splinting is strictly maintained for 3 weeks. This critical period allows the fibrin clot at the coaptation site to organize, early collagen cross-linking to secure the graft, and neovascularization to commence. The patient is allowed only minimal active movement of the distal un-immobilized joints (e.g., finger joints if only the wrist is splinted) strictly within the physical limits of the splint to prevent extensor or flexor tendon adhesions.
Phase 2: Gradual Mobilization (Weeks 3 to 8)
After the initial 3-week period of absolute immobilization, the rigid plaster splint is removed, and the transition to gradual mobilization begins. If a joint was immobilized in slight flexion to accommodate a massive soft tissue defect (though tension on the nerve itself is avoided by the graft), it is gradually extended. The joint is brought first to a neutral position, and then to slight extension over the next 3 to 4 weeks. This gradual, controlled stretching prevents traction injury to the newly vascularizing nerve graft while positioning the limb for effective biomechanics. Between 4 to 8 weeks postoperatively, custom-molded, removable thermoplastic splints are fabricated by a specialized hand therapist. These allow for controlled hygiene and supervised active-assisted range of motion therapy sessions.
Phase 3: Contracture Prevention and Strengthening (Weeks 6 to 12)
As the graft solidifies, the focus shifts heavily toward the prevention of fixed joint contractures, which can severely compromise ultimate limb function even if nerve regeneration is biologically successful. Careful attention is paid to the thumb web space; patients are instructed in passive stretching, and a removable C-bar or web-spacer splint is applied at the first sign of an adduction contracture. In patients with intrinsic paralysis (e.g., high ulnar nerve injury), passive stretching of the fingers is mandatory to prevent metacarpophalangeal (MCP) joint extension contractures and proximal interphalangeal (PIP) joint flexion contractures. If a "claw" deformity develops, a custom MCP extension-blocking splint (lumbrical bar) is highly effective in redirecting extrinsic extensor force to extend the PIP joints. Progressive strengthening exercises for the innervated and recovering musculature are initiated cautiously around 8 to 12 weeks.
Phase 4: Sensory Reeducation and Monitoring
Clinical evaluations of motor and sensory return are conducted monthly. The surgeon meticulously tracks the advancing Tinel sign, which progresses at approximately 1 mm per day (or roughly 1 inch per month) after an initial latent period of 3 to 4 weeks. When the advancing Tinel sign reaches the target end-organs, and the patient demonstrates the appreciation of constant touch, moving touch, and vibratory perception (assessed using 30 Hz and 256 Hz tuning forks), formal sensory reeducation is initiated. The Dellon, Curtis, and Edgerton protocol is the gold standard for this phase. This structured reeducation program relies on neuroplasticity, helping the somatosensory cortex reinterpret the altered, often overlapping neural signals arriving from misdirected axons. It begins with early-phase reeducation (distinguishing moving versus constant touch) and progresses to late-phase reeducation (tactile gnosis, object identification without visual cues, and spatial orientation), maximizing the functional utility of the regenerated nerve.
Summary of Landmark Literature and Clinical Guidelines
The modern approach to interfascicular nerve grafting is built upon a foundation of landmark anatomical, biomechanical, and clinical studies. The paradigm shift away from tension-laden primary repairs was initiated by Hanno Millesi in his seminal papers published in the early 1970s. Millesi's clinical series definitively proved that bridging a gap with multiple, tension-free cutaneous nerve grafts yielded vastly superior motor and sensory recovery compared to end-to-end repairs performed under tension, even when the latter required extensive joint flexion and bone shortening.
The biomechanical rationale for Millesi's clinical findings was elucidated by Göran Lundborg and colleagues. Lundborg's elegant microvascular injection studies demonstrated the profound vulnerability of the intraneural microcirculation to longitudinal strain. His work established the "8% rule"—that elongation of a nerve by just 8% causes significant venular stasis, and 15% causes complete arterial ischemia. This foundational science cemented the absolute necessity of tension-free grafting techniques in modern microsurgery.
Further anatomical contributions by Sir Sydney Sunderland mapped the complex, changing internal topography of peripheral nerves. Sunderland's detailed cross-sectional studies highlighted the plexiform nature of proximal nerves and the parallel nature of distal nerves, forming the anatomical basis for modern fascicular mapping and the step-cutting techniques utilized to minimize cross-innervation.
Current clinical guidelines from the American Academy of Orthopaedic Surgeons (AAOS) and the American Society for Surgery of the Hand
