Orthopaedic Skin Grafts and Flaps: Surgical Techniques

Key Takeaway
Free skin grafts are fundamental in orthopaedic soft tissue reconstruction. The selection between split-thickness and full-thickness grafts dictates both graft survival and functional outcome. This guide details the biomechanical principles of graft contraction, precise dermatome harvesting techniques, and the application of tie-over bolster dressings to ensure optimal graft adherence and integration in complex musculoskeletal defects.
Comprehensive Introduction and Patho-Epidemiology
The management of complex musculoskeletal trauma frequently necessitates advanced soft tissue reconstruction, representing one of the most formidable challenges in orthopaedic surgery. The traditional reconstructive ladder dictates that wound coverage should be achieved using the simplest, most effective method that restores both form and function, progressing from secondary intention and primary closure to skin grafts, local flaps, and ultimately free tissue transfer. However, in contemporary orthopaedics, this paradigm has evolved into the "reconstructive elevator," where the surgeon bypasses intermediate steps to immediately select the optimal coverage modality that maximizes functional preservation. When primary closure is impossible due to massive tissue loss, free skin grafts and local flaps become indispensable, life-altering tools in the reconstructive surgeon’s armamentarium.
The patho-epidemiology of traumatic soft tissue defects is inextricably linked to high-energy mechanisms of injury, including motorcycle collisions, industrial crush injuries, agricultural avulsions, and ballistic trauma. These high-velocity impacts impart massive kinetic energy to the appendicular skeleton and its surrounding soft tissue envelope, resulting in the classic "zone of injury." This zone extends far beyond the macroscopic wound margins, encompassing microvascular thrombosis, cellular stunning, and an intense localized inflammatory cascade. The compromised soft tissue envelope is highly susceptible to progressive necrosis, rendering underlying fractures, tendons, and neurovascular bundles vulnerable to desiccation and devastating deep infections.
Following the initial trauma, a predictable physiological cascade of soft tissue deterioration ensues if definitive coverage is delayed. Ischemia-reperfusion injury exacerbates cellular death through the generation of reactive oxygen species, while the exposed, avascular planes become rapidly colonized by nosocomial pathogens. The Gustilo-Anderson classification of open fractures underscores this relationship: Type IIIB and IIIC injuries, characterized by extensive soft tissue stripping and periosteal devascularization, mandate flap coverage precisely because the local physiological environment cannot support a free skin graft or secondary healing. Consequently, the orthopaedic surgeon must possess a profound understanding of wound bed physiology to arrest this necrotic cascade.
The evolution of grafts and flaps in orthopaedics has transitioned from the historical reliance on random pattern flaps with unpredictable viability to the modern era of precision microsurgery, axial pattern flaps, and bioengineered dermal substitutes. The successful application of these techniques requires a profound understanding of skin biomechanics, vascular physiology, and meticulous surgical execution. This comprehensive guide explores the critical principles of free skin grafting, the precise utilization of dermatomes, the step-by-step application of split-thickness skin grafts (STSG), and the execution of advanced local reconstructive techniques, such as the filleted finger flap for severe hand trauma.
Detailed Surgical Anatomy and Biomechanics
A thorough mastery of cutaneous and neurovascular anatomy is the absolute prerequisite for successful orthopaedic soft tissue reconstruction. The skin is a highly specialized, bilayered organ consisting of the superficial epidermis and the deeper dermis. The epidermis is an avascular, stratified squamous epithelium that relies entirely on diffusion from the underlying dermal capillary beds. The dermis itself is subdivided into the superficial papillary dermis, rich in capillary loops and loose connective tissue, and the deeper reticular dermis, which contains a dense, interwoven network of thick collagen and elastin fibers. The biomechanical properties of a skin graft—specifically its durability, pliability, and resistance to shear—are directly proportional to the amount of reticular dermis included in the harvest.
The vascular anatomy of the integumentary system dictates the design and survival of all flaps. Cutaneous perfusion is organized into distinct functional territories known as angiosomes, which are supplied by specific source arteries. Blood reaches the skin via three primary pathways: direct cutaneous vessels, septocutaneous perforators traveling between muscle bellies, and musculocutaneous perforators traversing through the muscle itself. These vessels ultimately feed the subdermal plexus, a rich anastomotic network located at the junction of the dermis and subcutaneous fat. Random pattern flaps rely entirely on the random arborization of this subdermal plexus, limiting their length-to-width ratio. In contrast, axial pattern flaps and pedicled flaps are designed around a known, named blood vessel, allowing for much larger territories of tissue transfer without ischemic compromise.
The physiology of free graft integration is a complex, highly orchestrated sequence of events that occurs in three distinct phases. During the first 24 to 48 hours, the graft survives via plasmatic imbibition. In this phase, the graft acts as a biological sponge, absorbing plasma exudate, erythrocytes, and nutrients directly from the recipient bed via capillary action. This process sustains the ischemic cells and causes the graft to swell and become edematous. Between days 3 and 4, the phase of inosculation begins. Capillary buds from the recipient bed proliferate, align, and directly connect with the severed, empty vascular channels on the undersurface of the graft. Finally, from day 5 onward, true angiogenesis occurs, wherein entirely new blood vessels grow from the recipient bed into the graft stroma, establishing a definitive and permanent vascular network.
The fundamental axiom of free skin grafting in orthopaedics is governed by the "Thickness Paradigm," representing a delicate biomechanical balance between graft survival (take) and long-term functional durability. Thin Split-Thickness Skin Grafts (STSG) consist of the epidermis and a minimal layer of the papillary dermis. Because they have a lower metabolic demand and a thinner physical barrier for revascularization, they exhibit a superior "take" rate, even in suboptimal recipient beds. However, thin grafts are highly susceptible to secondary contraction—often contracting by 50% to 75% of their original size as myofibroblasts pull the wound edges together. Conversely, Full-Thickness Skin Grafts (FTSG) include the entirety of the reticular dermis. The dense collagen network provides excellent durability and limits secondary contraction to approximately 10%. The critical trade-off is a massive metabolic demand, requiring a pristine, highly vascularized recipient bed for successful integration.
Exhaustive Indications and Contraindications
The decision to utilize a specific soft tissue coverage modality is dictated by the anatomical location of the defect, the physiological status of the recipient bed, and the systemic health of the patient. Split-thickness skin grafts are primarily indicated for the coverage of large, superficial defects where the recipient bed is highly vascularized. Ideal beds include healthy, contractile muscle, intact fascia, vascularized subcutaneous fat, and mature, uninfected granulation tissue. STSGs are frequently utilized for fasciotomy wound closures, massive avulsion injuries where the deep fascia remains intact, and as coverage for the muscle bellies of pedicled or free muscle flaps (e.g., a latissimus dorsi or gastrocnemius flap).
Conversely, local, regional, or free vascularized flaps are absolutely indicated when vital structures are exposed and devoid of their native vascular supply. A free skin graft will universally fail if placed over exposed cortical bone stripped of its periosteum, exposed tendon devoid of its paratenon, exposed articular cartilage, or exposed neurovascular bundles. In these scenarios, vascularized flap coverage is mandatory to provide a robust blood supply that can combat local infection, nourish the desiccated structures, and provide a durable gliding surface for tendons. Furthermore, flaps are indicated for coverage over joint creases (to prevent severe flexion contractures associated with STSG secondary contraction) and weight-bearing surfaces (such as the plantar aspect of the foot), which require thick, sensate, and shear-resistant tissue.
In the specialized realm of severe hand trauma, the "filleted flap" represents a unique and highly specific indication. When a digit is injured beyond functional salvage—such as in severe crush injuries with irreversible skeletal comminution or profound neurovascular devascularization—the glabrous skin of the unsalvageable digit remains a highly specialized, durable, and sensate tissue. Rather than discarding this valuable tissue through a standard amputation, the surgeon is indicated to harvest a filleted flap from the injured finger to cover adjacent palmar or dorsal hand defects, perfectly adhering to the principle of "spare parts" microsurgery.
Systemic contraindications must also be rigorously evaluated. Severe malnutrition (albumin < 3.0 g/dL), uncontrolled diabetes mellitus (HbA1c > 8.0%), severe peripheral vascular disease, and active systemic sepsis drastically reduce the likelihood of graft or flap survival. In such patients, temporizing measures such as Negative Pressure Wound Therapy (NPWT) or the application of dermal regeneration templates (e.g., Integra) may be indicated until the patient's physiological parameters are optimized.
Indications and Contraindications Matrix
| Coverage Modality | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Thin STSG (0.008 - 0.012 in) | Large surface areas, heavily contaminated but debrided beds, fasciotomy closures. | Exposed bare bone, tendon, nerve, or cartilage. | Joint creases, weight-bearing surfaces (due to high contraction). |
| Thick STSG (0.012 - 0.018 in) | Moderate defects requiring durability, dorsal hand coverage, healed granulation beds. | Avascular recipient beds, active beta-hemolytic streptococcal infection. | Irradiated tissue beds, severely malnourished patients. |
| Full-Thickness Graft (FTSG) | Small defects in aesthetic/functional zones (face, palmar hand), flexion creases. | Large surface area defects, poor recipient bed vascularity. | Active smoking, peripheral arterial disease. |
| Local / Pedicled Flap | Exposed vital structures, joint coverage, coverage of orthopaedic hardware. | Zone of injury encompassing the pedicle, inadequate donor tissue laxity. | Systemic coagulopathy, prior radiation to the flap territory. |
| Filleted Finger Flap | Unsalvageable digit adjacent to a severe palmar/dorsal hand defect. | Crush injury destroying the cutaneous envelope of the donor digit. | Concomitant injury to the common digital vessels supplying the flap. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the cornerstone of orthopaedic soft tissue reconstruction. The process begins with an exhaustive assessment of the defect and systematic surgical debridement. The surgeon must execute radical excision of all devitalized osseous and soft tissue structures until punctate cortical bleeding—the classic "paprika sign"—and healthy, contractile muscle are visualized. This establishes an obligate vascularized recipient bed. If the bed is deemed marginal, the strategic application of Negative Pressure Wound Therapy (NPWT) is employed as a bridging modality. NPWT promotes macro-deformation (drawing wound edges together), micro-deformation (stimulating cellular proliferation and angiogenesis), and the clearance of inhibitory matrix metalloproteinases, effectively priming the bed for subsequent grafting.
Donor site selection for skin grafting requires a careful balancing of aesthetic outcomes, ease of harvest, and patient positioning. The anterolateral thigh is the most common donor site for STSGs due to its broad, flat surface and ease of access in the supine position. The buttocks provide a more aesthetically concealed donor site, highly preferred in pediatric populations, but require prone or lateral decubitus positioning. For full-thickness grafts, donor sites are chosen based on skin color and texture match, with the groin crease, hypothenar eminence, and medial arm being common choices. Once the site is selected, precise templating of the defect is performed using sterile foil, an Esmarch bandage, or a specialized surgical glove wrapper to ensure the harvested graft perfectly matches the defect's dimensions, accounting for approximately 10-15% primary contraction immediately upon harvest.
Patient positioning and anesthesia must be coordinated to ensure simultaneous, unhindered access to both the donor and recipient sites. In complex extremity trauma, this often requires the use of specialized radiolucent tables, lateral supports, and strategic padding to prevent iatrogenic pressure neuropathies during prolonged procedures. The use of pneumatic tourniquets is highly nuanced in these cases. While a tourniquet provides a bloodless field for meticulous debridement and recipient bed preparation, it induces a state of ischemia. Prior to graft application, the tourniquet must be deflated, and meticulous hemostasis must be achieved using bipolar electrocautery and topical hemostatic agents (e.g., epinephrine-soaked lap sponges). Failure to achieve absolute hemostasis will result in an expanding hematoma beneath the graft, the leading cause of graft failure.
Equipment preparation is a critical, often overlooked step in the pre-operative phase. The surgeon must personally select and verify the calibration of the dermatome. Electrically powered dermatomes (e.g., Zimmer or Padgett) are the modern standard, allowing for rapid, uniform harvesting. The surgeon must ensure the blade is inserted correctly (bevel up or down depending on the specific model) and that the width plate matches the templated defect. The depth gauge must be set meticulously—typically between 0.012 and 0.015 inches for a standard orthopaedic STSG. For highly specific or very wide grafts, a manual drum dermatome (e.g., the Reese dermatome) may be selected, requiring the preparation of specialized skin adhesives and dermatome tape.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of harvesting and applying a skin graft demands absolute precision to ensure both graft viability and the minimization of donor site morbidity. When utilizing an electrically powered dermatome, the donor skin must be lubricated lightly with sterile mineral oil to prevent the blade from catching and creating full-thickness gouges. The surgeon’s assistant applies firm, counter-directional traction using a sterile tongue depressor or the edge of a rigid board to create a perfectly flat, taut surface. The dermatome is engaged before contacting the skin, applied at a 45-degree angle, and advanced with steady, firm, downward and forward pressure. The surgeon must maintain a consistent speed; hesitation or lifting of the device will result in uneven "chatter" marks or premature termination of the graft.
Once harvested, the graft is often subjected to meshing. Meshing serves two critical biomechanical functions: it allows for the expansion of the graft to cover a larger surface area (typically at ratios of 1.5:1 or 3:1), and, more importantly in orthopaedic trauma, it provides multiple fenestrations for the egress of underlying hematoma or seroma. However, meshing leaves a permanent, aesthetically displeasing "cobblestone" pattern. Therefore, in highly aesthetic or functional zones such as the face, neck, or dorsal hand, unmeshed "sheet" grafts are preferred, requiring meticulous pie-crusting with a #11 blade to allow for fluid drainage without compromising the cosmetic outcome.
The application and inset of the graft are paramount. The graft is carefully transferred to the recipient bed, ensuring the dermal (shiny, pale) side is facing down. It is secured using fine non-absorbable sutures (e.g., 4-0 or 5-0 nylon) or surgical staples. The graft must be tension-free but perfectly smooth, conforming intimately to the micro-contours of the recipient bed to facilitate plasmatic imbibition.
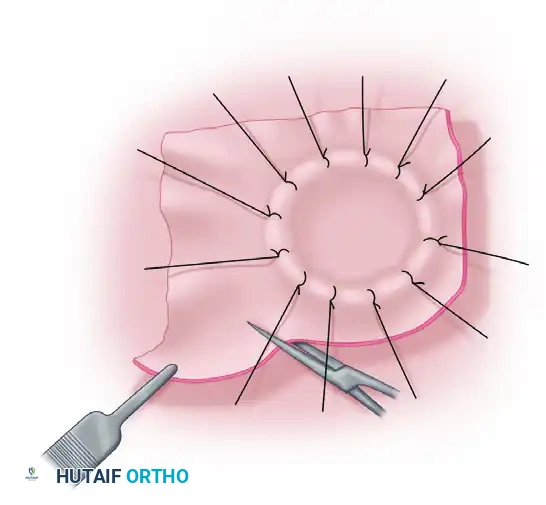
Figure A: The split-thickness graft has been sutured over the defect. The redundant edges of the graft are being carefully trimmed to match the exact contour of the wound.
To prevent shear forces that would inevitably disrupt the fragile capillary buds during the inosculation phase, a tie-over bolster dressing is absolutely mandatory for complex or contoured orthopaedic defects.

Figure B: A sheet of finely meshed, non-adherent gauze (such as Xeroform or Adaptic) is placed directly over the graft. A pack of moist cotton or fluffed gauze is then placed over the non-adherent layer to act as a compressive bolster.
The sutures used to inset the graft are left intentionally long. These tails are then gathered and tied tightly over the compressive bolster, creating an immobile, uniform pressure gradient across the entire surface of the graft.
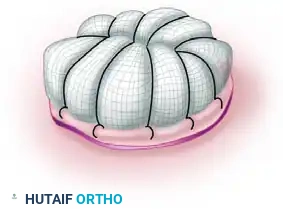
Figure C: The long sutures have been tied over the pack, creating a secure, immobile tie-over bolster dressing. This ensures intimate contact between the graft and the vascular bed, facilitating plasmatic imbibition.
After the critical integration period, the bolster is removed, and the graft is evaluated. Areas of redundancy that did not contact the vascular bed will naturally desiccate and require sharp debridement.
Figure D: The necrotic, redundant edges of the graft are being trimmed away after the central portion of the graft has successfully healed and revascularized.
Advanced Reconstruction: The Filleted Finger Flap
In the context of severe orthopaedic hand trauma, the filleted finger flap represents a pinnacle of local reconstructive technique. When a digit is deemed unsalvageable, its soft tissue envelope can be radically repurposed.
1. Defect Assessment and Flap Design: The primary defect is debrided. The unsalvageable digit is identified, and mid-axial or Brunner-type incisions are planned to "fillet" the skin off the underlying skeletal architecture while meticulously preserving the digital neurovascular bundles.

Figure 65-3 A: Visualization of the palmar defect and the adjacent severely injured digit selected for filleting.
2. Skeletal and Tendinous Excision: The phalanges, flexor and extensor tendons, and joint capsules are sharply excised. The surgeon must work in a sub-fascial plane to avoid injuring the subdermal vascular plexus, effectively unfolding the finger into a flat sheet.

Figure 65-3 B: Internal view of the digit during the filleting process. The phalanges and flexor apparatus are removed, leaving the vascularized soft tissue envelope intact.
3. Flap Elevation: The filleted skin is fully opened. The digital artery and nerve are protected at the base, ensuring robust axial perfusion and preserving protective sensation, which is critical for palmar hand reconstruction.
Figure 65-3 C: The filleted tissue is elevated, demonstrating a broad, durable sheet of glabrous skin ready for transposition.
4. Transposition and Inset: The flap is rotated into the primary defect. The glabrous tissue provides an exact match in thickness, durability, and color, offering superior coverage for exposed tendons or nerves compared to distant grafts.

Figure 65-3 D: The flap is transposed over the palmar defect. The robust subcutaneous fat and thick dermis provide excellent coverage for exposed tendons or neurovascular structures.
5. Final Closure: The flap is sutured into place with fine monofilament. The donor site is closed primarily, achieving a highly functional reconstruction while entirely avoiding distant donor site morbidity.

Figure 65-3 E: Final appearance after the filleted graft has been fully inset and sutured, successfully reconstructing the complex palmar defect.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications in orthopaedic soft tissue coverage are inevitable and must be managed aggressively to prevent catastrophic failure. The most common mechanism of free skin graft failure is the accumulation of fluid—either a hematoma or seroma—beneath the graft. This physical barrier prevents plasmatic imbibition and severs the fragile capillary buds attempting inosculation, leading to rapid ischemic necrosis of the overlying graft. Infection is the second most common cause of failure, with Streptococcus pyogenes (beta-hemolytic strep) and Pseudomonas aeruginosa being particularly destructive, as they produce proteolytic enzymes that rapidly dissolve the fibrin bonds anchoring the graft to the bed.
Donor site complications, while often considered secondary, can cause significantly more morbidity than the recipient site itself. Delayed healing, hypertrophic scarring, severe dyschromia, and intractable pain are frequent sequelae of STSG harvesting. If the dermatome blade gouges the tissue, creating an inadvertent full-thickness defect, primary closure or even secondary grafting of the donor site may be required. Modern management of the donor site emphasizes the use of occlusive, moisture-retentive dressings (e.g., calcium alginates, hydrocolloids, or polyurethane films) which have been shown to significantly reduce pain and accelerate epithelialization compared to traditional dry gauze.
Flap complications present a more complex clinical challenge, typically manifesting as either arterial insufficiency or venous congestion. Arterial insufficiency presents with a pale, cool flap with absent capillary refill and no bleeding upon pinprick. This is often due to pedicle tension, arterial thrombosis, or vasospasm. Venous congestion, conversely, presents with a swollen, violaceous, or deeply purple flap with brisk, dark bleeding on pinprick. Venous outflow obstruction is statistically more common than arterial failure and is highly detrimental, as the accumulation of metabolic waste products rapidly induces cellular death.
Complications and Salvage Management Table
| Complication | Estimated Incidence | Clinical Presentation | Salvage Strategy / Management |
|---|---|---|---|
| Sub-graft Hematoma | 10 - 15% | Localized dark fluctuance under graft, failure of graft adherence. | Early (<48h): Evacuation via rolling swab or pie-crusting. Late: Debridement and re-grafting. |
| Graft Infection | 5 - 8% | Purulent exudate, graft dissolution, surrounding erythema. | Aggressive systemic antibiotics, removal of necrotic graft, NPWT, secondary grafting when clean. |
| Flap Venous Congestion | 5 - 10% | Violaceous color, rapid capillary refill, dark bleeding, severe edema. | Release restrictive sutures, dependent positioning, application of medicinal leeches (Hirudo medicinalis). |
| Flap Arterial Ischemia | 2 - 5% | Pale, cool tissue, absent capillary refill, no bleeding on pinprick. | Immediate surgical re-exploration, pedicle repositioning, intra-arterial vasodilators (papaverine). |
| Donor Site Hypertrophy | 15 - 20% | Raised, erythematous, pruritic scarring at the harvest site. | Silicone gel sheeting, compressive garments, intralesional corticosteroid injections. |
Salvage management requires decisive action. In cases of severe venous congestion where surgical revision is not feasible, the application of medicinal leeches (Hirudo medicinalis) is a highly effective, albeit unconventional, salvage technique. The leech saliva contains hirudin, a potent direct thrombin inhibitor, which provides localized anticoagulation and continuous venous decompression. If a graft or flap fails completely, radical re-debridement is mandatory. In these salvage scenarios, the application of a dermal regeneration template (e.g., Integra) can be utilized to
