Anterior Thoracic Spine Approach: An Intraoperative Masterclass for Fellows
Key Takeaway
Master the anterior thoracic spine approach for complex pathologies. This immersive guide covers meticulous patient positioning, intricate surgical anatomy, and granular, real-time intraoperative steps. Fellows will learn critical dissection techniques, neurovascular protection, and strategies to avoid pitfalls, ensuring optimal patient outcomes and effective complication management.
Comprehensive Introduction and Patho-Epidemiology
The anterior approach to the thoracic spine represents a fundamental evolution in orthopedic and neurosurgical spine care, transitioning the field from the historically morbid posterior laminectomies for anterior pathology to direct, anatomically sound surgical corridors. For decades, attempting to decompress a ventral thoracic lesion via a posterior approach frequently resulted in catastrophic neurological deterioration due to the manipulation of the tenuous thoracic spinal cord. The advent and refinement of the anterior transthoracic approach have provided spine surgeons with a powerful, direct tool in our armamentarium for conditions ranging from massive calcified disc herniations and pyogenic infections to complex primary tumors, metastatic disease, and severe traumatic burst fractures. This approach offers unparalleled direct access for ventral decompression, deformity correction, and robust anterior column stabilization. However, it demands meticulous preoperative planning, a profound understanding of intrathoracic anatomy, and flawless intraoperative execution.
From a patho-epidemiological standpoint, the thoracic spine is uniquely vulnerable to specific disease processes due to its biomechanical properties and vascular watershed zones. The anterior column of the thoracic spine bears approximately eighty percent of the axial load, making it the primary site of failure in high-energy axial loading trauma, such as burst fractures. Furthermore, the highly vascularized nature of the vertebral bodies creates a hospitable microenvironment for hematogenous seeding of both pathogens (resulting in discitis-osteomyelitis) and metastatic neoplastic cells (commonly from breast, prostate, lung, and renal primary tumors). When these pathologies expand, they invariably compress the anterior aspect of the dural sac. Because the thoracic kyphosis naturally drapes the spinal cord over the posterior aspect of the vertebral bodies, any ventral mass effect leads to rapid and often irreversible myelopathy. Therefore, mastering the anterior approach is not merely an academic exercise; it is a critical, limb-saving, and life-altering skill for the complex spine surgeon.
As we guide our fellows through this masterclass, it is imperative to recognize that this operation is a multidisciplinary endeavor. It requires seamless collaboration with our anesthesia colleagues for lung isolation, our neuromonitoring teams for real-time cord assessment, and occasionally our thoracic surgery colleagues for complex exposures or visceral complications. The modern spine surgeon must be as comfortable navigating the pleural cavity, mobilizing the great vessels, and managing the diaphragm as they are with a Cobb elevator and a pedicle probe. This chapter will serve as your definitive, exhaustive guide to mastering the anterior thoracic approach, leaving no anatomical nuance or technical pearl unexplored.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel ever touches skin, a profound and three-dimensional understanding of thoracic anatomy is absolute paramount. The thoracic spine is a biomechanically rigid segment, stabilized by the rib cage, the sternum, and robust costovertebral ligaments. This rigidity, while protective of the cardiopulmonary organs, presents a formidable barrier to surgical access. The natural kyphosis of the thoracic spine (typically ranging from twenty to forty degrees) dictates our trajectory; an anterior approach allows us to work within the concavity of this curve, providing a direct line of sight to the ventral pathology without requiring manipulation of the spinal cord.
The vascular anatomy of the thoracic spine is notoriously unforgiving and represents one of the most critical aspects of this surgical exposure. The thoracic spinal cord relies on a tenuous blood supply, particularly in the midthoracic "watershed" region between T4 and T9. The primary arterial supply is derived from the anterior spinal artery, which is fed by variable radiculomedullary arteries arising from the segmental vessels. The most prominent of these is the Artery of Adamkiewicz (arteria radicularis magna), which originates on the left side in approximately eighty percent of individuals, typically between the levels of T8 and L2. Inadvertent ligation of this artery or bilateral ligation of multiple critical segmental vessels can lead to catastrophic anterior spinal artery syndrome, characterized by profound motor paraplegia with preservation of dorsal column sensory function. Therefore, meticulous identification and strategic management of the segmental vessels are non-negotiable.
Beyond the vascular considerations, the surgeon must navigate a complex array of visceral and somatic structures. Superficial dissection requires traversing the robust musculature of the shoulder girdle and chest wall, including the latissimus dorsi, trapezius, rhomboids, and serratus anterior. Deep to the ribs lies the parietal pleura, a delicate membrane that must be carefully incised to enter the thoracic cavity. Once inside the chest, the lungs must be managed via selective deflation and gentle retraction. The mediastinal structures dictate our side of approach: the heart and aortic arch dominate the left upper thorax, while the descending aorta courses slightly to the left of the midline along the vertebral bodies. The inferior vena cava and azygos venous systems lie to the right. Furthermore, the sympathetic trunk runs longitudinally along the anterolateral aspect of the vertebral bodies, medial to the psoas muscle in the lower thorax; injury to this structure can result in Horner's syndrome in the upper thorax or regional vasomotor disturbances lower down. Finally, the thoracic duct, which typically ascends on the right side of the lower thoracic spine before crossing to the left around T4-T5, must be respected to prevent a debilitating postoperative chylothorax.
Exhaustive Indications and Contraindications
The decision to proceed with an anterior thoracic approach must be grounded in a rigorous assessment of the patient's pathology, overall physiological reserve, and the biomechanical goals of the surgery. The primary indication is the presence of a ventral pathology that requires direct decompression, structural reconstruction, or both, which cannot be safely or effectively addressed via a posterior or posterolateral trajectory. This approach is the gold standard for pathologies that have destroyed the anterior weight-bearing column, necessitating a corpectomy and strut graft reconstruction to restore sagittal alignment and mechanical stability.
Specific indications span the gamut of spinal pathology. In the realm of degenerative disease, large, central, or calcified thoracic disc herniations causing progressive myelopathy are classic indications. Attempting to remove a hard, calcified central disc past the spinal cord from a posterior approach carries an unacceptably high risk of iatrogenic paralysis. For infectious etiologies, such as pyogenic vertebral osteomyelitis or tuberculous spondylitis (Pott's disease) with significant anterior bone destruction and epidural abscess formation, the anterior approach allows for radical debridement of infected necrotic tissue and placement of a vascularized or structural graft in a clean bed. In spinal oncology, both primary bone tumors (e.g., giant cell tumors, chordomas) and metastatic lesions causing ventral cord compression and mechanical instability are prime candidates for anterior corpectomy and stabilization. Traumatic burst fractures with significant retropulsion of bone fragments into the spinal canal, particularly those presenting with incomplete neurological deficits, also benefit immensely from direct anterior decompression and plating.
Conversely, there are strict contraindications that must be respected. Absolute contraindications include profound medical comorbidities that preclude single-lung ventilation or the physiological stress of a thoracotomy, such as severe chronic obstructive pulmonary disease (COPD) or prohibitive cardiac disease. Relative contraindications include a history of extensive prior ipsilateral thoracotomies or empyema, which can result in dense pleural adhesions that make lung mobilization exceedingly treacherous. Additionally, if the pathology involves a circumferential lesion with significant posterior column disruption, an isolated anterior approach may be biomechanically insufficient, necessitating either a combined anterior-posterior approach or a purely posterior approach with extended pedicle subtraction osteotomies.
Indications and Contraindications Summary
| Category | Specific Pathologies | Rationale for Anterior Approach | Contraindications (Absolute & Relative) |
|---|---|---|---|
| Degenerative | Calcified central disc herniations, severe ventral osteophytes. | Direct visualization of the ventral dura; avoids manipulation of the thoracic cord. | Absolute: Severe pulmonary hypertension, prohibitive cardiopulmonary risk. |
| Trauma | Burst fractures with >50% canal compromise, retropulsed fragments, kyphosis. | Direct removal of retropulsed bone; optimal biomechanical restoration of the anterior column. | Relative: Severe concurrent pulmonary contusions or ARDS precluding single-lung ventilation. |
| Oncology | Metastatic disease (breast, lung, prostate), primary tumors (chordoma). | Allows for en bloc or piecemeal corpectomy, tumor debulking, and structural reconstruction. | Relative: Expected survival < 3 months, highly radiosensitive tumors (e.g., myeloma) without instability. |
| Infection | Pyogenic osteomyelitis, Discitis, Tuberculous spondylitis. | Radical debridement of avascular necrotic tissue; placement of graft in a well-vascularized bed. | Relative: Dense pleural adhesions from prior empyema or multiple thoracotomies. |
| Deformity | Scheuermann's kyphosis, rigid scoliotic curves. | Anterior release (discectomies) maximizes flexibility for subsequent posterior correction. | Absolute: Purely posterior column pathology or isolated posterior tension band failure. |
Pre-Operative Planning, Templating, and Patient Positioning
Before we even think about touching the patient, our battle is won or lost in the planning phase. The anterior thoracic approach leaves no room for improvisation when it comes to level localization and vascular anatomy. Preoperative templating and exhaustive imaging review are the cornerstones of a successful, complication-free procedure.
Imaging Review and Level Localization
Wrong-level surgery is a devastating, "never-event" complication that we must avoid at all costs. The thoracic spine is particularly treacherous for localization due to the lack of easily palpable external landmarks and the repetitive, uniform nature of the vertebral segments. High-quality anteroposterior and lateral thoracic spine radiographs, along with a full chest radiograph, are mandatory. We use these for initial rib counting, identifying transitional vertebrae, and noting any anatomical anomalies such as cervical ribs or lumbarized sacral segments. Remember, the first rib can be hard to palpate radiographically, but the second intercostal space is typically the largest. In severely kyphotic or scoliotic patients, scrutinize these films carefully. Knowing the exact number of lumbar segments below the last thoracic rib is invaluable for counting up from the sacrum if intraoperative landmarks remain ambiguous.
Magnetic Resonance Imaging (MRI) and Computed Tomography (CT) are our surgical blueprints. The MRI is essential for understanding the soft tissue pathology—the exact morphology of the disc herniation, the craniocaudal extent of a tumor, the degree of epidural compression, and the presence of myelomalacia within the spinal cord. Always mandate a topogram (scout image) with your MRI. This provides a full-length sagittal view from the craniocervical junction to the sacrum, eliminating ambiguity about precise vertebral levels. The CT scan provides exquisite bony detail and is critical for assessing bone quality for instrumentation. Pay meticulous attention to the axial CT cuts. This is where you will map out the exact position of the aorta and inferior vena cava relative to the pathology. This axial relationship dictates our side of approach, especially if a deep corpectomy is planned. Furthermore, in cases of suspected vascular anomalies, congenital kyphosis, or if a patient has had a prior spine exposure on the contralateral side, a preoperative spinal angiogram is highly prudent. This identifies crucial arterial feeders, particularly the Artery of Adamkiewicz, allowing us to plan segmental vessel ligation strategically and avoid devastating spinal cord ischemia.
Side of Approach: A Critical Decision
The choice of approach side is a calculated decision based on multiple interacting factors. If there is a clear posterolateral or lateral herniation, approaching from the side of the herniation provides the most direct access for decompression. However, the position of the great vessels usually dictates the approach in centrally located pathology. In most thoracic cases, the heart and great vessels are either on the left or central. Therefore, a right-sided approach is generally favored in the midthoracic region (T4-T9) to avoid the heart and facilitate mobilization of the great vessels.
Conversely, in the distal thoracic spine (T10-T12), the right-sided approach is often obstructed by the dome of the liver. Retracting the liver is technically challenging and carries a higher risk of capsular tear and hemorrhage than retracting the spleen or kidney. Therefore, a left-sided approach is generally favorable in the thoracolumbar junction. A general principle for vascular mobilization is that it is often safer and easier to mobilize the thick-walled, pulsatile aorta from its left-central position toward the right, rather than attempting to mobilize the thin-walled, easily avulsed inferior vena cava toward the left. For upper thoracic exposures (T1-T4), a right-sided approach is almost universally preferred to avoid the aortic arch and the bulk of the heart.
Anesthesia Considerations and Patient Positioning
Our anesthesia colleagues are integral to the success of this operation. An oral gastric tube is essential for decompressing the stomach and providing a palpable landmark for the esophagus, especially during upper thoracic approaches. A double-lumen endotracheal tube is crucial for selective deflation of the ipsilateral lung. This allows the lung to collapse and fall away from our surgical field, significantly improving exposure and minimizing the need for aggressive mechanical retraction, which can cause pulmonary contusions. Neurologic monitoring, specifically Somatosensory Evoked Potentials (SSEPs) and Motor Evoked Potentials (MEPs), must be utilized to provide real-time assessment of spinal cord function, particularly during segmental vessel temporary clipping or permanent ligation.
Patient positioning is the foundation of the exposure. The patient is placed in the strict lateral decubitus position, with the side of the approach facing upwards.

Position the patient so the thorax vertex is directly over the break in the OR table. This allows for slight flexion or extension of the thoracic spine, optimizing our working angle and "opening up" the disc spaces on the operative side. Padding all pressure points is non-negotiable. Place a soft, well-padded axillary roll just caudal to the dependent axilla to prevent compression of the axillary neurovascular bundle, which can lead to devastating postoperative brachial plexopathies. Pillows must be placed between the legs to protect the peroneal nerve, and the arms are typically placed in a "prayer position" in front of the face, supported by specialized arm boards. This arm position helps to pull the scapula anteriorly and superiorly, improving access to the upper and mid-thoracic ribs. Finally, ensure the C-arm fluoroscopy unit can easily swing into the field to obtain true AP and lateral views without obstruction from the table base.
Step-by-Step Surgical Approach and Fixation Technique
The intraoperative execution of the anterior thoracic approach is a masterclass in layered, anatomical dissection. We will break this down into the complex high thoracic approach (T1-T4) and the standard midthoracic approach, followed by the deep spinal exposure common to both.
The High Anterior Thoracic Approach (T1 to T4)
This is arguably the most challenging thoracic exposure due to the obstruction of the shoulder girdle and the presence of the superior mediastinal structures. We utilize a right-sided approach to avoid the heart and aortic arch.
-
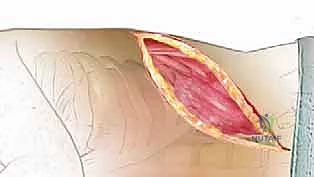
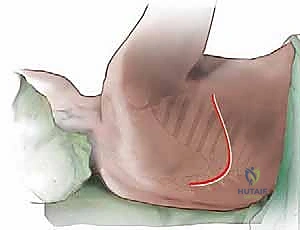
Skin Incision and Superficial Dissection: Palpate the inferior angle of the scapula. Using a #10 blade, make a generous curved skin incision just below the tip of the scapula, extending from the posterior axillary line anteriorly and superiorly toward the axilla.
This curvilinear incision provides optimal access while allowing for superior retraction of the entire shoulder girdle. Incise the subcutaneous fat with meticulous electrocautery to maintain a dry field. -
Muscle Division: Dissect down to the broad latissimus dorsi muscle. Incise the latissimus dorsi in line with your skin incision. Crucially, leave a sufficient cuff of muscle attached to the scapula to ensure a robust fascial repair during closure, minimizing dead space and seroma formation.
Deep to the latissimus, you will encounter the trapezius and rhomboid muscles posteriorly. These must also be divided in line with the incision to fully mobilize the scapula.
-
Scapular Mobilization: Once the superficial and intermediate muscle layers are divided, place a large scapular retractor (such as a Finochietto or specialized scapula lifter) under the inferior angle of the scapula. Elevate and retract the scapula superiorly and anteriorly. This maneuver exposes the upper ribs (ribs 2 through 5) and the underlying serratus anterior muscle.
Standard Thoracotomy and Rib Resection (T4-T10)
For mid-to-lower thoracic lesions, the incision is centered directly over the rib corresponding to the pathology (usually one or two levels above the target vertebra to account for the downward slope of the ribs).
-
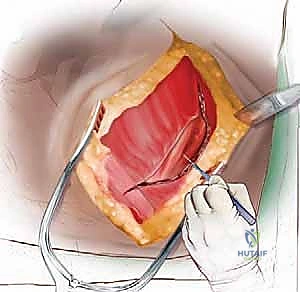
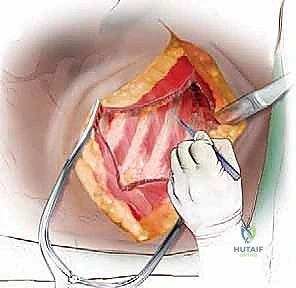
Rib Exposure and Periosteal Elevation: Once the appropriate rib is identified (confirmed via fluoroscopy with a metallic marker), the periosteum overlying the rib is incised longitudinally using electrocautery. Using a Cobb elevator or a specialized rib raspatory (e.g., Doyen elevator), meticulously strip the periosteum from the outer, superior, and inferior aspects of the rib.

Surgical Pearl: Always sweep the raspatory from posterior to anterior on the superior border, and anterior to posterior on the inferior border, respecting the direction of the intercostal muscle fibers. Stay strictly subperiosteal on the inferior border to avoid injuring the intercostal neurovascular bundle. -
Rib Excision: Once the rib is circumferentially subperiosteally dissected, use rib shears to transect the rib anteriorly at the costochondral junction and posteriorly near the costotransverse articulation. Remove the rib segment. This excised bone is an excellent source of autograft for later fusion.
In some cases, to gain adequate exposure of the disc space and neuroforamen, the rib head must be entirely disarticulated and removed using a high-speed burr, Kerrison rongeurs, and pituitary rongeurs. -
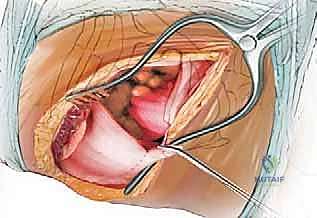
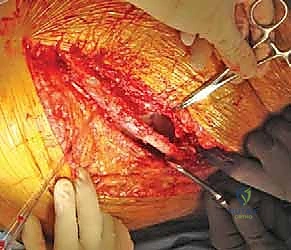
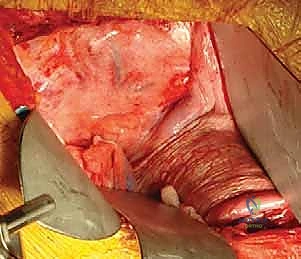
Pleural Entry and Lung Management: The bed of the resected rib consists of the deep periosteal layer and the underlying parietal pleura. Carefully incise this layer using a scalpel or scissors, taking care not to lacerate the underlying lung parenchyma.

Once the pleural cavity is entered, coordinate with anesthesia to ensure the ipsilateral lung is deflated. Use moist laparotomy sponges and a broad, padded malleable retractor to gently retract the deflated lung medially and anteriorly, exposing the vertebral column.
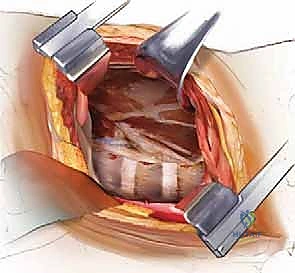
Deep Spinal Exposure and Segmental Vessel Management
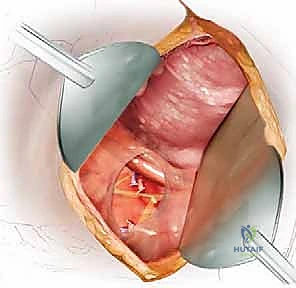
With the lung retracted, the lateral aspect of the thoracic spine comes into clear view, covered by the shiny parietal pleura.
-
Identifying the Target Level: You will see the segmental vessels coursing over the "valleys" of the vertebral bodies, while the "hills" represent the avascular intervertebral disc spaces.

Incise the parietal pleura longitudinally over the spine. Use blunt dissection (peanut sponges or Kittner dissectors) to sweep the pleura and underlying loose areolar tissue off the spine. -
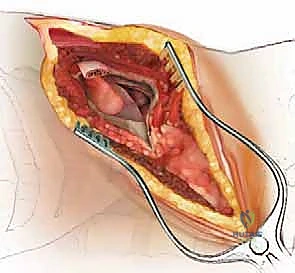
Segmental Vessel Ligation: This is a critical step. The segmental arteries and veins must be isolated, ligated, and divided to allow mobilization of the great vessels and access to the vertebral body.
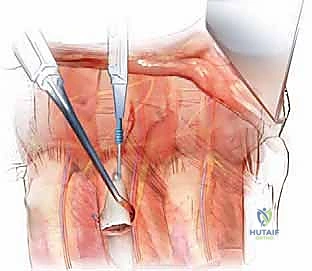
Using right-angle clamps, carefully dissect under the segmental vessels. Pass heavy silk ties (e.g., 2-0 silk) or use surgical clips to ligate the vessels.
Crucial Warning: Always ligate the segmental vessels at the mid-vertebral body level, anterior to the neural foramen. Ligating them too far posteriorly near the foramen risks compromising collateral anastomotic arcades that feed the radiculomedullary arteries, increasing the risk of spinal cord ischemia. -
Mobilization of Great Vessels and Sympathetic Chain: Once the segmentals are divided, the aorta (or IVC) can be gently mobilized anteriorly using blunt dissection.
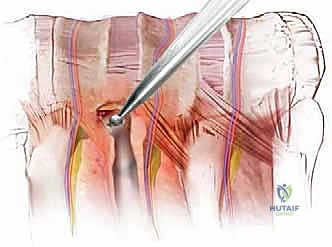
During this dissection, identify and protect the sympathetic chain, which runs longitudinally over the rib heads and lateral vertebral bodies.