Mastering the Posterior Iliac Crest for Bone Graft Harvest
Key Takeaway
Looking for accurate information on Mastering the Posterior Iliac Crest for Bone Graft Harvest? The posterior iliac crest is a common source for autogenous bone grafts, frequently used in posterior spine surgery or other fusions. An 8-cm oblique incision is made over the posterior superior iliac spine, in line with the iliac crest. The outer border of the iliac crest serves as an internervous plane, minimizing muscle denervation when harvesting the crest for bone.
Introduction and Epidemiology
Autologous bone grafting remains the gold standard for achieving osseous fusion in orthopedic and spinal surgery. Despite the advent of synthetic bone graft substitutes, demineralized bone matrix, and recombinant human bone morphogenetic proteins (rhBMP), autogenous bone provides the essential triad required for successful arthrodesis: osteogenesis (viable osteoprogenitor cells), osteoinduction (growth factors such as BMPs that stimulate cellular differentiation), and osteoconduction (a structural scaffold for vascular and cellular ingrowth).

The posterior iliac crest is widely considered the premier anatomical site for autologous bone graft harvest. Compared to the anterior iliac crest, the posterior ilium offers a significantly larger volume of high-quality corticocancellous and pure cancellous bone. Surgeons can typically harvest between 30 to 50 cubic centimeters of uncompressed cancellous bone from the posterior crest, whereas the anterior crest yields approximately 15 to 20 cubic centimeters. Furthermore, posterior iliac crest bone graft (PICBG) harvesting is associated with lower overall morbidity, decreased postoperative ambulation pain, and a reduced risk of clinically significant cutaneous nerve entrapment compared to its anterior counterpart.
Epidemiologically, the posterior approach to the iliac crest is most frequently utilized in conjunction with posterior spinal arthrodesis, including lumbar, thoracic, and cervical fusions where the patient is already positioned prone. It is also a critical technique for orthopedic traumatologists and reconstructive surgeons managing complex nonunions, massive segmental bone defects, and major joint arthrodesis. Mastery of this surgical approach requires a profound understanding of the regional pelvic anatomy, meticulous surgical technique, and strict adherence to defined anatomical safe zones to minimize harvest-site morbidity.
Surgical Anatomy and Biomechanics
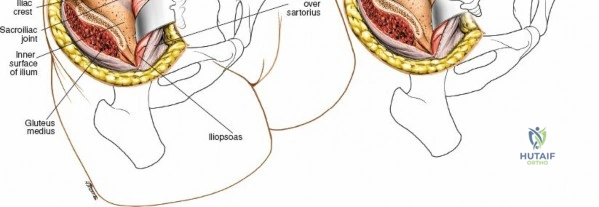
A thorough comprehension of the osseous, muscular, and neurovascular anatomy of the posterior pelvis is paramount for safe and efficacious bone graft harvesting. The posterior ilium is characterized by a thick cortical rim surrounding a dense, highly vascularized cancellous diploë.
Osseous Landmarks
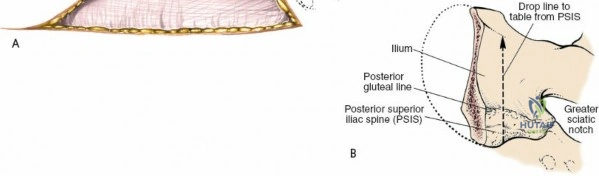
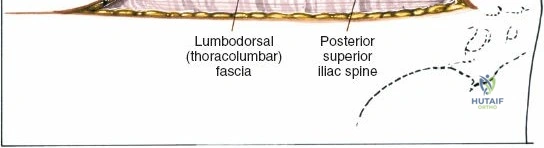
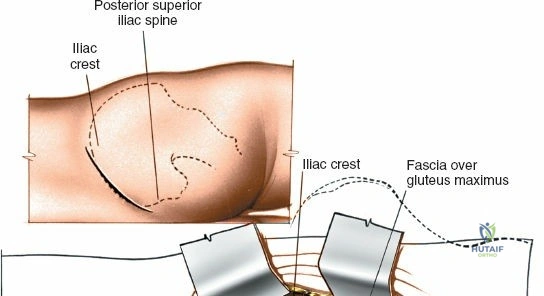
The primary osseous landmark is the posterior superior iliac spine (PSIS). The PSIS is typically identifiable by a visible cutaneous dimple in the sacral region and is easily palpable subcutaneously. The iliac crest extends laterally and anteriorly from the PSIS. Inferior to the PSIS lies the posterior inferior iliac spine (PIIS), which marks the superior boundary of the greater sciatic notch. The sacroiliac (SI) joint lies immediately medial and deep to the PSIS. Violating the SI joint during harvest is a severe technical error that can lead to chronic, debilitating pelvic pain and iatrogenic instability.
Muscular Anatomy and Internervous Planes
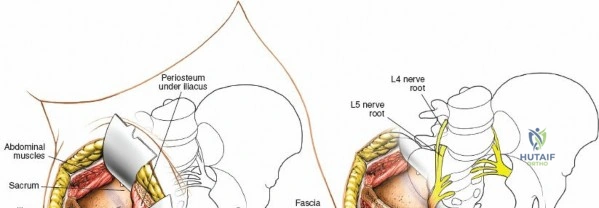
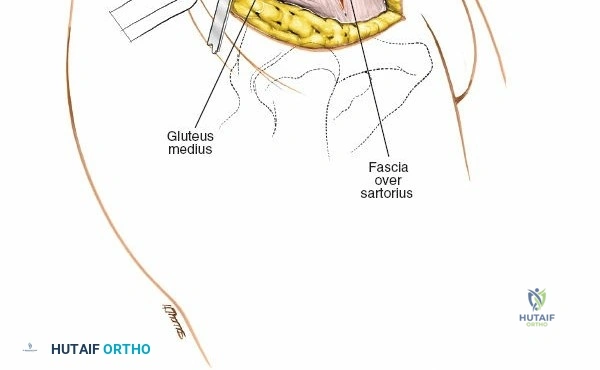
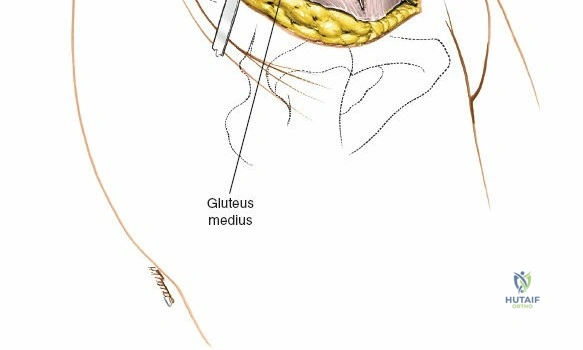
The posterior iliac crest serves as an origin and insertion point for multiple muscle groups, but it is fundamentally an internervous plane. The outer table of the ilium provides the origin for the gluteal musculature. The gluteus maximus (innervated by the inferior gluteal nerve) originates from the posterior gluteal line, while the gluteus medius and minimus (innervated by the superior gluteal nerve) originate more anteriorly and laterally.
Medial to the crest, the paraspinal musculature (erector spinae and multifidus, innervated by dorsal rami of spinal nerves) and the latissimus dorsi (innervated by the thoracodorsal nerve) take their origins. Because these muscles do not cross the crest itself, a precise subperiosteal dissection along the outer or inner border of the iliac crest does not denervate the surrounding musculature.
Neurovascular Structures and Safe Zones
The most critical neurovascular structures in this region are the superior cluneal nerves and the superior gluteal artery. The superior cluneal nerves are sensory branches derived from the dorsal rami of L1, L2, and L3. They pierce the lumbodorsal fascia and cross the posterior iliac crest to provide cutaneous sensation to the upper buttocks. Anatomical studies consistently demonstrate that these nerves cross the crest at a distance ranging from 7 to 9 centimeters lateral to the PSIS. Therefore, the "safe zone" for posterior iliac crest harvest is strictly confined to the medial 8 centimeters of the crest, measured from the PSIS. Extending the dissection lateral to this 8-cm mark significantly increases the risk of cluneal nerve transection or entrapment, leading to painful postoperative neuromas.
The superior gluteal artery and nerve exit the pelvis through the greater sciatic notch, located approximately 4 to 6 centimeters inferior to the PSIS. When elevating the gluteal musculature off the outer table of the ilium, surgeons often place a Taylor retractor or a blunt Hohmann retractor into the sciatic notch. If the retractor slips or is driven too aggressively, it can lacerate the superior gluteal artery. This vessel can retract into the pelvis, resulting in catastrophic, life-threatening hemorrhage that is exceptionally difficult to control from a posterior approach.
Indications and Contraindications
The decision to harvest bone from the posterior iliac crest must be weighed against the availability of alternative grafting materials and the specific biological requirements of the primary surgical site.
Indications
Posterior iliac crest bone grafting is indicated whenever a substantial volume of highly osteogenic, osteoinductive, and osteoconductive material is required. Common indications include:
* Posterior or posterolateral spinal arthrodesis (cervical, thoracic, or lumbar).
* Treatment of atrophic or oligotrophic nonunions of long bones.
* Filling of cavitary bone defects following tumor curettage or osteomyelitis debridement.
* Arthrodesis of major joints (e.g., ankle, subtalar, wrist).
* Reconstruction of severe comminution in acute fracture management.
Contraindications
Absolute contraindications are rare but include active local infection at the harvest site or severe systemic bacteremia. Relative contraindications require careful preoperative assessment. Patients with a history of prior posterior iliac crest harvest may have insufficient residual bone stock, necessitating advanced preoperative imaging (CT scan) to identify available diploic space. Severe osteoporosis reduces the structural integrity of the corticocancellous blocks and diminishes the cellular yield of the cancellous harvest. Additionally, patients with pre-existing sacroiliac joint pathology or pelvic ring instability should be approached with extreme caution, as the harvest may exacerbate mechanical instability.
Operative Indications Summary
| Clinical Scenario | Primary Grafting Strategy | Rationale for Posterior Iliac Crest |
|---|---|---|
| Lumbar Pseudarthrosis Revision | Autologous PICBG | High osteogenic potential required to overcome hostile local biology and prior fusion failure. |
| Acute Long Bone Fracture (Minor Defect) | Local Autograft / Allograft | PICBG morbidity outweighs benefits if local bone or structural allograft is sufficient. |
| Cavitary Defect (Post-Tumor) | Allograft / Bone Substitutes | Large volume required, but structural integrity and osteoconduction are prioritized over osteogenesis. |
| Atrophic Tibial Nonunion | Autologous PICBG | Essential need for viable osteoprogenitor cells and osteoinductive factors to stimulate healing. |
| Multilevel Spinal Deformity | PICBG + Local Bone + Extenders | High volume required; PICBG provides the biological spark, while extenders provide volume. |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning minimizes intraoperative complications and optimizes graft yield. Reviewing standard anteroposterior and lateral pelvic radiographs is mandatory. In cases of prior harvest or complex pelvic anatomy, a non-contrast computed tomography (CT) scan is invaluable for assessing the thickness of the iliac wing and the exact location of the sacroiliac joint.

Patient Positioning
The patient is placed in the prone position on the operating table. The choice of table depends on the primary procedure. For spinal surgery, a Jackson spinal table or a standard operating table equipped with a Wilson frame or longitudinal bolsters is utilized.
It is highly critical to position the longitudinal bolsters to support the lateral chest wall and the anterior superior iliac spines (ASIS) and pelvis. This arrangement allows the abdomen to hang free, unimpeded by external pressure. A free abdomen decreases intra-abdominal pressure, which in turn reduces pressure in the inferior vena cava and the epidural venous plexus (Batson's plexus). This physiological optimization significantly decreases intraoperative blood loss during both the spinal exposure and the iliac crest harvest.
Preparation and Draping
The surgical field must be prepped and draped widely. The drapes should extend distally enough to visualize the beginning of the gluteal cleft and bilaterally to expose the entire posterior pelvis. The PSIS must be easily palpable within the sterile field. A wide exposure ensures that the surgeon can accurately identify anatomical landmarks and maintain proper orientation throughout the dissection.
Detailed Surgical Approach and Technique
The surgical approach to the posterior iliac crest can be performed through a dedicated separate incision or via fascial undermining from a midline spinal incision.
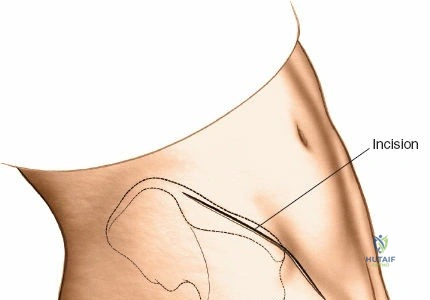
Incision and Superficial Dissection
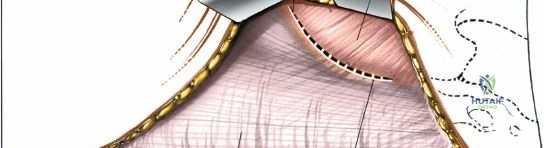
For a dedicated harvest, make an 8-cm oblique incision centered over the PSIS and oriented in line with the iliac crest. Incise the skin and the thick, fatty subcutaneous layer. Meticulous hemostasis is required in the subcutaneous tissues to prevent postoperative hematoma formation.
If a concurrent midline lumbar or scoliosis surgery is being performed, the midline incision can be extended distally to the level of the sacrum. The skin and subcutaneous fat are then aggressively retracted laterally. Using a Hibbs or Gelpi retractor, dissect the subcutaneous flap free from the underlying lumbodorsal fascia until the PSIS and the posterior crest can be directly palpated and visualized. This fascial undermining technique avoids a second skin incision but requires extensive dead space management during closure.
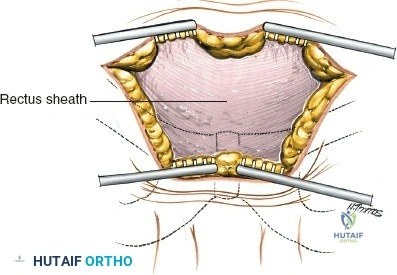
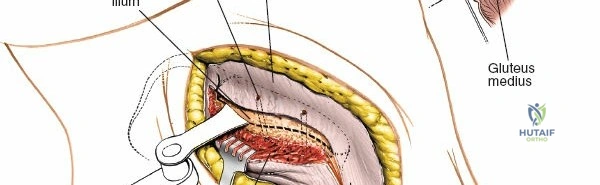
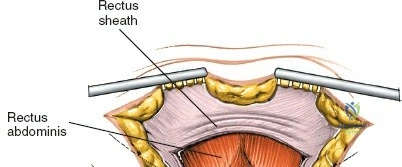
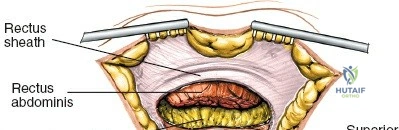
Deep Dissection and Exposure
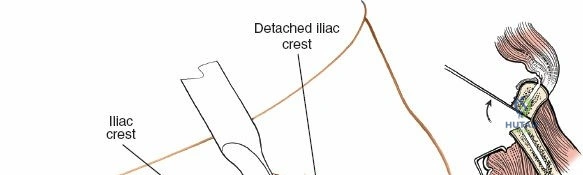
Once the fascia overlying the crest is identified, incise the tissue directly in line with the iliac crest down to the bone. In pediatric patients, the iliac apophysis is cartilaginous, white, and highly visible; it may be split sharply in line with the crest to expose the underlying bone.
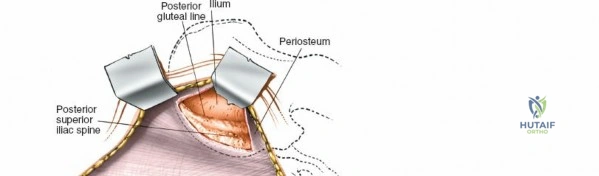
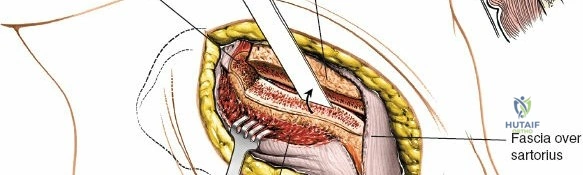
Using a Cobb elevator or electrocautery, perform a subperiosteal elevation. For an outer table harvest, elevate the gluteal musculature laterally and inferiorly. The dissection should remain strictly subperiosteal to minimize bleeding and avoid injury to the superior gluteal artery. A Taylor retractor can be carefully placed with its tip resting gently in the greater sciatic notch to maintain exposure. Ensure the retractor is not driven forcefully into the notch.
Graft Harvesting Techniques
Several techniques exist for harvesting bone, dependent on whether structural corticocancellous blocks or pure cancellous slurry is required.
The Trapdoor Technique
The trapdoor technique is highly favored as it preserves the structural contour of the iliac crest, thereby minimizing postoperative cosmetic deformity and reducing localized pain.
1. Using a sharp osteotome or an oscillating saw, make a longitudinal cut along the superior aspect of the iliac crest, approximately 1 cm lateral to the medial border.
2. Make two perpendicular cuts at the anterior and posterior extents of the longitudinal cut.
3. Hinge the cortical "trapdoor" laterally, leaving the lateral periosteum and muscular attachments intact to act as a hinge.
4. This exposes the rich, cancellous diploë. Using sharp gouges or curettes, harvest the cancellous bone. Direct the curettes anteriorly and inferiorly, following the contour of the iliac wing.
5. Strictly avoid directing instruments medially to prevent violation of the sacroiliac joint, and avoid penetrating the inner or outer cortical tables.

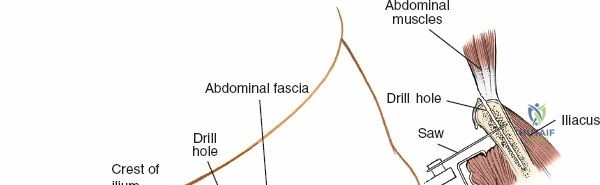
Corticocancellous Block Harvest
If structural bone is required (e.g., for anterior cervical discectomy and fusion or structural nonunion repair):
1. Expose the outer table of the ilium.
2. Use an oscillating saw to outline the required dimensions of the block.
3. Use curved osteotomes to free the deep cancellous surface of the block.
4. Carefully extract the block, ensuring it remains intact.
Hemostasis and Closure
Following harvest, meticulous hemostasis of the bony bed is imperative. Apply bone wax to bleeding cortical edges. The cancellous void can be packed with hemostatic agents such as Gelfoam or oxidized regenerated cellulose (Surgicel). Some surgeons advocate for the use of a localized drain (e.g., a closed suction drain) placed deep within the harvest site to prevent hematoma formation, particularly if a large volume of bone was removed.
If the trapdoor technique was utilized, reduce the cortical lid back to its anatomical position. Closure must be robust. Reapproximate the thick lumbodorsal fascia and the periosteum over the crest using heavy, absorbable sutures (e.g., #1 or 0 Vicryl) in an interrupted or continuous locking fashion. Failure to achieve a watertight fascial closure can result in muscle herniation or a clinically significant fascial defect. Close the subcutaneous tissue in layers to eliminate dead space, followed by a meticulous skin closure.
Complications and Management
While posterior iliac crest bone graft harvesting is generally safe, it is not without risk. The overall complication rate is reported to be between 1% and 10%, depending on the volume of graft taken and the specific technique employed.
Superior Cluneal Nerve Injury
The most common nerve injury is to the superior cluneal nerves, resulting in localized anesthesia, dysesthesia, or a painful neuroma over the buttocks. This is almost exclusively caused by extending the incision or dissection further than 8 cm lateral to the PSIS. Management of a neuroma includes local anesthetic/corticosteroid injections, gabapentinoids, and rarely, surgical excision and burying of the nerve stump.
Hematoma and Seroma
Due to the highly vascular nature of the cancellous bone and the extensive dead space created during fascial undermining, hematomas are a frequent complication. Preventative measures include meticulous intraoperative hemostasis, the use of bone wax, and closed suction drainage. If a large, tense hematoma develops postoperatively, it may require bedside aspiration or formal surgical evacuation to prevent secondary infection or wound dehiscence.
Sacroiliac Joint Violation
Violation of the SI joint occurs when curettes or osteotomes are misdirected medially and inferiorly. This leads to chronic, severe mechanical back and pelvic pain. Prevention relies on strict adherence to anatomical landmarks and directing instruments parallel to the outer table of the ilium. If recognized intraoperatively, the defect should not be grafted, and the patient must be monitored for instability.
Pelvic Fracture
Aggressive harvesting, particularly in osteoporotic patients, can lead to fractures of the iliac wing or avulsion fractures of the PSIS. Maintaining a thick cortical strut and utilizing the trapdoor technique minimizes this risk. Postoperative fractures are typically managed non-operatively with protected weight-bearing, though severe displacement may rarely necessitate internal fixation.
Complications Summary Table
| Complication | Estimated Incidence | Etiology / Risk Factor | Salvage / Management Strategy |
|---|---|---|---|
| Cluneal Nerve Neuroma | 1% - 3% | Dissection >8 cm lateral to PSIS. | Gabapentinoids, local injections, surgical excision of neuroma. |
| Hematoma | 3% - 5% | Inadequate hemostasis, large dead space. | Observation if small; surgical evacuation if tense/expanding. |
| SI Joint Violation | < 1% | Medial misdirection of curettes. | Non-operative management; intra-articular injections for chronic pain. |
| Iliac Wing Fracture | 1% - 2% | Osteoporosis, excessive cortical resection. | Protected weight-bearing; rarely requires ORIF. |
| Superior Gluteal Artery Laceration | < 0.5% | Misplaced retractor in sciatic notch. | Emergent packing, pelvic angiography with embolization. |
Post Operative Rehabilitation Protocols
The postoperative rehabilitation protocol following a posterior iliac crest bone graft harvest is almost entirely dictated by the primary surgical procedure (e.g., the spinal fusion or fracture fixation). However, specific attention must be paid to the harvest site.
Pain Management
Harvest site pain is universally reported and can occasionally eclipse the pain of the primary procedure. A multimodal analgesic approach is essential. Intraoperative infiltration of the periosteum and subcutaneous tissues with a long-acting local anesthetic (e.g., liposomal bupivacaine or standard bupivacaine with epinephrine) significantly reduces immediate postoperative narcotic requirements. Systemic NSAIDs (if not contraindicated by the fusion procedure), acetaminophen, and short courses of opioids are standard.
Mobilization and Weight Bearing
Unless contraindicated by the primary orthopedic or spinal intervention, early mobilization is encouraged. Ambulation helps prevent deep vein thrombosis and pulmonary complications. Patients may experience an antalgic gait initially due to gluteal muscle stripping, but this typically resolves within 2 to 4 weeks. If a massive structural graft was taken, or if there is a concern for an impending iliac wing fracture, restricted weight-bearing on the ipsilateral extremity may be instituted for 4 to 6 weeks.
Wound Care
The surgical dressing should remain clean, dry, and intact. If a surgical drain was placed, it is typically discontinued when output falls below 30 cc per 24-hour period. Sutures or staples are removed at 14 to 21 days postoperatively, depending on the patient's healing status and nutritional profile.
Summary of Key Literature and Guidelines
The academic literature extensively supports the use of the posterior iliac crest as the optimal site for autologous bone grafting.
Classic anatomical studies by Colterjohn and Bednar definitively established the safe zone for avoiding the superior cluneal nerves, demonstrating that these neural structures cross the crest a minimum of 7 cm lateral to the PSIS. This anatomical axiom dictates modern surgical approaches to the posterior ilium.
Kurz et al. provided a landmark comprehensive review of the complications associated with iliac crest bone grafting, highlighting that while the anterior approach has a higher rate of lateral femoral cutaneous nerve injuries, the posterior approach is more prone to hematoma formation and potential SI joint violation if meticulous technique is not followed.
Recent meta-analyses comparing autologous bone graft to recombinant human bone morphogenetic protein (rhBMP-2) in spinal surgery indicate that while rhBMP-2 reduces harvest site morbidity, autologous PICBG remains the most cost-effective and biologically reliable method for achieving solid arthrodesis, particularly in revision scenarios or complex nonunions. Consequently, mastering the posterior iliac crest harvest remains an indispensable skill for the modern orthopedic surgeon.
