Ortho Peds Review | Dr Hutaif Pediatric Orthopedics Rev -...
20 Jun 2026
63 min read
128 Views
Key Takeaway
For anyone wondering about ORTHO MCQS PEDS 10, A pediatric orthopaedic examination is the assessment of musculoskeletal symptoms in children, such as limps, pain, or swelling. It helps differentiate benign, self-limited conditions like osteochondrosis of the tarsal navicular from serious pathologies like Ewing's sarcoma. This examination guides appropriate management, ranging from observation and orthotics to advanced diagnostics and specialized treatment.
Ortho Peds Review | Dr Hutaif Pediatric Orthopedics Rev -...
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 6-week-old female infant is currently being treated with a Pavlik harness for Developmental Dysplasia of the Hip (DDH). During her 2-week follow-up appointment, the mother reports that the infant is no longer kicking her left leg. On examination, the infant exhibits a lack of spontaneous knee extension on the left side, though ankle and toe movements are intact. What is the most appropriate next step in management?
Explanation
The clinical presentation is highly suggestive of a femoral nerve palsy, a known complication of Pavlik harness treatment caused by excessive hip flexion. The femoral nerve becomes compressed beneath the inguinal ligament, leading to decreased quadriceps function (lack of knee extension). The most appropriate management is immediate removal of the harness to allow for neurologic recovery, which typically occurs within days to weeks. Once the nerve recovers, a different method of treatment (such as a rigid orthosis or closed reduction) should be considered.
Question 2
A 12-year-old obese male presents with a 4-week history of left groin pain and a limp. He is diagnosed with a stable left slipped capital femoral epiphysis (SCFE) and undergoes in situ pinning. Prophylactic pinning of the contralateral asymptomatic hip is widely debated but is most strongly indicated in patients with which of the following underlying conditions?
Explanation
Prophylactic pinning of the contralateral hip in SCFE is generally recommended for patients with endocrine disorders (e.g., hypothyroidism, growth hormone deficiency, panhypopituitarism), renal osteodystrophy, or a history of prior pelvic radiation. These patients have a significantly higher risk of bilateral involvement compared to the idiopathic SCFE population. The modified Oxford bone age score is also used to determine risk, but among the choices provided, hypothyroidism is the primary indication for prophylactic pinning.
Question 3
An 8-year-old boy is evaluated for a painless limp and restricted hip abduction. Radiographs confirm Legg-Calvé-Perthes disease in the fragmentation stage. According to the Lateral Pillar (Herring) classification, which radiograph is evaluated, and what is the primary determinant for a 'C' classification?
Explanation
The Lateral Pillar (Herring) classification evaluates the AP pelvis radiograph specifically during the fragmentation phase of Legg-Calvé-Perthes disease. It is divided into three groups based on the height of the lateral third of the femoral epiphysis. Group A has no lateral pillar involvement. Group B maintains >50% of lateral pillar height. Group C maintains <50% of lateral pillar height. Age >8 years at onset and a lateral pillar B/C or C grade portend a poor prognosis and typically warrant surgical containment.
Question 4
A 3-year-old child who was successfully treated for an idiopathic right clubfoot via the Ponseti method presents with a relapsed deformity. The parents note that the child walks on the lateral border of the right foot. Examination reveals dynamic supination during the swing phase of gait, but the foot is passively correctable. Which of the following is the most appropriate surgical management?
Explanation
In cases of relapsed clubfoot treated via the Ponseti method, dynamic supination during the swing phase is the most common presentation. If the foot is passively correctable (often achieved with a short period of re-casting), the treatment of choice in a child over 2.5-3 years of age is a full tibialis anterior tendon transfer (TATT) to the lateral cuneiform. A split transfer (SPLATT) is not recommended in Ponseti-treated clubfeet because the medial half of the tendon continues to act as a supinator.
Question 5
A 6-year-old girl with spastic quadriplegic cerebral palsy (GMFCS Level V) is evaluated in the multidisciplinary hip surveillance clinic. Her AP pelvis radiograph demonstrates a Reimers migration percentage (MP) of 55% on the right hip with associated acetabular dysplasia. What is the most widely accepted surgical intervention for this degree of subluxation?
Explanation
In children with cerebral palsy (especially GMFCS levels IV and V), a Reimers migration percentage >40-50% indicates significant hip subluxation that is unlikely to respond to soft tissue release alone. The gold standard surgical management for a displaced and dysplastic hip in this population is a combined procedure: a proximal femoral varus derotational osteotomy (VDRO) combined with a volume-reducing pelvic osteotomy (such as Dega or San Diego) to improve acetabular coverage. Salvage procedures (like resection) are reserved for painful, chronically dislocated, arthritic hips in older patients.
Question 6
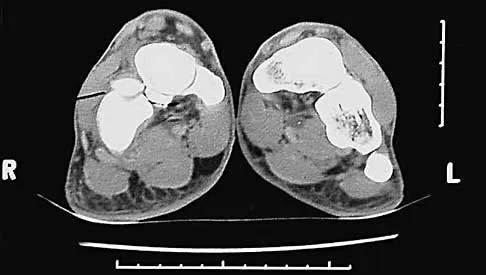
A 13-year-old male presents with recurrent ankle sprains and chronic vague midfoot pain. Physical examination demonstrates a rigid flatfoot with absent subtalar motion. Radiographs reveal a 'C-sign' on the lateral view. A CT scan confirms a talocalcaneal coalition. Which of the following specific anatomical sites is most commonly involved in this type of coalition?
Explanation
Talocalcaneal coalitions most commonly involve the middle facet of the subtalar joint. Radiographically, the 'C-sign' (formed by the medial outline of the talar dome and the inferior outline of the sustentaculum tali) is highly indicative of a middle facet talocalcaneal coalition. Resection of the coalition is typically considered if the coalition involves less than 50% of the posterior facet surface area and there are no significant degenerative changes; otherwise, subtalar fusion may be required.
Question 7
A 2-year-old boy is brought to the clinic for bilateral bowing of the lower extremities. The physician is trying to differentiate between physiological genu varum and infantile Blount's disease. Measurement of the metaphyseal-diaphyseal (MD) angle of Drennan on standing AP radiographs is performed. Which of the following MD angles most strongly indicates a high likelihood of progression to true infantile Blount's disease?
Explanation
The metaphyseal-diaphyseal (MD) angle, described by Drennan, is a critical radiographic parameter to differentiate physiological bowing from infantile tibia vara (Blount's disease). An MD angle greater than 16 degrees has a high positive predictive value for progression to Blount's disease. An angle between 10 and 16 degrees requires close follow-up, while an angle less than 10 degrees is typical for physiologic bowing.
Question 8
A 4-year-old female with blue sclerae and a history of multiple long bone fractures after minimal trauma is diagnosed with Osteogenesis Imperfecta (OI). Genetic testing is ordered. The primary pathophysiology of this condition is a mutation in the COL1A1 or COL1A2 genes leading to the substitution of a crucial amino acid in the triple helix of Type I collagen. Which of the following amino acids is abnormally substituted in this disorder?
Explanation
Osteogenesis Imperfecta is predominantly caused by mutations in the COL1A1 or COL1A2 genes, which encode the alpha-1 and alpha-2 chains of type I collagen. The most common and structurally devastating mutation is a point mutation leading to the substitution of glycine by a bulkier amino acid. Glycine normally occupies every third position (Gly-X-Y) in the collagen alpha chain. Its small side chain (a single hydrogen atom) allows the three alpha chains to pack tightly into the triple helix. Substitution disrupts this tight packing, leading to defective collagen (quantitative or qualitative defects).
Question 9
A 16-month-old male presents with a refusal to bear weight on his left leg and a low-grade fever (38.1°C). His WBC count is normal, but CRP is elevated (35 mg/L). Joint aspiration of the knee yields synovial fluid with 65,000 WBCs/mm³. Standard Gram stain and routine cultures are negative at 48 hours. A specialized PCR of the synovial fluid returns positive for a Gram-negative coccobacillus. Which of the following organisms is the most likely pathogen?
Explanation
Kingella kingae is now recognized as the most common cause of septic arthritis in children between the ages of 6 months and 4 years. It is a slow-growing, Gram-negative coccobacillus that frequently colonizes the oropharynx. It is notoriously difficult to grow on solid routine culture media but grows better when inoculated directly into blood culture vials (BACTEC) or detected via specific PCR assays. Standard Gram stains are often negative.
Question 10
Achondroplasia is the most common form of skeletal dysplasia and short-limb dwarfism. The underlying genetic defect is an activating mutation in the Fibroblast Growth Factor Receptor 3 (FGFR3) gene. In which zone of the epiphyseal growth plate does this mutation primarily exert its inhibitory effect?
Explanation
Achondroplasia is caused by an autosomal dominant, gain-of-function mutation in the FGFR3 gene. FGFR3 normally acts as a negative regulator of bone growth. The mutation leads to constitutive activation of the receptor, which severely inhibits chondrocyte proliferation and differentiation. This primarily affects the proliferative zone of the physis, leading to decreased longitudinal bone growth and the classic rhizomelic dwarfism.
Question 11
A 10-year-old girl is evaluated for an idiopathic limb length discrepancy (LLD). Radiographs indicate her right lower extremity is 20 mm longer than her left. Her bone age matches her chronological age. Utilizing the Menelaus rule of thumb for growth remaining, at what age should an isolated right distal femoral epiphysiodesis be performed to equalize her leg lengths at maturity?
Explanation
According to the Menelaus method (Rule of Thumb), girls complete longitudinal growth at age 14 (boys at 16). The distal femur grows at a rate of approximately 3/8 inch (9 mm or ~1 cm) per year. The proximal tibia grows at 1/4 inch (6 mm) per year. To correct a 20 mm (2 cm) discrepancy using ONLY the distal femur, 20 mm / 9 mm/year = 2.22 years of growth are required. Therefore, the epiphysiodesis should be performed 2.22 years before growth ceases: 14 - 2.2 = 11.8 years of age.
Question 12
An 8-year-old boy presents with an intermittent snapping sensation and catching in the lateral aspect of his left knee. MRI demonstrates a classic complete discoid lateral meniscus. During arthroscopy, the meniscus is found to be hypermobile and translates completely anteriorly with knee extension. Which of the following anatomical variants explains this specific hypermobility?
Explanation
The Wrisberg variant of a discoid meniscus is characterized by an absence of the normal posterior meniscotibial (coronary) ligament attachments. The posterior horn is only tethered by the meniscofemoral ligament of Wrisberg. This lack of posterior capsular attachment allows the meniscus to displace anteriorly into the joint during knee extension, leading to the classic 'snapping knee' syndrome. Treatment requires saucerization and secure stabilization/repair of the posterior horn.
Question 13
A 4-month-old infant is referred to pediatric orthopedics due to an obvious bowing deformity of the right lower leg. Radiographs reveal an anterolateral bow of the tibia with medullary sclerosis and cortical thickening. Based on the most common association with this specific condition, which of the following physical examination findings should the physician actively search for?
Explanation
The clinical and radiographic presentation describes Congenital Pseudarthrosis of the Tibia (CPT), typically preceded by an anterolateral bowing of the tibia. CPT is highly associated with Neurofibromatosis Type 1 (NF-1). More than 50% of patients with CPT have NF-1. Therefore, the physician must thoroughly examine the child for signs of NF-1, such as café-au-lait spots (need 6 or more for diagnosis), axillary/inguinal freckling, or neurofibromas.
Question 14
A 14-year-old male sustains an ankle injury while skateboarding. Radiographs reveal a Salter-Harris III fracture of the anterolateral aspect of the distal tibial epiphysis. This fracture pattern (Tillaux fracture) is specifically dictated by the asymmetric closure of the distal tibial physis. What is the correct chronological order of distal tibial physeal closure?
Explanation
The distal tibial physis undergoes asymmetric closure over an 18-month period. Closure begins centrally, proceeds medially (posteromedial), and finally closes anterolaterally. During this transitional period, an external rotation force causes the anterior inferior tibiofibular ligament (AITFL) to avulse the unfused anterolateral portion of the epiphysis, resulting in a Tillaux fracture (Salter-Harris III).
Question 15
A pediatric orthopedic surgeon is discussing ambulation prognosis with the parents of a child born with myelomeningocele (spina bifida). The infant has a documented neurologic level of L4. Assuming appropriate orthopedic care and bracing are provided, what is the most likely lifelong ambulatory potential for this patient?
Explanation
Ambulation potential in myelomeningocele correlates directly with the lowest functioning motor level. A patient with an L4 level has functioning hip flexors (L1, L2, L3), hip adductors (L2, L3, L4), knee extensors/quadriceps (L2, L3, L4), and medial hamstrings, as well as tibialis anterior (L4, allowing dorsiflexion). The strong quadriceps function is the primary discriminator for community ambulation. These patients typically function as excellent community ambulators but usually require AFOs (due to absent plantar flexion/gluteal weakness) and crutches to prevent crouch gait and optimize efficiency.
Question 16
A 15-month-old child undergoes open reduction for a neglected developmental dysplasia of the hip (DDH) via an anterior approach. During the procedure, several intra-articular anatomical obstacles to reduction are encountered and addressed. Which of the following structures is located most inferiorly and must be incised to allow the femoral head to seat concentrically in the true acetabulum?
Explanation
Obstacles to reduction in DDH include extra-articular structures (iliopsoas tendon, adductor longus) and intra-articular structures. The intra-articular obstacles include the pulvinar (fibrofatty tissue in the cotyloid fossa), an elongated/hypertrophic ligamentum teres, an inverted acetabular labrum (limbus), and a contracted transverse acetabular ligament. The transverse acetabular ligament crosses the acetabular notch at the inferior aspect of the joint. It is often contracted in DDH and must be radially incised (not excised) to allow the femoral head to seat fully.
Question 17
A 9-month-old boy is referred for evaluation of a left thoracic scoliosis. The curve measures 25 degrees on the AP radiograph. The surgeon is determining if this infantile idiopathic scoliosis curve is likely to resolve spontaneously or progress. According to Mehta's criteria, what calculation provides the highest predictive value for curve progression?
Explanation
In infantile idiopathic scoliosis, the Rib-Vertebral Angle Difference (RVAD), described by Mehta, is the most crucial radiographic predictor of progression. It is measured at the apical vertebra. An RVAD > 20 degrees suggests a progressive curve (Phase 2) requiring treatment (typically serial casting or bracing). An RVAD < 20 degrees usually indicates a resolving curve (Phase 1) that can be observed.
Question 18
The pathogenesis of Legg-Calvé-Perthes disease involves avascular necrosis of the capital femoral epiphysis. In a 6-year-old child, the predominant blood supply to the femoral head is provided by the lateral epiphyseal artery. From which parent vessel does this specific artery originate?
Explanation
In children between the ages of 4 and 8 years (the peak age for Perthes disease), the metaphyseal blood supply across the physis decreases dramatically, and the foveal artery provides negligible contribution. The femoral head becomes almost entirely dependent on the lateral epiphyseal artery. This artery is the terminal branch of the medial circumflex femoral artery (MCFA). Disruption or thrombosis of this vessel leads to avascular necrosis of the capital femoral epiphysis.
Question 19
A 6-month-old infant is brought to the emergency department for irritability and swelling of the right knee. Radiographs reveal a distal femoral fracture characterized by a thin layer of metaphyseal bone avulsed at the periphery of the physis. Which of the following best describes the specificity of this injury for non-accidental trauma (child abuse)?
Explanation
The description provided is that of a classic metaphyseal lesion (CML), also known as a 'corner' or 'bucket-handle' fracture. These occur due to forceful pulling, twisting, or shaking (shear forces across the primary spongiosa of the metaphysis). CMLs, along with posterior rib fractures, scapular fractures, and sternal fractures, have a very high specificity for non-accidental trauma (child abuse) and mandate a thorough child protection investigation.
Question 20
A 7-year-old boy with spastic diplegic cerebral palsy is classified as Level III on the Gross Motor Function Classification System (GMFCS). Based on this classification, which of the following best describes his expected functional mobility in community settings?
Explanation
The GMFCS is a 5-level classification system for cerebral palsy.
Level I: Walks without limitations.
Level II: Walks with limitations (e.g., struggles with long distances or uneven terrain).
Level III: Walks using a handheld mobility device (canes, crutches, or walkers) indoors/outdoors, and may use wheeled mobility when traveling long distances.
Level IV: Self-mobility with limitations; may use powered mobility or require assistance.
Level V: Transported in a manual wheelchair in all settings (severe limitations in head and trunk control).
Question 21
A 5-year-old child with spastic quadriplegic cerebral palsy presents for a routine visit. Gross Motor Function Classification System (GMFCS) level is V. Radiographs show a migration percentage of 55% bilaterally with an acetabular index of 35 degrees. What is the most appropriate next step in management?
Explanation
In a non-ambulatory child (GMFCS V) with a high migration percentage (>50%) and significant acetabular dysplasia (acetabular index >30 degrees), a combined approach including a varus derotational osteotomy (VDRO) of the proximal femur and a pelvic osteotomy (e.g., Dega or San Diego) is required to establish stable hip reduction and prevent painful dislocation. Soft tissue release alone is insufficient at this stage.
Question 22
A 4-year-old boy presents with a recurrent clubfoot deformity after successful initial Ponseti casting and Achilles tenotomy in infancy. The mother notes he drops his foot and walks on the lateral border. Examination reveals dynamic supination during the swing phase of gait. Passive range of motion allows the foot to be brought to neutral. What is the most appropriate management?
Explanation
Dynamic supination during swing phase is a classic presentation of recurrent clubfoot deformity caused by an overactive tibialis anterior pulling against a weakened or lengthened antagonist. Since the deformity is flexible passively, the treatment of choice is transferring the tibialis anterior tendon to the lateral cuneiform to balance the foot dynamically. Bony procedures are reserved for fixed deformities.
Question 23
A 6-year-old girl falls off monkey bars and sustains a widely displaced extension-type supracondylar fracture of the humerus. On presentation, her hand is pink and warm, but the radial pulse is absent. Capillary refill is 2 seconds. The anterior interosseous nerve (AIN) function is decreased. She undergoes prompt closed reduction and percutaneous pinning. Post-reduction, the hand remains pink and warm, but the radial pulse remains absent. What is the next step in management?
Explanation
In the setting of a 'pulseless, pink' hand after closed reduction and pinning of a pediatric supracondylar humerus fracture, the standard of care is close observation and admission for 24-48 hours. The collateral circulation is typically sufficient to perfuse the hand. Vascular exploration is indicated if the hand becomes cold, pale, and pulseless (ischemic) despite reduction. AIN palsy is the most common nerve injury in extension-type fractures and usually resolves spontaneously.
Question 24
A 12-year-old obese boy presents to the emergency department with severe acute left hip pain after slipping on ice. He is completely unable to bear weight, even with crutches. Radiographs show a severe left Slipped Capital Femoral Epiphysis (SCFE). Which of the following complications is he at greatest risk for compared to a patient who presents with an ability to bear weight?
Explanation
The inability to bear weight defines an unstable SCFE according to the Loder classification. Unstable SCFE has a significantly higher risk of avascular necrosis (AVN), reported to be up to 20-50%, compared to a nearly 0% risk in stable SCFE. Chondrolysis is more commonly associated with unrecognized hardware penetration into the joint.
Question 25
A 7-year-old boy is diagnosed with Legg-Calvé-Perthes disease. According to the Herring Lateral Pillar Classification, which of the following is the most important radiographic parameter for determining long-term prognosis?
Explanation
The Herring Lateral Pillar Classification is the most reliable prognostic indicator for Legg-Calvé-Perthes disease. It assesses the height of the lateral pillar of the femoral head on an AP radiograph during the fragmentation stage. Group A (>100%), Group B (>50%), and Group C (<50%). Patients with <50% lateral pillar height (Group C) have a poor prognosis and a higher likelihood of an aspherical femoral head and early osteoarthritis.
Question 26
A 3-year-old girl presents with a painless limp. Examination reveals a positive Galeazzi sign and asymmetric thigh folds. Radiographs reveal a dislocated left hip with a broken Shenton's line and an acetabular index of 40 degrees. The right hip is normal. What is the most appropriate primary surgical treatment?
Explanation
In a child older than 2 to 3 years presenting with a completely dislocated hip (Developmental Dysplasia of the Hip), closed reduction is rarely successful and carries a high risk of avascular necrosis. The standard of care is an open reduction combined with a femoral shortening osteotomy (to relieve tension on the reduced hip and decrease AVN risk) and a pelvic osteotomy (e.g., Pemberton or Dega) to address the significant acetabular dysplasia (acetabular index of 40 degrees).
Question 27
A 2-year-old boy presents with anterolateral bowing of the tibia. Radiographs demonstrate a pseudarthrosis of the middle third of the tibia. Examination reveals six café-au-lait spots. Which of the following surgical treatments provides the most reliable long-term outcome for achieving and maintaining union?
Explanation
Congenital pseudarthrosis of the tibia (CPT) is strongly associated with Neurofibromatosis type 1 (NF-1). The pseudarthrosis site contains dense, hamartomatous fibrous tissue that inhibits healing. The standard surgical treatment involves complete resection of this tissue, stabilization with an intramedullary device (e.g., Williams rod or Fassier-Duval rod) that crosses the ankle to prevent recurrent deformity, and copious autogenous bone grafting. Cross-union procedures to the fibula or vascularized fibular grafts are also options.
Question 28
A 4-year-old obese girl presents with bilateral severe genu varum. Standing radiographs demonstrate a metaphyseal-diaphyseal angle (Drennan angle) of 22 degrees bilaterally, with prominent medial metaphyseal beaking. Which of the following is the most appropriate management?
Explanation
The patient has infantile Blount's disease. A Drennan angle >16 degrees is highly predictive of progression. By age 4, the likelihood of success with bracing is very low, and irreversible damage to the medial physis may occur. A proximal tibial valgus osteotomy, often combined with a fibular osteotomy or release, is indicated to acutely correct the deformity and unload the medial physis before permanent physeal arrest occurs. Guided growth (lateral hemiepiphysiodesis) has higher failure rates in severe, early-onset Blount's, particularly in obese patients.
Question 29
A 14-year-old boy presents with a history of recurrent ankle sprains and rigid, painful flatfeet. Examination shows markedly decreased subtalar motion bilaterally and spasm of the peroneal tendons upon passive inversion. Lateral radiographs of the foot demonstrate a continuous bony bridge between the talus and calcaneus, forming a 'C-sign'. Which of the following is the most likely diagnosis?
Explanation
The clinical presentation is classic for a tarsal coalition, characterized by rigid flatfoot and peroneal spasticity. The 'C-sign' on a lateral radiograph is formed by the medial outline of the talar dome and the posterior outline of the sustentaculum tali, strongly indicating a talocalcaneal coalition. Calcanonavicular coalitions are best seen on a 45-degree internal oblique radiograph ('anteater nose' sign).
Question 30
A 5-year-old girl with a history of multiple fractures, blue sclerae, and dentinogenesis imperfecta presents with a new diaphyseal femur fracture. She is currently treated with intravenous pamidronate. What is the primary mechanism of action of this medication in her condition?
Explanation
The patient has Osteogenesis Imperfecta (OI), caused by mutations in COL1A1 or COL1A2. Bisphosphonates, such as pamidronate, are the medical treatment of choice. They act by binding to hydroxyapatite crystals in bone and inhibiting osteoclast-mediated bone resorption. This increases bone mineral density and decreases fracture incidence, though it does not correct the underlying collagen defect.
Question 31
A 7-year-old boy presents with torticollis and severe neck stiffness 2 weeks after an uncomplicated adenotonsillectomy. He is afebrile but has persistent pain, holding his head tilted to the right and rotated to the left. Neurological examination is completely normal. Radiographs demonstrate an asymmetric atlantodental interval. What is the most likely diagnosis?
Explanation
Grisel syndrome is a non-traumatic atlantoaxial subluxation that occurs secondary to an inflammatory process in the upper neck, such as an upper respiratory infection or following head/neck surgery (e.g., adenotonsillectomy). The inflammation leads to laxity of the transverse ligament. Patients present with torticollis (head tilted to one side and rotated to the opposite side). Neurological deficits are rare but can occur.
Question 32
A 10-year-old boy (Tanner stage 1) sustains a midsubstance ACL tear while playing soccer. Following recurrent episodes of instability despite bracing and physical therapy, surgical reconstruction is planned. To minimize the risk of iatrogenic growth arrest, which of the following techniques is most appropriate?
Explanation
In a skeletally immature patient with significant growth remaining (Tanner stage 1 or 2), techniques that avoid drilling across the physes with bone blocks are preferred to prevent growth arrest (leg length discrepancy or angular deformity). An all-epiphyseal reconstruction using a soft tissue graft (like hamstrings) avoids violating the distal femoral and proximal tibial physes. Bone-patellar tendon-bone grafts are contraindicated due to the high risk of physeal damage from the bone plugs.
Question 33
A 12-year-old boy sustains a displaced Salter-Harris type II fracture of the distal femur. He is treated with closed reduction and percutaneous crossed-pin fixation. Due to the specific anatomy and biomechanics of the distal femoral physis, which of the following complications is most frequently encountered with this injury?
Explanation
The distal femoral physis is highly undulated and relies heavily on its structural interlocking for stability. Salter-Harris II fractures here are notorious for causing significant physeal injury during the initial trauma. The incidence of growth arrest (resulting in limb length discrepancy or angular deformity) is extremely high, reported to be up to 40-50%, even with anatomic reduction and appropriate fixation.
Question 34
A 14-year-old boy sustains a twisting ankle injury. Radiographs show a Salter-Harris III fracture of the anterolateral portion of the distal tibial epiphysis. What anatomical characteristic explains this specific fracture pattern?
Explanation
A juvenile Tillaux fracture is a Salter-Harris III avulsion of the anterolateral distal tibial epiphysis by the anterior inferior tibiofibular ligament (AITFL). This occurs because the distal tibial physis closes in an asymmetrical pattern: central, then medial, then posterior, and finally anterolateral. During this specific window of adolescence, the anterolateral physis remains open and is the weakest link when external rotation forces are applied.
Question 35
A newborn is evaluated for a congenital lower extremity deformity. Examination reveals a shortened right leg, anteromedial bowing of the tibia, absence of the lateral two rays of the foot, and a dimple over the anterior aspect of the tibia. What intra-articular knee anomaly is most frequently associated with this diagnosis?
Explanation
The clinical description is classic for fibular hemimelia. It is the most common congenital long bone deficiency. It is characterized by anteromedial tibial bowing, equinovalgus foot, absent lateral rays, and a shortened limb. In the knee, there is a very high association with an absent or hypoplastic anterior cruciate ligament (ACL), leading to anteroposterior instability, though patients often adapt well functionally without reconstruction.
Question 36
A newborn presents with a severe right radial clubhand. Examination shows an absent thumb and radial deviation of the wrist. An echocardiogram reveals an atrial septal defect (ASD). Which of the following syndromes best fits this clinical picture?
Explanation
Holt-Oram syndrome is an autosomal dominant condition characterized by upper extremity anomalies (often radial ray deficiencies, including absent thumb) and congenital heart defects, most commonly an ASD or VSD. In contrast, TAR syndrome features an absent radius but a PRESENT thumb. Fanconi anemia involves bone marrow failure and requires chromosomal breakage testing. VACTERL includes vertebral, anal, cardiac, tracheoesophageal, renal, and limb anomalies, but Holt-Oram is specifically defined by the heart-hand connection.
Question 37
A 3-year-old girl is brought in for a waddling gait and noticeable 'bow legs'. Standing radiographs reveal bilateral genu varum. Which of the following radiographic parameters is the most reliable for differentiating infantile Blount's disease from resolving physiologic genu varum?
Explanation
The metaphyseal-diaphyseal angle (MDA), or Drennan angle, is the most reliable radiographic tool to differentiate physiologic bowing from infantile Blount's disease. An MDA greater than 16 degrees has a high positive predictive value for progression to Blount's disease, while an angle less than 10 degrees suggests physiologic bowing that will likely resolve.
Question 38
A 3-year-old boy presents with an isolated, closed spiral fracture of the midshaft of the femur after falling from a toddler bed. He weighs 16 kg (35 lbs). The fracture is shortened by 1 cm. What is the most appropriate definitive management?
Explanation
For pediatric femoral shaft fractures in children under 5 years of age and weighing less than 50 lbs (22.7 kg), early hip spica casting is the standard of care. It provides excellent outcomes with minimal risk of complications. Flexible intramedullary nails are typically indicated for children aged 5 to 11 years. Rigid nailing is contraindicated due to the risk of avascular necrosis of the femoral head from piriformis fossa entry.
Question 39
A 5-year-old boy presents with a painless limp. Examination reveals a positive Trendelenburg sign on the right. Radiographs show a right neck-shaft angle of 95 degrees, a vertical proximal femoral physis, and an inverted Y-shaped radiolucency in the inferior femoral neck. What radiographic measurement is the primary indication to perform a valgus-producing subtrochanteric osteotomy?
Explanation
The diagnosis is developmental coxa vara. The Hilgenreiner-epiphyseal angle (HEA) is used to predict progression and guide treatment. An HEA > 60 degrees indicates a high likelihood of progression and is a clear indication for surgical intervention (valgus subtrochanteric osteotomy). An HEA < 45 degrees usually resolves spontaneously. Angles between 45 and 60 degrees require close observation.
Question 40
A 7-year-old girl presents with a prominent snapping sensation and pain in her lateral knee when squatting. Examination reveals a palpable clunk on knee flexion and extension. MRI confirms a complete, symptomatic discoid lateral meniscus with a peripheral tear. What is the most appropriate surgical treatment?
Explanation
Symptomatic discoid menisci, especially those with an associated peripheral tear (Wrisberg variant or standard tear), are best treated with partial meniscectomy (saucerization) to reshape the meniscus to a more normal crescentic form, combined with repair of the peripheral tear. Total meniscectomy is avoided in children due to the extremely high risk of early, severe compartment osteoarthritis.
Question 41
A 4-year-old girl presents with a unilaterally elevated left shoulder. Physical exam reveals restricted abduction of the left shoulder and a noticeably smaller left scapula. Radiographs confirm an elevated scapula with an omovertebral bone connecting the cervical spine to the superior angle of the scapula. Which of the following conditions is most commonly associated with this congenital deformity?
Explanation
Sprengel's deformity is a congenital failure of descent of the scapula. The most common associated condition is Klippel-Feil syndrome (congenital cervical spine fusion), seen in up to 30% of cases. The omovertebral bone is a fibrous, cartilaginous, or osseous connection found in roughly 30% of Sprengel patients.
Question 42
A newborn male is noted to have a limb length discrepancy and deformity of the right lower extremity. Radiographs reveal partial absence of the fibula, anteromedial bowing of the tibia, and a foot with three digits. Which of the following foot deformities is most characteristically associated with this condition?
Explanation
Fibular hemimelia is the most common congenital long bone deficiency. It is characterized by partial or complete absence of the fibula, anteromedial bowing of the tibia, absence of lateral rays of the foot, and an equinovalgus foot deformity. Associated findings include femoral shortening (PFFD), cruciate ligament deficiency, and a ball-and-socket ankle joint.
Question 43
A newborn presents with a rigid flatfoot deformity characterized by a convex plantar surface (rocker-bottom foot). Radiographs show the talus in a severe plantarflexed position. On a maximum plantarflexion lateral radiograph, the navicular remains dorsally dislocated on the talar neck. What is the most appropriate initial management for this condition?
Explanation
Congenital vertical talus (CVT) is characterized by a fixed dorsal dislocation of the navicular on the talus. The most appropriate initial management is the Dobbs method, which involves serial manipulation and casting (stretching the forefoot into plantarflexion and inversion to align it with the plantarflexed talus), followed by minimally invasive pinning of the talonavicular joint and percutaneous Achilles tenotomy.
Question 44
A 6-year-old boy with spastic quadriplegic cerebral palsy is evaluated for hip instability. An AP pelvis radiograph is obtained and the Reimers migration percentage is calculated. At what migration percentage is surgical intervention (e.g., adductor/iliopsoas release or reconstructive osteotomy) generally indicated to prevent frank hip dislocation?
Explanation
The Reimers migration percentage (MP) measures the percentage of the femoral head outside of the acetabulum (lateral to Perkins line). An MP > 30% is a critical threshold in children with cerebral palsy, indicating significant hip subluxation. It generally prompts surgical intervention such as soft tissue release or varus derotational osteotomy (VDRO) with pelvic osteotomy depending on the patient's age and degree of dysplasia.
Question 45
A 5-year-old boy falls from monkey bars and sustains a widely displaced extension-type supracondylar humerus fracture. On presentation, the hand is pink but the radial pulse is absent. After urgent closed reduction and percutaneous pinning, the hand remains well-perfused (pink and warm with brisk capillary refill) but the radial pulse remains absent. What is the most appropriate next step in management?
Explanation
In a pediatric supracondylar humerus fracture presenting with a 'pink, pulseless' hand, the initial step is closed reduction and pinning. If the hand remains pink and well-perfused with an absent radial pulse after adequate reduction and stabilization, the standard of care is close observation. The collateral circulation is sufficient to maintain limb viability, and the pulse typically returns over days to weeks. Surgical exploration is indicated for a 'white, pulseless' hand that does not improve after reduction.
Question 46
A 13-year-old girl sustains an ankle injury while playing soccer. Radiographs reveal a Salter-Harris III fracture of the anterolateral aspect of the distal tibial epiphysis. What is the mechanism of injury and the anatomic structure responsible for avulsing this fragment?
Explanation
A juvenile Tillaux fracture is a Salter-Harris type III fracture of the anterolateral distal tibial epiphysis. It occurs in adolescents due to the asymmetric closure pattern of the distal tibial physis (closing centrally first, then medially, then laterally). An external rotation force causes the anterior inferior tibiofibular ligament (AITFL) to avulse the unfused anterolateral epiphysis.
Question 47
A 9-year-old boy presents with an asymptomatic snapping sensation in his right knee, which his mother notes occurs predominantly when he extends his knee. He has no history of trauma, pain, or swelling. Which of the following anatomic variations is most likely responsible for this symptomatic presentation?
Explanation
The patient has the Wrisberg variant of a discoid lateral meniscus. This variant is characterized by the absence of the normal posterior meniscotibial capsular attachments; its only posterior attachment is the meniscofemoral ligament of Wrisberg. This instability allows the meniscus to subluxate anteriorly during knee extension, producing a palpable or audible 'snap' or 'clunk'.
Question 48
A 5-year-old child with a known diagnosis of Morquio syndrome (Mucopolysaccharidosis Type IV) is scheduled to undergo bilateral lower extremity osteotomies for severe genu valgum. Before proceeding with any surgical intervention involving general anesthesia, what is the most critical screening evaluation required?
Explanation
Morquio syndrome (MPS IV) is a skeletal dysplasia characterized by normal intelligence but profound skeletal changes, including odontoid hypoplasia. Odontoid hypoplasia leads to life-threatening atlantoaxial instability. This places the child at extreme risk for spinal cord injury or death during intubation and neck extension for surgery. Therefore, a cervical spine MRI (or flexion/extension radiographs if reliable) is mandatory prior to anesthesia.
Question 49
A 10-month-old infant with achondroplasia is noted to have a persistent thoracolumbar kyphosis. Which of the following statements regarding the natural history and management of this deformity is most accurate?
Explanation
Thoracolumbar kyphosis is present in up to 90% of infants with achondroplasia. It is primarily positional, exacerbated by relative hypotonia and large head size, and typically resolves spontaneously once the child develops truncal muscle strength and begins to walk independently. Bracing or surgery is rarely indicated unless it persists and becomes a fixed structural deformity (wedged vertebrae) later in childhood.
Question 50
A newborn is diagnosed with radial longitudinal deficiency (radial clubhand). The right thumb is completely absent. You are counseling the parents on the management plan. Prior to any reconstructive orthopedic surgical intervention such as centralization of the carpus on the ulna, which of the following is an absolute prerequisite regarding the affected upper extremity?
Explanation
In radial longitudinal deficiency, centralization of the carpus on the distal ulna is often performed to improve alignment and function. However, adequate passive elbow flexion is an absolute prerequisite. If the elbow is stiff in extension (which can occur in these patients), centralizing the wrist will leave the child completely unable to reach their mouth for feeding. The radial deviation of the hand actually helps them reach their face if the elbow cannot flex.
Question 51
A 2-year-old boy with multiple café-au-lait spots and axillary freckling presents with marked anterolateral bowing of his left tibia. Radiographs demonstrate diaphyseal narrowing and cystic changes. What is the most appropriate surgical management to prevent or treat pseudoarthrosis in this condition once indicated?
Explanation
Congenital anterolateral bowing of the tibia is highly associated with Neurofibromatosis type 1 (NF1) and frequently progresses to a recalcitrant pseudoarthrosis due to abnormal hamartomatous tissue in the periosteum. The standard surgical treatment involves radical excision of the diseased periosteum and pseudoarthrosis, autologous bone grafting, and intramedullary rodding (often combined with an external fixator to maximize stability).
Question 52
A 10-year-old boy presents with a painful, swollen knee after falling off his bicycle. Radiographs reveal a displaced, completely elevated fracture of the anterior tibial spine (Meyers and McKeever Type 3). Which of the following structures is most commonly entrapped, blocking anatomic closed reduction?
Explanation
In Meyers and McKeever Type 3 tibial eminence (spine) fractures, the anterior horn of the medial meniscus is the most common structure that becomes entrapped under the avulsed fragment, blocking anatomic reduction. The intermeniscal ligament can also be involved. This entrapment necessitates arthroscopic or open reduction.
Question 53
A 12-year-old boy sustains an elbow dislocation. After closed reduction in the emergency department, a post-reduction radiograph shows the ulnohumeral joint is concentrically reduced, but there is a displaced medial epicondyle fracture. What is an absolute indication for open reduction and internal fixation of this fracture?
Explanation
Absolute indications for operative intervention (ORIF) of a medial epicondyle fracture include incarceration of the fracture fragment within the joint (often recognized by a non-concentric reduction or visible fragment on post-reduction X-ray) and an open fracture. Entrapment of the ulnar nerve is also considered an absolute or strong relative indication. Displacement > 5-15 mm and high-demand overhead athletic activity are debated relative indications.
Question 54
A 6-month-old infant is brought to the clinic with bilateral femur fractures and blue sclerae. Genetic testing confirms a diagnosis of Osteogenesis Imperfecta (OI). This condition is primarily caused by a mutation affecting the synthesis of which of the following proteins?
Explanation
Osteogenesis Imperfecta is a group of genetic disorders that mainly affect the formation of Type I collagen, the major structural protein in bone, skin, and sclerae. The mutations typically occur in the COL1A1 or COL1A2 genes, leading to decreased production or abnormal structure of collagen, resulting in brittle bones, blue sclerae, and dentinogenesis imperfecta.
Question 55
An 8-year-old boy is diagnosed with Legg-Calvé-Perthes disease. Which of the following radiographic findings is considered a 'head at risk' sign, portending a poorer prognosis and a higher risk of femoral head deformation?
Explanation
Catterall described 'head at risk' signs in Legg-Calvé-Perthes disease, which indicate a high risk for progressive subluxation and a poorer outcome. These include: Gage sign (a V-shaped radiolucency in the lateral portion of the epiphysis and adjacent metaphysis), lateral (not medial) subluxation of the femoral head, calcification lateral to the epiphysis, diffuse metaphyseal reaction, and a horizontal physis.
Question 56
A 1-year-old child is evaluated for a markedly shortened right lower extremity. Radiographs show a shortened femur, an absent femoral head, and no bony connection between the proximal femur and the acetabulum. The tibia is relatively normal in length, but the fibula is absent. What classification system is most commonly used for this specific femoral condition?
Explanation
The Aitken classification is used for Proximal Focal Femoral Deficiency (PFFD). It evaluates the presence of the femoral head, the continuity of the femoral shaft with the neck/head, and the severity of the deficiency (Classes A through D). Langenskiöld is for Blount disease. Herring is for Perthes disease. Gartland is for supracondylar humerus fractures.
Question 57
A 4-year-old, significantly overweight boy presents with progressive bowing of both legs. Standing radiographs reveal bilateral genu varum, metaphyseal-diaphyseal angles of 20 degrees, and medial physeal beaking of the proximal tibiae. What is the primary pathophysiologic mechanism underlying this condition?
Explanation
Blount disease (tibia vara) is an acquired condition resulting from mechanical overload of the posteromedial aspect of the proximal tibial physis. According to the Hueter-Volkmann principle, excessive compressive forces inhibit physeal growth. This leads to progressive varus, flexion, and internal rotation deformity of the tibia.
Question 58
A 4-week-old infant is brought to the clinic for a right-sided neck mass and a head tilt. The infant's head is tilted to the right and rotated to the left. Palpation reveals a firm, non-tender 'olive-like' mass in the right sternocleidomastoid muscle. What is the most appropriate initial management?
Explanation
The clinical presentation is classic for congenital muscular torticollis with a sternocleidomastoid (SCM) tumor (fibromatosis colli). Initial management consists of parental education, repositioning, and physical therapy for passive stretching of the affected SCM muscle. Over 90% of cases resolve with conservative management. Surgery is reserved for cases refractory to at least 6-12 months of dedicated therapy.
Question 59
A 13-year-old boy with Duchenne muscular dystrophy, who uses a wheelchair full-time, develops a progressive neuromuscular scoliosis measuring 35 degrees. His forced vital capacity (FVC) is 45% of predicted. What is the most appropriate recommendation for managing his spinal deformity?
Explanation
In patients with Duchenne muscular dystrophy, scoliotic curves progress rapidly once wheelchair-bound. Bracing is ineffective and poorly tolerated. Posterior spinal fusion is recommended early, typically when the curve exceeds 20-30 degrees, while the patient's pulmonary function is still adequate (FVC > 35% predicted). Delaying surgery increases cardiopulmonary risks. Fusion is typically extended to the pelvis to correct pelvic obliquity and provide a level sitting base.
Question 60
A 12-year-old gymnast presents with persistent lower back pain. Radiographs reveal a Grade II isthmic spondylolisthesis at L5-S1. She is neurologically intact. After failing 6 months of dedicated physical therapy, bracing, and activity modification, her back pain remains disabling. What is the most appropriate surgical treatment?
Explanation
For pediatric patients with symptomatic low-grade (Grade I or II) isthmic spondylolisthesis that fails conservative management, the standard surgical treatment is an L5-S1 in situ posterolateral fusion. Decompression (Gill procedure) alone is contraindicated in children as it increases instability and slip progression. Reduction of low-grade slips is unnecessary and carries a high risk of L5 nerve root injury without added clinical benefit.
Question 61
In the Ponseti method for the management of idiopathic clubfoot, what is the correct sequence of deformity correction?
Explanation
The sequence of correction in the Ponseti method is Cavus, Adductus, Varus, and finally Equinus (CAVE). Elevating the first ray corrects the cavus and unlocks the midfoot for further corrective casting.
Question 62
A 6-year-old boy presents with a displaced lateral condyle fracture of the humerus. Which of the following is the most common long-term complication if this fracture goes on to nonunion?
Explanation
Nonunion of a lateral condyle fracture typically results in a progressive cubitus valgus deformity. This valgus angulation stretches the ulnar nerve over time, leading to tardy ulnar nerve palsy.
Question 63
A 14-year-old girl is diagnosed with adolescent idiopathic scoliosis (AIS). Her Lenke classification is 1AN. Which of the following best describes the structural characteristics of her curve?
Explanation
Lenke 1 curves are main thoracic structural curves with non-structural proximal thoracic and thoracolumbar curves. The "A" modifier indicates the lumbar apex falls between the pedicles, and "N" designates normal thoracic kyphosis.
Question 64
A 7-year-old child presents with an acute inability to bear weight on the right leg. Kocher's criteria are used to differentiate septic arthritis from transient synovitis. Which of the following is NOT one of the original four Kocher criteria?
Explanation
The original Kocher criteria include non-weight-bearing, fever > 38.5°C, ESR > 40 mm/hr, and WBC > 12,000/mm³. Although CRP is a highly sensitive modern marker, it was not included in Kocher's original 1999 study.
Question 65
An 18-month-old girl with Developmental Dysplasia of the Hip (DDH) is planned for a Salter innominate osteotomy. Which of the following is an absolute prerequisite for performing this procedure?
Explanation
A Salter osteotomy is a redirectional pelvic osteotomy that hinges through the symphysis pubis. A concentric reduction of the hip joint is an absolute prerequisite for the procedure to provide adequate anterolateral coverage.
Question 66
A 14-year-old boy presents with right knee pain following a twisting injury. Radiographs reveal a Salter-Harris III fracture of the anterolateral aspect of the distal tibia epiphysis. Which ligament's pull is primarily responsible for this avulsion fracture?
Explanation
This is a Tillaux fracture, caused by avulsion of the anterolateral distal tibial epiphysis due to pull from the anterior inferior tibiofibular ligament (AITFL). It occurs in adolescents because the lateral physis is the last portion to close.
Question 67
A newborn is noted to have a missing thumb and severe radial deviation of the wrist. Radiographs confirm radial clubhand. Which of the following screening tests is most appropriate to rule out a potentially fatal associated condition?
Explanation
Radial clubhand is strongly associated with Fanconi anemia, a life-threatening aplastic anemia syndrome. It is screened via chromosomal breakage analysis using clastogenic agents like diepoxybutane (DEB).
Question 68
A 5-year-old boy presents with bilateral genu varum. Standing radiographs show proximal tibial metaphyseal beaking, and the metaphyseal-diaphyseal angle is 18 degrees. Which of the following is the most appropriate management?
Explanation
This patient has late-onset infantile Blount's disease with a metaphyseal-diaphyseal angle > 16 degrees, making spontaneous resolution highly unlikely. Surgical intervention with a proximal tibial valgus osteotomy is indicated for severe or progressive cases in children over 4 years old.
Question 69
A 12-year-old boy presents with a painful, rigid flatfoot. Radiographs demonstrate a 'C-sign' on the lateral view of the foot. Which of the following is the most likely diagnosis?
Explanation
The 'C-sign' on a lateral foot radiograph is classic for a talocalcaneal (subtalar) coalition, representing a continuous bony outline from the talar dome to the sustentaculum tali. Calcaneonavicular coalitions typically display the 'anteater nose' sign.
Question 70
A child with cerebral palsy is evaluated for hip subluxation. The Reimers Migration Index (MI) is measured on an AP pelvis radiograph. At what minimum MI percentage is prophylactic surgical intervention (e.g., adductor tenotomy) typically recommended?
Explanation
A Reimers Migration Index exceeding 30-33% indicates significant, progressive hip subluxation in cerebral palsy. Soft tissue releases, such as adductor longus and iliopsoas tenotomies, are typically recommended at this threshold to prevent complete dislocation.
Question 71
A 9-year-old boy presents with a progressive leg length discrepancy. He has a history of an isolated lateral distal femoral physeal arrest after trauma. If left untreated, which of the following deformities will develop?
Explanation
Premature arrest of the lateral distal femoral physis allows the medial side to continue growing unchecked. This asymmetric growth pushes the knee into a varus alignment, combined with overall limb shortening.
Question 72
A 3-year-old girl is diagnosed with a diaphyseal femur fracture after a low-energy fall. She weighs 18 kg (40 lbs). Which of the following is the most appropriate definitive treatment?
Explanation
For children aged 1 to 5 years weighing less than 20 kg (44 lbs) with an isolated diaphyseal femur fracture, early hip spica casting is the gold standard. Flexible intramedullary nailing is typically reserved for children aged 5 to 11 years.
Question 73
Which of the following genetic mutations is responsible for Achondroplasia, the most common form of disproportionate short-stature dwarfism?
Explanation
Achondroplasia is caused by an activating mutation in the Fibroblast Growth Factor Receptor 3 (FGFR3) gene. This overactivity profoundly inhibits chondrocyte proliferation within the proliferative zone of the physis.
Question 74
A newborn is diagnosed with congenital vertical talus. What is the classic radiographic relationship between the talus and the navicular in this condition?
Explanation
Congenital vertical talus creates a rigid rocker-bottom foot deformity. Radiographically, the hallmark is a rigid dorsal dislocation of the navicular upon a vertically oriented, plantarflexed talus.
Question 75
A 10-year-old girl is brought in for a mild limp. Radiographs show a centrally located, lytic lesion in the proximal humerus metaphysis with a 'fallen leaf' sign. She has minimal pain after a minor fall. What is the most likely diagnosis?
Explanation
The 'fallen leaf' or 'fallen fragment' sign is pathognomonic for a Unicameral Bone Cyst (UBC) that has sustained a pathologic fracture. A piece of cortical bone breaks off and settles at the dependent portion of the fluid-filled cyst.
Question 76
A 7-year-old boy sustains a completely displaced extension-type supracondylar humerus fracture. Upon examination, he is unable to flex the interphalangeal joint of his thumb or the distal interphalangeal joint of his index finger. Which nerve is most likely injured?
Explanation
The Anterior Interosseous Nerve (AIN) is the most frequently injured nerve in extension-type supracondylar fractures. Clinically, AIN palsy presents as the inability to form an 'OK' sign due to weakness of the flexor pollicis longus and flexor digitorum profundus to the index finger.
Question 77
A 14-year-old obese male presents with left groin pain and an altered gait. Radiographs reveal a slipped capital femoral epiphysis (SCFE). Which of the following is the most significant clinical predictor for the development of subsequent avascular necrosis (AVN)?
Explanation
The inability to bear weight defines an unstable SCFE according to the Loder classification. Instability is the paramount risk factor for developing AVN, carrying a risk of up to 50% compared to near 0% in stable slips.
Question 78
A 2-year-old boy presents with a history of recurrent fractures following minimal trauma. Physical exam reveals blue sclerae and delayed dentition. Which of the following accurately describes the underlying molecular defect?
Explanation
The patient's presentation of multiple fragility fractures, blue sclerae, and dentinogenesis imperfecta is classic for Osteogenesis Imperfecta (OI). OI is caused by mutations in the COL1A1 or COL1A2 genes, resulting in defective Type I collagen synthesis.
Question 79
A 13-year-old gymnast complains of refractory lower back pain. Radiographs reveal an isthmic spondylolisthesis at L5-S1 with a 60% slip (Meyerding Grade III). Which surgical option is most appropriate if conservative management fails?
Explanation
A high-grade slip (>50%) in an actively growing adolescent is highly unstable and poses a significant risk for progression. Surgical management typically requires instrumented stabilization and fusion (posterolateral with or without interbody fusion) to halt progression and alleviate symptoms.
Question 80
A 6-month-old infant is diagnosed with congenital fibular hemimelia. Which of the following associated clinical findings is most universally expected with this deficiency?
Explanation
Fibular hemimelia is frequently associated with a spectrum of lower limb anomalies, most notably the absence or severe hypoplasia of the anterior cruciate ligament (ACL). Other hallmark associations include anterolateral tibial bowing and absent lateral rays of the foot.
Question 81
A 4-week-old female infant is evaluated for developmental dysplasia of the hip (DDH). Ultrasound shows an alpha angle of 45 degrees and a beta angle of 65 degrees. According to the Graf classification, what is the appropriate management?
Explanation
An alpha angle of 45 degrees indicates a Graf type IIc or worse (dysplastic hip). The standard of care for a dysplastic but reducible hip in an infant under 6 months is treatment with a Pavlik harness.
Question 82
A 14-year-old male with a BMI of 35 presents with acute-on-chronic left knee pain and an inability to bear weight. Radiographs show a severe left slipped capital femoral epiphysis (SCFE). He undergoes urgent in situ pinning. Which of the following is the most significant preventable risk factor for developing chondrolysis in this patient?
Explanation
Unrecognized hardware penetration into the joint space is the most significant preventable risk factor for chondrolysis following in situ pinning of a SCFE. Intraoperative fluoroscopy with approach-withdrawal views is essential to confirm extra-articular pin placement.
Question 83
A 6-month-old boy with idiopathic clubfoot was successfully treated with the Ponseti method. After serial casting and a percutaneous Achilles tenotomy, his foot is fully corrected. What is the most common cause of relapse in this patient over the next few years?
Explanation
The most common cause of clubfoot relapse following successful correction with the Ponseti method is non-compliance with the foot abduction brace. The brace must be worn full-time initially, then at night until age 3 to 4 years.
Question 84
An 8-year-old girl is evaluated for severe in-toeing. On examination, she has 80 degrees of internal hip rotation and 10 degrees of external hip rotation bilaterally. The thigh-foot angle is neutral. What is the most likely diagnosis and its expected natural history?
Explanation
Increased internal hip rotation and decreased external rotation indicate increased femoral anteversion. This condition typically peaks around age 5-6 and spontaneously resolves or compensates by age 10-12 without surgical intervention.
Question 85
A 4-year-old boy presents with progressive bowing of his left leg. Radiographs reveal a prominent medial metaphyseal beak, lucency, and an epiphyseal-metaphyseal angle of 20 degrees. What is the most appropriate management?
Explanation
The patient has infantile Blount disease with significant radiographic changes (epiphyseal-metaphyseal angle > 16 degrees). At age 4, bracing is ineffective, making a proximal tibial corrective osteotomy the treatment of choice to prevent permanent deformity.
Question 86
A 10-year-old boy with spastic diplegic cerebral palsy is evaluated for bilateral hip subluxation. His Reimers migration percentage is 50% bilaterally, and he experiences pain with seating. What is the most appropriate surgical intervention?
Explanation
In a child with cerebral palsy and a Reimers migration percentage > 40-50%, soft tissue releases alone are insufficient. Bony reconstruction with VDRO and a pelvic osteotomy is required to restore joint congruency and stability.
Question 87
A 3-year-old girl is evaluated for multiple recurrent fractures with minimal trauma. She has blue sclerae and mild bowing of her femurs. Genetic testing confirms a mutation affecting type I collagen. Which of the following medical treatments is most commonly used to decrease fracture frequency in this condition?
Explanation
Intravenous bisphosphonates (e.g., pamidronate) are the standard of care in moderate to severe Osteogenesis Imperfecta. They inhibit osteoclast activity, increase bone mineral density, and significantly reduce fracture rates.
Question 88
A 13-year-old boy sustains a Salter-Harris type III fracture of the anterolateral distal tibia. Which of the following best explains the specific fracture pattern seen in this Tillaux fracture?
Explanation
A Tillaux fracture occurs due to the asymmetric closure of the distal tibial physis, which closes first centrally, then medially, and finally laterally. An external rotation force causes the anterior inferior tibiofibular ligament to avulse the unfused anterolateral epiphysis.
Question 89
A 7-year-old boy presents with a painless limp. Radiographs reveal fragmentation of the left capital femoral epiphysis. Physical exam shows a loss of hip internal rotation and abduction. What is the primary overarching goal of treatment for this condition?
Explanation
In Legg-Calvé-Perthes disease, the primary goal of treatment is containment of the inflamed, plastic femoral head within the acetabulum. This maintains a spherical head shape during the remodeling phase and minimizes future joint incongruity.
Question 90
A 12-year-old girl complains of vague, recurrent foot pain and frequent ankle sprains. Examination shows a rigid flatfoot with no arch reconstitution on toe-standing. Radiographs reveal a "C sign" on the lateral view. What is the most likely diagnosis?
Explanation
A talocalcaneal coalition often presents as a rigid flatfoot in early adolescence. It is radiographically characterized by the "C sign" on a lateral view, formed by the medial outline of the talar dome and the inferior outline of the sustentaculum tali.
Question 91
A 5-year-old boy with Down syndrome presents with neck pain and torticollis following a minor fall. Neurological examination is completely normal. Open-mouth odontoid radiographs reveal an atlanto-dens interval (ADI) of 6 mm. What is the most appropriate initial management?
Explanation
An ADI of up to 4-5 mm can be normal in children, but 6 mm indicates mild atlantoaxial instability common in Down syndrome. Without neurologic symptoms, conservative management with activity restriction and close follow-up is indicated.
Question 92
A neonate is diagnosed with bilateral clubfeet. The parents ask about the specific sequence of deformity correction using the Ponseti method. What is the correct order of correction?
Explanation
The Ponseti method corrects clubfoot deformities in a very specific sequence: Cavus (by supinating the forefoot), Adductus, Varus, and finally Equinus (CAVE). Equinus is usually corrected last, often requiring a percutaneous Achilles tenotomy.
Question 93
A 6-year-old boy sustained a supracondylar humerus fracture treated with closed reduction and percutaneous pinning. Several years later, he presents with a noticeable cosmetic deformity of his elbow, though his range of motion is full and painless. What is the most likely deformity, and how does it affect elbow function?
Explanation
Malunion of a supracondylar humerus fracture most commonly results in cubitus varus (gunstock deformity). This is typically a cosmetic deformity that does not significantly restrict range of motion or daily function.
Question 94
A 9-year-old boy presents with knee pain. Radiographs and an MRI reveal a stable osteochondritis dissecans (OCD) lesion on the lateral aspect of the medial femoral condyle. There is no fluid behind the lesion. What is the most appropriate initial management?
Explanation
In a skeletally immature patient with a stable OCD lesion (intact articular cartilage, no fluid behind the lesion on MRI), initial management is non-operative. Activity modification and protected weight-bearing yield a high rate of spontaneous healing.
Question 95
A 2-year-old girl presents with a limp. Radiographs reveal a lytic lesion in the proximal femur with a "ground-glass" appearance and a coxa vara deformity. The mother has a history of café-au-lait spots. What is the most likely diagnosis?
Explanation
A "ground-glass" lytic lesion causing deformity (like coxa vara or shepherd's crook) is characteristic of fibrous dysplasia. The presence of café-au-lait spots suggests McCune-Albright syndrome, which is associated with polyostotic fibrous dysplasia.
None
Previous ChapterOrthopedic Pediatrics Review | Dr Hutaif Pediatric Orth -...
Next Chapter Pediatric Orthopedic MCQs Online: Advanced Exam & Review

Medically Verified Content by
Prof. Dr. Mohammed Hutaif Clinic
Consultant Orthopedic & Spine Surgeon