Cervical Instability in Down Syndrome: Comprehensive Surgical Management
Key Takeaway
Cervical instability in Down syndrome arises from inherent collagen defects causing ligamentous laxity at the atlantoaxial and atlantooccipital joints. While often asymptomatic, progressive instability can lead to severe neurological compromise. Diagnosis relies on precise radiographic measurements, including the atlantodens interval and Powers ratio. Operative management is indicated for significant instability or neurological deficits, requiring meticulous surgical technique, rigid fixation, and prolonged postoperative immobilization to mitigate high rates of graft resorption.
Comprehensive Introduction and Patho-Epidemiology
Cervical instability in patients with Down syndrome (Trisomy 21) represents a profoundly complex intersection of genetic collagen synthesis abnormalities, generalized ligamentous laxity, and unique osteocartilaginous morphology. The underlying structural defect primarily involves aberrations in Type VI collagen, which fundamentally compromises the tensile strength, structural integrity, and viscoelastic properties of the critical stabilizing ligaments of the upper cervical spine. Trisomy 21 leads to an overexpression of the genes located on the 21st chromosome, specifically the COL6A1 and COL6A2 genes, resulting in a disorganized extracellular matrix. This intrinsic biochemical defect predisposes this highly vulnerable patient population to both atlantoaxial instability (AAI) and atlantooccipital instability (AOI), creating a clinical scenario where the cervical spine is inherently ill-equipped to handle standard biomechanical loads.
The epidemiological prevalence of asymptomatic atlantoaxial instability in the Down syndrome population is remarkably high, with radiographic evidence present in approximately 10% to 30% of individuals. However, the academic and clinical paradox lies in the fact that despite this high radiographic prevalence, clinically significant neurological symptoms manifest in only 1% to 2.6% of these patients. Consequently, instability is most frequently identified incidentally during routine radiographic screening, pre-anesthetic evaluations, or assessments required for participation in athletic events such as the Special Olympics. When progressive instability leads to neurological compromise, it is most frequently observed in males older than 10.5 years of age, as historically noted by Burke et al. The clinical presentation is typically insidious, driven by repetitive microtrauma to the spinal cord or acute dynamic compression during hyperflexion or hyperextension events.
Furthermore, it is imperative for the orthopedic spine surgeon to recognize the high prevalence of concurrent osseous anomalies in the upper cervical spine of these patients. Pueschel and colleagues demonstrated that nearly 60% of evaluated patients with Down syndrome exhibited structural cervical spine defects alongside ligamentous laxity. These anomalies include, but are not limited to, os odontoideum, odontoid hypoplasia, assimilation of the atlas (occipitalization), and incomplete ossification of the posterior arch of C1. These osseous anomalies are statistically more prevalent in patients with documented atlantoaxial instability. The academic debate remains ongoing regarding whether these osseous anomalies are the primary etiology of the instability or a secondary adaptive response to chronic ligamentous laxity and abnormal biomechanical stress. Regardless of the developmental sequence, their presence fundamentally alters the surgical approach, fixation strategy, and overall prognosis.
When evaluating a patient with Down syndrome, the clinician must never assume the instability is purely ligamentous. A high index of suspicion for concurrent osseous anomalies must be maintained, as these structural deficits dictate the feasibility of specific instrumentation techniques. The diagnostic challenge is further compounded by the varying degrees of intellectual disability and communication barriers inherent to this population. Subtle signs of myelopathy—such as a deteriorating gait, loss of fine motor skills, or declining physical endurance—can easily be missed, misattributed to baseline developmental delays, or dismissed as behavioral changes. Therefore, a comprehensive understanding of the patho-epidemiology is the foundational prerequisite for the safe and effective management of cervical instability in Trisomy 21.
Detailed Surgical Anatomy and Biomechanics
The craniocervical junction (CCJ) is an anatomically intricate and biomechanically unique transition zone designed to provide maximum triplanar mobility while simultaneously protecting the cervicomedullary junction of the spinal cord. In the normal physiological state, stability at the atlantoaxial (C1-C2) and atlantooccipital (C0-C1) articulations relies heavily on a complex network of intrinsic ligaments, as the osseous articulations are inherently shallow and horizontally oriented. The primary stabilizer of the atlantoaxial joint is the transverse atlantal ligament (TAL), a robust, thick band of tissue that spans the inner margins of the lateral masses of C1, securely constraining the odontoid process against the anterior arch of the atlas. In patients with Down syndrome, the Type VI collagen defect severely diminishes the tensile yield strength of the TAL, allowing abnormal anterior translation of C1 on C2 during cervical flexion.
Secondary stabilization of the upper cervical spine is provided by the alar ligaments, the apical ligament, and the tectorial membrane. The alar ligaments originate from the posterolateral aspect of the odontoid process and attach to the medial aspect of the occipital condyles, functioning primarily to limit axial rotation and lateral bending. The tectorial membrane, the cephalad continuation of the posterior longitudinal ligament, provides critical resistance against excessive flexion and vertical distraction (cranial settling). In Trisomy 21, the generalized ligamentous laxity affects all these structures globally. When the transverse ligament undergoes plastic deformation due to repetitive stress, the secondary stabilizers (alar ligaments and tectorial membrane) are subjected to supra-physiologic loads. Over time, these secondary restraints also fail, converting an isolated atlantoaxial instability into a complex, multidirectional craniocervical instability.
Understanding the concept of the "Space Available for the Cord" (SAC), also known as the Posterior Atlantodens Interval (PADI), is paramount in this population. The anatomical relationship at the C1 level is governed by Steel’s Rule of Thirds: the ring of the atlas is divided equally into three zones occupied by the odontoid process, the spinal cord, and the "safe zone" (subarachnoid space and epidural fat). In a normal adult, the sagittal diameter of the spinal canal at C1 is approximately 30 mm. The odontoid occupies 10 mm, the cord occupies 10 mm, and the remaining 10 mm provides a buffer against dynamic compression. However, as the transverse ligament fails and the Atlantodens Interval (ADI) increases, this safe zone is rapidly obliterated. Once the SAC falls below 14 mm, the buffer is exhausted, and the spinal cord is subjected to direct mechanical compression against the posterior arch of C1, initiating the cascade of ischemic myelopathy.
The biomechanics of the atlantooccipital joint (C0-C1) are equally compromised in Down syndrome. The occipital condyles articulate with the superior articular facets of the atlas in a cup-shaped configuration that primarily permits flexion and extension. Atlantooccipital instability (AOI) in this population is characterized by abnormal anterior or posterior translation of the cranium relative to the cervical spine. This translation drastically alters the instantaneous axis of rotation, placing extreme shear forces on the lower medulla and upper cervical cord. Furthermore, the presence of osseous anomalies, such as odontoid hypoplasia, eliminates the bony buttress that normally prevents excessive translation, placing the entire biomechanical burden on the defective ligamentous complex. Surgical intervention must therefore aim not only to decompress the neural elements but to completely neutralize these abnormal translational and rotational forces through rigid, multi-point arthrodesis.
Exhaustive Indications and Contraindications
The management algorithm for cervical instability in Down syndrome must be meticulously individualized, requiring the orthopedic surgeon to balance the catastrophic risk of irreversible spinal cord injury against the notoriously high complication rates associated with cervical arthrodesis in this specific patient cohort. Decision-making is rarely straightforward and relies heavily on a combination of absolute radiographic measurements, dynamic imaging studies, detailed neurological examinations, and an assessment of the patient's functional baseline.
Surgical intervention (posterior cervical fusion) is strictly indicated under several absolute conditions. The most critical absolute indication is the presence of any objective neurological symptoms attributable to cervical myelopathy, regardless of the absolute ADI measurement. Symptoms such as hyperreflexia, sustained clonus, positive Babinski signs, broad-based spastic gait, or progressive loss of motor milestones mandate urgent surgical stabilization and decompression. A second absolute indication for operative management is an ADI of 10 mm or greater in an asymptomatic patient. At this degree of subluxation, the biomechanical failure of the transverse and alar ligaments is considered complete. The "safe zone" defined by Steel's Rule of Thirds is entirely compromised, and the risk of sudden, catastrophic neurological compromise from minor trauma is unacceptably high.
Relative indications require nuanced clinical judgment. A progressive increase in instability observed on serial dynamic radiographs, coupled with a declining Space Available for the Cord (SAC) approaching the critical threshold of 14 mm, is a strong relative indication for prophylactic fusion. Additionally, the presence of subclinical cord signal changes (myelomalacia) on T2-weighted MRI, even in the absence of overt clinical symptoms, strongly suggests that repetitive microtrauma is occurring, warranting surgical intervention. Some surgeons also advocate for prophylactic fusion in asymptomatic patients with an ADI between 7 mm and 9 mm if the patient exhibits extreme hypermobility, poor compliance with activity restrictions, or requires general anesthesia for other recurrent medical issues, which poses a risk for iatrogenic positioning injuries.
Contraindications to surgical intervention in this population must be carefully weighed. Active, untreated systemic infections or unoptimized severe medical comorbidities—most notably the congenital cardiac defects (e.g., atrioventricular septal defects) that affect nearly 50% of Down syndrome patients—serve as absolute contraindications until medical clearance is obtained. Relative contraindications include poor bone stock or severe osteopenia, which dramatically increases the risk of hardware pullout and graft subsidence. In such cases, surgical delay for metabolic bone optimization may be required. Furthermore, attempting a complex craniocervical fusion in an environment where postoperative immobilization (such as a halo-vest) cannot be tolerated due to severe behavioral or psychiatric comorbidities presents a profound clinical dilemma, often requiring extensive multidisciplinary planning prior to any operative commitment.
| Clinical Scenario | Indication Classification | Rationale / Surgical Directive |
|---|---|---|
| Presence of Myelopathic Signs (e.g., clonus, spastic gait, weakness) | Absolute Indication | Immediate surgical stabilization and decompression required. Neurological deficit indicates exhaustion of the SAC. |
| ADI ≥ 10 mm (Asymptomatic) | Absolute Indication | Complete biomechanical failure of the TAL and alar ligaments. High risk of sudden catastrophic cord injury. |
| SAC/PADI < 14 mm with MRI signal changes | Absolute Indication | Cord compression is actively occurring (myelomalacia). Decompression and fusion are mandatory. |
| ADI 6 - 9 mm with progressive widening on serial films | Relative Indication | Prophylactic fusion considered based on patient compliance, activity level, and rate of progression. |
| Unoptimized Congenital Heart Defect | Absolute Contraindication | High perioperative mortality risk. Cardiac optimization must precede elective orthopedic intervention. |
| Severe Behavioral Non-compliance | Relative Contraindication | High risk of postoperative hardware failure due to inability to tolerate halo-vest immobilization. |
Pre-Operative Planning, Templating, and Patient Positioning
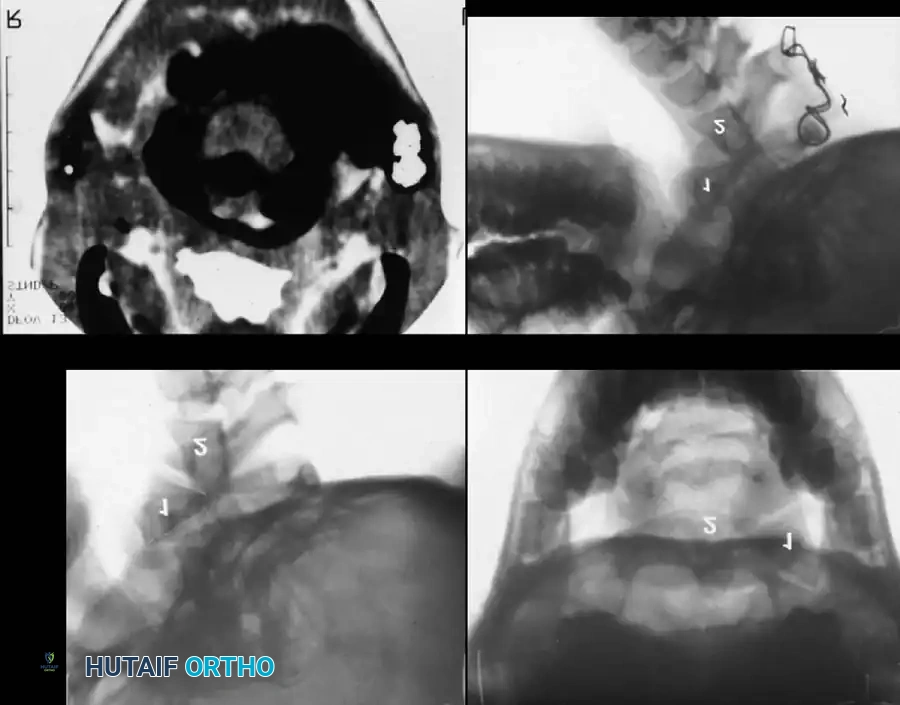
A rigorous, standardized, and exhaustive radiographic protocol is mandatory for all patients with Down syndrome suspected of having cervical instability. The standard radiographic series must include high-quality anteroposterior (AP), open-mouth odontoid, and dynamic (flexion-extension) lateral radiographs. These images form the foundation of the preoperative templating process. The primary metric for evaluating Atlantoaxial Instability (AAI) is the Atlantodens Interval (ADI), measured from the posterior margin of the anterior ring of C1 to the anterior cortex of the odontoid process. An ADI of greater than 4 to 5 mm indicates definitive ligamentous laxity. If the ADI exceeds 6 to 7 mm, dynamic MRI or CT in flexion and extension is strictly indicated to evaluate the Space Available for the Cord (SAC).
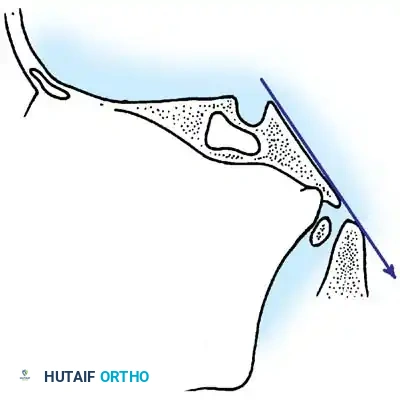
Evaluating Atlantooccipital Instability (AOI) requires a more sophisticated geometric analysis. The orthopedic surgeon must master several validated measurement techniques. The Wackenheim Clivus-Canal Line evaluates the relationship between the cranium and the cervical canal. A line drawn along the posterior aspect of the clivus should pass perfectly tangential to, or just posterior to, the tip of the odontoid process. Any intersection with the odontoid indicates cranial settling or abnormal translation.
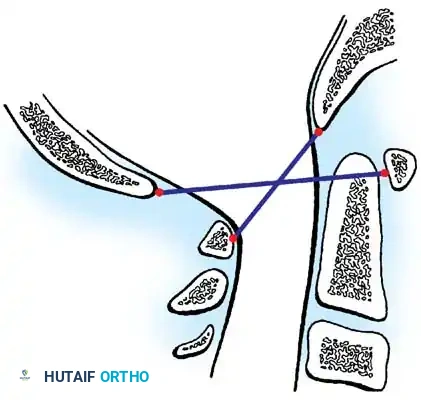
The Powers Ratio is another critical metric, calculated by dividing the distance from the Basion (B) to the posterior arch of the atlas (C) by the distance from the Opisthion (O) to the anterior arch of the atlas (A). A ratio greater than 1.0 is diagnostic of abnormal anterior translation of the occiput, while a ratio less than 0.55 indicates abnormal posterior translation.
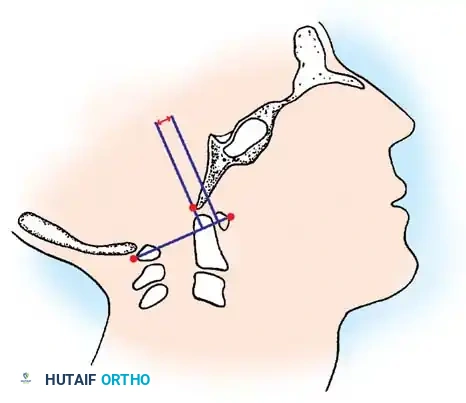
Furthermore, the Wiesel and Rothman Measurement quantifies dynamic occipitoatlantal translation by comparing the distance from the basion to a perpendicular line drawn from the anterior arch of C1 on both flexion and extension films. A translation difference of more than 1 mm is diagnostic of AOI. Advanced 3D CT reconstructions are essential for evaluating osseous anomalies, assessing bone stock, and determining the precise trajectory, length, and diameter of planned lateral mass or pedicle screws.
Preoperative patient positioning and anesthesia induction represent one of the most critical phases of the surgical intervention. Due to the severe instability, standard endotracheal intubation involving neck extension is strictly contraindicated. Fiberoptic awake intubation or video laryngoscopy with rigid manual in-line stabilization is mandatory. Once the airway is secured, the patient is carefully transitioned to the prone position. The head must be secured in a Mayfield skull clamp or a halo ring, maintaining the neck in a strictly neutral position. Neuro-monitoring, including Somatosensory Evoked Potentials (SSEPs) and Motor Evoked Potentials (MEPs), must be established prior to positioning and monitored continuously throughout the transfer and the entire surgical procedure. Any loss of SSEP or MEP signals during positioning requires immediate reversal of the maneuver and reassessment of spinal alignment.
Step-by-Step Surgical Approach and Fixation Technique
Performing a posterior cervical fusion in a patient with Down syndrome is fraught with unique anatomical and physiological challenges. The surgical approach begins with a standard posterior midline incision extending from the external occipital protuberance (inion) down to the spinous process of C3 or C4, depending on the planned fusion levels. Meticulous subperiosteal dissection is performed using electrocautery and Cobb elevators to expose the posterior arch of C1 and the lamina, pars interarticularis, and spinous process of C2. During the exposure of the C1 posterior arch, the surgeon must exercise extreme caution. Dissection along the superior margin of the C1 arch must not extend more than 1.5 cm lateral to the midline. Violating this boundary risks catastrophic iatrogenic injury to the vertebral artery as it courses medially through the sulcus arteriosus on the superior surface of the C1 ring.
Once the posterior elements are adequately exposed, the surgeon must address the reduction of the unstable joint. Preoperative or intraoperative cranial traction (using Gardner-Wells tongs) may be utilized to attempt a gentle, closed reduction of the atlantoaxial subluxation under continuous fluoroscopic guidance and neuromonitoring. However, a critical surgical pitfall must be avoided: the surgeon must never forcefully reduce a chronic, stiff atlantoaxial subluxation. If anatomical reduction cannot be obtained safely via traction, an in situ fusion is absolutely mandatory. Attempting an intraoperative structural reduction by forcibly pulling the C1 arch posteriorly toward C2 using instrumentation can cause catastrophic neurological compromise by drawing the anterior arch of C1 against the spinal cord through a critically narrowed SAC.
Modern instrumentation techniques have revolutionized the biomechanical stability of C1-C2 arthrodesis. The Harms and Goel technique, utilizing C1 lateral mass screws combined with C2 pedicle or pars screws, is the current gold standard. The entry point for the C1 lateral mass screw is identified at the junction of the posterior arch and the midpoint of the lateral mass. The C2 pedicle screw entry point is in the superior-medial quadrant of the C2 isthmus. These rigid screw-rod constructs provide superior biomechanical stability and significantly enhance fusion rates compared to historical techniques. However, in pediatric Down syndrome patients with diminutive osseous dimensions or anomalous vertebral artery anatomy, traditional sublaminar wiring techniques (such as the Gallie or Brooks-Jenkins constructs) remain highly relevant and necessary backup strategies.
When utilizing sublaminar wires, the ligamentum flavum is carefully opened, and contoured titanium or stainless steel cables are passed beneath the posterior arch of C1 and the lamina of C2. If an in situ fusion is required due to irreducibility, a structural tricortical iliac crest bone graft is meticulously fashioned to fit the existing deformity without attempting to pull the spine into alignment. Regardless of the instrumentation used, the biological aspect of the fusion is paramount. The posterior arches of C1 and C2, as well as the lateral facet joints, must be aggressively decorticated using a high-speed burr to expose bleeding cancellous bone. Copious amounts of autologous cancellous bone graft, ideally harvested from the posterior superior iliac spine (PSIS), are packed tightly over the decorticated surfaces to maximize the osteogenic potential in a patient population known for impaired bone healing.
Complications, Incidence Rates, and Salvage Management
The postoperative management of Down syndrome patients requires profound vigilance, as complication rates following cervical arthrodesis in this cohort are exponentially higher than in the general pediatric or adult spine populations. The unique physiological environment of Trisomy 21—characterized by intrinsic collagen defects, altered inflammatory responses, and impaired osteogenesis—creates a highly hostile environment for achieving solid bony fusion. The surgeon must be prepared to identify, mitigate, and manage a wide array of severe postoperative complications.
The most formidable complication is graft resorption and subsequent pseudarthrosis. Segal et al. reported an alarmingly high rate of graft resorption and non-union following posterior fusions in this population. The underlying Type VI collagen defects and an inadequate local inflammatory response severely impair the initial stages of osteogenesis. When pseudarthrosis occurs, the instrumentation is subjected to continuous cyclical loading, inevitably leading to hardware failure, screw pullout, or wire breakage. Salvage management of pseudarthrosis typically requires revision surgery, aggressive re-decortication, the application of robust biological adjuvants (such as Bone Morphogenetic Protein, rhBMP-2, used off-label with extreme caution), and an extension of the fusion construct to incorporate the occiput or subaxial spine to increase biomechanical rigidity.
Adjacent segment instability is another frequent and highly concerning complication. Msall et al. documented the frequent development of new-onset instability at the segments immediately adjacent to the fused C1-C2 segment—most commonly at the occipitoatlantal (C0-C1) articulation above, or the C2-C3 articulation below. This phenomenon occurs because the rigid fusion of the atlantoaxial joint transfers immense biomechanical stress to the adjacent hypermobile, ligamentously lax joints. Long-term, lifelong radiographic surveillance is mandatory even after a radiographically successful arthrodesis. If adjacent segment disease progresses to neurological compression, salvage management requires extending the fusion construct, often resulting in a complex occipitocervical fusion (C0-C3 or C4).
Furthermore, the altered immune profile in Down syndrome significantly increases the risk of surgical site infections (SSIs) and delayed wound healing. Meticulous soft tissue handling, dead-space management, and optimized postoperative nutritional support are critical preventative measures. Should a deep SSI occur, emergent surgical debridement, copious irrigation, and prolonged culture-directed intravenous antibiotic therapy are required. Hardware is generally retained unless it is loose or the infection cannot be eradicated.
| Complication | Estimated Incidence in Trisomy 21 | Etiology / Risk Factors | Salvage Management Strategy |
|---|---|---|---|
| Pseudarthrosis / Graft Resorption | 15% - 30% | Type VI collagen defect; impaired local osteogenesis; inadequate immobilization. | Revision arthrodesis; use of structural autograft; biological adjuvants (BMP); extension of fusion levels. |
| Adjacent Segment Instability | 20% - 40% (Long-term) | Stress transfer to adjacent lax ligaments (C0-C1 or C2-C3); intrinsic hypermobility. | Lifelong surveillance; extension of fusion construct (e.g., Occipitocervical fusion) if symptomatic. |
| Hardware Failure / Pullout | 10% - 20% | Poor bone mineral density; cyclical loading from pseudarthrosis; patient non-compliance. | Revision instrumentation; use of larger diameter/longer screws; conversion to rigid halo immobilization. |
| Surgical Site Infection (SSI) | 5% - 10% | Altered immune profile; poor wound healing; prolonged operative times. | Aggressive surgical debridement; retention of stable hardware; prolonged IV antibiotics. |
| Vertebral Artery Injury | < 2% | Aberrant vascular anatomy; lateral dissection > 1.5 cm from midline on C1 arch. | Intraoperative tamponade; primary repair (rare); endovascular embolization; postoperative angiography. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation and immobilization protocol for a patient with Down syndrome undergoing cervical fusion deviates significantly from standard spine surgery pathways. Due to the inherent collagen defects and altered inflammatory responses, the timeline for bone healing is notoriously delayed, and the risk of early hardware failure is exceptionally high. Consequently, standard rigid cervical collars (e.g., Aspen or Miami J collars) are universally considered insufficient for postoperative immobilization in this specific patient population.
The immediate postoperative phase (Weeks 0-2) focuses on strict immobilization and medical stabilization. Upon completion of the surgical procedure, the patient is typically placed directly into a rigid halo-vest or a custom-molded Minerva cast while still under anesthesia. The halo-vest provides the maximum possible restriction of triplanar cervical motion, neutralizing the shear and rotational forces that threaten the nascent bone graft. During this acute phase, the patient is monitored in the intensive care unit for signs of airway compromise, neurological deterioration, or pin-site complications. Pin torque must be checked regularly, and meticulous pin-site care protocols are initiated to prevent superficial infections that could track to the calvarium.
The intermediate phase (Weeks 2-12) involves transitioning the patient to a specialized rehabilitation environment. Physical therapy is initiated, but it is strictly limited to lower extremity mobilization, ambulation training, and isometric core strengthening. Absolutely no active or passive range of motion of the cervical spine is permitted. Radiographic surveillance is intense during this period, with AP and lateral radiographs taken at 2, 6, and 12 weeks to monitor hardware integrity and assess early graft incorporation. The surgeon must remain vigilant for any signs of halo-vest loosening or patient non-compliance, which may require cast modification or pin replacement.
The late phase (Months 3-6+) is dictated by radiographic evidence of osseous union. Unlike the general population, where a halo may be removed at 12 weeks, patients with Down syndrome typically require continuous halo-vest immobilization for a minimum of 4 to 6 months. Only when high-resolution CT imaging demonstrates definitive, continuous bridging trabecular bone across the decorticated surfaces and graft sites can the halo be safely removed. Following halo removal, the patient is transitioned to a rigid cervical collar for an additional 4 to 6 weeks to prevent sudden whiplash injuries as the atrophied cervical musculature slowly regains strength. Long-term rehabilitation focuses on gentle, progressive restoration of muscular endurance, though permanent restriction from high-impact activities, contact sports, and gymnastics remains a lifelong mandate.
Summary of Landmark Literature and Clinical Guidelines
The evolution of surgical management for cervical instability in Down syndrome is deeply rooted in several landmark epidemiological and clinical studies that have shaped modern orthopedic guidelines. The seminal work by Pueschel et al. (1990) fundamentally altered the understanding of the pathoanatomy in Trisomy 21. By evaluating a massive cohort of patients, Pueschel demonstrated not only the high prevalence of ligamentous atlantoaxial instability but, more importantly, the staggering 60% prevalence of concurrent osseous anomalies. This study established the absolute necessity of advanced preoperative imaging (CT and MRI) to delineate bony anatomy before any surgical intervention is contemplated, moving the field away from relying solely on plain radiographs.
Burke et al. provided critical insights into the natural history and clinical presentation of myelopathy in this population. Their research highlighted that while radiographic instability is common in early childhood, catastrophic neurological decline most frequently presents in males older than 10.5 years. This demographic data has been instrumental in guiding surveillance protocols, emphasizing the need for heightened clinical vigilance as male patients transition into adolescence. Furthermore, Burke's work underscored the insidious nature of the neurological decline, prompting the modern recommendation for the use of Somatosensory Evoked Potentials (SSEPs) to objectively document subclinical neurological involvement when physical examinations are confounded by intellectual disability.
The high complication rates associated with surgical intervention were comprehensively documented by Segal et al. and Msall et al. Segal’s alarming reports on graft resorption and pseudarthrosis directly led to the current mandate for prolonged halo-vest immobilization and the aggressive use of structural autograft. Msall’s documentation of adjacent segment instability highlighted the biomechanical consequences of fusing a hypermobile spine, establishing the requirement for lifelong radiographic surveillance post-fusion.
These landmark studies have heavily influenced the clinical guidelines established by organizations such as the American Academy of Pediatrics (AAP) and the Special Olympics. Current Special Olympics guidelines mandate radiographic screening (lateral flexion-extension views) for all athletes with Down syndrome prior to participation in high-risk sports. While routine radiographic screening of asymptomatic children remains a topic of debate within the AAP, the consensus is clear: any patient with Down syndrome exhibiting an ADI greater than 4.5 mm must be restricted from contact sports, and any patient with an ADI approaching 10 mm, or an SAC less than 14 mm, requires urgent orthopedic surgical evaluation. Mastery of this literature is essential for the orthopedic surgeon to navigate the complex, high-stakes management of craniocervical instability in Trisomy 21.
