Full Question & Answer Text (for Search Engines)
Question 1:
A 4-week-old female is placed in a Pavlik harness for developmental dysplasia of the hip. At her one-week follow-up, she is noted to have absent active knee extension on the affected side. Which of the following is the most appropriate next step in management?
Options:
- Adjust the harness to increase abduction
- Discontinue the harness temporarily or significantly decrease anterior strap tension
- Proceed to closed reduction and spica casting
- Increase anterior strap tension to secure reduction
- Transition immediately to a rigid hip abduction orthosis
Correct Answer: Discontinue the harness temporarily or significantly decrease anterior strap tension
Explanation:
Absent active knee extension indicates a femoral nerve palsy, a known complication of the Pavlik harness occurring in about 2% of cases. It is caused by excessive hyperflexion, which compresses the femoral nerve against the inguinal ligament. The most appropriate immediate management is to discontinue the harness temporarily or decrease the tension on the anterior flexion straps to allow the nerve to recover. Recovery typically occurs within a few days to a week.
Question 2:
A 12-year-old boy with a BMI of 32 presents with a left slipped capital femoral epiphysis (SCFE). Prophylactic pinning of the contralateral asymptomatic hip is most strongly indicated in which of the following scenarios?
Options:
- The patient is an African American male
- The patient presents with a chronic SCFE rather than an acute one
- The patient has underlying renal osteodystrophy
- The patient has a closed triradiate cartilage on the AP pelvis radiograph
- The patient has a positive family history of SCFE
Correct Answer: The patient has underlying renal osteodystrophy
Explanation:
Prophylactic pinning of the contralateral hip in SCFE is controversial for idiopathic cases but is strongly indicated in patients with underlying endocrinopathies or metabolic bone diseases (e.g., renal osteodystrophy, hypothyroidism, panhypopituitarism) and in patients receiving radiation therapy, because the risk of contralateral slip approaches 50-100% in these populations.
Question 3:
A 6-year-old child sustains an extension-type supracondylar humerus fracture with posterolateral displacement. Which of the following neurologic structures is at greatest risk of injury?
Options:
- Ulnar nerve
- Anterior interosseous nerve (AIN)
- Radial nerve
- Musculocutaneous nerve
- Axillary nerve
Correct Answer: Anterior interosseous nerve (AIN)
Explanation:
In an extension-type supracondylar humerus fracture with posterolateral displacement of the distal fragment, the proximal fragment is directed anteromedially. This anteromedial spike places the median nerve (specifically the anterior interosseous nerve branch) and the brachial artery at the greatest risk of injury. Conversely, posteromedial displacement of the distal fragment drives the proximal fragment anterolaterally, risking the radial nerve.
Question 4:
When applying the Ponseti method for the correction of a severe idiopathic clubfoot, which of the following represents the correct sequential order of deformity correction?
Options:
- Cavus, Adductus, Varus, Equinus
- Cavus, Varus, Adductus, Equinus
- Equinus, Cavus, Adductus, Varus
- Adductus, Varus, Cavus, Equinus
- Varus, Cavus, Adductus, Equinus
Correct Answer: Cavus, Adductus, Varus, Equinus
Explanation:
The Ponseti method corrects clubfoot deformities in a specific sequence summarized by the acronym CAVE: Cavus, Adductus, Varus, and Equinus. The cavus is corrected first by elevating the first ray. The adductus and varus are then corrected simultaneously by abducting the foot around the head of the talus. Equinus is corrected last, often requiring a percutaneous Achilles tenotomy.
Question 5:
A 7-year-old with spastic quadriplegic cerebral palsy has progressive hip subluxation with a Reimer's migration index of 45%. The primary deforming forces responsible for this progressive subluxation are spasticity of which muscle groups?
Options:
- Abductors and extensors
- Adductors and flexors
- Adductors and internal rotators
- Abductors and external rotators
- Hamstrings and quadriceps
Correct Answer: Adductors and flexors
Explanation:
In cerebral palsy, progressive hip subluxation and dislocation are driven by the muscle imbalance caused by spasticity. The spastic adductors and hip flexors (iliopsoas) overpower the relatively weaker abductors and extensors, driving the femoral head posteromedially and causing a progressive valgus and anteverted proximal femur, which leads to superolateral uncovering and eventual dislocation.
Question 6:
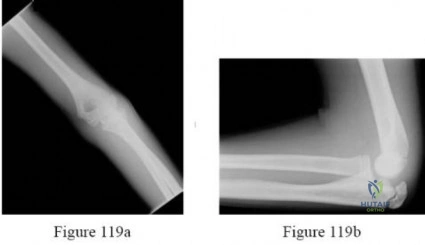
A 4-year-old boy undergoes open reduction and internal fixation of a displaced Milch Type II lateral condyle fracture of the humerus. Which of the following is the most common complication associated with this injury and its treatment?
Options:
- Avascular necrosis of the trochlea
- Cubitus varus
- Nonunion
- Lateral spur formation (lateral condylar overgrowth)
- Ulnar nerve palsy
Correct Answer: Lateral spur formation (lateral condylar overgrowth)
Explanation:
Lateral spur formation, or lateral condylar overgrowth, is the most common complication of a lateral condyle fracture, occurring in up to 50-70% of cases. It causes a cosmetic bump on the lateral elbow but rarely restricts motion or causes functional deficits. While nonunion and tardy ulnar nerve palsy (due to cubitus valgus) are classic severe complications of a missed or poorly treated lateral condyle fracture, lateral overgrowth is far more frequent.
Question 7:
A 3-year-old girl with a BMI in the 98th percentile presents with bilateral severe bowing of the lower extremities. Radiographs reveal an abrupt varus angulation at the proximal tibial metaphysis with medial beaking. The metaphyseal-diaphyseal (Drennan) angle is 20 degrees. What is the most appropriate initial management?
Options:
- Reassurance and annual observation
- Bilateral knee-ankle-foot orthoses (KAFOs)
- Proximal tibial valgus osteotomies
- Eight-plate guided growth (hemiepiphysiodesis) of the lateral proximal tibia
- Epiphysiodesis of the medial proximal tibia
Correct Answer: Bilateral knee-ankle-foot orthoses (KAFOs)
Explanation:
The patient has infantile Blount's disease (tibia vara), characterized by medial metaphyseal beaking and a Drennan angle >16 degrees (which distinguishes it from physiologic bowing). For children under the age of 4 with Langenskiöld Stage I or II, bracing with KAFOs during weight-bearing hours is the standard initial treatment. Surgery (osteotomy) is indicated if bracing fails, or if the child is over age 4 at presentation.
Question 8:
In Legg-Calvé-Perthes disease, which of the following clinical factors is considered the most significant prognostic factor for long-term hip joint survival and prevention of early osteoarthritis?
Options:
- Age at clinical presentation
- Gender of the patient
- Presence of a Gage sign on radiographs
- Degree of metaphyseal cyst formation
- Amount of initial limb length discrepancy
Correct Answer: Age at clinical presentation
Explanation:
Age at clinical presentation is universally recognized as the most critical prognostic factor in Legg-Calvé-Perthes disease. Children who present at less than 6 to 8 years of age have a significant remodeling potential and generally fare better. Those over age 8 at presentation have a much higher rate of poor outcomes and early secondary osteoarthritis. The Lateral Pillar classification is the most significant radiographic prognostic factor.
Question 9:
A 13-year-old girl sustains an ankle injury while playing soccer. Radiographs demonstrate a Salter-Harris III fracture of the anterolateral distal tibia. Which of the following describes the mechanism of injury and the anatomic structure responsible for avulsing this fragment?
Options:
- Supination-inversion; Calcaneofibular ligament
- Pronation-eversion; Deltoid ligament
- External rotation; Anterior inferior tibiofibular ligament (AITFL)
- Internal rotation; Posterior inferior tibiofibular ligament (PITFL)
- Plantarflexion; Anterior talofibular ligament (ATFL)
Correct Answer: External rotation; Anterior inferior tibiofibular ligament (AITFL)
Explanation:
This is a juvenile Tillaux fracture, which is a Salter-Harris III fracture of the anterolateral distal tibial epiphysis. It occurs in adolescents due to the asymmetric closure of the distal tibial physis (central, then medial, then lateral). An external rotation force placed on the foot causes the strong Anterior Inferior Tibiofibular Ligament (AITFL) to avulse the unfused anterolateral epiphysis.
Question 10:
A 4-year-old boy with achondroplasia presents with clumsiness, increased sleeping, and hyperreflexia in the lower extremities. Which of the following is the most likely etiology of his new neurologic findings?
Options:
- Thoracolumbar kyphosis
- Atlantoaxial instability
- Foramen magnum stenosis
- Lumbar spinal stenosis
- Tethered cord syndrome
Correct Answer: Foramen magnum stenosis
Explanation:
Foramen magnum stenosis is a critical and potentially life-threatening complication of achondroplasia. Narrowing at the craniocervical junction can lead to cervicomedullary compression. Symptoms include hyperreflexia, clumsiness, sleep apnea, central respiratory depression, and in severe cases, sudden death. It typically presents in infants or young children and requires prompt neurosurgical decompression.
Question 11:
A 12-year-old premenarchal female (Risser 0) presents with a right thoracic adolescent idiopathic scoliosis. Her curve measures 22 degrees on a standing PA radiograph. What is the approximate risk of curve progression to greater than 30 degrees?
Options:
Correct Answer: 68%
Explanation:
According to the Lonstein and Carlson progression formula and established general guidelines for Adolescent Idiopathic Scoliosis, a patient who is highly immature (Risser 0-2, premenarchal) with a curve measuring between 20-29 degrees has approximately a 68% risk of curve progression. This warrants close observation or initiation of bracing.
Question 12:
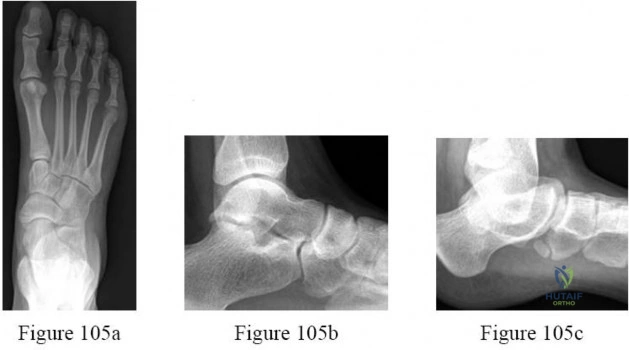
A 14-year-old male presents with recurrent ankle sprains and rigid flatfeet. On examination, he has restricted subtalar motion and pain reproduced with forced inversion. Radiographs show a "C sign" on the lateral view. Which of the following is the most appropriate initial management for this condition?
Options:
- Custom foot orthotics with medial arch support
- Serial casting or a controlled ankle motion (CAM) boot for 4 to 6 weeks
- Subtalar arthrodesis
- Excision of the coalition with fat pad interposition
- Calcaneal lengthening osteotomy
Correct Answer: Serial casting or a controlled ankle motion (CAM) boot for 4 to 6 weeks
Explanation:
The clinical presentation and "C sign" on a lateral radiograph are pathognomonic for a talocalcaneal coalition. Initial management of a symptomatic tarsal coalition is conservative and aims to break the pain-spasm cycle. This is best achieved with a period of immobilization using a short leg cast or CAM boot for 4 to 6 weeks. Operative intervention (resection or arthrodesis) is reserved for cases that fail conservative management.
Question 13:
A 5-year-old child with a history of multiple fractures, blue sclerae, and dentinogenesis imperfecta is diagnosed with Osteogenesis Imperfecta Type I. This condition is most commonly caused by a mutation in which of the following genes?
Options:
- FGFR3
- COMP
- COL1A1
- COL2A1
- RUNX2
Correct Answer: COL1A1
Explanation:
Osteogenesis Imperfecta (OI) is a genetic disorder of connective tissue primarily affecting Type I collagen. It is most commonly inherited in an autosomal dominant pattern and is caused by mutations in the COL1A1 or COL1A2 genes. FGFR3 is associated with achondroplasia; COMP with pseudoachondroplasia and multiple epiphyseal dysplasia; COL2A1 with spondyloepiphyseal dysplasia (SED); and RUNX2 with cleidocranial dysplasia.
Question 14:
A 2-year-old boy sustains a closed, isolated midshaft femur fracture. The decision is made to treat him with early spica casting. To appropriately control the proximal fragment and align the fracture, in what position should the hip be casted?
Options:
- Extension and adduction
- Flexion and adduction
- Flexion, abduction, and external rotation
- Extension, abduction, and internal rotation
- Neutral flexion/extension and internal rotation
Correct Answer: Flexion, abduction, and external rotation
Explanation:
In a proximal or midshaft pediatric femur fracture, the proximal fragment assumes a predictable position due to muscle pull: flexion (iliopsoas), abduction (gluteus medius and minimus), and external rotation (short external rotators). To achieve alignment, the distal fragment (controlled by the spica cast) must be matched to the position of the proximal fragment. Thus, the cast is applied with the hip flexed, abducted, and externally rotated.
Question 15:
A 13-year-old boy presents to the emergency department unable to bear weight on his right leg after a minor fall 2 days ago. He has a history of vague right groin pain for 3 months. Radiographs demonstrate a severe, unstable slipped capital femoral epiphysis (SCFE). Which of the following best describes the rationale for performing a capsulotomy during surgical fixation?
Options:
- To assist with anatomic closed reduction
- To reduce intracapsular pressure and minimize the risk of avascular necrosis
- To prevent chondrolysis
- To facilitate removal of loose bodies
- To allow for placement of a second stabilizing screw
Correct Answer: To reduce intracapsular pressure and minimize the risk of avascular necrosis
Explanation:
Unstable SCFE (defined by the inability to bear weight) carries a high risk of avascular necrosis (AVN), reportedly up to 50%. The primary rationale for performing an anterior capsulotomy during surgical treatment of an unstable SCFE is to evacuate the fracture hematoma, thereby decompressing the joint and reducing intracapsular pressure, which theoretically improves perfusion to the femoral head and decreases the risk of AVN.
Question 16:
A 15-year-old gymnast complains of chronic low back pain exacerbated by extension. Oblique radiographs demonstrate a "Scotty dog with a collar" appearance at L5. A bilateral pars interarticularis defect is confirmed. If conservative management fails, which of the following is the most appropriate surgical intervention for an isolated L5 pars defect without spondylolisthesis in this young athlete?
Options:
- L5-S1 posterior spinal fusion with pedicle screws
- L4-L5 posterior spinal fusion
- Direct repair of the pars defect (e.g., Buck or Scott wiring technique)
- L5 laminectomy
- Anterior lumbar interbody fusion (ALIF) at L5-S1
Correct Answer: Direct repair of the pars defect (e.g., Buck or Scott wiring technique)
Explanation:
The patient has symptomatic spondylolysis (pars interarticularis defect) without spondylolisthesis. In a young, high-level athlete (like a gymnast) who fails extensive conservative management, direct pars repair (using techniques such as Buck's screws, Scott wiring, or Morscher hooks) is indicated. This approach restores the bony continuity of the pars while preserving the motion segment, avoiding the loss of mobility inherent to a spinal fusion.
Question 17:
A 4-year-old boy presents with right hip pain, a limp, and refusal to bear weight. His temperature is 38.6°C (101.5°F), WBC count is 13.5 x 10^9/L, and ESR is 45 mm/hr. Based on the modified Kocher criteria, what is the approximate probability that this child has septic arthritis rather than transient synovitis?
Options:
Correct Answer: 99%
Explanation:
The Kocher criteria for differentiating septic arthritis from transient synovitis include: 1) Non-weight bearing on the affected side, 2) ESR > 40 mm/hr, 3) Fever > 38.5°C (101.3°F), and 4) WBC count > 12.0 x 10^9/L. This patient meets all 4 criteria. The probability of septic arthritis is approximately 3% for 1 criterion, 40% for 2, 93% for 3, and 99% for 4 criteria.
Question 18:
A 2-year-old boy presents with anterolateral bowing of the left tibia and a newly developed midshaft fracture. Radiographs reveal a narrowed, sclerotic medullary canal with a pseudarthrosis. This clinical presentation is most strongly associated with which of the following systemic conditions?
Options:
- Osteogenesis Imperfecta
- Neurofibromatosis type 1 (NF1)
- Achondroplasia
- Marfan syndrome
- Ehlers-Danlos syndrome
Correct Answer: Neurofibromatosis type 1 (NF1)
Explanation:
Congenital pseudarthrosis of the tibia (CPT) classically presents with anterolateral bowing of the tibia that fractures and fails to heal due to abnormal periosteum. It is strongly associated with Neurofibromatosis type 1 (NF1); approximately 50% of children with CPT have NF1. Conversely, posteromedial bowing is generally benign and resolves spontaneously.
Question 19:
An 8-year-old girl presents with a painless snapping and popping sensation in her lateral right knee, particularly during extension. MRI confirms a complete (Watanabe Type I) discoid lateral meniscus with no evidence of tearing or instability. What is the most appropriate management?
Options:
- Observation and reassurance
- Arthroscopic saucerization
- Arthroscopic total meniscectomy
- Open meniscus repair
- Physical therapy for quadriceps strengthening
Correct Answer: Observation and reassurance
Explanation:
A discoid meniscus is an abnormally shaped, thickened meniscus (most commonly lateral) that can cause a snapping knee. However, if the discoid meniscus is asymptomatic or causes only painless snapping without a tear or significant instability (e.g., Wrisberg variant), the standard of care is observation and reassurance. Surgical intervention (saucerization) is indicated only if there are mechanical symptoms like pain, locking, or documented tears.
Question 20:
A 9-month-old infant is incidentally noted to have a left-sided thoracic scoliosis measuring 25 degrees. To differentiate between a resolving and a progressive infantile idiopathic scoliosis, the rib-vertebra angle difference (RVAD) of Mehta is measured at the apical vertebra. An RVAD greater than what value is highly predictive of curve progression?
Options:
- 5 degrees
- 10 degrees
- 20 degrees
- 30 degrees
- 45 degrees
Correct Answer: 20 degrees
Explanation:
In infantile idiopathic scoliosis, Mehta's Rib-Vertebra Angle Difference (RVAD) is critical for predicting whether a curve will resolve or progress. An RVAD > 20 degrees at the apical vertebra implies a high likelihood of progression (Phase II rib head overlap often accompanies this), warranting aggressive non-operative treatment such as serial elongation-derotation-flexion (EDF) casting.
Question 21:
A 2-year-old boy presents with anterolateral bowing of the tibia. Radiographs show a narrowing of the medullary canal at the apex of the deformity. A diagnosis of congenital pseudarthrosis of the tibia (CPT) is suspected. Which of the following interventions during surgical reconstruction is most critical for achieving long-term union?
Options:
- Application of a circular external fixator alone for gradual correction
- Complete resection of the pseudarthrosis site including the surrounding hamartomatous periosteum, followed by intramedullary fixation
- In situ bone grafting utilizing recombinant human bone morphogenetic protein-2 (rhBMP-2)
- Prophylactic complete fibulectomy to prevent varus drift
- Immediate Syme amputation as primary treatment
Correct Answer: Complete resection of the pseudarthrosis site including the surrounding hamartomatous periosteum, followed by intramedullary fixation
Explanation:
Congenital pseudarthrosis of the tibia (CPT) is strongly associated with Neurofibromatosis Type 1 (NF-1). The underlying pathology is concentrated in the thickened, hamartomatous periosteum which acts as a barrier to osteogenesis. To achieve union, it is critical to completely excise the pseudarthrosis site and the abnormal periosteum. This is typically combined with robust intramedullary fixation (often a cross-ankle telescoping rod) and bone grafting (often utilizing BMP-2 and autograft/allograft) to provide the mechanical stability and biological environment needed for healing.
Question 22:
An 11-year-old girl with a body mass index (BMI) in the 99th percentile is diagnosed with a unilateral slipped capital femoral epiphysis (SCFE). Which of the following is considered an absolute indication for prophylactic in situ pinning of the contralateral, asymptomatic hip?
Options:
- A modified Southwick angle greater than 50 degrees on the symptomatic side
- Patient age younger than 12 years at the time of presentation
- The presence of an underlying endocrine or metabolic disorder (e.g., hypothyroidism)
- A patient BMI exceeding the 95th percentile
- Female sex
Correct Answer: The presence of an underlying endocrine or metabolic disorder (e.g., hypothyroidism)
Explanation:
While factors such as young age, obesity, and open triradiate cartilage are relative indications that surgeons consider when discussing prophylactic pinning, the presence of an underlying endocrine or metabolic disorder (such as hypothyroidism, panhypopituitarism, or renal osteodystrophy) is universally considered an absolute indication for prophylactic pinning of the contralateral hip due to the extremely high risk of a subsequent slip.
Question 23:
A 3-and-a-half-year-old child presents with worsening bilateral genu varum. Radiographs demonstrate a prominent metaphyseal beak and depression of the medial proximal tibial physis consistent with Langenskiöld Stage III infantile Blount disease. What is the most appropriate management for this patient?
Options:
- Observation with serial clinical examinations every 6 months
- Full-time use of a Knee-Ankle-Foot Orthosis (KAFO)
- Proximal tibial valgus osteotomy and concomitant fibular osteotomy
- Guided growth via lateral hemi-epiphysiodesis
- Asymmetric guided growth utilizing tension band plates medially
Correct Answer: Proximal tibial valgus osteotomy and concomitant fibular osteotomy
Explanation:
Infantile Blount disease management is dependent on age and Langenskiöld stage. Bracing (KAFO) is generally indicated for children under 3 years old with Stage I or II disease. For a child over the age of 3 presenting with Stage III disease or higher, conservative management is unlikely to succeed. The standard of care is surgical realignment, typically through a proximal tibial valgus osteotomy combined with a fibular osteotomy to prevent recurrence and correct the mechanical axis.
Question 24:
A 6-year-old boy falls from the monkey bars and sustains a Gartland Type III supracondylar humerus fracture. Upon initial evaluation, his hand is pale and pulseless. After prompt closed reduction and percutaneous pinning in the operating room, the hand becomes warm and pink, with a capillary refill of less than 2 seconds, but the radial pulse remains unpalpable. What is the next best step in management?
Options:
- Immediate open vascular exploration of the brachial artery
- Removal of the pins, extension of the elbow to 30 degrees, and re-evaluation
- Admit the patient for close inpatient observation and neurovascular monitoring
- Administration of intra-arterial vasodilators (e.g., papaverine)
- Perform an immediate forearm fasciotomy
Correct Answer: Admit the patient for close inpatient observation and neurovascular monitoring
Explanation:
The management of the 'pink, pulseless hand' following reduction of a supracondylar humerus fracture is a well-established algorithm. If the hand is well-perfused (pink, warm, good capillary refill) after adequate reduction and stabilization, collateral circulation is sufficient. The standard of care is to admit the patient for close neurovascular monitoring (observation) rather than pursuing immediate vascular exploration, as the brachial artery is often in spasm and recanalizes over time.
Question 25:
A 3-month-old infant is undergoing treatment for Developmental Dysplasia of the Hip (DDH) using a Pavlik harness. During a follow-up visit, the mother notes that the infant has stopped kicking the affected leg. On examination, the infant exhibits absent knee extension but normal ankle dorsiflexion and plantarflexion. Which nerve injury is most likely, and what specific mechanical factor in the harness caused it?
Options:
- Femoral nerve palsy; caused by excessive hip flexion
- Obturator nerve palsy; caused by excessive hip abduction
- Sciatic nerve palsy; caused by excessive hip extension
- Femoral nerve palsy; caused by excessive hip abduction
- Sciatic nerve palsy; caused by excessive knee flexion
Correct Answer: Femoral nerve palsy; caused by excessive hip flexion
Explanation:
Femoral nerve palsy is the most common nerve injury associated with the use of a Pavlik harness for DDH. It is caused by excessive hip flexion, which tethers the femoral nerve against the inguinal ligament. The clinical presentation is an infant who stops kicking and loses active knee extension. Treatment consists of temporarily loosening or discontinuing the flexion straps or the harness entirely until function returns.
Question 26:
An 8-year-old boy presents with a painful limp and limited hip abduction. Radiographs reveal fragmentation of the proximal femoral epiphysis with maintained height of the lateral pillar (>50% of original height), classifying it as Herring Lateral Pillar Group B Legg-Calve-Perthes Disease (LCPD). According to the multicenter prospective study by Herring et al., which intervention provides the best radiographic outcome for this specific patient profile?
Options:
- Non-weight-bearing strictly enforced with crutches
- Scottish Rite abduction bracing
- Surgical containment via a proximal femoral varus osteotomy or pelvic osteotomy
- Core decompression of the femoral head
- Total hip arthroplasty
Correct Answer: Surgical containment via a proximal femoral varus osteotomy or pelvic osteotomy
Explanation:
According to the landmark multicenter prospective LCPD study by Herring et al., surgical containment (proximal femoral varus osteotomy or pelvic osteotomy) provides significantly better radiographic outcomes (Stulberg classification) compared to nonoperative treatment for children who are 8 years of age or older at the time of onset and who have Lateral Pillar Group B or B/C border disease.
Question 27:
A 5-year-old girl with recurrent long bone fractures and blue sclerae is diagnosed with Osteogenesis Imperfecta (OI) type I. She is started on intravenous pamidronate therapy. What is the primary mechanism of action of this pharmacological treatment?
Options:
- It stimulates osteoblast-mediated bone formation
- It inhibits osteoclast-mediated bone resorption by inducing osteoclast apoptosis
- It increases gastrointestinal absorption of calcium and phosphate
- It promotes the cross-linking of type I collagen fibers
- It directly downregulates the Wnt/beta-catenin signaling pathway
Correct Answer: It inhibits osteoclast-mediated bone resorption by inducing osteoclast apoptosis
Explanation:
Pamidronate is a nitrogen-containing bisphosphonate. Bisphosphonates primarily act by inhibiting osteoclast-mediated bone resorption. They are internalized by osteoclasts and inhibit the enzyme farnesyl pyrophosphate synthase in the mevalonate pathway, which ultimately disrupts cell function and induces osteoclast apoptosis, leading to increased bone mineral density.
Question 28:
A 6-year-old boy with spastic quadriplegic cerebral palsy (GMFCS level V) presents for routine hip surveillance. Anteroposterior pelvic radiograph reveals a Reimers migration percentage (migration index) of 45% in the right hip and 30% in the left hip. The patient experiences pain during diapering. What is the most appropriate surgical management for the right hip?
Options:
- Adductor longus tenotomy alone
- Proximal femoral varus derotation osteotomy (VDRO) with a pelvic osteotomy
- Intrathecal baclofen pump insertion
- Total hip arthroplasty
- Observation with repeat radiograph in 6 months
Correct Answer: Proximal femoral varus derotation osteotomy (VDRO) with a pelvic osteotomy
Explanation:
In children with cerebral palsy, a Reimers migration percentage greater than 40-50% indicates significant subluxation with a high risk of progression to dislocation. Adductor tenotomy alone is generally reserved for lower migration indices (<30%) in younger patients. For a migration index of 45% in a 6-year-old, bony reconstruction utilizing a proximal femoral varus derotation osteotomy (VDRO) combined with a pelvic osteotomy (such as a Dega or Pemberton) is the gold standard to provide definitive coverage and containment.
Question 29:
A 4-year-old boy presents with progressive bowing of his lower extremities and short stature. Laboratory evaluation reveals hypophosphatemia, normal serum calcium, normal parathyroid hormone (PTH), and elevated alkaline phosphatase. What is the underlying genetic defect in the most likely diagnosis?
Options:
- A mutation in the PHEX gene leading to elevated levels of FGF23
- A mutation in the FGFR3 gene resulting in an overactive receptor
- A mutation in the COL1A1 gene leading to abnormal type I collagen
- A mutation in the gene encoding the Vitamin D receptor (VDR)
- A mutation in the 1-alpha-hydroxylase gene
Correct Answer: A mutation in the PHEX gene leading to elevated levels of FGF23
Explanation:
The clinical presentation and lab profile (low phosphate, normal calcium, normal PTH) are classic for X-linked hypophosphatemic (XLH) rickets. This condition is caused by a mutation in the PHEX gene (phosphate-regulating endopeptidase homolog, X-linked). This mutation leads to an overproduction or decreased degradation of fibroblast growth factor 23 (FGF23), a phosphatonin that causes renal phosphate wasting and inhibits the conversion of 25-OH vitamin D to active 1,25-(OH)2 vitamin D.
Question 30:
An orthopaedic surgeon is treating a newborn with an idiopathic clubfoot using the Ponseti method of serial casting. Which of the following describes the correct sequential order of deformity correction using this technique?
Options:
- Equinus, Varus, Adductus, Cavus
- Cavus, Adductus, Varus, Equinus
- Cavus, Varus, Adductus, Equinus
- Adductus, Varus, Cavus, Equinus
- Varus, Adductus, Cavus, Equinus
Correct Answer: Cavus, Adductus, Varus, Equinus
Explanation:
The Ponseti method dictates a very specific sequential correction of the clubfoot deformities, remembered by the acronym CAVE: 1) Cavus (corrected by supinating the forefoot to align it with the hindfoot), 2) Adductus, 3) Varus (corrected simultaneously by abducting the foot around the talar head), and finally 4) Equinus (often requiring a percutaneous Achilles tenotomy once the heel is in valgus or neutral).
Question 31:
A newborn is evaluated for a congenital limb deficiency. Clinical examination and radiographs demonstrate an absent lateral malleolus, a shortened tibia, absent lateral rays of the foot, and marked anteromedial bowing of the tibia. Which of the following internal knee derangements is nearly universally associated with this condition?
Options:
- Anterior cruciate ligament (ACL) deficiency
- Posterior cruciate ligament (PCL) deficiency
- Discoid lateral meniscus
- Medial patellofemoral ligament (MPFL) dysplasia
- Bipartite patella
Correct Answer: Anterior cruciate ligament (ACL) deficiency
Explanation:
The clinical picture describes fibular hemimelia (longitudinal deficiency of the fibula). It is well established that fibular hemimelia is a spectrum that affects the entire limb. A nearly universal association with fibular hemimelia is the absence or severe deficiency of the anterior cruciate ligament (ACL). Other common associations include a ball-and-socket ankle joint, tarsal coalitions, and absence of the lateral rays of the foot.
Question 32:
A 13-year-old boy presents with recurrent ankle sprains and a rigid, painful flat foot. Passive inversion and eversion of the subtalar joint are significantly restricted and painful. You suspect a tarsal coalition. Which radiographic sign is classically associated with a calcaneonavicular coalition on an oblique radiograph of the foot?
Options:
- The 'C' sign
- The anteater nose sign
- The fleck sign
- The double density sign
- The crescent sign
Correct Answer: The anteater nose sign
Explanation:
The 'anteater nose sign' is classically seen on a 45-degree internal oblique radiograph of the foot in patients with a calcaneonavicular coalition. It represents a tubular elongation of the anterior process of the calcaneus projecting toward the navicular. The 'C' sign, seen on a lateral radiograph, is associated with a talocalcaneal (middle facet) coalition.
Question 33:
A 10-year-old girl sustains a knee injury while skiing. Radiographs reveal a completely displaced (Meyers and McKeever Type III) avulsion fracture of the tibial eminence. During a closed reduction attempt, the fragment fails to reduce into its anatomical bed. Which anatomical structure is most commonly responsible for blocking the reduction?
Options:
- Anterior horn of the medial meniscus
- Transverse intermeniscal ligament
- Anterior horn of the lateral meniscus
- Ligament of Wrisberg
- Infrapatellar fat pad
Correct Answer: Anterior horn of the medial meniscus
Explanation:
In Meyers and McKeever Type II and III tibial eminence (tibial spine) avulsion fractures, the most common structure to interpose and block an anatomic reduction is the anterior horn of the medial meniscus, and occasionally the intermeniscal ligament. Because of this entrapment, anatomic reduction often requires arthroscopic or open intervention to extricate the meniscus and anatomically secure the bony fragment.
Question 34:
A 14-year-old boy presents with ankle pain after twisting his leg while playing soccer. Radiographs demonstrate an isolated Salter-Harris Type III fracture of the anterolateral aspect of the distal tibial epiphysis. What is the mechanism of injury, and which ligament provides the deforming force causing this specific fracture pattern?
Options:
- Supination-inversion mechanism; pulled by the anterior talofibular ligament (ATFL)
- External rotation mechanism; pulled by the anterior inferior tibiofibular ligament (AITFL)
- Plantarflexion mechanism; pulled by the Achilles tendon
- Pronation-abduction mechanism; pulled by the deltoid ligament
- Axial loading mechanism; pulled by the posterior inferior tibiofibular ligament (PITFL)
Correct Answer: External rotation mechanism; pulled by the anterior inferior tibiofibular ligament (AITFL)
Explanation:
The fracture described is a juvenile Tillaux fracture. It occurs in adolescents (typically ages 12-15) because the distal tibial physis closes in a specific pattern: central, then medial, and finally lateral. An external rotation force on the foot creates tension in the anterior inferior tibiofibular ligament (AITFL), which avulses the still-open anterolateral portion of the distal tibial epiphysis (a Salter-Harris III fracture).
Question 35:
A 15-year-old competitive gymnast presents with worsening lower back pain that is exacerbated by leaning backward. Radiographs and subsequent MRI confirm a bilateral pars interarticularis defect at L5 without spondylolisthesis. This injury (spondylolysis) is primarily the result of repetitive mechanical stress applied during which combination of spinal motions?
Options:
- Hyperflexion and lateral bending
- Hyperextension and rotation
- Axial loading and forward flexion
- Distraction and pure axial rotation
- Shear force during forward trunk flexion
Correct Answer: Hyperextension and rotation
Explanation:
Spondylolysis (a defect in the pars interarticularis) is a stress fracture most commonly occurring at L5. It is highly prevalent in adolescent athletes who perform repetitive spinal hyperextension and rotation (e.g., gymnasts, fast bowlers in cricket, offensive linemen in football). These motions place massive cyclic shear and compressive forces on the pars, ultimately leading to fatigue failure.
Question 36:
A 2-year-old child is diagnosed with congenital scoliosis. Radiographic evaluation of the spine reveals a unilateral unsegmented bar with a fully segmented hemivertebra at the same level on the contralateral side. What is the expected natural history of this specific spinal anomaly if left untreated?
Options:
- Spontaneous resolution by skeletal maturity
- Slow, benign progression averaging 1-2 degrees per year
- Rapid and relentless progression often exceeding 5-10 degrees per year
- Progression strictly limited to the adolescent growth spurt
- Development of compensatory curves without progression of the primary deformity
Correct Answer: Rapid and relentless progression often exceeding 5-10 degrees per year
Explanation:
The combination of a unilateral unsegmented bar with a contralateral fully segmented hemivertebra at the same level is widely recognized as the most severe and rapidly progressive form of congenital scoliosis. Due to the complete tethering of growth on one side (the bar) and excessive growth potential on the convex side (the hemivertebra), this deformity progresses relentlessly (often >5 degrees per year) and requires early surgical intervention (e.g., hemivertebra excision or in situ fusion).
Question 37:
A 4-year-old boy presents to the emergency department refusing to bear weight on his right leg. His temperature is 38.8°C (101.8°F). You are attempting to differentiate between transient synovitis and septic arthritis of the hip using the Kocher criteria. Which of the following laboratory or clinical findings was NOT one of the four original criteria published by Kocher et al. in 1999?
Options:
- Inability to bear weight on the affected side
- Erythrocyte sedimentation rate (ESR) > 40 mm/hr
- Serum white blood cell (WBC) count > 12,000 cells/mm³
- C-reactive protein (CRP) > 2.0 mg/dL
- Temperature > 38.5°C (101.3°F)
Correct Answer: C-reactive protein (CRP) > 2.0 mg/dL
Explanation:
The original four predictive criteria published by Kocher et al. (1999) for septic arthritis of the pediatric hip are: 1) Non-weight-bearing on affected side, 2) ESR > 40 mm/hr, 3) Fever > 38.5°C, and 4) Serum WBC count > 12,000 cells/mm³. C-reactive protein (CRP) > 2.0 mg/dL was later identified as an independent predictor and added by Caird et al. (2006), making it a five-part clinical prediction rule, but it was not one of the original four Kocher criteria.
Question 38:
An 8-year-old boy with a known diagnosis of Duchenne Muscular Dystrophy (DMD) presents with progressively rigid equinovarus foot deformities that are severely impacting his ambulation. Surgical lengthening of the Achilles tendon and tendon transfers are planned. During the anesthetic planning for this procedure, which of the following agents must be strictly avoided due to a severe, potentially fatal complication?
Options:
- Propofol
- Ketamine
- Succinylcholine
- Nitrous oxide
- Fentanyl
Correct Answer: Succinylcholine
Explanation:
Patients with Duchenne Muscular Dystrophy (DMD) lack dystrophin, which compromises the integrity of the muscle cell membrane. The use of depolarizing neuromuscular blocking agents, such as succinylcholine, can cause a massive release of intracellular potassium and catastrophic rhabdomyolysis. This leads to severe hyperkalemia, triggering malignant hyperthermia-like reactions and intractable cardiac arrest. Therefore, succinylcholine is absolutely contraindicated in DMD.
Question 39:
A 2-month-old infant is brought to the clinic due to a consistent head posture. The mother notes the baby's head is tilted toward the right shoulder, and the chin is rotated toward the left. On examination, a firm, non-tender, olive-shaped mass is palpable in the lower third of the right sternocleidomastoid muscle. What is the most appropriate initial management for this condition?
Options:
- Immediate MRI of the cervical spine to rule out congenital vertebral anomalies
- Surgical unipolar release of the sternocleidomastoid muscle
- Initiation of a physical therapy program focused on gentle stretching exercises
- Botulinum toxin A injection into the affected muscle mass
- Application of a cervical collar to force the head into a neutral position
Correct Answer: Initiation of a physical therapy program focused on gentle stretching exercises
Explanation:
The clinical presentation is classic for Congenital Muscular Torticollis (CMT) with an SCM pseudo-tumor (fibromatosis colli). The initial management for CMT is conservative, consisting of a physical therapy program emphasizing gentle, sustained passive stretching of the affected sternocleidomastoid muscle, as well as positioning techniques. This resolves the condition in over 90% of cases if initiated early (<1 year of age). Surgical release is reserved for recalcitrant cases persisting beyond 12-18 months of age.
Question 40:
A newborn is evaluated in the nursery for severe radial deviation of the right wrist, an absent thumb, and a foreshortened forearm. Radiographs confirm complete absence of the radius (radial longitudinal deficiency / radial clubhand). Before proceeding with any orthopaedic surgical interventions, which set of screening tests is most critical to perform to rule out associated life-threatening syndromic anomalies?
Options:
- Complete blood count (CBC), echocardiogram, and renal ultrasound
- MRI of the brain and entire neuraxis
- Sweat chloride test and pulmonary function testing
- Skeletal survey and genetic testing for Neurofibromatosis Type 1
- Ophthalmologic examination for congenital cataracts and glaucoma
Correct Answer: Complete blood count (CBC), echocardiogram, and renal ultrasound
Explanation:
Radial longitudinal deficiency (radial clubhand) is frequently associated with systemic, potentially life-threatening syndromes. These include VACTERL association (requires renal ultrasound for anomalies and echocardiogram), Holt-Oram syndrome (cardiac septal defects requiring an echocardiogram), Thrombocytopenia-Absent Radius (TAR) syndrome, and Fanconi anemia (both requiring a CBC to check for severe cytopenias/aplastic anemia). Therefore, a CBC, echocardiogram, and renal ultrasound are mandatory initial screening tests.
Question 41:
A 12-year-old boy presents with frequent ankle sprains and a painful, rigid flatfoot. Physical examination reveals limited subtalar motion and peroneal muscle spasm. A lateral radiograph demonstrates a continuous C-shaped arc connecting the talar dome and the sustentaculum tali. What is the most appropriate initial management for this condition?
Options:
- Surgical resection of the coalition with interposition arthroplasty
- Subtalar arthrodesis
- Short leg walking cast for 4 to 6 weeks
- Triple arthrodesis
- Physical therapy focusing on peroneal strengthening
Correct Answer: Short leg walking cast for 4 to 6 weeks
Explanation:
The clinical and radiographic presentation ('C-sign') is diagnostic of a talocalcaneal (subtalar) coalition. Initial treatment for a symptomatic tarsal coalition is almost always nonoperative, typically involving immobilization in a short leg walking cast for 4 to 6 weeks. This helps to rest the joint and relieve the painful peroneal muscle spasms. Surgical resection is indicated only if conservative measures fail.
Question 42:
A 13-year-old obese boy presents with acute on chronic left groin pain and an inability to bear weight on the left leg for the past 24 hours. Radiographs confirm a slipped capital femoral epiphysis (SCFE). Which of the following is the most significant prognostic factor for the development of osteonecrosis in this patient?
Options:
- The degree of posterior epiphyseal tilt
- The chronicity of his preceding pain
- His body mass index (BMI)
- The inability to bear weight at presentation
- The presence of bilateral involvement
Correct Answer: The inability to bear weight at presentation
Explanation:
The inability to bear weight (with or without crutches) defines an 'unstable' SCFE according to the Loder classification. This is the most critical prognostic factor for avascular necrosis (AVN). Unstable SCFE has a significantly higher rate of AVN, ranging from 24% to 47%, compared to stable SCFE, where the risk is near zero.
Question 43:
A 6-year-old boy falls from the monkey bars and sustains a Gartland type III supracondylar humerus fracture. Upon arrival in the emergency department, his hand is pink but the radial pulse is absent. After closed reduction and percutaneous pinning in the operating room, the hand remains pink and well-perfused with brisk capillary refill, but the pulse remains absent via Doppler. What is the most appropriate next step in management?
Options:
- Immediate vascular surgery consultation for brachial artery exploration
- Removal of pins and transition to open reduction
- Observation and hospital admission for close neurovascular monitoring
- Perform a CT angiogram of the upper extremity
- Administer intravenous heparin and systemic vasodilators
Correct Answer: Observation and hospital admission for close neurovascular monitoring
Explanation:
In the setting of a 'pink, pulseless' hand following the closed reduction and pinning of a supracondylar humerus fracture, the most appropriate management is observation and close monitoring (admission). As long as the hand remains well-perfused (capillary refill < 2 seconds, warm, pink), surgical vascular exploration is not indicated because collateral circulation is adequate. Routine angiogram or empirical exploration in a well-perfused hand is unnecessary and potentially harmful.
Question 44:
A 6-week-old female infant is undergoing treatment for developmental dysplasia of the hip (DDH) with a Pavlik harness. During a routine follow-up visit 2 weeks after initiation, the mother notes the child is no longer kicking her affected leg. On examination, there is an absence of active knee extension. What is the most appropriate next step in management?
Options:
- Readjust the anterior strap to increase hip flexion to 120 degrees
- Discontinue the Pavlik harness and switch immediately to a rigid abduction orthosis
- Remove the harness and observe for neurological recovery
- Order an urgent MRI of the lumbar spine to rule out tethered cord
- Perform a closed reduction and spica casting under general anesthesia
Correct Answer: Remove the harness and observe for neurological recovery
Explanation:
The infant has developed a femoral nerve palsy, which is a known complication of the Pavlik harness typically caused by excessive hip flexion (anterior straps adjusted too tightly). The correct initial management is to temporarily remove the harness and allow for neurologic recovery, which almost always occurs spontaneously over several days to weeks. Continuing the harness or increasing flexion would exacerbate the nerve compression.
Question 45:
A 14-year-old girl sustains a twisting ankle injury. Radiographs show a Salter-Harris III fracture of the anterolateral aspect of the distal tibia. Which anatomic structure's avulsion force is directly responsible for this specific fracture pattern?
Options:
- Anterior talofibular ligament
- Posterior inferior tibiofibular ligament
- Calcaneofibular ligament
- Anterior inferior tibiofibular ligament
- Deltoid ligament
Correct Answer: Anterior inferior tibiofibular ligament
Explanation:
This patient has a juvenile Tillaux fracture, which is a Salter-Harris III fracture of the anterolateral distal tibial epiphysis. It is caused by an avulsion force from the anterior inferior tibiofibular ligament (AITFL) during external rotation of the foot. It occurs in adolescents because the distal tibial physis closes in a specific pattern: central, then medial, and finally lateral, leaving the anterolateral portion vulnerable to avulsion.
Question 46:
An 8-year-old boy is diagnosed with Legg-Calvé-Perthes disease. Radiographs reveal approximately 25% collapse of the lateral pillar of the femoral head. According to the Herring lateral pillar classification, what is his classification group, and what is the recommended treatment based on prospective multicenter studies?
Options:
- Group A; symptomatic treatment only
- Group B; observation with restricted weight-bearing
- Group B; surgical containment (e.g., femoral or pelvic osteotomy)
- Group C; physical therapy and NSAIDs
- Group C; surgical containment
Correct Answer: Group B; surgical containment (e.g., femoral or pelvic osteotomy)
Explanation:
This patient has a Herring Lateral Pillar Group B hip (defined as >50% of lateral pillar height maintained; here, 25% collapse means 75% is maintained). According to the benchmark multicenter prospective study by Herring et al., children aged 8 years or older at the time of disease onset with Group B (or B/C border) hips have significantly better radiographic outcomes when treated with surgical containment compared to nonoperative treatment.
Question 47:
During the Ponseti method for the treatment of idiopathic congenital talipes equinovarus, what is the specific pathoanatomic structure primarily targeted by the very first casting manipulation?
Options:
- Equinus of the hindfoot
- Varus of the subtalar joint
- Adductus of the forefoot
- Plantarflexion of the first metatarsal
- Subluxation of the talonavicular joint
Correct Answer: Plantarflexion of the first metatarsal
Explanation:
The Ponseti method corrects the components of clubfoot in a specific sequence: CAVE (Cavus, Adductus, Varus, Equinus). The very first step is to correct the cavus deformity. Cavus is primarily driven by a plantarflexed first ray (first metatarsal). The first manipulation involves elevating the first ray to align the forefoot with the hindfoot, supinating it to match the hindfoot varus.
Question 48:
A 3-year-old girl is evaluated for worsening genu varum. Standing long-leg radiographs demonstrate a metaphyseal-diaphyseal angle (Drennan's angle) of 18 degrees. What is the most appropriate initial management for this patient?
Options:
- Observation and reassurance
- Knee-ankle-foot orthosis (KAFO) during weight-bearing
- Proximal tibial valgus osteotomy
- Guided growth with lateral tension band plating
- Medial plateau elevation osteotomy
Correct Answer: Knee-ankle-foot orthosis (KAFO) during weight-bearing
Explanation:
A metaphyseal-diaphyseal angle (Drennan's angle) greater than 16 degrees strongly predicts progression to infantile Blount disease rather than representing benign physiologic bowing. In a 3-year-old with early infantile Blount disease (typically Langenskiöld stages I-II), a trial of bracing with a KAFO during weight-bearing hours is the initial recommended treatment before considering surgical realignment.
Question 49:
A 4-year-old child with a history of multiple low-energy fractures, blue sclerae, and dentinogenesis imperfecta is started on pamidronate therapy. What is the primary cellular mechanism of action of this pharmacological agent?
Options:
- Stimulation of osteoblast differentiation via Wnt signaling
- Inhibition of farnesyl pyrophosphate synthase in osteoclasts
- Direct binding to the RANKL receptor, preventing osteoclast activation
- Enhancement of type I collagen synthesis in osteoblasts
- Inhibition of sclerostin, increasing bone formation
Correct Answer: Inhibition of farnesyl pyrophosphate synthase in osteoclasts
Explanation:
Pamidronate is a nitrogen-containing bisphosphonate frequently used in the treatment of moderate to severe Osteogenesis Imperfecta (OI) to decrease fracture incidence and improve bone density. Nitrogen-containing bisphosphonates exert their antiresorptive effect by inhibiting farnesyl pyrophosphate synthase within the mevalonate pathway in osteoclasts. This leads to disruption of intracellular protein lipidation, resulting in osteoclast apoptosis.
Question 50:
A newborn is evaluated in the nursery and diagnosed with isolated fibular hemimelia. Which of the following associated physical findings or structural anomalies is MOST likely to be present in this patient?
Options:
- Absent medial rays of the foot
- Anterior cruciate ligament deficiency
- Developmental dysplasia of the hip
- Sprengel deformity
- Radial clubhand
Correct Answer: Anterior cruciate ligament deficiency
Explanation:
Fibular hemimelia is the most common congenital long bone deficiency. It is highly associated with anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL) deficiency, absent lateral rays of the foot, a ball-and-socket ankle joint, tarsal coalition, and anteromedial tibial bowing. Absent medial rays are classically associated with tibial hemimelia.
Question 51:
A 2-year-old child presents with a significantly shortened lower extremity. Radiographs reveal a severe congenital anomaly of the femur characterized by a complete lack of osseous connection between the femoral head and the short femoral shaft, although a competent femoral head is present within a normal acetabulum. According to the Aitken classification of Proximal Focal Femoral Deficiency (PFFD), which class does this represent?
Options:
- Class A
- Class B
- Class C
- Class D
- Class E
Correct Answer: Class B
Explanation:
In the Aitken classification of PFFD: Class A has a short femur with a femoral head and a cartilaginous connection that eventually ossifies. Class B has a femoral head present in the acetabulum but no osseous connection between the head and the short femoral shaft (pseudarthrosis). Class C lacks a femoral head or has a severely dysplastic one, with an absent connection. Class D has neither a femoral head nor an acetabulum, and a severely shortened femur.
Question 52:
A 7-year-old non-ambulatory child with spastic quadriplegic cerebral palsy (GMFCS Level V) is undergoing routine radiographic hip surveillance. Measurement of the Reimers Migration Percentage (RMP) is obtained. At what specific RMP threshold is surgical intervention (e.g., adductor/iliopsoas release or varus derotational osteotomy) most widely recommended to prevent progression to complete dislocation?
Options:
Correct Answer: 30-40%
Explanation:
In children with cerebral palsy, a Reimers Migration Percentage (RMP) greater than 30% to 40% is highly predictive of continued lateral subluxation and eventual painful dislocation. Orthopedic guidelines universally recommend surgical intervention (which may range from soft tissue release to bony reconstruction, depending on age and femoral head deformity) once the RMP exceeds the 30-40% threshold to maintain a concentric, painless hip.
Question 53:
A 14-year-old gymnast presents with chronic lower back pain and notably tight hamstrings. Standing lateral radiographs reveal a 60% anterior slip of L5 on S1. Which type of spondylolisthesis according to the Wiltse classification is most commonly associated with this specific patient demographic and clinical presentation?
Options:
- Type I (Dysplastic)
- Type II (Isthmic)
- Type III (Degenerative)
- Type IV (Traumatic)
- Type V (Pathologic)
Correct Answer: Type II (Isthmic)
Explanation:
Type II (Isthmic) spondylolisthesis is caused by a defect or stress fracture in the pars interarticularis. It is the most common type of spondylolisthesis in children and adolescents, particularly in athletes who perform repetitive hyperextension activities (e.g., gymnasts, divers, football linemen). Tight hamstrings (causing the Phalen-Dickson sign or a 'waddling' gait) are a classic physical finding in high-grade slips.
Question 54:
An 8-year-old boy presents with a painful clunking sensation in his left knee when walking. MRI confirms a discoid lateral meniscus. During arthroscopic evaluation, the meniscus is found to be hypermobile due to an absent posterior meniscotibial attachment, tethered only by the meniscofemoral ligament. Which Watanabe type does this represent?
Options:
- Type I
- Type II
- Type III
- Type IV
- Type V
Correct Answer: Type III
Explanation:
The Watanabe classification of discoid meniscus describes three types: Type I (Complete) covers the entire tibial plateau and has normal attachments; Type II (Incomplete) partially covers the plateau and has normal attachments; Type III (Wrisberg variant) lacks the normal posterior meniscotibial attachment (coronary ligament), relying solely on the meniscofemoral ligament of Wrisberg. This leads to a hypermobile meniscus and the classic 'snapping knee' syndrome.
Question 55:
A 1-month-old infant is brought to the clinic for a right-sided neck mass and a persistent head tilt to the right with the chin rotated to the left. The mass is firm, non-tender, and located within the sternocleidomastoid muscle. What associated condition must be actively screened for in this patient?
Options:
- Vesicoureteral reflux
- Sprengel deformity
- Developmental dysplasia of the hip
- Congenital scoliosis
- Craniosynostosis
Correct Answer: Developmental dysplasia of the hip
Explanation:
The infant's presentation is classic for congenital muscular torticollis (CMT), which typically presents with a palpable sternocleidomastoid 'tumor' (fibrosis) at 2 to 4 weeks of age. There is a well-established clinical association between CMT and developmental dysplasia of the hip (DDH), occurring in up to 8-20% of cases. Rigorous screening for DDH, usually including an ultrasound of the hips, is the standard of care for these infants.
Question 56:
A 12-year-old girl presents with bilateral wrist pain and a noticeable prominence of the distal ulna. Radiographs show increased volar tilt and ulnar inclination of the distal radial articular surface, with premature fusion of the ulnar half of the distal radial physis. If this condition is part of an underlying genetic syndrome, what is the most likely gene mutation?
Options:
- COL1A1
- FGFR3
- SHOX
- EXT1
- FBN1
Correct Answer: SHOX
Explanation:
The clinical and radiographic presentation is classic for Madelung deformity, characterized by premature closure of the volar-ulnar aspect of the distal radial physis. When presenting bilaterally and associated with mesomelic short stature, it is often part of Léri-Weill dyschondrosteosis. This condition is inherited in a pseudoautosomal dominant manner due to mutations or deletions in the SHOX gene.
Question 57:
A 2-year-old boy presents with severe anterolateral bowing of his left tibia that recently sustained a low-energy fracture. Radiographs show a midshaft tibial nonunion with 'hourglass' tapering of the sclerotic bone ends. What systemic condition is overwhelmingly associated with this specific orthopedic pathology?
Options:
- Osteogenesis Imperfecta
- Neurofibromatosis type 1
- Achondroplasia
- Ehlers-Danlos Syndrome
- McCune-Albright Syndrome
Correct Answer: Neurofibromatosis type 1
Explanation:
Anterolateral bowing of the tibia and subsequent congenital pseudarthrosis of the tibia (CPT) are highly associated with Neurofibromatosis type 1 (NF1). Over 50% of patients with CPT have an underlying diagnosis of NF1. CPT is notorious for being refractory to standard fracture healing, often requiring complex reconstructive surgery (e.g., Ilizarov bone transport, vascularized free fibular grafts) or occasionally amputation.
Question 58:
A 10-year-old soccer player with widely open physes (Tanner stage 1) sustains an isolated, complete rupture of the anterior cruciate ligament. Operative reconstruction is planned using a completely physeal-sparing technique to avoid growth arrest. Which graft choice and routing strategy best describes the classic modified MacIntosh (Micheli/Kocher) technique?
Options:
- Transphyseal hamstring autograft with suspensory cortical fixation
- Bone-patellar tendon-bone autograft drilled directly through the physeal plates
- Iliotibial band autograft routed over the top of the lateral femoral condyle and under the intermeniscal ligament
- Quadriceps tendon autograft using all-inside partial tunnels
- Achilles tendon allograft through standard adult trans-tibial tunnels
Correct Answer: Iliotibial band autograft routed over the top of the lateral femoral condyle and under the intermeniscal ligament
Explanation:
In prepubescent children with significant remaining growth, a completely physeal-sparing technique is indicated. The modified MacIntosh (Micheli/Kocher) technique utilizes an iliotibial band (ITB) autograft. It is left attached distally at Gerdy's tubercle, routed 'over the top' of the lateral femoral condyle (avoiding the distal femoral physis), and passed under the intermeniscal ligament or through the proximal tibial epiphysis (avoiding the proximal tibial physis).
Question 59:
A 10-year-old girl sustains a valgus injury to her knee. Radiographs reveal a fracture passing completely through the physis of the distal femur without any extension into the metaphysis or epiphysis. According to the Salter-Harris classification, what type of fracture is this, and what is its unique prognostic characteristic at this specific anatomical location?
Options:
- Type I; associated with a high rate of physeal growth arrest
- Type I; low risk of growth arrest due to an intact germinal layer
- Type II; characterized by a metaphyseal flag and extremely low risk of deformity
- Type III; completely extra-articular but high risk of nonunion
- Type V; invariably benign outcome despite initial appearance
Correct Answer: Type I; associated with a high rate of physeal growth arrest
Explanation:
A fracture entirely through the physis without metaphyseal or epiphyseal extension is a Salter-Harris Type I. While Type I fractures generally have a low risk of growth arrest in most locations, the distal femoral physis is a notable exception. Salter-Harris I and II fractures of the distal femur have a notoriously high rate of growth arrest (up to 40-50%) because the undulating, highly interdigitated nature of this physis sustains significant crushing force to the germinal layer during displacement.
Question 60:
A 6-year-old child presents with a short neck, low posterior hairline, and severely limited cervical range of motion. A diagnosis of Klippel-Feil syndrome is clinically suspected and confirmed on radiographs showing multiple fused cervical vertebrae. Which associated systemic anomaly is most critical to evaluate for in the initial screening of this patient?
Options:
- Congenital heart defects
- Renal anomalies
- Sensorineural hearing loss
- Intestinal malrotation
- Hypothyroidism
Correct Answer: Renal anomalies
Explanation:
Klippel-Feil syndrome is characterized by congenital fusion of two or more cervical vertebrae. The classic triad (short neck, low hairline, restricted neck motion) is present in fewer than 50% of patients. Renal anomalies (e.g., unilateral kidney, horseshoe kidney, duplication of the collecting system) are highly prevalent (occurring in 30-35% of cases) and can be life-threatening if missed. Therefore, renal ultrasound screening is universally mandated in orthopedic guidelines for these patients.
Question 61:
A 2-year-old presents with anteromedial bowing of the tibia and a shortened lower extremity. Radiographs reveal an absent fibula. Which of the following findings is most commonly associated with this condition?
Options:
- Anterolateral tibial bowing
- Polydactyly of the foot
- Anterior cruciate ligament deficiency
- Congenital coxa vara
- Talocalcaneal coalition
Correct Answer: Anterior cruciate ligament deficiency
Explanation:
Fibular hemimelia is the most common congenital long bone deficiency. It presents with anteromedial bowing of the tibia, limb shortening, and is frequently associated with an absent or deficient anterior cruciate ligament (ACL) (up to 100% of cases), absent lateral rays of the foot, ball-and-socket ankle joint, and tarsal coalitions (most commonly talocalcaneal). Anterolateral tibial bowing is associated with congenital pseudarthrosis of the tibia.
Question 62:
A 6-year-old child with GMFCS level IV spastic quadriplegic cerebral palsy is evaluated during routine hip surveillance. Radiographs demonstrate a Reimers migration index of 45% bilaterally with disruption of Shenton's line, but no advanced degenerative changes or head deformation. What is the most appropriate management?
Options:
- Botulinum toxin injections to the adductors
- Adductor and iliopsoas tenotomies alone
- Bilateral varus derotational osteotomies (VDRO) with or without pelvic osteotomies
- Bilateral proximal femoral resection (Castle procedure)
- Observation and repeat radiograph in 6 months
Correct Answer: Bilateral varus derotational osteotomies (VDRO) with or without pelvic osteotomies
Explanation:
In children with spastic cerebral palsy, hip subluxation is common and monitored via the Reimers migration index (percentage of the femoral head uncovered by the acetabulum). Soft tissue releases alone are indicated for early disease (migration index 20-30%, generally in children <4 years old). Once the migration index exceeds 30-40%, or in older children (like this 6-year-old), bony reconstruction with a Varus Derotational Osteotomy (VDRO) and frequently a concomitant pelvic osteotomy is indicated to safely center the hip and prevent painful dislocation. Salvage procedures like a Castle procedure are for chronically painful, dislocated hips with severe articular damage.
Question 63:
A 4-year-old boy presents with multiple low-energy fractures, blue sclerae, and dentinogenesis imperfecta. He is diagnosed with Osteogenesis Imperfecta (OI) type I. The genetic defect most likely involves a mutation resulting in which of the following abnormalities?
Options:
- Defective mineralization of the osteoid matrix
- Quantitative deficiency in the production of normal type I collagen
- Qualitative defect in type II collagen synthesis
- Fibroblast growth factor receptor 3 (FGFR3) gain-of-function
- Defect in Cartilage Oligomeric Matrix Protein (COMP)
Correct Answer: Quantitative deficiency in the production of normal type I collagen
Explanation:
Osteogenesis Imperfecta (OI) type I is the mildest and most common form of the disease. According to the Sillence classification, Type I is characterized by a null mutation in the COL1A1 gene, leading to a decreased amount (quantitative defect) of structurally normal type I collagen. This leads to mild to moderate bone fragility, blue sclerae, and hearing loss. In contrast, OI types II, III, and IV typically involve missense mutations causing structurally abnormal (qualitative defect) type I collagen, resulting in more severe phenotypes.
Question 64:
An infant presents with unilateral anterolateral bowing of the tibia. A radiograph demonstrates medullary narrowing and cortical sclerosis at the apex of the bow. This condition has the strongest association with which of the following genetic disorders?
Options:
- Neurofibromatosis type 1
- Marfan syndrome
- Osteogenesis imperfecta
- Achondroplasia
- Ehlers-Danlos syndrome
Correct Answer: Neurofibromatosis type 1
Explanation:
Anterolateral bowing of the tibia is characteristic of Congenital Pseudarthrosis of the Tibia (CPT). The tissue at the pseudoarthrosis site is a fibrous hamartoma. Approximately 50% of patients diagnosed with CPT also have Neurofibromatosis type 1 (NF1). Patients with NF1 must be screened clinically for this deformity. In contrast, posteromedial bowing is typically physiological or associated with a calcaneovalgus foot and resolves spontaneously, and anteromedial bowing is seen with fibular hemimelia.
Question 65:
A 6-month-old infant with a homozygous FGFR3 mutation (achondroplasia phenotype) presents with failure to thrive, hyperreflexia, and central sleep apnea. Which of the following is the most appropriate next step in management?
Options:
- Polysomnography followed by nocturnal CPAP
- MRI of the craniocervical junction
- Observation, as these symptoms typically resolve by age 2 with cranial growth
- Immediate suboccipital decompression with C1 laminectomy without further imaging
- High-dose Vitamin D and calcium supplementation
Correct Answer: MRI of the craniocervical junction
Explanation:
Achondroplasia is caused by an activating mutation in FGFR3, inhibiting enchondral ossification. The most life-threatening complication in infants is cervicomedullary compression at the foramen magnum. Clinical signs include central sleep apnea, failure to thrive, brisk reflexes, and hypotonia. When these symptoms are present, prompt MRI of the craniocervical junction is mandatory to evaluate the severity of foramen magnum stenosis prior to surgical intervention (suboccipital decompression).
Question 66:
A newborn is noted to have severe radial deviation of the right wrist, an absent right thumb, and shortening of the right forearm. Radiographs reveal an absent radius. To rule out the most life-threatening associated condition, which of the following screening tests should be ordered initially?
Options:
- Renal ultrasound
- Echocardiogram
- Chromosomal breakage test (Diepoxybutane test)
- Complete blood count (CBC) with peripheral smear
- Whole-spine MRI
Correct Answer: Chromosomal breakage test (Diepoxybutane test)
Explanation:
Radial longitudinal deficiency (radial clubhand) is strongly associated with several systemic syndromes including VACTERL, TAR (Thrombocytopenia-Absent Radius), Holt-Oram, and Fanconi anemia.
Fanconi anemia is the most life-threatening because it leads to fatal aplastic anemia and a high risk of malignancies (leukemia). The definitive screening test is chromosomal breakage analysis induced by diepoxybutane (DEB). A CBC may be normal in the neonatal period before marrow failure manifests, making it an insufficient screen.
Question 67:
A 9-month-old male is evaluated for a left thoracic spinal curve of 25 degrees. The rib-vertebra angle difference (RVAD) of Mehta is measured at 28 degrees. Phase 2 rib-head overlap is noted on the apical vertebra. What is the most likely natural history and appropriate treatment for this deformity?
Options:
- High likelihood of spontaneous resolution; observe
- High likelihood of progression; serial Mehta casting
- High likelihood of progression; immediate posterior spinal fusion
- Moderate likelihood of progression; prescribe a Milwaukee brace
- Likelihood of progression cannot be determined; observe for 6 months
Correct Answer: High likelihood of progression; serial Mehta casting
Explanation:
Infantile idiopathic scoliosis occurs in children <3 years old, most commonly in males with left-sided thoracic curves. The Mehta Rib-Vertebra Angle Difference (RVAD) predicts progression: an RVAD >20 degrees, especially with Phase 2 rib-head overlap, indicates a progressive curve. The gold standard early treatment for progressive infantile idiopathic scoliosis is elongation-derotation-flexion casting (Mehta casting), which harnesses infantile growth to correct the deformity.
Question 68:
A 3-year-old child presents with severe genu varum and short stature. Laboratory tests reveal normal serum calcium, significantly decreased serum phosphate, normal parathyroid hormone (PTH), and elevated alkaline phosphatase. Genetic testing reveals a PHEX mutation. The underlying pathophysiology involves an excess of which of the following?
Options:
- Parathyroid hormone-related peptide (PTHrP)
- Fibroblast growth factor 23 (FGF23)
- 1-alpha-hydroxylase
- Bone morphogenetic protein 2 (BMP-2)
- Osteoprotegerin
Correct Answer: Fibroblast growth factor 23 (FGF23)
Explanation:
The clinical picture describes X-linked hypophosphatemic rickets (XLHR), the most common heritable form of rickets. It is caused by a mutation in the PHEX gene. The PHEX mutation leads to an inability to degrade FGF23, resulting in high levels of circulating FGF23. FGF23 acts on the kidneys to inhibit phosphate reabsorption (causing phosphaturia and hypophosphatemia) and inhibits 1-alpha-hydroxylase, thereby reducing the synthesis of active Vitamin D (1,25-dihydroxyvitamin D).
Question 69:
A 13-year-old girl sustains an ankle injury. Radiographs demonstrate a Salter-Harris III fracture of the anterolateral distal tibia. Which of the following ligaments is responsible for the avulsion of this fracture fragment?
Options:
- Anterior talofibular ligament
- Calcaneofibular ligament
- Anterior inferior tibiofibular ligament
- Posterior inferior tibiofibular ligament
- Deltoid ligament
Correct Answer: Anterior inferior tibiofibular ligament
Explanation:
A juvenile Tillaux fracture is a Salter-Harris III fracture of the anterolateral distal tibial epiphysis. It occurs during adolescence due to the asymmetric closure pattern of the distal tibial physis (closes central -> anteromedial -> posteromedial -> lateral last). An external rotation force applied to the foot puts tension on the Anterior Inferior Tibiofibular Ligament (AITFL), which avulses the unfused anterolateral epiphysis.
Question 70:
A 2-year-old girl is noted to have a spinal deformity. Radiographs show a fully segmented hemivertebra at T8 causing a 35-degree scoliotic curve. Prior to surgical intervention, which of the following screening studies are mandatory to evaluate for the most commonly associated anomalies?
Options:
- Echocardiogram and brain MRI
- Renal ultrasound and whole-spine MRI
- Renal ultrasound and pulmonary function tests
- Echocardiogram and chromosomal microarray
- Pelvic ultrasound and lower extremity radiographs
Correct Answer: Renal ultrasound and whole-spine MRI
Explanation:
Congenital scoliosis, resulting from failures of formation (e.g., hemivertebra) or segmentation, has a high association with other organ system anomalies occurring during the same embryonic period. Genitourinary anomalies (e.g., renal agenesis) occur in 20-30% of patients, requiring a screening renal ultrasound. Intraspinal anomalies (e.g., tethered cord, syringomyelia, diastematomyelia) occur in up to 40%, necessitating an MRI of the entire neural axis. Cardiac anomalies are also common, making echocardiogram a standard part of the workup, but the strict combination of renal US and spine MRI is absolute board-tested standard.
Question 71:
A newborn is diagnosed with Aitken Class A proximal focal femoral deficiency (PFFD). The predicted leg length discrepancy at maturity is 15 cm. The hip joint is present with a cartilaginous connection between the femoral head and shaft, and the foot is normal. Which of the following is the most appropriate long-term surgical strategy?
Options:
- Early knee fusion and Boyd amputation
- Ilizarov lengthening of the femur and tibia
- Van Nes rotationplasty
- Hip arthrodesis and Syme amputation
- Pelvic support osteotomy
Correct Answer: Ilizarov lengthening of the femur and tibia
Explanation:
Aitken Class A PFFD is characterized by the presence of a femoral head and acetabulum, with a cartilaginous connection to the shortened femoral shaft that typically ossifies later, providing a stable, functioning hip. For patients with stable hip and knee joints, a functional foot, and a predicted limb length discrepancy (LLD) of less than 20 cm, limb lengthening procedures (usually staged femoral and tibial lengthening) are indicated. Amputations and rotationplasties are reserved for more severe deficiencies (Aitken C and D, or LLD > 20 cm) where joints are unstable or absent.
Question 72:
A 10-year-old boy presents with frequent ankle sprains and foot pain. Examination reveals a rigid flatfoot and peroneal spasticity. Radiographs demonstrate an 'anteater nose' sign. Which of the following is the most appropriate initial management for this specific condition?
Options:
- Talonavicular arthrodesis
- Resection of the coalition with interposition of the extensor digitorum brevis
- Subtalar arthrodesis
- Short leg cast immobilization for 4-6 weeks
- Medial displacement calcaneal osteotomy
Correct Answer: Short leg cast immobilization for 4-6 weeks
Explanation:
The 'anteater nose' sign is seen on the oblique foot radiograph and is pathognomonic for a calcaneonavicular tarsal coalition. Regardless of the coalition type (calcaneonavicular or talocalcaneal), the initial management for symptomatic tarsal coalition is nonoperative to allow for inflammation to subside. This typically involves immobilization with a short leg walking cast or a rigid orthosis for 4 to 6 weeks. Surgical resection (e.g., with EDB or fat interposition) is indicated only if conservative measures fail.
Question 73:
A 2.5-year-old overweight female presents with bilateral tibial bowing. Radiographs demonstrate medial metaphyseal beaking. The Drennan metaphyseal-diaphyseal angle (MDA) is measured at 18 degrees on the right and 10 degrees on the left. Which of the following is the most appropriate management?
Options:
- Reassurance and observation for both legs
- Knee-ankle-foot orthosis (KAFO) for the right leg, observe the left
- Bilateral proximal tibial valgus-producing osteotomies
- Right proximal tibial valgus-producing osteotomy, observe the left
- Guided growth with lateral tension band plates bilaterally
Correct Answer: Knee-ankle-foot orthosis (KAFO) for the right leg, observe the left
Explanation:
Infantile Blount's disease is differentiated from physiologic bowing by an abnormal metaphyseal-diaphyseal angle (MDA) described by Drennan. An MDA > 16 degrees carries a high likelihood of progression, whereas an MDA < 10 degrees is likely physiologic and will resolve. Given the age (under 3 years) and an MDA of 18 degrees on the right, bracing with a KAFO (worn during weight-bearing) is the standard initial treatment to unload the medial compartment. Surgery is indicated if bracing fails or if the child presents with advanced disease > 3-4 years of age.
Question 74:
A 12-year-old obese boy is brought to the emergency department unable to bear weight on his left leg after a minor fall 12 hours ago. He has a 3-week history of preceding left groin pain. Radiographs confirm a severe left slipped capital femoral epiphysis (SCFE). Which of the following accurately describes his risk of developing avascular necrosis (AVN) based on his presentation, and the appropriate urgency of treatment?
Options:
- High risk (up to 50%); urgent pinning or open reduction within 24 hours
- Low risk (<10%); elective pinning within 1 week
- High risk (up to 50%); closed reduction followed by spica casting
- Low risk (<10%); urgent open reduction and internal fixation
- Absolute risk (100%); primary proximal femoral osteotomy
Correct Answer: High risk (up to 50%); urgent pinning or open reduction within 24 hours
Explanation:
The inability to bear weight even with crutches defines an unstable SCFE according to the Loder classification. Unstable SCFE has a very high risk of avascular necrosis (up to 47-50%), in stark contrast to stable SCFE (<10% risk).
Current literature suggests that urgent decompression of the intracapsular hematoma and stable fixation (either pinning in situ or open reduction with a modified Dunn procedure) within 24 hours can mitigate the risk of AVN. Forceful closed reduction is contraindicated as it further increases AVN risk.
Question 75:
A 4-year-old girl is undergoing surgical treatment for residual developmental dysplasia of the hip (DDH). The surgeon plans an incomplete transiliac osteotomy that hinges on the triradiate cartilage, allowing primarily anterior and lateral coverage of the femoral head by changing the volume and shape of the acetabulum, without disrupting the sciatic notch. Which osteotomy is being described?
Options:
- Salter osteotomy
- Pemberton osteotomy
- Dega osteotomy
- Steel triple osteotomy
- Chiari osteotomy
Correct Answer: Pemberton osteotomy
Explanation:
The Pemberton osteotomy is a pericapsular, incomplete osteotomy of the ilium that uses the flexible triradiate (Y) cartilage as a hinge. It redirects the acetabular roof to provide anterolateral coverage and effectively decreases acetabular volume. The Salter osteotomy is a complete transiliac cut that hinges at the pubic symphysis. The Dega is an incomplete transiliac osteotomy typically hinging on intact medial iliac cortex, used heavily in neuromuscular dysplasia to provide lateral, anterior, and posterior coverage without entering the sciatic notch.
Question 76:
A newborn male is noted to have complete simple syndactyly of the right thumb and index finger, as well as the long and ring fingers. No other congenital anomalies are present. Which of the following is the most appropriate surgical timing and strategy?
Options:
- Release all involved digits simultaneously at 18 months
- Release the long/ring syndactyly at 6 months and thumb/index at 18 months
- Release the thumb/index syndactyly at 6 months and long/ring at 12-18 months
- Release both syndactylies simultaneously at 6 months
- Delay all releases until age 3 years to minimize anesthesia risks
Correct Answer: Release the thumb/index syndactyly at 6 months and long/ring at 12-18 months
Explanation:
Syndactyly of 'border digits' (thumb-index, and ring-small) involves digits with significantly different lengths and growth rates. Failure to release these early leads to tethering and progressive angular deformity. Therefore, border digit syndactyly should be released early, typically at 6 months of age. Syndactyly of central digits (long-ring) involves digits that grow at more similar rates; these can be released later, typically between 12-18 months to allow structures to grow larger for easier reconstruction.
Question 77:
A 9-year-old boy presents with a painless limp. Radiographs demonstrate fragmentation of the right capital femoral epiphysis with >50% loss of lateral pillar height. Based on the Herring Lateral Pillar Classification, what is the assigned grade and the expected prognosis?
Options:
- Lateral Pillar B; good outcome with nonoperative treatment
- Lateral Pillar C; poor outcome regardless of treatment
- Lateral Pillar B/C; excellent outcome if contained surgically
- Lateral Pillar C; improved outcome with surgical containment compared to conservative
- Lateral Pillar A; good outcome without treatment
Correct Answer: Lateral Pillar C; poor outcome regardless of treatment
Explanation:
According to the Herring Lateral Pillar classification for Legg-Calve-Perthes disease: Group A = no loss of lateral pillar height; Group B = <50% loss; Group C = >50% loss. This patient has Pillar C. The multicenter prospective study by Herring et al. demonstrated that patients over the age of 8 years at the time of disease onset who present with Pillar C hips have uniformly poor outcomes (development of non-spherical femoral heads and early osteoarthritis) regardless of whether they receive conservative or operative containment treatment.
Question 78:
A 6-year-old boy sustains a severe extension-type supracondylar fracture of the humerus. On examination in the emergency department, his hand is pink and warm, with brisk capillary refill, but the radial pulse is not palpable. What is the most appropriate initial management step?
Options:
- Immediate vascular surgery consultation for brachial artery exploration
- CT angiogram of the upper extremity
- Closed reduction and percutaneous pinning, followed by reassessment of the pulse
- Open reduction through an anterior approach to explore the brachial artery
- Application of a long arm cast in 120 degrees of flexion and admit for observation
Correct Answer: Closed reduction and percutaneous pinning, followed by reassessment of the pulse
Explanation:
A 'pink, pulseless hand' following a supracondylar humerus fracture indicates that, while the brachial artery may be kinked or in spasm, collateral circulation is adequately maintaining distal perfusion. The gold standard initial management is prompt closed reduction and percutaneous pinning (CRPP) to restore anatomy and relieve kinking. Reassessment of the pulse and perfusion follows fixation. Routine vascular exploration is not indicated initially if the hand remains well-perfused. Casting in severe flexion is contraindicated due to the risk of compartment syndrome.
Question 79:
A 7-year-old ambulatory patient with spastic diplegic cerebral palsy undergoes 3-D computerized gait analysis. Kinematic data reveals decreased peak knee flexion during the swing phase, causing foot drag. Dynamic electromyography (EMG) demonstrates continuous, inappropriate firing of the rectus femoris throughout the swing phase. Which of the following surgical interventions is most specifically indicated for this gait abnormality?
Options:
- Hamstring lengthening
- Distal femoral extension osteotomy
- Rectus femoris transfer to the sartorius or gracilis
- Patellar tendon advancement
- Gastrocnemius recession
Correct Answer: Rectus femoris transfer to the sartorius or gracilis
Explanation:
A 'stiff-knee gait' in cerebral palsy is characterized by reduced peak knee flexion during the swing phase, which impairs ground clearance (causing toe drag or circumduction). It is primarily caused by overactivity or spasticity of the rectus femoris muscle during swing. The standard treatment to address this dynamic contracture is a rectus femoris transfer (e.g., to the sartorius, gracilis, or semitendinosus), which converts the rectus from a knee extensor/inhibitor of flexion into a knee flexor, thereby improving swing-phase knee kinematics.
Question 80:
A 2-week-old neonate presents with decreased spontaneous movement of the right lower extremity, swelling of the right thigh, and pain with passive hip motion. Ultrasound demonstrates a large hip effusion. What anatomical feature unique to infants younger than 18 months predisposes them to concurrent osteomyelitis and septic arthritis in this location?
Options:
- An incomplete physical barrier at the articular cartilage
- A highly cellular hypertrophic zone of the physis
- The presence of transphyseal blood vessels connecting the metaphysis and epiphysis
- A thick, non-yielding periosteum surrounding the femoral neck
- The absence of an intra-articular ligamentum teres
Correct Answer: The presence of transphyseal blood vessels connecting the metaphysis and epiphysis
Explanation:
In neonates and infants younger than 12-18 months, there are transphyseal blood vessels that cross the physis, establishing direct communication between the metaphysis and the epiphysis (and by extension, the intra-articular space). This unique vascular anatomy allows an infection that begins as metaphyseal osteomyelitis to easily cross into the joint space, resulting in concomitant septic arthritis, which rapidly destroys the chondroepiphysis and increases the risk of avascular necrosis of the femoral head.
Question 81:
A pediatric patient presents with a congenital spinal deformity. Which of the following specific vertebral anomalies carries the highest risk of rapid curve progression and often requires early surgical intervention?
Options:
- A single block vertebra
- A wedge vertebra
- An unsegmented hemivertebra
- A fully segmented hemivertebra with a contralateral unsegmented bar
- A butterfly vertebra
Correct Answer: A fully segmented hemivertebra with a contralateral unsegmented bar
Explanation:
The highest risk for rapid curve progression in congenital scoliosis is seen with a fully segmented hemivertebra accompanied by a contralateral unsegmented bar. This creates unbalanced, asymmetric growth (growth potential on one side without corresponding growth on the contralateral tethered side). This combination progresses at a rate of 5 to 10 degrees per year and requires early surgical fusion to halt progression.
Question 82:
A 3-year-old child presents with worsening bilateral tibia vara. You are evaluating the radiograph to differentiate between physiologic bowing and infantile Blount disease. Which of the following radiographic parameters correctly points towards the diagnosis of infantile Blount disease?
Options:
- Tibiofemoral angle > 15 degrees
- Metaphyseal-diaphyseal angle (MDA) > 16 degrees
- Metaphyseal-diaphyseal angle (MDA) < 11 degrees
- Mechanical axis deviation (MAD) strictly in the lateral compartment
- A narrow distal femoral physis
Correct Answer: Metaphyseal-diaphyseal angle (MDA) > 16 degrees
Explanation:
The metaphyseal-diaphyseal angle (MDA), or Drennan's angle, is used to differentiate physiologic bowing from infantile Blount disease. An MDA greater than 16 degrees has a high likelihood of progressing to Blount disease, whereas an MDA of less than 11 degrees typically indicates physiologic bowing that will resolve spontaneously.
Question 83:
A neonate sustains multiple long bone fractures during delivery. Genetic testing reveals a qualitative defect in Type I collagen. According to the Sillence classification for Osteogenesis Imperfecta (OI), which type is characterized as perinatally lethal?
Options:
- Type I
- Type II
- Type III
- Type IV
- Type V
Correct Answer: Type II
Explanation:
Osteogenesis imperfecta (OI) is a connective tissue disorder typically caused by defects in the COL1A1 or COL1A2 genes. In the Sillence classification, Type II is perinatally lethal, often presenting with multiple rib and long bone fractures in utero and severe pulmonary hypoplasia. Type I is the most common and mildest form; Type III is progressively deforming; and Type IV is intermediate in severity.
Question 84:
A 2-year-old child presents with short stature, frontal bossing, and rhizomelic shortening of the limbs. Which of the following best describes the molecular pathophysiology of this condition?
Options:
- Loss-of-function mutation in COL1A1
- Loss-of-function mutation in FGFR3
- Gain-of-function mutation in FGFR3
- Mutation in Cartilage Oligomeric Matrix Protein (COMP)
- Mutation in the CBFA1/RUNX2 transcription factor
Correct Answer: Gain-of-function mutation in FGFR3
Explanation:
The patient has achondroplasia, the most common form of dwarfism, which is characterized by rhizomelic (proximal) limb shortening. It is inherited in an autosomal dominant fashion, though 80% are new mutations. The pathophysiology involves a gain-of-function mutation in the Fibroblast Growth Factor Receptor 3 (FGFR3) gene on chromosome 4, which abnormally inhibits chondrocyte proliferation in the proliferative zone of the physis.
Question 85:
A 14-year-old boy presents with recurrent right ankle sprains, pain, and a rigid, flat arch. A classic 'C-sign' is noted on the lateral ankle radiograph. This finding indicates a tarsal coalition most commonly involving which specific joint?
Options:
- Calcaneonavicular joint
- Anterior facet of the talocalcaneal joint
- Middle facet of the talocalcaneal joint
- Posterior facet of the talocalcaneal joint
- Talonavicular joint
Correct Answer: Middle facet of the talocalcaneal joint
Explanation:
The 'C-sign' on a lateral radiograph is a continuous C-shaped arc formed by the medial border of the talar dome and the posterior outline of the sustentaculum tali. It is highly specific for a talocalcaneal coalition, which overwhelmingly involves the middle facet. Calcaneonavicular coalitions are visualized on oblique radiographs (the 'anteater nose' sign).
Question 86:
You are evaluating a 6-year-old with spastic quadriplegic cerebral palsy as part of routine hip surveillance. According to most hip surveillance guidelines, reconstructive bony surgery (e.g., varus derotational osteotomy and pelvic osteotomy) is generally indicated when the Reimers Migration Percentage (MP) exceeds what threshold?
Options:
Correct Answer: 40%
Explanation:
In cerebral palsy hip surveillance, Reimers Migration Percentage (MP) is the key radiographic parameter. An MP > 30% indicates subluxation. While soft tissue releases (adductors/psoas) may be indicated for an MP of 30-40%, reconstructive bony surgery (VDRO and often pelvic osteotomy) is formally indicated when the MP exceeds 40% with architectural dysplasia, as non-operative or soft tissue management alone is likely to fail.
Question 87:
A 5-year-old girl is evaluated for a high-riding, hypoplastic left scapula. Imaging reveals a bony bridge between the cervical spine and the superior angle of the scapula (an omovertebral bone). This deformity is most frequently associated with which of the following?
Options:
- Trisomy 21
- Klippel-Feil syndrome
- VACTERL association
- Neurofibromatosis Type 1
- Marfan syndrome
Correct Answer: Klippel-Feil syndrome
Explanation:
The patient has Sprengel deformity, an arrest of the normal embryologic descent of the scapula. About 30% of cases feature an omovertebral bone. It is strongly associated with Klippel-Feil syndrome (congenital fusion of cervical vertebrae) as well as congenital scoliosis and diastematomyelia. Careful screening of the cervical spine and renal system is mandated.
Question 88:
A newborn presents with a shortened right lower extremity, an anteromedial bowing of the tibia, and an absent lateral ray (toe) of the right foot. Radiographs confirm fibular hemimelia. Which of the following soft-tissue anomalies of the knee is almost universally present in this condition?
Options:
- Absent anterior cruciate ligament
- Absent posterior cruciate ligament
- Absent medial collateral ligament
- Congenital bipartite patella
- Medial patellofemoral ligament hypoplasia
Correct Answer: Absent anterior cruciate ligament
Explanation:
Fibular hemimelia is the most common congenital longitudinal deficiency of the long bones. It is almost universally associated with an absent or hypoplastic anterior cruciate ligament (ACL), a ball-and-socket ankle joint, absent lateral rays of the foot, and variable femoral shortening (often linked with PFFD).
Question 89:
In a patient with Proximal Focal Femoral Deficiency (PFFD), the Aitken classification is widely used to guide treatment. Which Aitken type is characterized by the complete absence of a femoral head and an absent or severely dysplastic acetabulum, precluding joint reconstruction?
Options:
- Type A
- Type B
- Type C
- Type D
- Type E
Correct Answer: Type D
Explanation:
The Aitken classification of PFFD includes four types (A-D). Type D represents the most severe form, characterized by an absent acetabulum, absent femoral head, and severely shortened femoral shaft without a proximal tuft. Types A and B have an existing femoral head with an osseous or cartilaginous connection to the shaft, while Type C has an absent femoral head but a present acetabulum.
Question 90:
A 9-year-old boy presents with a progressive angular deformity of the distal femur following a distal femoral physeal fracture two years prior. Advanced imaging confirms a bony physeal bar. What are the generally accepted criteria for attempting a surgical physeal bar excision?
Options:
- Bar involves > 50% of the physis, and at least 2 cm of growth remaining
- Bar involves < 50% of the physis, and at least 2 cm of growth remaining
- Bar involves < 50% of the physis, and less than 1 year of growth remaining
- Only peripheral bars, regardless of size or growth remaining
- Only central bars, regardless of size or growth remaining
Correct Answer: Bar involves < 50% of the physis, and at least 2 cm of growth remaining
Explanation:
Surgical excision of a physeal bar (with interposition of fat or cranioplast) is generally indicated if the bar encompasses less than 50% of the cross-sectional area of the physis AND the patient has at least 2 years or 2 cm of growth remaining. Exceeding 50% carries a very high rate of failure, and limited remaining growth makes the procedure futile, warranting corrective osteotomy or epiphysiodesis instead.
Question 91:
You are treating an infant with an idiopathic clubfoot using the Ponseti method. The first step involves correcting the cavus deformity. What specific manipulation is required to achieve this first step?
Options:
- Supination of the forefoot with depression of the first metatarsal
- Pronation of the forefoot with depression of the first metatarsal
- Elevation of the first metatarsal to supinate the forefoot
- Abduction of the midfoot with counter-pressure on the medial malleolus
- Forced dorsiflexion of the ankle
Correct Answer: Elevation of the first metatarsal to supinate the forefoot
Explanation:
In the Ponseti method, the acronym CAVE guides the sequence of correction: Cavus, Adductus, Varus, and Equinus. The cavus is corrected first. Because the cavus in a clubfoot is caused by a plantarflexed first ray, correction is achieved by supinating the forefoot to match the hindfoot, which specifically requires elevating the first metatarsal.
Question 92:
A 3-month-old infant is being treated with a Pavlik harness for Developmental Dysplasia of the Hip (DDH). During follow-up, the parents note the child is not kicking the affected leg. On examination, there is decreased spontaneous extension of the knee on the affected side. What is the most likely cause?
Options:
- Sciatic nerve palsy due to hyperflexion
- Obturator nerve palsy due to hyperabduction
- Femoral nerve palsy due to hyperflexion
- Avascular necrosis of the femoral head
- Transient synovitis
Correct Answer: Femoral nerve palsy due to hyperflexion
Explanation:
Femoral nerve palsy is a known complication of the Pavlik harness, typically caused by excessive hip flexion (usually >100-110 degrees). It presents as an inability to extend the knee (quadriceps weakness). The treatment involves relaxing the anterior straps to decrease hip flexion, which usually leads to spontaneous recovery. Hyperabduction, on the other hand, puts the hip at risk for avascular necrosis (AVN).
Question 93:
A 12-year-old boy requires in-situ fixation for a severe, stable slipped capital femoral epiphysis (SCFE). Which of the following clinical profiles is a strong, widely accepted indication for prophylactic pinning of the contralateral, asymptomatic hip?
Options:
- A 12-year-old obese male with an acute unstable SCFE
- A 10-year-old with panhypopituitarism and a history of cranial radiation therapy
- A 14-year-old female with a chronic stable SCFE
- An 11-year-old male with a positive family history of SCFE
- A 13-year-old male with an isolated slip angle of 45 degrees
Correct Answer: A 10-year-old with panhypopituitarism and a history of cranial radiation therapy
Explanation:
Prophylactic pinning of the contralateral hip in SCFE remains controversial for typical idiopathic cases. However, it is strongly indicated in patients with underlying endocrine disorders (such as hypothyroidism, panhypopituitarism), renal osteodystrophy, previous pelvic/cranial radiation, or very young age at presentation (<10 years old), because their risk of developing a contralateral slip can exceed 50-100%.
Question 94:
A 6-year-old boy is undergoing treatment for Legg-Calvé-Perthes disease. You are grading the severity using the Herring Lateral Pillar classification. During the fragmentation phase, the radiograph shows that approximately 60% of the lateral pillar height is maintained. How is this classified?
Options:
- Lateral Pillar Group A
- Lateral Pillar Group B
- Lateral Pillar Group B/C
- Lateral Pillar Group C
- Catterall Group IV
Correct Answer: Lateral Pillar Group B
Explanation:
The Herring Lateral Pillar classification is assessed during the early fragmentation phase. Group A: no involvement of the lateral pillar (100% height). Group B: >50% of lateral pillar height maintained. Group C: <50% of lateral pillar height maintained. Group B/C is a border category with intermediate findings (thin lateral pillar, exactly 50%). Since 60% is maintained, it is Group B.
Question 95:
A 6-year-old girl sustained a Gartland III supracondylar humerus fracture that was managed non-operatively. She develops a severe malunion. If a persistent cubitus varus deformity (gunstock deformity) remains, what is the most significant long-term clinical consequence aside from the cosmetic appearance?
Options:
- Ulnar neuropathy and tardy posterolateral rotatory instability (PLRI)
- Median neuropathy and tardy posteromedial rotatory instability (PMRI)
- Recurrent radial nerve entrapment
- High incidence of recurrent supracondylar fractures
- Avascular necrosis of the trochlea
Correct Answer: Ulnar neuropathy and tardy posterolateral rotatory instability (PLRI)
Explanation:
Cubitus varus is historically considered a largely cosmetic issue with minimal functional deficit in childhood. However, in adulthood, it alters the triceps vector, causing chronic lateral ulnar collateral ligament (LUCL) attenuation, leading to tardy posterolateral rotatory instability (PLRI) and snapping of the medial head of the triceps, which can cause ulnar neuritis/neuropathy.
Question 96:
A 13-year-old girl presents with an ankle fracture involving the anterolateral distal tibial epiphysis, following an external rotation injury. What physiological closure pattern of the distal tibial physis explains the biomechanics of a juvenile Tillaux fracture?
Options:
- Central closes first, followed by anterolateral, then posteromedial
- Central closes first, followed by posteromedial, then anterolateral
- Posteromedial closes first, followed by anterolateral, then central
- Anterolateral closes first, followed by central, then posteromedial
- The physis closes symmetrically from medial to lateral
Correct Answer: Central closes first, followed by posteromedial, then anterolateral
Explanation:
The distal tibial physis begins closing around age 12-14 in an asymmetric pattern: it closes first centrally, then spreads to the anteromedial and posteromedial aspects, and finally closes the anterolateral aspect. Because the anterolateral physis remains open last, an external rotation force avulses the anterolateral epiphysis via the anterior inferior tibiofibular ligament (AITFL), producing a Salter-Harris III fracture (Tillaux fracture).
Question 97:
A 4-year-old boy with multiple café-au-lait spots is diagnosed with Neurofibromatosis Type 1 (NF1) and presents with anterolateral bowing of the tibia. A frank pseudarthrosis has developed. What is the standard, most reliable orthopedic management to achieve union?
Options:
- Simple observation and long leg casting
- Resection of the pseudarthrosis, autogenous bone grafting, and intramedullary rod fixation
- Pulsed electromagnetic field therapy and bracing
- Immediate below-knee amputation
- Epiphysiodesis of the contralateral limb
Correct Answer: Resection of the pseudarthrosis, autogenous bone grafting, and intramedullary rod fixation
Explanation:
Congenital pseudarthrosis of the tibia (CPT) is strongly associated with NF1 (anterolateral bowing). Achieving union is notoriously difficult. The standard and most reliable surgical approach is aggressive resection of the hamartomatous pseudarthrosis tissue back to healthy bleeding bone, voluminous autogenous bone grafting (or BMP), and sturdy intramedullary fixation (e.g., Williams rod or Fassier-Duval rod) that crosses the ankle joint if necessary. Cast immobilization or bracing alone will not achieve union once a pseudarthrosis is present.
Question 98:
A 6-year-old girl with Morquio syndrome (Mucopolysaccharidosis Type IV) is scheduled for orthopedic evaluation. Before planning any surgical procedures, which of the following conditions poses the most immediate, life-threatening risk to this patient?
Options:
- Severe thoracolumbar kyphoscoliosis
- Progressive genu valgum
- Atlantoaxial instability due to odontoid hypoplasia
- Rapidly progressive hip dysplasia
- Early-onset osteoarthritis of the knees
Correct Answer: Atlantoaxial instability due to odontoid hypoplasia
Explanation:
Morquio syndrome (MPS IV) is caused by a deficiency in N-acetylgalactosamine-6-sulfatase or beta-galactosidase. A hallmark skeletal feature is severe odontoid hypoplasia and ligamentous laxity, which leads to life-threatening atlantoaxial instability and cervical myelopathy. Flexion-extension cervical spine radiographs are mandatory to rule out instability before administering general anesthesia to avoid catastrophic spinal cord injury.
Question 99:
Multiple hereditary exostoses (MHE) is a disorder characterized by multiple osteochondromas. It is inherited in an autosomal dominant pattern and is primarily caused by mutations in genes that encode glycosyltransferases. Which genes are implicated in this disorder?
Options:
- FGFR3 and FGFR1
- COMP and MATN3
- COL1A1 and COL1A2
- EXT1 and EXT2
- CBFA1 / RUNX2
Correct Answer: EXT1 and EXT2
Explanation:
Multiple hereditary exostoses (MHE) is caused by mutations in the EXT1 (chromosome 8) or EXT2 (chromosome 11) genes. These genes are tumor suppressors that encode glycosyltransferases responsible for synthesizing heparan sulfate, which is vital for normal chondrocyte proliferation and Indian hedgehog (Ihh) signaling at the physis. FGFR3 is associated with achondroplasia; COMP with multiple epiphyseal dysplasia; COL1A1 with osteogenesis imperfecta; and CBFA1/RUNX2 with cleidocranial dysplasia.
Question 100:
A 10-year-old boy with spastic hemiplegic cerebral palsy presents with a dynamic equinovarus foot deformity evident strictly during the swing phase of gait. He fails bracing, and a Split Anterior Tibial Tendon Transfer (SPLATT) is considered. To which structural location is the lateral half of the transferred tendon typically attached?
Options:
- Navicular tuberosity
- Medial cuneiform
- Cuboid or peroneus brevis tendon
- Achilles tendon
- Flexor hallucis longus tendon
Correct Answer: Cuboid or peroneus brevis tendon
Explanation:
The dynamic equinovarus deformity in CP is often caused by an overactive anterior tibial tendon (ATT) during swing phase. The SPLATT procedure involves splitting the ATT, leaving the medial half attached to its native insertion (medial cuneiform/1st metatarsal) and transferring the lateral half to the lateral aspect of the midfoot, typically the cuboid or into the peroneus brevis tendon. This balances the dorsiflexion forces, neutralizing the varus moment.