Osteochondrosis and Epiphysitis: Comprehensive Surgical Management

Key Takeaway
Osteochondrosis and epiphysitis encompass a spectrum of disorders affecting actively growing epiphyses, primarily driven by localized vascular insufficiency or repetitive microtrauma. While predominantly self-limiting and responsive to conservative measures, refractory cases or late-stage deformities—such as Freiberg infraction or unresolved Osgood-Schlatter ossicles—may necessitate precise surgical intervention. This guide details the biomechanics, diagnostic imaging, and operative techniques required for optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
The terms osteochondrosis and epiphysitis designate a heterogeneous, yet clinically overlapping, group of disorders that primarily affect actively growing epiphyses and apophyses in the pediatric and adolescent populations. While the disorder may occasionally manifest as a localized entity confined to a single epiphysis, it frequently presents with multifocal involvement, either simultaneously or successively across different anatomical regions. The precise etiology of these conditions remains highly debated and is undoubtedly multifactorial; however, an overwhelming consensus within the orthopedic literature points toward a transient, critical lack of vascularity as the primary inciting event. This localized ischemia may be the direct sequela of repetitive microtrauma, subacute embolic infection, rapid periods of skeletal growth outstripping vascular supply, or underlying congenital malformations affecting the microvasculature.
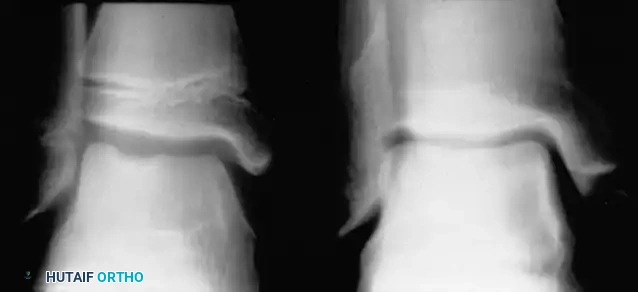
In specific anatomical locations, osteochondrosis presents as a highly distinctive and recognizable clinical entity, such as Freiberg infraction in the metatarsal head or Köhler disease in the tarsal navicular. However, osteochondrosis of intraarticular epiphyses can closely mimic other severe, systemically driven pediatric joint diseases, necessitating a rigorous and exhaustive diagnostic evaluation. For instance, multiple epiphyseal dysplasia (MED) may present with radiographic features that are strikingly similar to Legg-Calvé-Perthes disease of the hip, leading to potential misdiagnosis and inappropriate surgical planning. It is a critical clinical pearl to evaluate the patient's bone age to differentiate MED from Perthes disease. In Perthes disease, the bone age typically lags one to two years behind the chronological age due to the systemic nature of the delayed ossification. In stark contrast, bone age usually remains completely normal in multiple epiphyseal dysplasia. Furthermore, radiographs of the ankle in MED often reveal characteristic lateral narrowing or wedging of the distal tibial epiphysis, a finding absent in isolated osteochondroses.
It is equally critical to distinguish true avascular osteochondroses, which involve a genuine ischemic event to an articular epiphysis, from traction apophysitides, which are purely mechanical in nature. Histological studies of excised specimens by pioneering researchers such as Cohen, Wilkinson, Thompson, Dickinson, Rapp, and Lazerte have definitively concluded that conditions like Osgood-Schlatter disease and Iselin disease are strictly traumatic in origin. These represent traction apophysitides caused by repetitive microavulsions at the tendinous insertion site and are not associated with a primary loss of vascularity. Therefore, they should not be strictly grouped with true osteochondroses in terms of pathophysiology, even though they share similar demographic presentations and conservative management principles.
This chapter focuses exclusively on epiphyseal and apophyseal disorders of the lower extremity that, while frequently self-limiting in their early stages, possess a high propensity to progress to severe structural deformity, secondary osteoarthritis, and debilitating pain requiring complex surgical intervention. Understanding the distinct patho-epidemiology of each entity—from the traction forces in Iselin disease to the ischemic collapse in Freiberg infraction and Köhler disease—is paramount for the practicing orthopedic surgeon to formulate an appropriate, stage-specific treatment algorithm.
Detailed Surgical Anatomy and Biomechanics
Traction Epiphysitis of the Fifth Metatarsal Base (Iselin Disease)
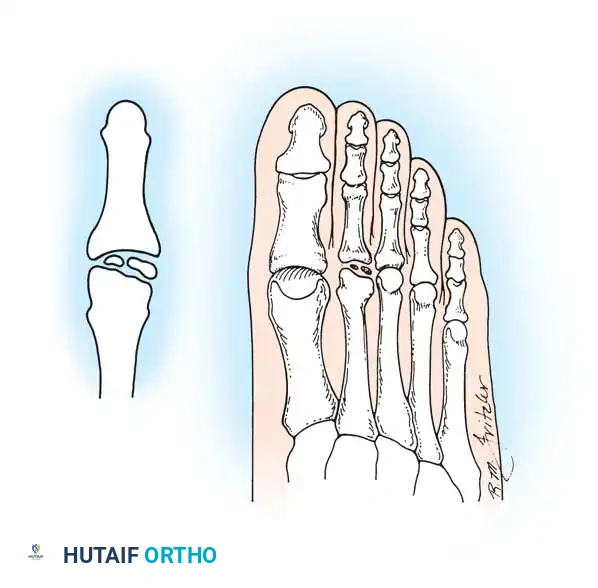
First described by Iselin in the German literature in 1912, Iselin disease is a traction epiphysitis of the base of the fifth metatarsal. It predominantly occurs in young adolescents, corresponding directly to the appearance and maturation of the proximal epiphysis of the fifth metatarsal. The secondary center of ossification is a small, shell-shaped fleck of bone oriented slightly obliquely with respect to the longitudinal axis of the metatarsal shaft. It is located on the lateral plantar aspect of the tuberosity. Anatomical dissections confirm that this ossification center is embedded deeply within the cartilaginous flare into which the peroneus brevis tendon inserts.

Biomechanically, the base of the fifth metatarsal serves as a critical insertion point for both the peroneus brevis tendon and the lateral band of the plantar fascia. During the stance phase of gait, and particularly during athletic activities involving running, jumping, and rapid cutting, the peroneus brevis contracts forcefully to evert the foot and stabilize the lateral column. Repetitive inversion stresses, coupled with the forceful eccentric pull of the peroneus brevis, lead to microavulsions at the chondro-osseous junction of the developing apophysis. This relentless mechanical stress induces a severe inflammatory cascade, resulting in apophysitis. Because the apophysis is extra-articular and subjected primarily to tensile rather than compressive forces, it does not undergo the classic ischemic collapse seen in true osteochondroses, but rather hypertrophies and fragments due to the traction injury.
Osteochondrosis of the Metatarsal Head (Freiberg Infraction)
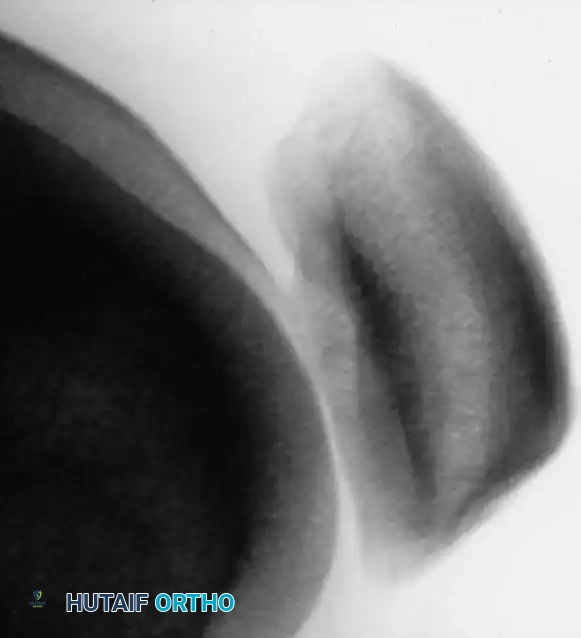
Freiberg infraction is a painful osteochondrosis most commonly affecting the head of the second metatarsal, though it frequently involves the third, and occasionally the fourth and fifth metatarsals. The anatomical predisposition of the second metatarsal to this condition is highly linked to its relative length and the rigid stabilization of its base within the mortise formed by the cuneiforms. Because the second metatarsal is typically the longest and most rigidly fixed ray, it absorbs the highest magnitude of stress during the propulsive toe-off phase of the gait cycle.
The vascular supply to the metatarsal head is precarious, relying heavily on small capsular arteries that penetrate the surgical neck. Repetitive microtrauma to the metatarsal head, particularly in patients with a long second ray or those wearing high-heeled footwear, increases intra-articular pressure and compresses these critical capsular vessels. This leads to a localized vascular watershed zone, resulting in subchondral ischemia, trabecular microfractures, and eventual structural collapse of the articular surface. The dorsal aspect of the metatarsal head is disproportionately affected because it bears the brunt of the compressive and shear forces during maximum dorsiflexion at toe-off.
Osteochondrosis of the Tarsal Navicular (Köhler Disease)
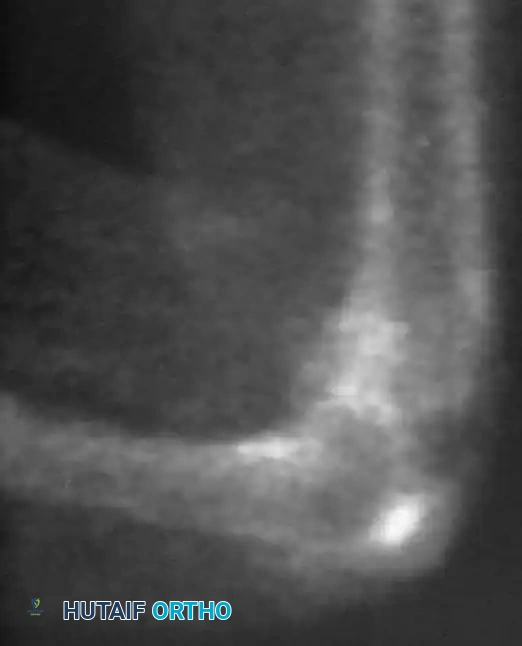
Originally described by Köhler in 1908, this osteochondrosis affects the tarsal navicular, a critical keystone of the medial longitudinal arch. Ossification centers of the navicular typically appear between 1.5 and 2 years of age in girls, and 2.5 and 3 years in boys, making it the last tarsal bone to ossify. Waugh's seminal anatomical studies described the unique and highly vulnerable blood supply to the pediatric navicular. The development of the ossific nucleus is frequently associated with a single central artery, rather than a robust anastomotic network.
Waugh postulated that the delayed ossification subjects the predominantly cartilaginous navicular to excessive mechanical pressure during weight-bearing. As the child grows and becomes more active, the cartilaginous envelope is compressed between the already ossified talus proximally and the cuneiforms distally. This mechanical compression squeezes the delicate osseous vessels passing through the cartilage-bone junction, inducing a transient ischemia. This ischemic event leads to an arrest in ossification, reactive hyperemia in the surrounding tissues, profound subchondral sclerosis, and the characteristic flattening of the navicular seen on radiographs.
Exhaustive Indications and Contraindications
The decision-making process for surgical intervention in osteochondrosis and epiphysitis requires a nuanced understanding of the disease stage, patient age, skeletal maturity, and response to conservative modalities. The vast majority of these conditions in the pediatric population are self-limiting and respond favorably to non-operative management. However, when structural collapse, intra-articular loose bodies, or severe degenerative changes occur, surgical intervention becomes mandatory to restore joint congruity and biomechanical function.
For Iselin disease, surgical intervention is almost universally contraindicated in the acute and subacute phases. Internal fixation or excision of the inflamed apophysis in a growing child risks premature physeal closure, iatrogenic fracture, and disruption of the peroneus brevis insertion. The absolute indication for non-operative management includes acute pain over the fifth metatarsal base with radiographic evidence of apophyseal widening without true fracture. Surgical intervention is strictly reserved for adults who present with a symptomatic, painful non-union of the apophysis (an un-united ossicle) that has failed exhaustive conservative measures, including prolonged immobilization and orthotic management.
In Freiberg infraction, indications for surgery are dictated by the Smillie classification. Early stages (Smillie I-III), characterized by subchondral fissuring and early collapse without severe deformity, are treated conservatively with offloading, metatarsal pads, and stiff-soled shoes. Operative intervention is indicated for advanced stages (Smillie IV-V) where there is significant flattening of the metatarsal head, formation of intra-articular loose bodies, and chronic pain refractory to at least 6 months of conservative care. Procedures range from simple debridement and synovectomy to complex intra-articular corrective osteotomies, such as the Gauthier and Elbaz dorsal closing wedge osteotomy, which aims to rotate healthy plantar cartilage into the functional weight-bearing articulation.
Köhler disease is inherently self-limiting in the pediatric population, and operative treatment is exceedingly rare during the active phase of the disease. The primary indication for treatment is symptomatic relief through short-leg cast immobilization. However, if the navicular heals with severe anatomical distortion, flattening, and sclerosis, it can lead to disabling midfoot arthrosis in adulthood. In these late-stage sequelae, the indication for surgery is severe, activity-limiting midfoot pain accompanied by radiographic evidence of talonavicular or naviculocuneiform osteoarthritis. In such cases, extensive midfoot arthrodesis is the only definitive surgical solution.
| Condition | Primary Surgical Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Iselin Disease | Painful adult non-union failing >6 months of conservative care; symptomatic Os vesalianum excision. | Acute inflammatory phase in children; open apophysis; misdiagnosed acute Jones fracture. | Mild intermittent pain; non-compliance with post-operative immobilization. |
| Freiberg Infraction | Smillie Stage IV-V; intra-articular loose bodies; chronic pain >6 months; severe joint incongruity. | Smillie Stage I-II (acute inflammatory phase); active local infection; severe peripheral vascular disease. | Poor soft tissue envelope; heavy smoking; uncontrolled diabetes mellitus. |
| Köhler Disease (Late) | Disabling adult midfoot arthrosis; severe navicular collapse with adjacent joint arthritis; failed orthotics. | Pediatric phase of active Köhler disease; asymptomatic radiographic sclerosis. | Charcot neuroarthropathy (relative depending on stability); active infection. |
| Talar OCD | Detached, unstable lesions; large cystic lesions >1.5cm; failed 3-6 months of conservative care. | Asymptomatic incidental findings; intact cartilage with subchondral edema only (early stage). | Advanced global ankle osteoarthritis; uncorrected severe hindfoot malalignment. |
Pre-Operative Planning, Templating, and Patient Positioning
Advanced Imaging and Templating
Meticulous pre-operative planning is the cornerstone of successful surgical outcomes in the management of osteochondroses. Standard weight-bearing anteroposterior, lateral, and oblique radiographs of the affected extremity are mandatory. For Iselin disease, the oblique view is critical; Hoerr et al. demonstrated that the fifth metatarsal epiphysis is visible on 99% of oblique radiographs in the target age group, whereas standard AP and lateral views often obscure the lesion due to bony overlap. Imaging typically reveals enlargement, widening of the cartilaginous-osseous junction, and occasionally fragmentation of the epiphysis.


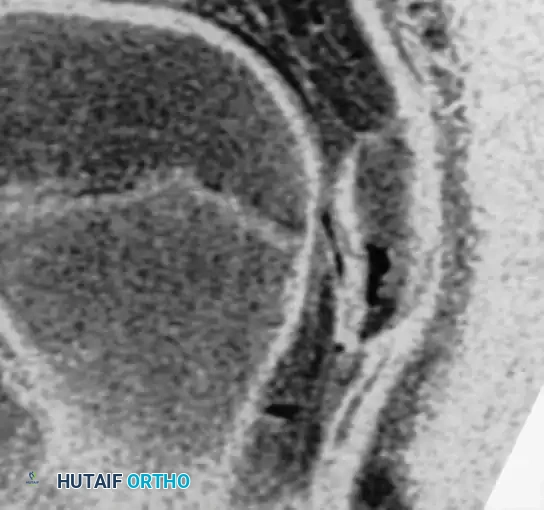
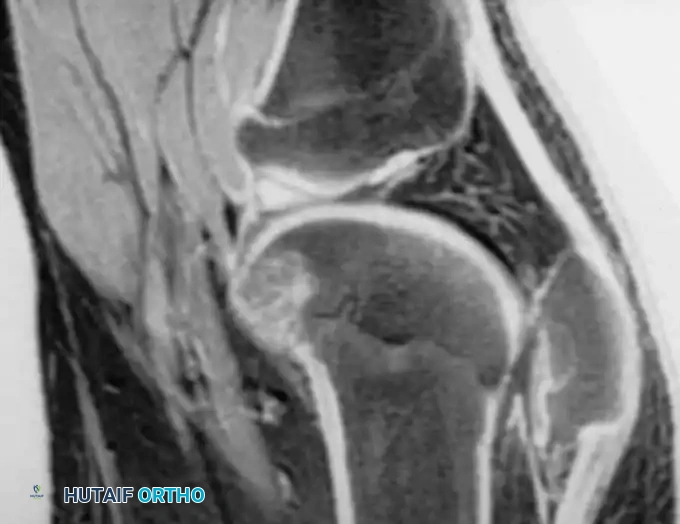
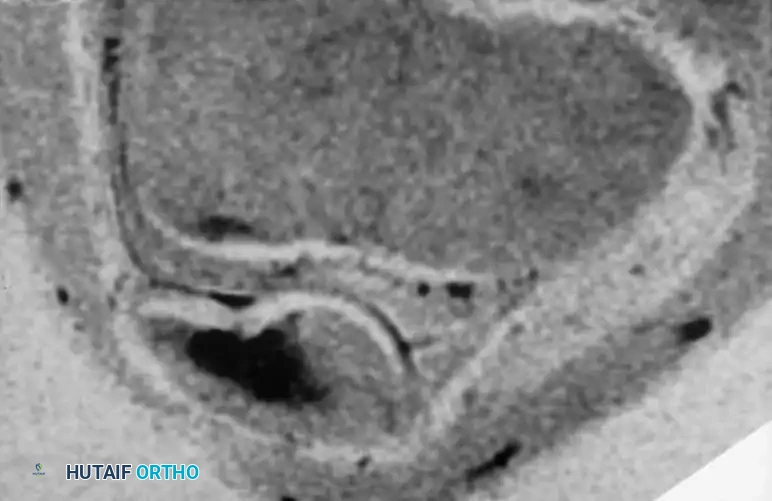
For Freiberg infraction and Talar Osteochondritis Dissecans (OCD), plain radiographs are often insufficient for definitive surgical planning. Magnetic Resonance Imaging (MRI) without contrast is the gold standard for evaluating the integrity of the overlying articular cartilage, the extent of subchondral edema, and the presence of cystic changes or loose bodies. In Freiberg infraction, MRI helps delineate the exact volume of the necrotic segment, which dictates the angle and depth of the planned dorsal closing wedge osteotomy.


When planning an arthrodesis for the late sequelae of Köhler disease, a fine-cut Computed Tomography (CT) scan with 3D reconstructions is highly recommended. The CT scan accurately defines the extent of degenerative changes across the talonavicular, naviculocuneiform, and calcaneocuboid joints. This allows the surgeon to template the exact size of the bone graft required to restore the medial column length and to select the appropriate low-profile plating systems or compression screws needed for rigid fixation.
Patient Positioning and Operating Room Setup
Optimal patient positioning is dictated by the specific anatomical lesion being addressed. For forefoot procedures such as the Freiberg dorsal wedge osteotomy or excision of a symptomatic Iselin non-union, the patient is positioned supine on a standard radiolucent operating table. An ipsilateral hip bump (using folded blankets or a specialized gel pad) is placed under the hemipelvis to internally rotate the lower extremity. This neutralizes the natural external rotation of the hip, presenting the dorsal midfoot and forefoot completely orthogonal to the surgeon, which is critical for accurate osteotomy execution.
A well-padded thigh tourniquet or a calf tourniquet is applied to ensure a bloodless surgical field, which is paramount when identifying delicate capsular structures and assessing cartilage viability. The C-arm fluoroscopy unit should be positioned on the contralateral side of the table, draped sterilely, and brought in perpendicular to the limb to allow for rapid intra-operative assessment of osteotomy angles, joint congruity, and hardware placement. For ankle arthroscopy and management of Talar OCD, the patient may be positioned supine with a non-invasive ankle distractor applied, or in the lateral decubitus position if a posterior approach is warranted for specific posterior lesions.
Step-by-Step Surgical Approach and Fixation Technique
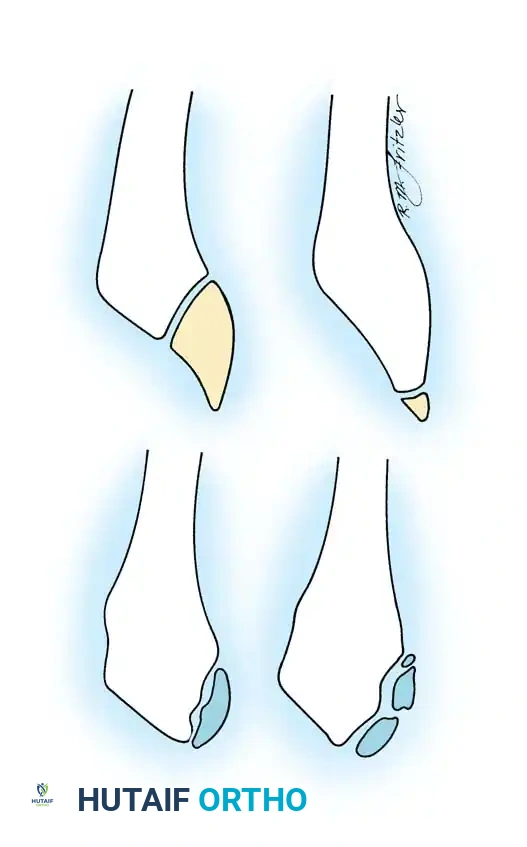
Dorsal Closing Wedge Osteotomy for Freiberg Infraction (Gauthier and Elbaz Technique)
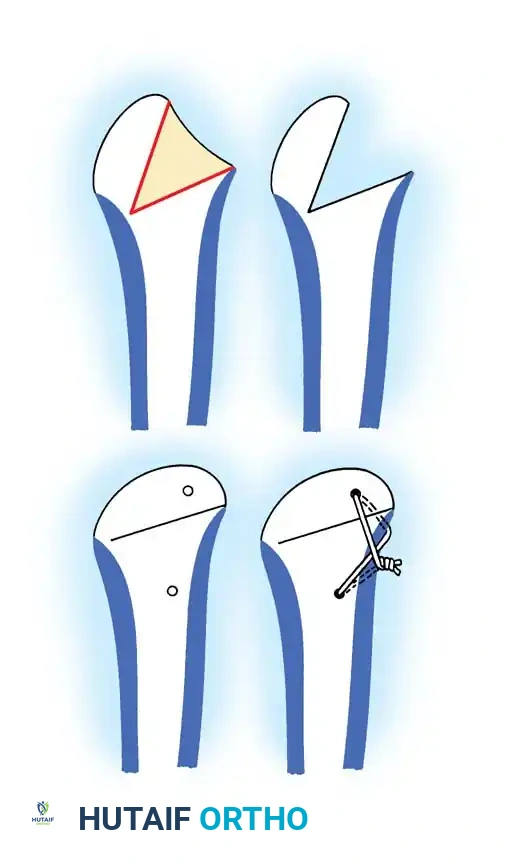
The dorsal closing wedge osteotomy remains the gold standard for symptomatic, deformed metatarsal heads in advanced Freiberg infraction. The primary biomechanical goal is to rotate the healthy, uninvolved plantar articular cartilage dorsally so that it articulates with the base of the proximal phalanx, effectively removing the necrotic dorsal lesion from the primary weight-bearing axis.
- Incision and Dissection: A 4-cm dorsal longitudinal incision is made centered directly over the affected metatarsophalangeal (MTP) joint. Careful blunt dissection is utilized to protect the dorsal cutaneous nerves. The extensor digitorum longus and brevis tendons are identified, mobilized, and retracted laterally using a Senn retractor to expose the dorsal joint capsule.
- Capsulotomy and Joint Debridement: A longitudinal dorsal capsulotomy is performed. The MTP joint is aggressively distracted and inspected. Hypertrophic, inflamed synovium is excised using a combination of a small rongeur and a motorized shaver. Any loose cartilaginous bodies or fragmented necrotic bone within the joint space are meticulously removed.
- Osteotomy Execution: The boundaries of the necrotic dorsal cartilage are identified. Using an oscillating microsaw under continuous saline irrigation to prevent thermal necrosis, a dorsal-based wedge of bone is resected from the metatarsal neck, immediately proximal to the articular surface. The distal cut is made parallel to the articular surface, while the proximal cut is angled to create a wedge that encompasses the entire necrotic dorsal lesion. The plantar cortex must be preserved to act as a stable hinge.
- Closure and Fixation: The osteotomy is carefully closed by applying a dorsiflexion force to the distal fragment. This rotates the healthy plantar cartilage into the functional joint space. The osteotomy is rigidly fixed using a 0.045-inch threaded Kirschner wire driven from dorsal-proximal to plantar-distal, or utilizing a low-profile 2.0mm titanium micro-screw for enhanced compression.
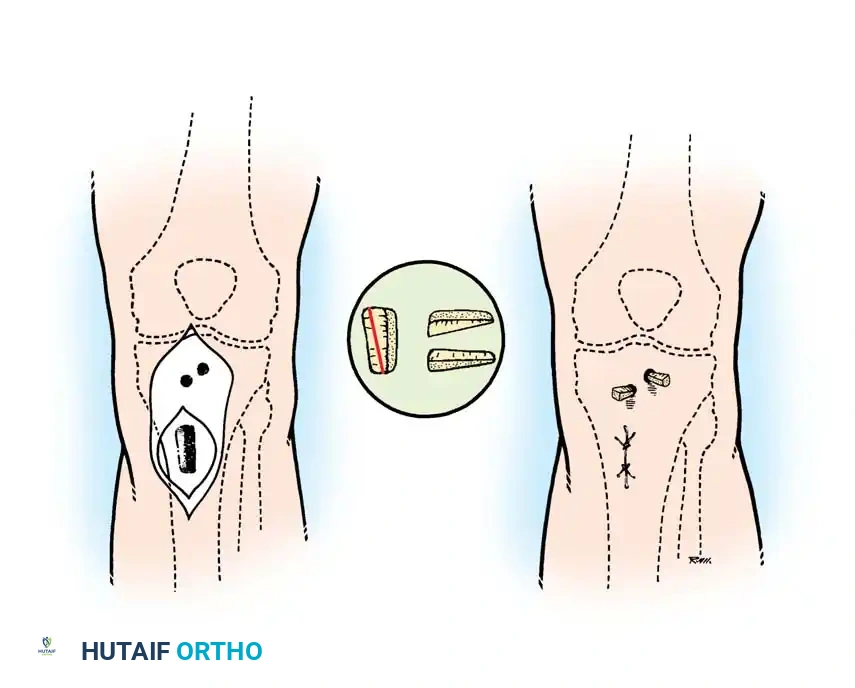
Midfoot Arthrodesis for Late Sequelae of Köhler Disease
When disabling midfoot arthrosis persists into adulthood due to severe navicular collapse, arthrodesis is required.
- Approach: A dorsal-medial or dorsal-lateral approach is utilized depending on the joints involved. For a combined talonavicular and calcaneocuboid fusion, a single extensile dorsal-lateral incision over the sinus tarsi extending distally provides excellent exposure.
- Joint Preparation: The sclerotic, degenerative articular cartilage of the talonavicular and calcaneocuboid joints is aggressively denuded down to bleeding, healthy subchondral bone using sharp curettes, osteotomes, and a high-speed burr. It is critical to penetrate the subchondral plate to expose the vascular cancellous bone, which is essential for fusion.
- Grafting and Fixation: Due to the severe sclerosis and potential bone loss from navicular collapse, autogenous cancellous bone graft—harvested from the proximal tibia or anterior iliac crest—is densely packed into the joint defects. The medial column is reduced to restore anatomical alignment. Rigid internal fixation is achieved using crossed 4.0mm or 4.5mm cannulated compression screws, or a specialized low-profile midfoot locking plate system.
Surgical Warning: Iselin Disease Misdiagnosis
A critical surgical warning must be highlighted regarding Iselin disease. It must be carefully distinguished from an acute Jones fracture (a transverse fracture at the metaphyseal-diaphyseal junction), a pseudo-Jones avulsion fracture (involving the tuberosity), and the presence of an Os vesalianum (an accessory sesamoid bone within the peroneus brevis tendon). Misdiagnosis of an inflamed apophysis as an acute fracture can lead to unnecessary, potentially harmful surgical internal fixation in a pediatric patient.
Complications, Incidence Rates, and Salvage Management
Surgical intervention for osteochondroses and epiphysitides, while often successful in relieving pain and restoring function, is not without significant risk. The unique vascular anatomy and immense biomechanical forces acting upon the foot and ankle make these procedures susceptible to specific complications.
In the management of Freiberg infraction via dorsal closing wedge osteotomy, the most devastating complication is the progression of avascular necrosis (AVN) of the metatarsal head, which occurs in approximately 5-10% of cases. This typically results from excessive stripping of the delicate capsular blood supply during the approach or thermal necrosis from the microsaw. If the metatarsal head undergoes complete ischemic collapse post-operatively, salvage management requires either a complete metatarsal head resection (arthroplasty) or an interpositional arthroplasty using an allograft or synthetic spacer. Additionally, malunion of the osteotomy in excessive dorsiflexion can lead to transfer metatarsalgia, where the weight-bearing load is abnormally shifted to the adjacent metatarsal heads, necessitating secondary corrective osteotomies or custom orthotic offloading.
Following midfoot arthrodesis for late-stage Köhler disease, non-union (pseudoarthrosis) is a major concern, with incidence rates reported between 10-15%, particularly at the notoriously difficult naviculocuneiform articulation. The dense, sclerotic nature of the previously ischemic navicular provides a poor biological environment for fusion. Salvage of a symptomatic midfoot non-union requires revision surgery with aggressive debridement of the pseudoarthrosis, massive structural autografting (often requiring an iliac crest tricortical graft to maintain column length), and revision hardware utilizing robust locking plates and prolonged non-weight-bearing immobilization.
For Talar OCD lesions treated with microfracture, the formation of mechanically inferior fibrocartilage (Type I collagen) rather than true hyaline cartilage (Type II collagen) can lead to early degradation and recurrent pain in up to 20-30% of large lesions (>1.5 cm). Salvage for failed microfracture involves more invasive cartilage restoration techniques, such as Osteochondral Autograft Transfer System (OATS) or Matrix-Induced Autologous Chondrocyte Implantation (MACI), which require malleolar osteotomies for access.
| Complication | Estimated Incidence | Primary Etiology | Salvage Management |
|---|---|---|---|
| Metatarsal Head AVN | 5-10% (Freiberg Osteotomy) | Vascular stripping; thermal necrosis; severe pre-op ischemia. | Metatarsal head resection; interpositional arthroplasty. |
| Transfer Metatarsalgia | 10-15% (Freiberg Osteotomy) | Malunion in excessive dorsiflexion; shortening of the ray. | Custom orthotics; adjacent Weil osteotomies. |
| Midfoot Non-union | 10-15% (Köhler Arthrodesis) | Sclerotic bone bed; inadequate fixation; smoking; non-compliance. | Revision arthrodesis with robust structural autograft and locking plates. |
| Hardware Prominence | 20-25% (General Foot/Ankle) | Thin dorsal soft tissue envelope; migration of K-wires. | Hardware removal after radiographic union is confirmed. |
| Recurrent Talar OCD Pain | 20-30% (Post-Microfracture) | Fibrocartilage degradation; unaddressed hindfoot malalignment. | OATS procedure; MACI; corrective calcaneal osteotomy. |
Phased Post-Operative Rehabilitation Protocols
The post-operative rehabilitation protocol must be meticulously phased and tailored to the specific surgical procedure performed, balancing the need for rigid tissue healing with the prevention of debilitating joint stiffness.
Phase I: Maximum Protection and Healing (Weeks 0-4)
Immediately following a Freiberg dorsal wedge osteotomy or a midfoot arthrodesis, the primary goal is the protection of the surgical construct and the mitigation of acute edema. The patient is placed in a well-padded, rigid short-leg splint or a bivalved cast in the operating room. Strict non-weight-bearing (NWB) status is enforced, utilizing crutches, a knee scooter, or a wheelchair. Elevation of the extremity strictly above the level of the heart is mandatory for the first 7-10 days to control swelling and prevent wound dehiscence, a common complication in the thin dorsal soft tissues of the foot. Deep vein thrombosis (DVT) prophylaxis is initiated based on patient risk factors. At the 2-week mark, sutures are removed, and the patient is transitioned to a rigid Controlled Ankle Motion (CAM) boot, but remains strictly NWB.
Phase II: Early Mobilization and Progressive Loading (Weeks 4-8)
At approximately 4 to 6 weeks post-operatively, serial radiographs are obtained to assess for early signs of trabecular bridging and hardware stability.
* For Freiberg Osteotomies: If the osteotomy demonstrates clinical stability and early radiographic union, the K-wire (if used and left protruding) is removed in the clinic. The patient may begin protected, partial weight-bearing in a stiff-soled post-operative shoe or CAM boot. Gentle, passive range of motion (ROM) exercises of the MTP joint are initiated to prevent capsular contracture, focusing on plantarflexion to stretch the dorsal capsule.
* For Midfoot Arthrodesis: The patient remains NWB in the CAM boot until a minimum of 6 to 8 weeks, given the longer healing time required for sclerotic midfoot fusions. Isometric strengthening of the intrinsic foot musculature and the triceps surae is initiated within the confines of the boot.
Phase III: Strengthening and Proprioception (Weeks 8-12)
Once definitive radiographic union is confirmed (typically 6-8 weeks for osteotomies, 8-12 weeks for fusions), the patient is gradually weaned from the CAM boot into a supportive, rigid-soled athletic shoe, often supplemented with a custom molded orthotic to support the transverse and medial longitudinal arches. Formal physical therapy is initiated. The focus shifts to aggressive active and passive ROM, intrinsic foot muscle strengthening (e.g., towel scrunches, marble pickups), and closed-kinetic chain exercises. Proprioceptive training using wobble boards and unstable surfaces is critical to retrain the mechanoreceptors disrupted during surgery.
Phase IV: Return to Sport and Advanced Activity (Weeks 12+)
Return to high-impact activities, running, and competitive sports is strictly prohibited until the patient demonstrates symmetrical lower extremity strength, pain-free full weight-bearing, and complete radiographic consolidation of the osteotomy or fusion mass. This typically occurs between 3 to 6 months post-operatively. Patients recovering from Freiberg osteotomies may require permanent modifications to their footwear, avoiding high heels or highly flexible minimalist shoes, to prevent recurrence of excessive stress across the lesser metatarsal heads.
Summary of Landmark Literature and Clinical Guidelines
The surgical management algorithms for osteochondrosis and epiphysitis are deeply rooted in several landmark anatomical and clinical studies that have shaped modern orthopedic guidelines.
Waugh's seminal anatomical studies on the vascularity of the pediatric tarsal navicular remain the bedrock of our understanding of Köhler disease. By demonstrating that the developing ossific nucleus is frequently supplied by a single, vulnerable central artery, Waugh provided the biomechanical and vascular rationale for why the navicular is so uniquely susceptible to ischemic collapse under compressive loads. This directly
Clinical & Radiographic Imaging Archive