Masterclass in Open Fractures: Surgical Management & Limb Salvage
Key Takeaway
Open fractures represent critical surgical emergencies requiring immediate, aggressive intervention. Successful management hinges on a multidisciplinary approach, prioritizing life preservation before limb salvage. This comprehensive guide details the evolution of open fracture care, from meticulous surgical debridement and targeted antibiotic prophylaxis to advanced stabilization techniques like intramedullary nailing. By understanding biofilm microbiology and utilizing validated severity scores, orthopedic surgeons can optimize functional outcomes and mitigate severe complications such as chronic osteomyelitis and amputation.
Comprehensive Introduction and Patho-Epidemiology
Open fractures are absolute surgical emergencies that, conceptually and practically, should be approached as incomplete amputations. The management of these complex, high-energy injuries has evolved significantly over the past century, a progression elegantly categorized by Tscherne into distinct eras of treatment. The first, or preantiseptic era, focused solely on life preservation and lasted well into the 20th century, where mortality from open long-bone fractures was staggeringly high. The second era, limb preservation, encompassed both World Wars; however, it was marred by a high incidence of amputations, which inadvertently spurred rapid advancements in artificial limb prosthetic designs but left a generation of young patients with profound physical disabilities.
The third era, lasting until the mid-1960s, shifted the paradigm toward infection avoidance through the advent and systematic use of systemic antibiotics. The fourth era—functional preservation—was characterized by aggressive, radical wound debridement, definitive fracture stabilization utilizing internal or external fixation, and the strategic use of delayed wound closure. Today, we operate within the fifth era: a product of rapid, high-value, multidisciplinary trauma care. Modern protocols dictate that these injuries be treated akin to battle wounds, requiring wide surgical exposure, meticulous excision of all devitalized soft tissues, immediate skeletal stabilization, and delayed primary or secondary closure dictated by the wound's physiological evolution.
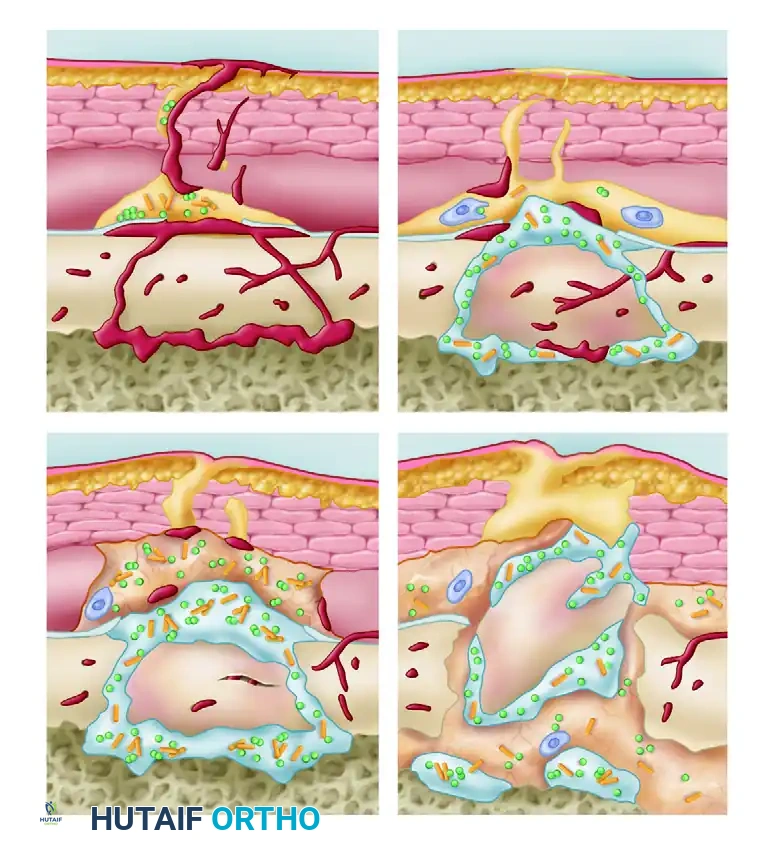
The treatment of an open fracture is fundamentally an exercise in applied microbiology and host-pathogen biomechanics. Once the protective skin barrier is breached, environmental and nosocomial bacteria infiltrate the wound, initiating a critical "race for the surface." The severity of the bacterial threat is directly proportional to the zone of injury. Extensive necrotic tissue provides a nutrient-rich substrate for bacterial proliferation, while localized ischemia severely compromises the host’s cellular and humoral immune responses. The disruption of the endosteal and periosteal blood supply creates an immunologically privileged environment for pathogens, rendering systemic antibiotics less effective at the exact site where they are needed most.
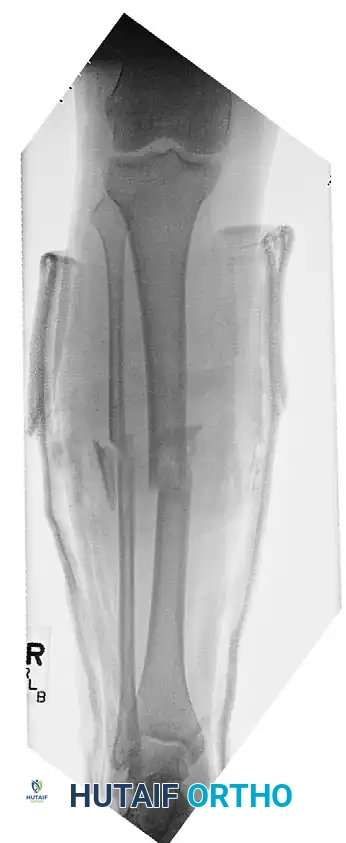
Epidemiologically, open fractures occur at an incidence of approximately 30 per 100,000 persons annually. The bimodal distribution mirrors that of general trauma: young males involved in high-energy mechanisms (such as motor vehicle collisions, motorcycle accidents, and industrial crush injuries) and elderly individuals sustaining low-energy falls resulting in open fragility fractures. The tibia is the most commonly involved long bone, owing to its precarious anteromedial subcutaneous position. The Gustilo-Anderson classification remains the universal language for describing these injuries, categorizing them from Type I (clean wound <1 cm) to Type IIIC (open fracture with an arterial injury requiring repair), directly correlating the severity of the soft tissue envelope disruption with the risk of deep infection and nonunion.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the surgical anatomy, specifically the soft tissue envelope and vascular supply, is paramount for the orthopedic trauma surgeon. The viability of a fractured bone is inextricably linked to its surrounding musculature and fascial attachments. In the lower extremity, the tibia is particularly vulnerable. Its anteromedial border is covered only by skin and subcutaneous tissue. The blood supply to the tibial diaphysis is dual-sourced: the nutrient artery (a branch of the posterior tibial artery) supplies the inner two-thirds of the cortex via the endosteal circulation, while the periosteal vessels supply the outer one-third. High-energy open fractures often obliterate the medullary canal and strip the periosteum, rendering the cortical bone completely avascular.
The biomechanics of open fractures are heavily influenced by the degree of soft tissue stripping and the energy imparted at the time of injury. According to Perren’s Strain Theory, fracture healing is dictated by the mechanical environment. In open fractures with massive bone loss or comminution, the strain across the fracture gap is often too high to support primary bone healing or even secondary callus formation without rigid stabilization. The loss of the soft tissue envelope removes the "biological chamber" necessary for hematoma retention and mesenchymal stem cell recruitment, shifting the biomechanical burden entirely onto the chosen orthopedic implant.
The Microbiology and Biomechanics of Biofilm Formation
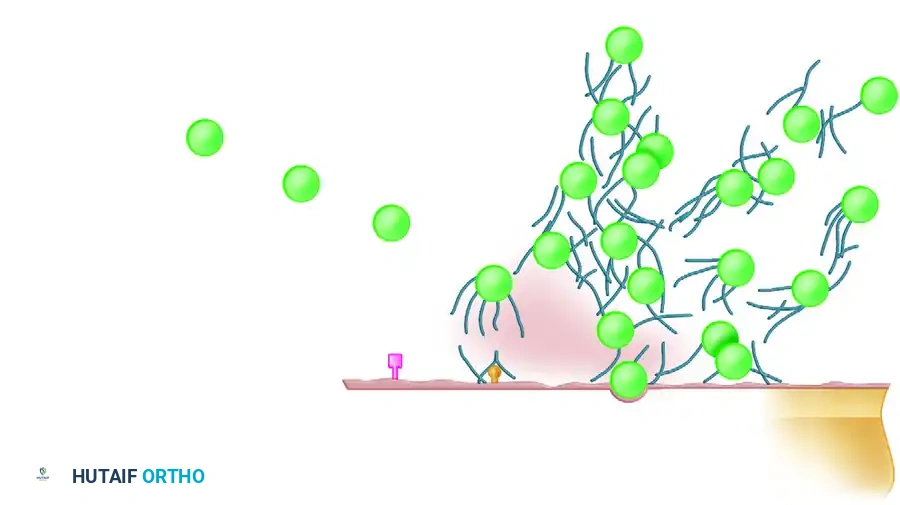
The virulence of the infecting organism in an open fracture is dictated by its capacity to adhere to host substrates (necrotic skin, fascia, devitalized muscle, and avascular bone), its intrinsic pathogenicity, and its ability to neutralize host defenses. At specific microscopic distances, the initial repelling forces of negative bacterial and substrate surface charges are overcome by attracting van der Waals forces and hydrophobic interactions.
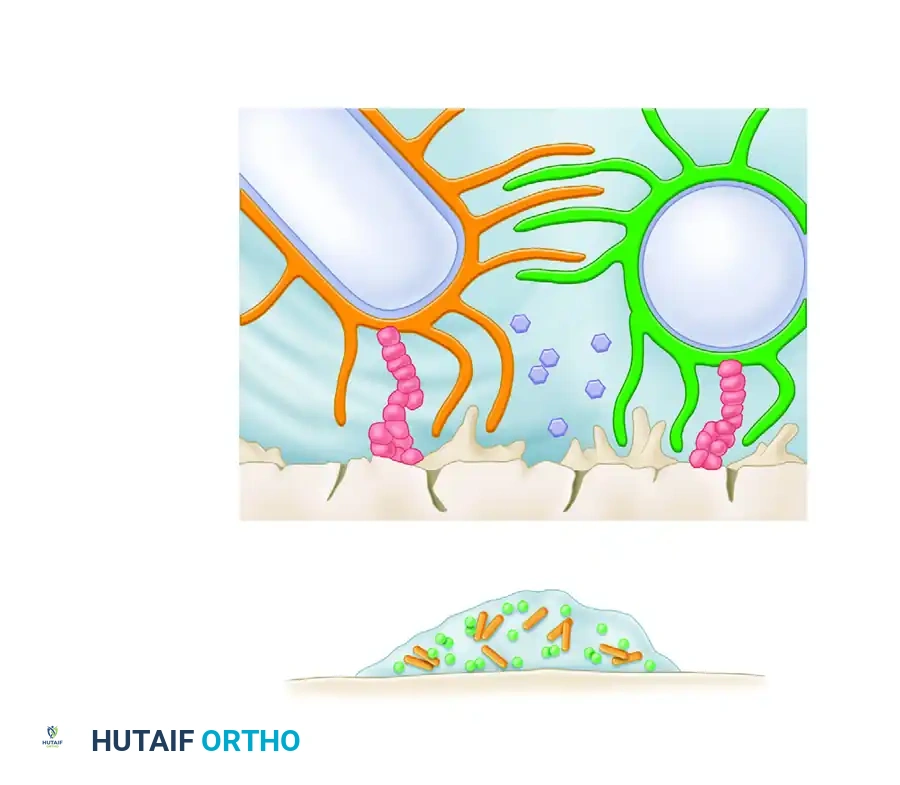
Once bacteria successfully adhere to the host cellular substrate or implanted orthopedic hardware, they secrete an exopolysaccharide polymer—a glycoprotein shield known as a biofilm. This glycocalyx protects the bacterial colony from phagocytic white blood cells and systemic antibiotics. The foreign body reaction is now recognized as a complex interaction driven by this bacterial glycoprotein shield. Once the biofilm is established, bacteria proceed with logarithmic cell replication, altering their metabolic state to become highly resistant sessile organisms. If the host survives the initial physiological insult, the bacteria will either be eradicated by surgical and medical intervention or suppressed and isolated, inevitably leading to chronic osteomyelitis.
Biomechanics of Ballistic Trauma
Gunshot wounds present unique biomechanical and physiological challenges based on the velocity and caliber of the projectile. The kinetic energy ($KE$) transferred to the tissue is calculated by the formula $KE = 1/2 mv^2$. Because velocity is squared, high-velocity weapons impart exponentially more energy than low-velocity weapons. Low-velocity handgun injuries often cause minimal soft tissue disruption, creating a permanent cavity roughly the size of the projectile, and can frequently be managed with local wound care and standard fracture fixation protocols.

Conversely, high-velocity rifle wounds impart massive kinetic energy, creating temporary cavitation that destroys tissue far beyond the permanent bullet tract. This cavitation stretches and tears microvasculature, leading to widespread muscle necrosis that may not be immediately apparent upon initial inspection. These injuries require extensive surgical exploration, radical debridement, and often serial excisions.

Exhaustive Indications and Contraindications
The advent of sophisticated microsurgical and fixation protocols has enabled the salvage of severely traumatized extremities. However, this has introduced a profound clinical dilemma: the creation of salvaged but entirely nonfunctional limbs. Surgeons must guard against the philosophy of "technique over reason." Delaying an inevitable amputation results in exponentially increased financial, personal, and social costs, alongside severe attendant morbidity and potential mortality. Studies consistently show that patients undergoing prolonged, unsuccessful limb salvage experience more complications, longer hospital stays, and higher rates of psychological disability compared to those who undergo early, definitive below-knee amputations.
To objectify the amputation decision, several scoring systems have been developed. The Mangled Extremity Severity Score (MESS) evaluates skeletal/soft tissue injury, shock, ischemia, and patient age. Historically, a MESS score of 7 or greater was highly predictive of amputation. However, recent validations reveal that while the specificity of MESS is high (low scores reliably predict salvage), its sensitivity is low, meaning it cannot be used as the sole criterion for amputation. For Gustilo Type IIIA and IIIB open tibial fractures, Rajasekaran’s scoring system evaluates covering structures, skeletal structures, functional tissues, and comorbid conditions. A score of 14 or greater demonstrated a positive predictive value of 100% for amputation. Despite these metrics, clinical judgment remains paramount.
| Clinical Scenario / Parameter | Indications for Limb Salvage | Indications for Primary Amputation (Contraindications to Salvage) |
|---|---|---|
| Hemodynamic Status | Stable patient, responsive to initial fluid resuscitation; isolated extremity trauma. | Hemodynamically unstable polytrauma patient (in extremis) where prolonged surgery threatens life. |
| Neurological Status | Intact plantar sensation; partial nerve injuries with potential for grafting or tendon transfer. | Complete, anatomically verified transection of the tibial/sciatic nerve with massive soft tissue loss. |
| Vascular Injury (Type IIIC) | Ischemia time < 6 hours; single vessel injury with good distal runoff and reconstructable soft tissue. | Warm ischemia time > 8 hours; irreparable vascular crush injury; unsalvageable distal capillary bed. |
| Soft Tissue Envelope | Gustilo Type I, II, IIIA; Type IIIB amenable to local or free flap coverage within 5-7 days. | Massive crush injury with complete loss of functional muscle compartments; severe contamination. |
| Bone Loss | Minimal to moderate bone loss amenable to acute shortening, bone transport (Ilizarov), or grafting. | Segmental bone loss > 10-15 cm combined with massive soft tissue loss and nerve injury. |
| Patient Factors | Young, healthy, compliant patient with strong psychosocial support and desire for salvage. | Elderly patient with severe medical comorbidities (e.g., severe peripheral vascular disease, uncontrolled diabetes). |
Pre-Operative Planning, Templating, and Patient Positioning
The management of an open fracture begins in the trauma bay, adhering strictly to Advanced Trauma Life Support (ATLS) principles. Life-threatening injuries must be addressed prior to focusing on the extremity. Once the patient is stabilized, a meticulous secondary survey is conducted. The open wound is photographed to prevent repeated dressing takedowns, gross contamination is gently removed, and the limb is splinted in anatomical alignment to restore gross vascular flow and minimize further soft tissue trauma.
A landmark 2004 Cochrane systematic review unequivocally confirmed the critical benefit of early antibiotic administration in open fracture management, demonstrating a 59% reduction in the risk of infection. Current evidence supports a short course of first-generation cephalosporins (e.g., Cefazolin), initiated as rapidly as possible following the injury. For Type III injuries, expanded gram-negative coverage (e.g., Gentamicin or Ceftriaxone) is added. In farm injuries or cases with heavy soil contamination, high-dose Penicillin is administered for Clostridium prophylaxis. Tetanus status must be verified and updated accordingly. Notably, the evidence does not support prolonged courses of antibiotics beyond 48-72 hours post-debridement, which only serve to select for resistant organisms.
Pre-operative imaging must include orthogonal radiographs of the injured extremity, encompassing the joints above and below the fracture. In high-energy trauma, a CT scan of the extremity may be warranted to evaluate intra-articular extension. If vascular compromise is suspected (diminished pulses, abnormal Ankle-Brachial Index < 0.9), a CT angiogram is mandatory, provided it does not delay urgent surgical revascularization. Templating is performed to anticipate the size and type of fixation required, whether it be an intramedullary nail, bridging plate, or external fixator components.
Patient positioning in the operating room must facilitate wide surgical exposure, intraoperative fluoroscopy, and potential access for vascular repair or soft tissue harvesting. The patient is typically placed supine on a radiolucent flat Jackson table. The entire limb must be prepped and draped free, often extending to the iliac crest for lower extremity injuries to allow for proximal control or bone graft harvesting. A sterile tourniquet may be placed proximally but should remain uninflated unless catastrophic hemorrhage occurs, as assessing tissue viability requires observing active bleeding during debridement.
Step-by-Step Surgical Approach and Fixation Technique
Principles of Radical Debridement
The cornerstone of open fracture management is meticulous, radical debridement. The procedure begins with a generous longitudinal extension of the traumatic wound, incorporating the original laceration into a standard surgical approach. This allows full visualization of the zone of injury. The debridement proceeds systematically from superficial to deep: skin, subcutaneous fat, fascia, muscle, and finally bone. All devitalized muscle must be aggressively excised. Muscle viability is assessed by the classic "4 Cs": Color (beefy red is viable, dark/pale is not), Consistency (firm and elastic vs. mushy), Contractility (responds to electrocautery or mechanical pinch), and Capacity to bleed.
Unattached cortical bone fragments without soft tissue attachments must be removed, as they will act as necrotic sequestra and harbor biofilm. However, large articular fragments, even if devoid of soft tissue, are often retained, meticulously cleaned, and fixed to preserve joint congruity. Following debridement, the wound undergoes copious irrigation. The FLOW (Fluid Lavage of Open Wounds) trial demonstrated that low-pressure gravity lavage with normal saline is as effective as high-pressure pulsatile lavage and is associated with less soft tissue damage and a lower risk of driving debris deeper into the tissue planes.
Management of Severe Tibial Fractures with Vascular Injury
Open Type IIIB and IIIC tibial fractures represent the zenith of orthopedic trauma complexity. In cases involving arterial injury (Type IIIC), a coordinated approach with vascular surgery is mandatory. The sequence of fixation versus vascular repair is a critical intraoperative decision.

If the limb is profoundly ischemic, a temporary intravascular shunt (e.g., Argyle shunt) is placed rapidly by the vascular surgeon to restore perfusion. The orthopedic surgeon then achieves rapid skeletal stabilization—typically using a spanning external fixator or, in select cases, an intramedullary nail. Once the bone is stabilized, the vascular surgeon returns to perform the definitive autogenous vein interposition graft. Data indicates that no disruption of vascular anastomoses occurs in patients where vascular repair precedes fracture fixation, provided the orthopedic surgeon exercises extreme care; however, the shunt-first approach minimizes warm ischemia time and is generally preferred in complex trauma.

Fracture Stabilization Strategies
The timing and technique of intramedullary (IM) nailing in open fractures have been subjects of extensive academic debate. Current evidence strongly supports the use of statically locked, reamed intramedullary nailing as the preferred treatment for most low-velocity and mid-velocity femoral and tibial shaft fractures. The SPRINT trial demonstrated that reamed nailing of open tibial fractures is safe and may reduce the need for secondary bone grafting procedures compared to unreamed nailing. Immediate reamed interlocked nailing of femoral fractures caused by gunshots has been shown to result in shorter hospital stays, significantly decreased hospital expenses, and no detrimental effects on clinical outcomes or infection rates compared to delayed nailing.

For high-velocity fractures with massive contamination, or in polytraumatized patients exhibiting the "lethal triad" (coagulopathy, hypothermia, acidosis), Damage Control Orthopedics (DCO) principles apply. The fracture is temporarily stabilized with a spanning external fixator. Pins must be placed outside the zone of injury and future definitive surgical incisions. Once the soft tissue envelope recovers and the patient’s physiology normalizes, conversion to definitive internal fixation is typically performed within 2 weeks post-injury to minimize the risk of pin-tract colonization leading to deep infection. For severe Gustilo Type III injuries where the soft tissue envelope precludes internal fixation indefinitely, advanced techniques such as Ilizarov circular ring fixation combined with delayed primary closure or rotational/free tissue transfer yield exceptionally low overall complication rates.
Complications, Incidence Rates, and Salvage Management
Despite optimal surgical management, open fractures carry a high burden of complications. The disruption of the soft tissue envelope, combined with initial bacterial inoculation, sets the stage for both early and late catastrophic failures. Deep infection and osteomyelitis are the most feared complications. The incidence of deep infection correlates directly with the Gustilo-Anderson grade: Type I (0-2%), Type II (2-7%), Type IIIA (7-15%), and Type IIIB/C (10-50%). When infection occurs, it manifests as purulent drainage, increasing pain, or systemic sepsis. Management requires a return to the operating room for radical excision of infected bone and soft tissue, removal of loose hardware, and placement of local antibiotic delivery systems (e.g., PMMA antibiotic beads or cement spacers).
Nonunion is another frequent complication, occurring in up to 30% of severe open tibial fractures. Nonunions can be aseptic (due to avascularity and mechanical instability) or septic. Differentiating between the two is critical, as the treatment algorithms diverge completely. Aseptic nonunions may be treated with dynamization of the IM nail, exchange nailing, or autologous bone grafting. Septic nonunions require a staged approach: eradication of the infection first (often utilizing the induced membrane technique of Masquelet), followed by definitive bone reconstruction.
| Complication | Estimated Incidence | Pathophysiology & Risk Factors | Salvage Management Strategy |
|---|---|---|---|
| Deep Infection / Osteomyelitis | 2% (Type I) to >30% (Type IIIB/C) | Biofilm formation on necrotic bone or hardware; inadequate initial debridement; delayed soft tissue coverage. | Radical repeat debridement, hardware removal (if loose), local antibiotic spacers, systemic IV antibiotics, delayed reconstruction. |
| Aseptic Nonunion | 10% - 25% | Periosteal stripping, endosteal ischemia, inadequate mechanical stability, smoking, NSAID use. | Exchange nailing (larger diameter), dynamization, autologous iliac crest bone grafting, or bone morphogenetic protein (BMP) application. |
| Septic Nonunion | 5% - 15% | Persistent bacterial colonization preventing osteogenesis; chronic inflammatory state. | Staged Masquelet technique: Stage 1 (debridement + antibiotic cement spacer), Stage 2 (spacer removal + massive bone grafting 6-8 weeks later). |
| Flap Failure / Soft Tissue Necrosis | 5% - 10% | Venous congestion, arterial thrombosis in free flaps; excessive tension in delayed primary closures. | Immediate return to OR for microvascular exploration; if unsalvageable, debridement and alternative coverage (e.g., cross-leg flap) or amputation. |
| Lead Toxicity (GSW) | Rare, but severe | Retained intra-articular lead fragments undergoing dissolution by synovial fluid. | Absolute indication for arthrotomy and removal of intra-articular lead fragments to prevent systemic plumbism and severe synovitis. |
Phased Post-Operative Rehabilitation Protocols
Rehabilitation following the surgical management of an open fracture is a protracted, highly individualized process that requires constant communication between the orthopedic surgeon, physical therapist, and patient. The rehabilitation protocol must be tailored to the stability of the skeletal fixation and the integrity of the soft tissue reconstruction.
Phase I: Immediate Post-Operative (Weeks 0-2)
Following aggressive debridement and skeletal stabilization, the wound is typically managed with negative pressure wound therapy (NPWT) or sterile non-adherent dressings. A planned "second look" debridement is mandatory at 48 to 72 hours. Definitive soft tissue coverage—whether via delayed primary closure, split-thickness skin grafting, local rotational flaps (e.g., gastrocnemius flap for proximal tibia), or free tissue transfer—should ideally be achieved within 5 to 7 days. During this phase, the limb is elevated to control edema. Joint mobilization is generally restricted if it places tension on a fresh flap or skin graft. Deep vein thrombosis (DVT) prophylaxis is strictly enforced.
Phase II: Early Mobilization and Tissue Healing (Weeks 2-6)
Once the soft tissue envelope is secure and sutures/staples are removed, early range of motion (ROM) of adjacent joints is aggressively encouraged to prevent arthrofibrosis, a common sequela of prolonged immobilization and soft tissue scarring. Weight-bearing status is dictated by the fracture pattern and the biomechanical properties of the chosen implant. For statically locked IM nails in length-stable fractures, partial to full weight-bearing may be permitted. For fractures managed with external fixators or plates with significant comminution, patients are typically restricted to touch-down weight-bearing (TDWB).
Phase III: Strengthening and Functional Restoration (Weeks 6-12+)
Regular clinical and radiographic surveillance is required to monitor for the insidious onset of chronic osteomyelitis or delayed union. As radiographic callus appears, weight-bearing is progressively advanced. Physical therapy shifts focus toward progressive resistance exercises, gait retraining, and proprioceptive recovery. For patients who underwent limb salvage, chronic pain and stiffness are common; therefore, setting realistic expectations is crucial. If the patient underwent an amputation, this phase focuses on residual limb desensitization, prosthetic socket fitting, and intensive gait training to maximize functional independence.
Summary of Landmark Literature and Clinical Guidelines
The modern management of open fractures is heavily guided by several landmark prospective trials and systematic reviews that have fundamentally altered orthopedic trauma protocols.
The Lower Extremity Assessment Project (LEAP) study was a monumental multicenter prospective study evaluating severe lower extremity trauma. It profoundly impacted the amputation versus salvage debate by demonstrating that at two and seven years post-injury, there was no significant difference in functional outcomes (using the Sickness Impact Profile) between patients who underwent early amputation and those who underwent successful limb salvage. However, limb salvage patients required significantly more secondary surgical procedures and experienced higher rates of rehospitalization. This study underscored that a salvaged limb does not equate to a normal limb, heavily influencing modern patient counseling.
The FLOW (Fluid Lavage of Open Wounds) Trial challenged the long-held dogma that high-pressure pulsatile lavage was superior for wound decontamination. This randomized controlled trial demonstrated that low-pressure gravity lavage with normal saline was not only non-inferior to high-pressure lavage regarding infection and reoperation rates, but it was also significantly more cost-effective. Furthermore, the addition of castile soap to the irrigation fluid offered no benefit over normal saline.
The SPRINT (Study to Prospectively Evaluate Reamed Intramedullary Nails in Patients with Tibial Fractures) trial provided definitive guidance on IM nailing techniques. It concluded that reamed intramedullary nailing of closed tibial fractures significantly reduced the risk of nonunion compared to unreamed nailing. For open fractures, reamed nailing was deemed safe, refuting earlier concerns that reaming would destroy the remaining endosteal blood supply and precipitate massive osteonecrosis and infection.
Finally, the 2004 Cochrane Systematic Review on antibiotic prophylaxis in open fractures remains the gold standard guideline. It unequivocally established that the early administration of systemic antibiotics reduces the risk of early infection by nearly 60%. This review solidified the protocol that antibiotics must be administered in the trauma bay as soon as intravenous access is established, shifting the paradigm from viewing antibiotics as a post-operative adjunct to a critical pre-operative resuscitative measure.
📚 Medical References
