Upper Extremity Escharotomy: Comprehensive Surgical Techniques and Protocols
Key Takeaway
Escharotomy is a limb-saving surgical procedure indicated for circumferential full-thickness burns that compromise distal perfusion. The unyielding eschar, combined with massive fluid resuscitation and capillary leak, elevates interstitial pressures, leading to burn-induced compartment syndrome. Timely midaxial incisions along the forearm, hand, and digits release this constricting tissue, restoring arterial flow and preventing irreversible ischemic necrosis, nerve damage, and subsequent amputation.
Comprehensive Introduction and Patho-Epidemiology
Severe thermal, electrical, and chemical injuries to the upper extremity, particularly deep partial-thickness and full-thickness circumferential burns, present a profound and immediate threat to limb viability. The thermal destruction of the dermis and underlying subcutaneous architecture results in a rigid, inelastic, and unyielding layer of coagulated, dead tissue known as an eschar. Concurrently, the systemic inflammatory response syndrome (SIRS) triggered by severe burns induces a massive capillary leak syndrome. As the patient undergoes aggressive, life-saving intravenous fluid resuscitation—classically guided by the Parkland or Brooke formulas—protein-rich plasma extravasates into the interstitial space, causing profound, rapidly progressive tissue edema.
When this rapidly expanding interstitial edema is constrained by the rigid, non-compliant eschar, interstitial hydrostatic pressure rises exponentially within the closed fascial and cutaneous compartments. The pathophysiology is governed by Starling’s forces; thermal injury causes direct microvascular thrombosis and the massive local release of vasoactive mediators, including histamine, bradykinin, prostaglandins, and reactive oxygen species. Once the interstitial pressure surpasses the capillary perfusion pressure, microvascular collapse occurs, initiating a devastating ischemic cascade. This phenomenon is clinically recognized as burn-induced compartment syndrome. If left unrecognized and untreated, it rapidly progresses to irreversible myonecrosis, ischemic nerve damage, rhabdomyolysis, and ultimately, the need for major limb amputation.
Epidemiologically, the upper extremity is disproportionately affected in severe burn injuries due to the reflexive use of the arms and hands to shield the face and torso during a fire or explosion. Studies indicate that up to 40% of patients with total body surface area (TBSA) burns exceeding 20% will require at least one escharotomy, with the upper extremities being the most frequent surgical site. The incidence of burn-induced compartment syndrome correlates directly with the depth of the burn, the circumferential nature of the injury, and the volume of crystalloid resuscitation administered during the first 24 hours post-injury. The critical window for intervention is exceedingly narrow; irreversible muscle necrosis can begin within four to six hours of complete microvascular collapse.
Escharotomy—the surgical incision through the eschar to release the underlying tension—is a critical, time-sensitive, limb-saving intervention. It restores distal perfusion, mitigates the ischemic cascade, and preserves the functional integrity of the upper extremity. As orthopedic surgeons, our mandate is not merely the preservation of the limb, but the optimization of its complex biomechanical function. The execution of a technically precise escharotomy is the foundational step in a long continuum of surgical and rehabilitative care that dictates the ultimate functional outcome for the burn survivor.
Detailed Surgical Anatomy and Biomechanics
Understanding the intricate surgical anatomy and the altered biomechanics of burn edema is essential for the orthopedic surgeon managing the burned upper extremity. In a normal physiological state, the fascial compartments and the elastic properties of the dermis can accommodate mild to moderate fluid shifts. However, a full-thickness burn obliterates this elasticity. The eschar acts as a biological tourniquet. The upper extremity is anatomically subdivided into distinct fascial compartments, each harboring critical neurovascular structures that are highly susceptible to compression ischemia.
The arm contains two primary compartments: the anterior (flexor) compartment, housing the biceps brachii, brachialis, and coracobrachialis muscles along with the brachial artery and median nerve; and the posterior (extensor) compartment, containing the triceps brachii and the radial nerve. The forearm is more complex, comprising the volar (flexor/pronator) compartment, the dorsal (extensor) compartment, and the mobile wad of Henry. The volar compartment is further subdivided into superficial and deep spaces, with the deep space being particularly vulnerable to elevated pressures that can lead to Volkmann's ischemic contracture. The hand contains ten distinct fascial compartments: four dorsal interosseous, three volar interosseous, the thenar, the hypothenar, and the adductor pollicis compartments. The digits, while lacking true muscle bellies, possess tight fascial sleeves containing the digital neurovascular bundles that are highly susceptible to compression.
Biomechanically, the expansion of tissue volume within these non-compliant spaces alters the pressure gradient required for cellular perfusion. Capillary blood flow is typically compromised when tissue pressure exceeds 30 mm Hg, or when the difference between diastolic blood pressure and compartment pressure (ΔP) falls below 30 mm Hg. In the burned upper extremity, this threshold can be reached within hours of the initial injury, exacerbated by the massive fluid shifts of burn shock resuscitation. The venous system, being a low-pressure network, collapses first, leading to venous congestion and a further increase in hydrostatic pressure, which subsequently halts arterial inflow.
Surgical anatomy dictates the precise placement of escharotomy incisions to avoid iatrogenic injury. The mid-axial lines of the arm, forearm, and digits are the preferred routes for incision. These lines represent the safest internervous and intervascular planes. Deviations from these precise anatomical landmarks risk catastrophic injury to superficial nerves, such as the superficial sensory branch of the radial nerve at the wrist, the ulnar nerve at the cubital tunnel, and the proper volar digital nerves in the hand. Furthermore, the extensor mechanisms of the hand and digits are covered by exceptionally thin integument; imprecise incisions here can expose the paratenon, leading to rapid desiccation, tendon rupture, and severe functional deficits.
Exhaustive Indications and Contraindications
The decision to perform an upper extremity escharotomy is primarily clinical, necessitating a high index of suspicion, continuous serial examinations, and the judicious use of objective vascular assessment modalities. The classic "6 Ps" of compartment syndrome (Pain, Pallor, Pulselessness, Paresthesia, Paralysis, and Poikilothermia) are notoriously unreliable and often present too late in the burn patient. Pain is frequently masked by the burn itself, systemic analgesia, or intubation; pallor and poikilothermia are obscured by the charred eschar; and pulselessness is a late, often irreversible sign of profound ischemia.
Objective assessment modalities are therefore mandatory. Doppler ultrasonography is the gold standard for non-invasive bedside assessment. The absence or progressive diminution of pulsatile flow in the radial, ulnar, and palmar arch arteries, or the digital vessels, is a definitive indication for immediate escharotomy. Compartment pressure monitoring via solid-state transducer or slit-catheter technique provides definitive data; pressures exceeding 30 mm Hg, or a ΔP of less than 30 mm Hg, mandate surgical release. Pulse oximetry and near-infrared spectroscopy (NIRS) can serve as adjuncts, though peripheral vasoconstriction and carbon monoxide poisoning can confound plethysmographic waveforms.
Contraindications to escharotomy are exceedingly rare given the limb-threatening nature of the pathology, but they must be understood to avoid unnecessary surgical morbidity. Absolute contraindications include limbs with established, irreversible necrosis where amputation is the only viable option, or superficial partial-thickness burns that remain supple and do not compromise perfusion. Relative contraindications involve severe, uncorrectable coagulopathy, though in the face of acute limb ischemia, the release must proceed with concurrent aggressive blood product resuscitation.
| Category | Indications / Clinical Scenarios | Contraindications / Cautions |
|---|---|---|
| Clinical Findings | Progressive loss of sensation or motor function; tense, woody palpation of compartments; disproportionate pain on passive stretch. | Supple, compressible soft tissues; superficial first-degree burns; isolated non-circumferential burns without edema. |
| Objective Vascular | Absence or progressive loss of Doppler signals in radial, ulnar, palmar, or digital arteries; absent capillary refill. | Normal, triphasic Doppler signals; robust capillary refill (<2 seconds); normal digital pulse oximetry plethysmography. |
| Pressure Metrics | Absolute compartment pressure > 30 mm Hg; Delta P (Diastolic BP - Compartment Pressure) < 30 mm Hg. | Normal compartment pressures (< 15 mm Hg); Delta P > 30 mm Hg with stable clinical exam. |
| Systemic Factors | Massive fluid resuscitation (>250cc/hr) in circumferential burns; delayed presentation with impending ischemia. | Irreversible limb necrosis (demarcated gangrene); unsurvivable total body trauma (palliative care pathway). |
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning for an upper extremity escharotomy begins immediately upon the patient's arrival at the burn center or trauma bay. Because these procedures are frequently performed emergently, the orthopedic surgeon must be adept at executing the release either in the controlled environment of the operating theater or at the bedside in the Burn Intensive Care Unit (BICU). "Templating" in the context of escharotomy refers to the meticulous pre-operative mapping and marking of the incision lines using a sterile surgical marker to ensure adherence to the mid-axial safe zones, preventing erratic incisions that could jeopardize neurovascular structures.
Hemodynamic and hematologic preparation is paramount. The systemic derangements of severe burn injury include a profound coagulopathy characterized by early hypercoagulability followed by consumptive coagulopathy and dilutional thrombocytopenia. The surgeon must prepare the patient preoperatively for potential massive blood transfusion. While the eschar itself is avascular and insensate, the incisions will inevitably traverse into the hyperemic, viable subcutaneous tissues and potentially the muscle fascia, leading to significant, rapid blood loss. A current type and crossmatch must be verified, and massive transfusion protocols should be on standby. Hypothermia is a critical risk in burn patients; the ambient room temperature must be elevated, and forced-air warming blankets applied to unburned areas.
Anesthesia and patient positioning require careful coordination with the critical care and anesthesia teams. With the patient supine, the procedure is optimally performed under general anesthesia to ensure patient comfort and immobility. However, in critically unstable, mechanically ventilated patients, bedside escharotomy may be performed with intravenous sedation, utilizing the fact that full-thickness eschar is inherently insensate. The upper extremity is positioned extended and abducted to 90 degrees on a radiolucent hand table. This position provides circumferential access to the limb and facilitates precise anatomical orientation.
The entire extremity must be thoroughly cleansed with an approved surgical antiseptic, such as chlorhexidine gluconate or povidone-iodine, taking care not to aggressively debride the eschar prematurely, which could induce bleeding. Sterile draping is applied to expose the limb completely from the axilla to the fingertips. The surgical armamentarium should include a high-frequency electrocautery device with a needle-tip electrode, sterile Doppler ultrasound probes, solid-state compartment pressure monitors, and a standard soft-tissue orthopedic tray in the event that the procedure must be converted to a formal deep fasciotomy.
Step-by-Step Surgical Approach and Fixation Technique
The fundamental goal of an escharotomy is to completely release the constricting eschar from the level of unburned, healthy tissue proximally to healthy tissue distally. The incisions must be carried down through the eschar and the superficial fascia, allowing the wound edges to separate widely, thereby decompressing the subcutaneous space. While "fixation" traditionally implies osseous stabilization, in the context of severe upper extremity burns, "fixation technique" refers to the securement of the soft tissue envelope, the potential use of temporary transarticular Kirschner wires to maintain the intrinsic-plus position against severe burn contracture forces, and the definitive graft fixation.
Arm and Forearm Escharotomy
The procedure commences with the mapping of the medial and lateral mid-axial longitudinal incisions. The mid-axial lines are specifically chosen to avoid injury to the major superficial veins (the cephalic vein laterally and the basilic vein medially) and the primary flexor and extensor tendon groups. Utilizing an electrocautery device set to a pure cutting or blend current, the surgeon incises the eschar. Electrocautery is vastly preferred over a cold scalpel to minimize blood loss in the hyperemic subcutaneous layer.
As the incision approaches the elbow, a critical anatomical transition occurs. A straight medial mid-axial incision at the elbow risks catastrophic iatrogenic transection of the ulnar nerve as it passes superficially through the cubital tunnel. Therefore, the medial incision must be routed anterior to the medial epicondyle. Once past the elbow, the incision returns to the mid-axial line of the forearm. The distal extension of these incisions must stop precisely at the level of the metacarpophalangeal (MCP) joints to avoid exposing the delicate joint capsules or the extensor mechanisms.
Transition to Fasciotomy
Escharotomy effectively releases the cutaneous envelope, but it does not release the deep fascial compartments. Following the escharotomy, the surgeon must reassess the muscle compartments. If the compartments remain tense to palpation, or if intracompartmental pressures remain elevated above 30 mm Hg, a formal fasciotomy must be performed immediately. This involves extending the release through the deep investing fascia of the volar and dorsal forearm compartments, mobilizing the mobile wad, and ensuring the deep flexor compartment is fully decompressed to prevent irreversible myonecrosis.
Hand, Metacarpal, and Digital Release
The dorsum of the hand is highly susceptible to burn edema due to its loose areolar tissue architecture and thin skin. Decompression requires dorsal longitudinal intermetacarpal incisions. These are typically placed between the index and middle metacarpals (the 2nd web space) and between the ring and little metacarpals (the 4th web space). These incisions allow direct access for the release of the dorsal interosseous fascia, effectively decompressing the intrinsic muscle compartments of the hand.
Following the proximal releases, distal perfusion is re-evaluated using a sterile Doppler probe. If finger perfusion remains unsatisfactory, digital escharotomies are strictly indicated. Using a pinpoint electrocautery tip, longitudinal incisions are made along only the ulnar sides of the index, middle, ring, and little fingers. The ulnar side is selected to preserve the critical tactile sensation on the radial side of the digits, which is essential for pinch grip. The thumb requires a radial incision to protect its ulnar digital nerve, vital for key pinch. The digital incision must be placed exactly in the mid-axial line—between the volar digital neurovascular bundles and the dorsal extensor tendon apparatus.
Definitive Coverage and Graft Fixation Technique
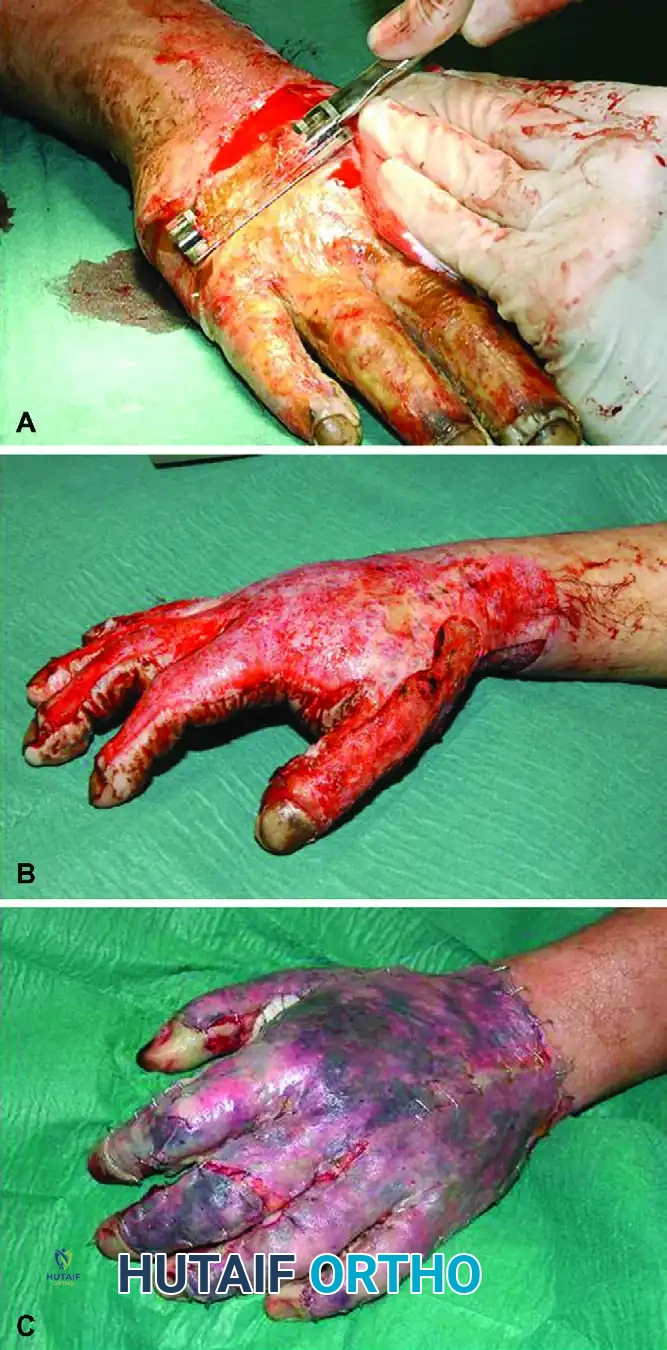
Escharotomy is a temporizing measure. Once the patient is hemodynamically stable, the necrotic eschar must be surgically excised and the soft tissue envelope reconstructed.
As demonstrated in the clinical progression above, definitive management involves tangential excision of the eschar using a Watson or Goulian knife down to healthy, punctate bleeding dermis or subcutaneous fat. The excised areas are then covered with unmeshed sheet autografts. In severe cases where burn contractures threaten joint alignment, temporary "fixation" utilizing axial Kirschner wires driven across the interphalangeal or MCP joints may be necessary to maintain the hand in a functional position while the sheet grafts incorporate. Sheet grafts are preferred over meshed grafts on the hand to minimize secondary fibroproliferative contracture and optimize the functional glide of the underlying extensor tendons.
Complications, Incidence Rates, and Salvage Management
Even when performed with meticulous technique, upper extremity escharotomies carry inherent risks and complications that the orthopedic surgeon must anticipate, recognize, and aggressively manage. The systemic fragility of the burn patient amplifies these localized surgical risks.
The most common complication is an inadequate or incomplete release. This occurs when the surgeon fails to extend the incisions far enough proximally or distally, leaving residual constricting bands of eschar, or fails to recognize the need to convert an escharotomy into a formal deep fasciotomy. This results in persistent compartment syndrome and subsequent myonecrosis. Iatrogenic nerve injury is a devastating complication, most frequently involving the ulnar nerve at the cubital tunnel or the proper digital nerves in the hand due to deviation from the mid-axial safe zones.
Tendon and joint capsule exposure is a profound risk, particularly on the dorsum of the hand and digits where the subcutaneous tissue is minimal. Incising too deeply exposes the delicate extensor paratenon. Exposed tendons rapidly desiccate, leading to necrosis, rupture, and profound loss of extension. Infection is a ubiquitous threat; the open escharotomy wound serves as a direct portal for bacterial and fungal invasion, potentially leading to invasive burn wound sepsis, osteomyelitis, and systemic septic shock.
| Complication | Estimated Incidence | Prevention Strategy | Salvage Management |
|---|---|---|---|
| Inadequate Release / Persistent Ischemia | 10 - 15% | Extend incisions from unburned to unburned skin; utilize objective compartment pressure monitoring post-release. | Immediate return to OR for extension of incisions; conversion to formal deep fascial fasciotomy. |
| Iatrogenic Nerve Injury (e.g., Ulnar Nerve) | 2 - 5% | Strict adherence to mid-axial lines; anterior routing of medial incision at the elbow epicondyle. | Microsurgical epineural repair if recognized acutely; delayed nerve grafting or tendon transfers for late deficits. |
| Tendon Desiccation and Rupture | 5 - 10% | Avoid deep incisions over the dorsal hand/digits; use pinpoint electrocautery; avoid cold scalpel plunging. | Continuous moist saline or biologic dressings; delayed reconstructive tendon grafting or joint arthrodesis. |
| Burn Wound Sepsis / Deep Infection | 15 - 25% | Strict aseptic technique; immediate application of topical antimicrobials (mafenide acetate, silver sulfadiazine). | Aggressive surgical debridement of necrotic tissue; targeted systemic intravenous antibiotic therapy; flap coverage. |
| Severe Hemorrhage / Hematoma | 5 - 8% | Use electrocautery for incisions; correct systemic coagulopathy; meticulous intraoperative hemostasis. | Evacuation of hematoma; surgical exploration and ligation of bleeding vessels; blood product transfusion. |
Phased Post-Operative Rehabilitation Protocols
The immediate post-operative period following an upper extremity escharotomy is intensely focused on maintaining distal perfusion, preventing invasive infection, and initiating early, aggressive rehabilitation to prevent devastating fibroproliferative burn contractures. The rehabilitation protocol is phased, requiring seamless collaboration between the orthopedic surgeon, burn nurses, and specialized hand therapists.
Phase 1: Immediate Post-Operative (Days 0-5)
The primary goals in this phase are edema control, wound protection, and the prevention of joint contractures. The escharotomy wounds are dressed with non-adhering, medicated gauze (such as bismuth tribromophenate or silver-impregnated mesh) to provide antimicrobial prophylaxis without adhering to the delicate underlying tissue. The extremity is covered with a bulky, highly absorbent, but strictly non-constricting dressing. Circumferential taping is absolutely contraindicated. The limb must be continuously elevated above the level of the heart using specialized foam wedges or suspension slings to promote venous and lymphatic drainage. When resting, the hand must be rigidly splinted in the "intrinsic-plus" (safe) position: wrist extended 20-30 degrees, MCP joints flexed 70-90 degrees, and interphalangeal joints fully extended. This maintains the collateral ligaments at their maximal length, preventing devastating extension contractures.
Phase 2: Intermediate and Grafting Phase (Weeks 1-4)
As the patient stabilizes and the eschar demarcates, the patient undergoes definitive tangential excision and sheet grafting. Rehabilitation during this phase balances graft immobilization with the need to prevent tendon adhesions. Following grafting, the hand is typically immobilized for 3 to 5 days to allow for initial graft inosculation and revascularization. Once graft take is confirmed, active and active-assisted range of motion (ROM) exercises are initiated. Passive ROM must be performed judiciously to avoid shearing the newly adherent grafts. Custom thermoplastic splints are fabricated and continuously adjusted to accommodate decreasing edema and to provide a sustained, low-load stretch to healing tissues.
Phase 3: Late Remodeling and Functional Restoration (Months 1-12+)
Burn scars undergo profound hypertrophy and contracture during the remodeling phase, which can last up to 18-24 months. The focus shifts to aggressive scar management and functional restoration. Compression garments (providing 25-30 mm Hg pressure) are worn 23 hours a day to induce scar ischemia and promote collagen reorganization. Silicone elastomer inserts are used over concavities and web spaces to prevent syndactyly. Intensive functional therapy focuses on restoring grip strength, fine motor dexterity, and independent activities of daily living. Despite optimal care, late reconstructive surgeries—such as Z-plasties for web space contractures, tenolysis for tendon adhesions, or capsulotomies for stiff joints—are frequently required to optimize the final orthopedic outcome.
Summary of Landmark Literature and Clinical Guidelines
The evolution of upper extremity escharotomy and burn care is deeply rooted in landmark surgical literature and established clinical guidelines. The American Burn Association (ABA) provides the definitive framework for the emergent management of thermal injuries, emphasizing the critical nature of fluid resuscitation and the early recognition of compartment syndrome.
Historically, the foundational understanding of burn shock and fluid resuscitation was established by the pioneering work of Charles Baxter, who developed the Parkland formula in the 1960s. This formula, while life-saving, highlighted the inevitable consequence of massive third-spacing and the subsequent necessity for escharotomy. The biomechanical principles of compartment syndrome and the critical pressure thresholds requiring surgical intervention were elucidated by Mubarak and Hargens in the 1970s. Their research established the 30 mm Hg threshold and the concept of Delta P, which remains the gold standard for objective monitoring today.
In the realm of surgical technique, Basil Pruitt and the team at the US Army Institute of Surgical Research (USAISR) standardized the anatomical approach to escharotomy, delineating the mid-axial safe zones and describing the catastrophic consequences of iatrogenic nerve injury. More recent literature has focused on advanced monitoring techniques. Studies investigating the efficacy of continuous intra-compartmental pressure monitoring and Near-Infrared Spectroscopy (NIRS) have shown promise in detecting impending microvascular collapse earlier than traditional intermittent Doppler assessments.
Furthermore, contemporary orthopedic literature heavily emphasizes the transition from delayed to early tangential excision and grafting. The work of Janzekovic in the 1970s revolutionized burn care by demonstrating that early excision of the eschar (within 3-5 days) significantly reduces the incidence of burn wound sepsis, mitigates the systemic inflammatory response, and dramatically improves long-term functional and cosmetic outcomes in the upper extremity. This paradigm shift underscores that while escharotomy is the critical initial step to save the limb, early definitive soft-tissue reconstruction is the definitive step to save its function.
