Management of Soft Tissue Injuries & Morel-Lavallée Lesions
Key Takeaway
The initial management of severe soft tissue injuries and Morel-Lavallée lesions requires a systematic, evidence-based approach. This encompasses immediate hemorrhage control, fracture splinting, and meticulous surgical débridement guided by the four C's of muscle viability. For closed degloving injuries, percutaneous drainage techniques combined with compressive therapy have revolutionized treatment, minimizing skin necrosis and deep infection risks while preserving the delicate vascular supply of the traumatized integument.
Comprehensive Introduction and Patho-Epidemiology
In the realm of operative orthopaedics, the ultimate functional outcome of any major musculoskeletal trauma is inextricably linked to the viability, perfusion, and meticulous management of the surrounding soft tissue envelope. The historical paradigm of prioritizing skeletal fixation over soft tissue preservation has long been abandoned in favor of an integrated, ortho-plastic approach. Modern trauma surgery recognizes that the bone and its soft tissue envelope function as a singular, interdependent biologic unit. Disruption of this unit, whether through high-energy open fractures or severe closed degloving injuries, dictates a treatment algorithm where soft tissue resuscitation is paramount. Initial treatment of open wounds and severe closed soft tissue injuries must begin immediately at the scene of the accident or upon arrival at the emergency department, well before transport to a definitive surgical facility. The foundational tenets of this initial phase include direct pressure over the wound to control hemorrhage, rigid splinting of fractures to prevent secondary soft tissue trauma, and the immediate placement of sterile dressings to mitigate nosocomial contamination.
Rapid transport to a definitive trauma center is critical; however, expedited transport should never supersede the fundamental principles of limb stabilization. Unsplinted fractures continue to inflict internal shearing forces, exacerbating muscle crush, disrupting microvascular networks, and significantly increasing the incidence of deep infection, skin necrosis, and subsequent wound breakdown. Among the most deceptive and devastating of these soft tissue insults is the Morel-Lavallée lesion (MLL). Originally described by French surgeon Victor-Auguste-François Morel-Lavallée in 1853, this lesion represents a severe, closed degloving injury characterized by the traumatic separation of the skin and subcutaneous tissue from the underlying deep fascia. This separation is driven by high-energy shearing forces, most commonly encountered in pelvic ring disruptions, acetabular fractures, and severe blunt trauma to the thigh or flank. The sheer magnitude of energy required to create this dissociation invariably results in profound microvascular disruption and widespread cellular necrosis.
When the hypodermis is violently sheared from the inextensible deep fascia, the trans-fascial perforating vessels and lymphatic channels are abruptly severed. This catastrophic mechanical failure creates a massive dead space that rapidly fills with a complex mixture of blood, lymph, and liquefied necrotic fat, forming a highly expansile hemolymphatic collection. If left untreated, the peripheral margins of this collection undergo a profound inflammatory response. Macrophages and fibroblasts migrate to the periphery of the hematoma, eventually forming a dense, fibrous pseudocapsule. This pseudocapsule is biologically inert and lacks the absorptive capacity of normal tissue, thereby preventing spontaneous resorption of the fluid. The clinical consequence is the development of chronic seromas, secondary bacterial colonization, and massive, irreversible skin necrosis that can compromise underlying orthopaedic implants.
Epidemiologically, Morel-Lavallée lesions are most frequently associated with high-velocity motor vehicle collisions, motorcycle accidents, and pedestrian-versus-auto incidents. Literature suggests that up to 10% of patients with pelvic or acetabular fractures will present with a concomitant MLL. The greater trochanter, flank, and lumbosacral regions are the most common anatomic sites, given the prominent bony protuberances and the relatively loose attachment of the subcutaneous fat to the underlying fascia lata or lumbodorsal fascia. Recognition of this injury requires a high index of suspicion, as the overlying epidermis may initially appear intact, masking the catastrophic internal degloving that threatens the viability of the entire regional soft tissue envelope.

FIGURE 53-11A: Clinical appearance of a large Morel-Lavallée lesion in the anterior thigh following a high-energy pelvic fracture. Note the massive swelling and loss of normal topographic landmarks.

FIGURE 53-11B: Posterior view of the same patient, demonstrating the circumferential nature of the fluid collection and the dependent pooling of the hemolymphatic fluid.
Detailed Surgical Anatomy and Biomechanics
The integument of the thigh, pelvis, and gluteal region is particularly vulnerable to ischemic necrosis following a degloving injury due to the erratic, delicate, and highly specific course of its blood supply. Cutaneous perfusion in these areas relies heavily on musculocutaneous and septocutaneous perforators that originate from deep axial vessels, traverse the muscular bellies, pierce the deep fascia, and arborize within the subcutaneous fat to supply the subdermal plexus. In the lateral thigh, for example, the blood supply is predominantly derived from perforators of the descending branch of the lateral circumflex femoral artery and the perforating branches of the profunda femoris. When a tangential shearing force is applied to the skin, the mobile subcutaneous fat translates over the rigid deep fascia (fascia lata), acting as a mechanical guillotine that tethers, stretches, and ultimately ruptures these vertical perforating vessels.
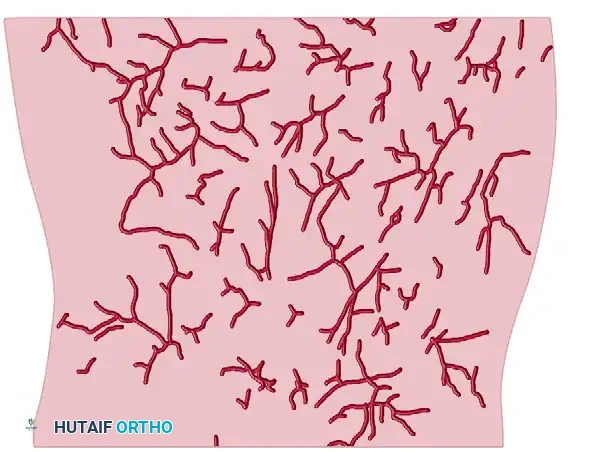

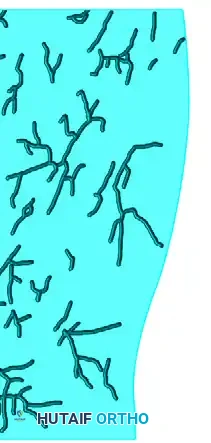
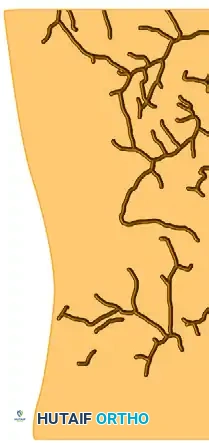
FIGURE 53-12: Tracings of the thigh vessels (internal diameter ≥ 0.25 mm) demonstrating the anterolateral (AL), posterior (P), and anteromedial (AM) vascular networks. The erratic distribution of these perforators highlights why shearing forces so easily devascularize the overlying skin flap.
The biomechanics of the Morel-Lavallée lesion are rooted in the differential viscoelastic properties of the tissue layers involved. The skin and subcutaneous fat exhibit high compliance and elasticity, allowing them to deform significantly under load. Conversely, the deep fascia is a dense, inextensible fibrous layer designed to compartmentalize muscle and transmit mechanical force. During a high-energy tangential impact, the kinetic energy is absorbed by the deformation of the superficial layers. When the limit of elasticity is exceeded, failure occurs precisely at the interface between the compliant hypodermis and the rigid fascia. This mechanical dissociation not only severs the vascular supply but also crushes the adipocytes within the subcutaneous layer, releasing free fatty acids that incite a severe local inflammatory response, further compromising the microcirculation of the overlying skin flap.
Understanding the viability of the underlying musculature is equally critical, particularly when the injury involves an open fracture or requires surgical exploration. Skeletal muscle is highly sensitive to ischemia and crush injury. Retained necrotic muscle serves as an ideal culture medium for catastrophic anaerobic infections, including clostridial myonecrosis (gas gangrene). During surgical exploration, the viability of skeletal muscle is strictly evaluated using the universally recognized Four "C's": Consistency, Color, Contractility, and Circulation. Normal muscle is firm, resilient, and rebounds when grasped; nonviable muscle is friable, mushy, and often described as having a "waxy" or "stewed" texture. Healthy muscle exhibits a bright, beefy red appearance, whereas ischemic muscle is dark, purple, pale, or gray. Contractility is the most reliable indicator; normal muscle will visibly twitch when mechanically pinched or stimulated with electrocautery. Finally, healthy muscle will bleed briskly when incised, whereas a lack of punctate capillary bleeding indicates irreversible ischemia.
The management of tendinous structures and deep fascia within the zone of injury requires a highly nuanced approach. Completely severed tendon ends that are highly contaminated, frayed, and crushed may require sharp excision to prevent deep infection. However, tendons are inherently avascular structures that rely heavily on their surrounding paratenon and ambient moisture for survival. Care must be taken to maintain continuous moisture around such structures during prolonged surgeries. Once a tendon becomes desiccated, it undergoes irreversible necrosis, and subsequent excision becomes absolutely necessary. To prevent desiccation during staged reconstructions, early flap placement, the use of saline-soaked gauze, or the application of a sealed Negative Pressure Wound Therapy (NPWT) dressing is highly recommended to maintain a physiologic, moist environment and promote angiogenesis.
Exhaustive Indications and Contraindications
The decision-making process for managing soft tissue degloving injuries and Morel-Lavallée lesions is dictated by the chronicity of the lesion, the viability of the overlying skin, the presence of underlying fractures requiring fixation, and the patient's physiologic status. Historically, conservative management with compression alone or simple percutaneous aspiration was attempted; however, simple aspiration is fraught with unacceptably high recurrence rates (often exceeding 50%) because it fails to address the necrotic fat and the ongoing lymphatic leak within the cavity. Currently, these lesions should be treated aggressively, ideally at the time of internal fixation of the underlying fracture, or within the first few days of admission before a mature pseudocapsule can form.
Indications for the targeted percutaneous drainage technique include acute lesions (typically presenting within 3 to 5 days of injury), lesions with intact and viable overlying skin, and fluid collections that are highly fluctuant without evidence of a thick, organized pseudocapsule on advanced imaging. This minimally invasive approach is particularly indicated when the lesion overlies a planned surgical approach for pelvic or acetabular fracture fixation. By evacuating the hematoma and mechanically debriding the cavity percutaneously, the surgeon can collapse the dead space and allow the skin flap to adhere, thereby minimizing the risk of wound breakdown when the formal orthopaedic incision is subsequently made.
Conversely, formal open debridement is indicated for chronic, neglected Morel-Lavallée lesions where a thick, mature pseudocapsule has already formed. These chronic lesions act as autonomous bursae that will continuously secrete fluid regardless of closed suction drainage. Open debridement is also absolutely indicated in the presence of frank skin necrosis, full-thickness eschar formation, or overt clinical signs of deep space infection (purulence, erythema, systemic sepsis). In these scenarios, the necrotic skin must be radically excised back to bleeding margins, and the entire pseudocapsule must be stripped from the underlying fascia to create a healthy, vascularized wound bed capable of supporting a split-thickness skin graft or a rotational flap.
Contraindications must be carefully weighed to avoid converting a closed, sterile degloving injury into an open, infected disaster. Traditional open surgical approaches to drain an acute Morel-Lavallée lesion carry a profound risk of further devascularizing the already compromised skin flap. Extensive incisions disrupt the few remaining intact collateral vessels, frequently resulting in massive full-thickness tissue loss. Therefore, large open incisions are contraindicated in the acute setting if the skin is viable and the lesion can be managed percutaneously. Furthermore, definitive closure of any degloving injury is contraindicated if the adequacy of the debridement is in question; such wounds must be left open and managed with NPWT until a second-look debridement confirms a pristine wound bed.
| Intervention Modality | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Percutaneous Drainage (Tseng/Tornetta) | Acute lesions (< 5 days); Viable overlying skin; Highly fluctuant fluid collection; Pre-operative optimization for pelvic fixation. | Frank skin necrosis; Established deep space infection; Thick, mature pseudocapsule (chronic). | Overlying abrasions/road rash compromising portal sites; Severe coagulopathy. |
| Open Radical Debridement | Chronic lesions with mature pseudocapsule; Full-thickness skin necrosis; Infected MLL; Failure of percutaneous drainage. | Acute lesions with viable skin (risk of iatrogenic devascularization); Hemodynamically unstable polytrauma patient. | Poor soft tissue envelope precluding future flap coverage; Severe peripheral vascular disease. |
| Simple Needle Aspiration | Diagnostic sampling to rule out infection; Extremely small, localized seromas (< 50cc). | Definitive treatment of large MLL (high recurrence); Presence of necrotic fat/debris. | Loculated fluid collections; Proximity to major neurovascular bundles without US guidance. |
| Negative Pressure Wound Therapy (NPWT) | Open MLL after debridement; Staged closure of massive degloving; Protection of exposed tendons/fascia. | Unexplored/undebrided necrotic tissue; Active, uncontrolled hemorrhage. | Exposed major blood vessels without muscle coverage; Malignant wounds. |

FIGURE 53-11C: Appearance of a large, neglected Morel-Lavallée lesion in the buttock. The delayed presentation has led to profound skin necrosis and full-thickness eschar formation, necessitating extensive open débridement.
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning is essential for the successful management of complex soft tissue injuries. Clinical evaluation begins with a meticulous physical examination. Patients typically present with a fluctuant, highly compressible mass, often accompanied by skin hypermobility, extensive ecchymosis, and decreased cutaneous sensation over the affected area due to the avulsion of cutaneous nerve branches. The "roll test," where the examiner's hand can smoothly glide the skin over the underlying fascia, is pathognomonic for a degloving injury. The boundaries of the fluctuance must be carefully palpated and marked with an indelible surgical marker prior to the induction of anesthesia, as the fluid can shift or become less apparent once the patient is positioned on the operating table.
Advanced imaging plays a pivotal role in pre-operative templating. Magnetic Resonance Imaging (MRI) is considered the gold standard for evaluating Morel-Lavallée lesions. MRI allows for precise volumetric measurement of the fluid collection, identification of loculations, and, most importantly, assessment of pseudocapsule formation. The Mellado and Bencardino classification system utilizes MRI characteristics (shape, signal intensity, capsule presence) to categorize these lesions into six types, guiding the surgeon toward percutaneous versus open management. In the acute trauma setting where MRI may be impractical, high-resolution ultrasonography serves as an excellent adjunct, providing real-time dynamic assessment of the fluid collection, identifying echogenic debris (necrotic fat), and guiding percutaneous drain placement.
Patient positioning is dictated by the anatomic location of the lesion and the requirements of any concomitant orthopaedic procedures. For lesions involving the greater trochanter or lateral thigh, the patient is typically placed in the lateral decubitus position on a radiolucent table. A beanbag positioner and axillary roll are utilized to secure the patient, ensuring that the entire lateral aspect of the limb, from the iliac crest to the knee, is accessible. For posterior pelvic, lumbosacral, or gluteal lesions, the prone position is required. Careful attention must be paid to padding all bony prominences, and the abdomen must hang free to prevent increased intra-abdominal pressure and subsequent venous engorgement, which can exacerbate intra-operative bleeding.
The surgical field must be prepped and draped widely. In cases of massive degloving, the prep should extend well beyond the marked borders of the lesion to accommodate potential extensile measures or the harvesting of split-thickness skin grafts. If the procedure is being performed in conjunction with pelvic or acetabular fracture fixation, the draping must allow for simultaneous access to the anterior and posterior pelvic rings, often necessitating a "floppy lateral" or highly modified supine position. The surgical team must ensure that rigid suction devices, surgical brushes, and a variety of closed-suction drains are available on the sterile field before the incision is made.
Step-by-Step Surgical Approach and Fixation Technique
The surgical management of Morel-Lavallée lesions has been revolutionized by the targeted percutaneous drainage technique described by Tseng and Tornetta. This minimally invasive approach effectively evacuates the hematoma and debrides the cavity while preserving the fragile cutaneous blood supply. The procedure begins with the creation of small (1-2 cm) incisions at the most dependent portions of the fluctuant collection, as determined by pre-operative marking and gravity. Careful placement of these portals is critical; they must be positioned to allow for optimal dependent drainage but should avoid traversing planned surgical incisions for underlying fracture fixation.
Once access is achieved, a rigid suction tip (such as a Yankauer) is introduced through the incisions to evacuate the gross hematoma and map the full anatomical extent of the cavity. Following evacuation, mechanical debridement of the dead space is mandatory. A sterile surgical brush (often referred to as a "bottle brush" or a standard orthopaedic prep brush) is introduced through the percutaneous portals. The brush is vigorously passed throughout the cavity, scraping the undersurface of the skin flap and the superficial surface of the deep fascia. This mechanical abrasion serves two vital purposes: it disrupts the early fibrinous pseudocapsule that prevents tissue adhesion, and it aggressively debrides the loose, necrotic, liquefied fat that acts as a nidus for infection.

FIGURE 53-13A: Percutaneous drainage of a Morel-Lavallée lesion. The extent of the lesion is carefully determined and evacuated using a rigid suction tip.
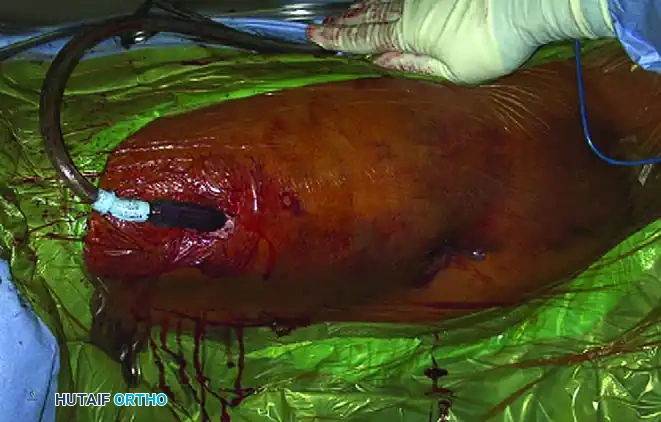
FIGURE 53-13B: A sterile surgical brush is utilized percutaneously to aggressively débride loose, necrotic fat and disrupt the fibrinous cavity lining.
Following mechanical debridement, copious low-pressure irrigation with normal saline (often 3 to 6 liters) is performed until the effluent is entirely clear of hematoma and fat globules. Large-bore closed suction drains (e.g., 10-French or 15-French Blake or Jackson-Pratt drains) are then placed through the incisions and tunneled extensively throughout the cavity. The drains must cross the dead space entirely to prevent isolated fluid pockets. Finally, a robust, uniform compression bandage is applied externally. This compression is the linchpin of the procedure; it obliterates the dead space, acts as an external splint, and forces the surgically abraded skin flap to adhere to the underlying fascia, promoting rapid revascularization and tissue synthesis.
In cases of delayed presentation or refractory lesions where percutaneous methods are contraindicated, formal open debridement is required. The incision is typically made longitudinally over the axis of the fluid collection, excising any grossly necrotic skin. The fundamental principle of open debridement is the radical excision of the fibrotic pseudocapsule. The surgeon must sharply dissect the capsule from the deep fascia and the undersurface of the dermis until a healthy, bleeding wound bed is achieved. Skin debridement should never be performed under tourniquet control, as a tourniquet obscures capillary bleeding, making it impossible to assess true viability. Following radical excision, the massive open wound is typically managed with Negative Pressure Wound Therapy (NPWT) to stimulate granulation tissue, followed by delayed primary closure, split-thickness skin grafting, or local rotational flap coverage.

FIGURE 53-11D: Operative exposure of a chronic Morel-Lavallée lesion. The image demonstrates the profound depth of the lesion and the necessity for radical excision of the fibrotic pseudocapsule and nonviable tissue to achieve a healthy, bleeding wound bed.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, the management of severe soft tissue degloving injuries is fraught with complications. The most common complication following the treatment of a Morel-Lavallée lesion is the recurrence of the seroma or hemolymphatic fluid collection. Literature demonstrates that simple needle aspiration carries a recurrence rate of 40% to 80%. Even with aggressive percutaneous drainage, recurrence rates hover around 10% to 15%, particularly if the compression dressing is inadequate or if the drains are removed prematurely. Recurrence necessitates a return to the operating room for repeat debridement, and chronic recurrences often mandate conversion to an open, radical excision of the newly formed pseudocapsule.
Surgical site infection (SSI) and deep space infections represent catastrophic complications, particularly when orthopaedic implants are present in the underlying bone. The incidence of infection in closed MLLs treated with early percutaneous drainage is remarkably low (less than 5%), but this rate skyrockets to over 30% in neglected lesions or those treated with inappropriate open incisions that devascularize the skin. The liquefied necrotic fat within the lesion serves as an ideal culture medium for both skin flora (Staphylococcus aureus) and nosocomial pathogens. If a deep infection develops, immediate open debridement, implant retention (if stable) or removal (if loose), and targeted intravenous antibiotic therapy are mandatory. The wound must be left open and managed with NPWT or antibiotic-impregnated polymethylmethacrylate (PMMA) beads.
Skin necrosis is the most visually apparent and reconstructively challenging complication. It occurs due to the initial shear-induced devascularization compounded by the pressure of the expanding hematoma. The incidence of partial or full-thickness skin loss ranges from 15% to 25% in high-energy pelvic trauma. When necrosis occurs, the dead eschar must be sharply excised. Small defects may heal by secondary intention or delayed primary closure, but massive defects require complex ortho-plastic salvage. Salvage management often involves the application of a split-thickness skin graft (STSG) once a healthy granulation bed is established via NPWT. In cases of exposed bone, tendon, or hardware, local muscle rotational flaps or free tissue transfer become necessary to provide durable, vascularized coverage.
For refractory seromas that persist despite repeated drainage and compression, chemical sclerotherapy has emerged as a viable salvage technique. Sclerosing agents, such as doxycycline, bleomycin, or sterile talc, are instilled into the cavity via the percutaneous drains. These agents incite a severe, localized inflammatory response that destroys the secretory lining of the pseudocapsule and promotes aggressive fibrosis, thereby sealing the dead space. While highly effective (success rates exceeding 80% in refractory cases), sclerotherapy is intensely painful and requires adequate patient analgesia. It is strictly contraindicated if there is any communication between the MLL cavity and an underlying joint space or fracture site.
| Complication | Estimated Incidence | Pathophysiology & Risk Factors | Prevention & Salvage Management |
|---|---|---|---|
| Seroma Recurrence | 10-15% (Percutaneous) >50% (Aspiration) |
Failure to disrupt pseudocapsule; premature drain removal; inadequate external compression. | Prevention: Vigorously use surgical brush; leave drains until <30cc/24hrs. Salvage: Repeat debridement; Chemical sclerotherapy (Doxycycline/Talc). |
| Skin Necrosis | 15-25% | Initial shear devascularization; iatrogenic injury from large open incisions; hematoma pressure. | Prevention: Use percutaneous techniques for acute lesions; avoid tourniquets during assessment. Salvage: Radical excision of eschar; NPWT; Split-thickness skin grafting (STSG) or flap coverage. |
| Deep Space Infection | <5% (Acute) >30% (Chronic/Open) |
Necrotic fat acting as a nidus; nosocomial contamination; contiguous spread to implants. | Prevention: Early aggressive evacuation; copious irrigation; prophylactic IV antibiotics. Salvage: Formal open debridement; antibiotic PMMA beads; hardware removal if loose. |
| Cosmetic Contour Deformity | 20-40% | Loss of subcutaneous fat volume; aggressive fibrosis and tethering of the skin to deep fascia. | Prevention: Uniform, smooth compression dressings to prevent irregular adherence. Salvage: Delayed fat grafting (lipofilling) or scar revision (rarely indicated unless severe). |
Phased Post-Operative Rehabilitation Protocols
The post-operative rehabilitation of a patient with a severe soft tissue injury or a treated Morel-Lavallée lesion requires a delicate balance between protecting the fragile soft tissue reconstruction and preventing the systemic complications of immobility. The immediate post-operative phase (Days 0 to 7) is characterized by strict protection of the surgical site. The primary goal is to facilitate the adherence of the degloved skin flap to the underlying deep fascia. This is achieved through the continuous application of a robust, uniform compression garment or specialized elastic bandaging. The compression must be monitored daily to ensure it is not causing distal ischemia or localized pressure necrosis. Closed suction drains are managed meticulously; the universal protocol dictates a mandatory delay in removal until the output is consistently less than 30 cc per 24-hour period, which often takes 7 to 14 days.
During the early mobilization phase (Weeks 1 to 4), rehabilitation focuses on maintaining joint range of motion (ROM) while strictly avoiding any tangential shearing forces over the healing lesion. For example, if the lesion is located over the greater trochanter, the patient must be instructed to avoid sliding transfers or pivoting on the affected hip, as these motions can easily disrupt the fragile fibrinous adhesions forming between the skin and fascia. Weight-bearing status is almost entirely dictated by the concomitant skeletal injuries (e.g., pelvic or acetabular fractures). If the underlying bone is stable, protected touch-down or partial weight-bearing may be initiated, utilizing assistive devices to minimize muscle contraction forces that could pull on the fascial attachments.
The intermediate rehabilitation phase (Weeks 4 to 8) introduces progressive mechanical loading of the soft tissues. As the skin flap becomes durably adherent, the compression garments can be gradually we
