Mastering Orthopaedic Trauma Principles and Open Fracture Management

Key Takeaway
The management of polytraumatized patients requires a multidisciplinary approach centered on Advanced Trauma Life Support (ATLS) protocols and Damage Control Orthopaedics (DCO). This comprehensive guide details the evidence-based evaluation of musculoskeletal injuries, the OTA 2010 open fracture classification, updated antibiotic prophylaxis guidelines, and surgical strategies for ballistic trauma. Early stabilization and physiological resuscitation remain paramount in mitigating systemic inflammatory responses and preventing mortality.
Comprehensive Introduction and Patho-Epidemiology
The management of the polytraumatized patient represents one of the most formidable challenges in clinical medicine, demanding a highly orchestrated, multidisciplinary approach that integrates the expertise of trauma surgeons, orthopaedic surgeons, neurosurgeons, and critical care specialists. The acute stabilization of high-energy appendicular, pelvic, and axial skeleton fractures requires not only specialized surgical acumen but also a profound understanding of the systemic physiological derangements that accompany massive tissue injury. Extensive epidemiological data unequivocally demonstrates that the rapid triage and treatment of polytrauma patients in designated Level 1 or Level 2 trauma centers significantly improve survival rates, decrease the incidence of devastating complications, and optimize long-term functional outcomes. The economic and clinical superiority of immediate referral to a dedicated trauma center is well-established, mitigating the morbidity associated with delayed resuscitation and secondary transfers.
Polytrauma initiates a profound and complex cascade of cellular, biochemical, and immunological events. The initial mechanical insult triggers a Systemic Inflammatory Response Syndrome (SIRS), characterized by the massive release of pro-inflammatory cytokines, including Interleukin-6 (IL-6), Interleukin-1 (IL-1), and Tumor Necrosis Factor-alpha (TNF-α). This hyper-inflammatory state is directly correlated with endothelial damage, increased capillary permeability, and the subsequent development of Acute Respiratory Distress Syndrome (ARDS) and Multiple Organ Dysfunction Syndrome (MODS). Concurrently, the body mounts a Compensatory Anti-inflammatory Response Syndrome (CARS), which, if disproportionate, can lead to severe immunosuppression and an increased susceptibility to nosocomial infections and sepsis. The orthopaedic surgeon must recognize that the timing and magnitude of surgical intervention directly influence this immunological balance; an ill-timed, prolonged reconstructive procedure can act as a "second hit," exacerbating SIRS and precipitating physiological collapse.
The Advanced Trauma Life Support (ATLS) protocol remains the universal algorithmic foundation for the initial evaluation and resuscitation of these critically ill patients. Orthopaedic surgeons must seamlessly integrate their assessment into the primary survey (ABCDE). Airway management must proceed with strict cervical spine precautions until formal clinical and radiographic clearance is achieved. Breathing assessment requires vigilance for thoracic trauma, such as flail chest or pneumothorax, which often accompany high-energy scapular or clavicular fractures. Circulation demands immediate attention to life-threatening orthopaedic hemorrhage, most notably unstable pelvic ring disruptions and multiple long-bone fractures. The application of a pelvic binder centered over the greater trochanters, rather than the iliac crests, is a critical, life-saving maneuver that reduces pelvic volume and provides a tamponade effect on venous plexus bleeding. Disability assessment necessitates a rapid Glasgow Coma Scale evaluation and a focused neurological examination of the extremities to document baseline deficits before any intervention. Finally, Exposure requires complete undressing to identify all injuries, coupled with aggressive measures to prevent hypothermia, which exacerbates coagulopathy and acidosis—the dreaded "lethal triad" of trauma.
Despite the rigorous application of primary and secondary surveys, the incidence of missed injuries in polytrauma patients remains a significant clinical concern, ranging from 5% to 20% in contemporary series. Factors contributing to delayed diagnosis include an altered level of consciousness due to traumatic brain injury or sedation, hemodynamic instability precluding a comprehensive examination, and the presence of distracting injuries where a severely mangled extremity masks a subtle, yet critical, contralateral or axial injury. Consequently, a formal Tertiary Survey is an absolute mandate. This comprehensive head-to-toe re-examination, coupled with a meticulous review of all radiological studies, must be performed once the patient is conscious, extubated, and physiologically stable, ensuring that occult fractures, subtle ligamentous instabilities, and peripheral nerve injuries are identified and managed appropriately.
Detailed Surgical Anatomy and Biomechanics
A masterful understanding of surgical anatomy and biomechanics is paramount for the orthopaedic trauma surgeon, dictating both the initial damage control interventions and the subsequent definitive reconstructions. In the context of high-energy trauma, the skeletal system cannot be viewed in isolation; it must be evaluated as an integral component of the surrounding soft tissue envelope, vascular networks, and neurological pathways. The pelvic ring, for instance, is a complex osteoligamentous structure designed to transfer axial loads from the spine to the lower extremities. Its stability relies heavily on the robust posterior ligamentous complex, including the anterior and posterior sacroiliac ligaments, the sacrospinous ligaments, and the sacrotuberous ligaments. Disruption of these structures, as seen in anteroposterior compression (APC) or vertical shear (VS) injuries, leads to massive retroperitoneal hemorrhage primarily from the presacral venous plexus and the branches of the internal iliac artery, necessitating immediate mechanical stabilization and potential angiographic embolization.
The vascular anatomy of long bones plays a critical role in fracture healing and the management of open fractures. The diaphyseal blood supply is dual in nature, comprising the high-pressure endosteal system (nutrient artery) and the low-pressure periosteal system. In high-energy open fractures, the periosteal stripping caused by the initial trauma, combined with the disruption of the nutrient artery, renders the cortical bone severely ischemic. This anatomical reality underscores the necessity for meticulous, tissue-preserving surgical approaches and the rationale behind utilizing intramedullary implants that offer biomechanical stability while minimizing further iatrogenic damage to the fragile periosteal blood supply. Furthermore, the fascial compartments of the extremities, particularly the four compartments of the lower leg (anterior, lateral, superficial posterior, and deep posterior), have distinct anatomical boundaries that are unyielding to increased volume. The orthopaedic surgeon must possess an intimate knowledge of these compartments, their neurovascular contents, and the precise surgical planes required to perform a complete and effective decompressive fasciotomy.
The biomechanics of trauma dictate the fracture pattern and the extent of soft tissue injury. Fractures result from forces that exceed the ultimate tensile or compressive strength of the bone, manifesting as transverse fractures from pure bending, spiral fractures from torsion, and complex comminuted fractures from high-energy axial loading. In the realm of ballistic injuries, the biomechanics of tissue destruction are governed by the kinetic energy equation ($KE = 1/2 mv^2$). High-velocity rifle projectiles (>2,000 feet/second) transfer massive kinetic energy, creating a temporary cavitational wave that stretches, tears, and devitalizes tissues far beyond the actual bullet tract. This phenomenon, known as cavitation, results in a zone of injury that behaves similarly to a severe crush injury or a high-grade open fracture, mandating aggressive, serial surgical debridement. Conversely, low-velocity civilian handgun projectiles typically impart minimal kinetic energy, causing tissue damage primarily confined to the direct path of the bullet, thereby requiring a less radical surgical approach.
The soft tissue envelope is the ultimate arbiter of success in orthopaedic trauma. The concept of the "zone of injury" extends well beyond the visible wound or the fracture lines seen on a radiograph. It encompasses the entire region of traumatized skin, subcutaneous tissue, fascia, and muscle that has sustained microvascular damage and is at risk for subsequent necrosis. Surgical incisions for definitive fixation must be meticulously planned to avoid traversing this compromised tissue, utilizing angiosome-based approaches and internervous planes to preserve the remaining vascularity. Failure to respect the anatomical and biomechanical realities of the soft tissue envelope inevitably leads to wound dehiscence, deep infection, and catastrophic failure of the reconstruction.
Exhaustive Indications and Contraindications
The decision-making process regarding the timing and type of surgical intervention in the polytraumatized patient is arguably the most critical cognitive skill required of the orthopaedic trauma surgeon. The historical paradigm of Early Total Care (ETC)—the definitive stabilization of all major fractures within the first 24 hours—was championed to facilitate early mobilization, reduce pulmonary complications, and minimize intensive care unit (ICU) length of stay. However, ETC is strictly indicated only for the physiologically stable patient. In patients presenting in a state of physiological extremis, the prolonged operative time, substantial blood loss, and additional inflammatory burden associated with definitive intramedullary nailing or complex plating act as a lethal "second hit."
Damage Control Orthopaedics (DCO) emerged as the life-saving alternative for physiologically unstable or "borderline" patients. The primary indication for DCO is the presence of the lethal triad (hypothermia, coagulopathy, and acidosis) or severe physiological derangement that precludes prolonged surgery. DCO focuses on the rapid, minimally invasive stabilization of major long bone and pelvic fractures, typically utilizing external fixation. This approach controls hemorrhage, minimizes ongoing soft tissue trauma, and provides sufficient mechanical stability to allow for upright positioning and pulmonary toilet in the ICU, all while limiting the surgical duration to less than 60-90 minutes. Once the patient is physiologically optimized—evidenced by the clearance of serum lactate, normalization of coagulation profiles, and resolution of the acute inflammatory phase—the patient is returned to the operating room for the conversion of external fixators to definitive internal fixation.
Contraindications to immediate definitive fixation are primarily physiological rather than anatomical. Severe traumatic brain injury (TBI) with elevated intracranial pressure (ICP) is a relative contraindication to early intramedullary nailing, particularly of the femur, due to the risk of secondary brain injury from intraoperative hypotension, hypoxia, or the theoretical risk of fat embolization exacerbating cerebral edema. Similarly, profound blunt thoracic trauma with bilateral pulmonary contusions and hypoxia (PaO2/FiO2 ratio < 200) strongly favors a DCO approach to avoid the pulmonary insult associated with intramedullary reaming.
Physiological Parameters Guiding Surgical Strategy
| Clinical Parameter | Stable (Indicated for ETC) | Borderline (Consider DCO) | Unstable (Strict DCO) | In Extremis (Life-Saving Only) |
|---|---|---|---|---|
| Systolic Blood Pressure | > 100 mm Hg | 80 - 100 mm Hg | < 80 mm Hg | Unrecordable / CPR |
| Blood Transfusion Requirement | < 2 Units | 2 - 6 Units | > 6 Units | Massive Transfusion Protocol |
| Serum Lactate | < 2.0 mmol/L | 2.0 - 2.5 mmol/L | > 2.5 mmol/L | > 5.0 mmol/L |
| Base Deficit | Normal | -2 to -6 mEq/L | < -6 mEq/L | < -10 mEq/L |
| Coagulation (Platelets/INR) | Plt > 110k, Normal INR | Plt 90-110k, INR > 1.2 | Plt < 90k, INR > 1.5 | DIC present |
| Core Body Temperature | > 35°C | 33°C - 35°C | < 33°C | < 32°C |
| Thoracic Trauma | None / Mild | Moderate (Unilateral) | Severe (Bilateral contusions) | ARDS / Severe Hypoxia |
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning in the setting of acute orthopaedic trauma must be executed with both speed and meticulous attention to detail. The foundation of this planning rests upon high-quality radiographic imaging. While the traditional ATLS trauma series (AP chest and AP pelvis) remains the initial screening tool, modern trauma protocols heavily rely on whole-body computed tomography (CT pan-scan). The CT scan provides unparalleled three-dimensional understanding of complex fracture morphology, particularly for pelvic ring disruptions, acetabular fractures, and intra-articular fractures of the lower extremity. It is the gold standard for identifying subtle ligamentous avulsions, occult spinal fractures, and the exact trajectory of ballistic projectiles. For open fractures or high-energy trauma in proximity to major vessels, CT angiography (CTA) is mandatory to rule out intimal tears, pseudoaneurysms, or complete transections that require immediate vascular intervention prior to or concurrent with orthopaedic stabilization.
Templating, even in the emergent setting, is a non-negotiable step. Digital templating software allows the surgeon to accurately determine the length and diameter of intramedullary nails, the appropriate contour and length of plates, and the optimal trajectory for locking screws. In the context of Damage Control Orthopaedics, templating involves planning the construct of the external fixator. The surgeon must anticipate the future definitive surgical approach and place the external fixation pins outside the planned surgical incisions and away from the ultimate zone of internal fixation. This strategic pin placement minimizes the risk of pin-tract infections compromising the definitive hardware and ensures that the external fixator does not obstruct the surgical field during the conversion procedure.
Patient positioning is a critical component of the operative plan, particularly for polytraumatized patients who may require concurrent interventions by multiple surgical teams (e.g., laparotomy by general surgery and femoral stabilization by orthopaedics). The patient is typically positioned supine on a fully radiolucent Jackson table or a standard operating table with a radiolucent top. This setup allows for unimpeded fluoroscopic access from the chest to the toes. Careful attention must be paid to padding all bony prominences to prevent pressure necrosis during prolonged procedures. The entire injured extremity, and often the contralateral extremity for length and rotation comparison, must be widely prepped and draped. In cases of severe pelvic trauma or bilateral lower extremity injuries, a "floating" setup where both legs are prepped free allows for dynamic assessment of pelvic stability, simultaneous bilateral surgery, and accurate restoration of limb length and rotational alignment.
Coordination with the anesthesia team is paramount before the incision is made. The orthopaedic surgeon must clearly communicate the anticipated blood loss, the need for muscle relaxation (essential for fracture reduction), and the potential requirement for intraoperative vasopressor support. In cases involving severe open fractures or mangled extremities, the tourniquet should be applied high on the limb but left uninflated unless life-threatening hemorrhage occurs, allowing the surgeon to accurately assess tissue perfusion and viability during the debridement process.
Step-by-Step Surgical Approach and Fixation Technique
The surgical management of high-energy orthopaedic trauma, particularly open fractures, is a masterclass in soft tissue handling, radical debridement, and biomechanical stabilization. The initial surgical intervention sets the trajectory for the patient's entire functional outcome.
The procedure commences with the management of the open wound. The fundamental principle is the radical excision of all devitalized tissue—the "Godina principles" of aggressive debridement. The traumatic wound must be systematically extended utilizing longitudinal incisions that respect angiosomes and internervous planes. The skin edges are sharply excised to healthy, bleeding margins. Subcutaneous fat, which has a poor blood supply and is highly susceptible to necrosis and infection, is generously debrided. The assessment of muscle viability is governed by the "4 Cs": Color, Consistency, Contractility, and Capacity to bleed. Any muscle that is dark, friable, non-contractile to electrocautery, or non-bleeding must be ruthlessly excised. Retention of necrotic muscle is the primary catalyst for deep infection and subsequent amputation.
Bone debridement requires the removal of all small, avascular cortical fragments devoid of soft tissue attachments. However, large articular fragments must be retained, meticulously cleaned, and provisionally stabilized. Following radical debridement, the wound undergoes copious irrigation. Contemporary evidence, notably the FLOW trial, has demonstrated that low-pressure irrigation with normal saline is superior to high-pressure pulsatile lavage or the addition of castile soap, as high pressure can drive contaminants deeper into the tissues and further damage the fragile microcirculation. The volume of irrigation should be proportional to the severity of the contamination, typically ranging from 3 to 9 liters.
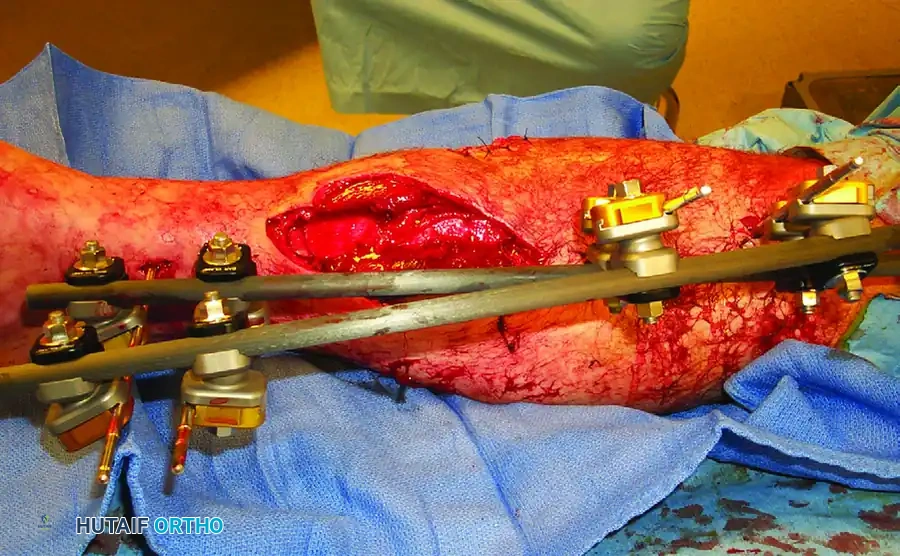
Following debridement and irrigation, the fracture requires immediate stabilization. In the physiologically unstable patient or the presence of a severe soft tissue envelope (Gustilo-Anderson Type IIIB or IIIC), Damage Control Orthopaedics dictates the application of a spanning external fixator.
The application of a spanning external fixator must be executed with precision. Schanz pins (typically 5.0mm for the femur and tibia) are inserted percutaneously, strictly outside the zone of injury and away from future definitive surgical incisions. For a knee-spanning construct, pins are placed in the anterior or anterolateral femur and the anteromedial face of the tibia. Pre-drilling both cortices with a sharp drill bit and utilizing cooling irrigation is mandatory to prevent thermal necrosis of the bone, which inevitably leads to pin loosening and deep infection. The pins are connected via carbon fiber rods and multi-pin clamps to create a rigid, multi-planar construct that restores length, alignment, and rotation. This rigid stabilization reduces ongoing soft tissue trauma, mitigates pain, and facilitates nursing care and wound management.
In the setting of acute compartment syndrome or a high-risk mechanism (e.g., severe crush injury, prolonged ischemia), a decompressive fasciotomy is an absolute emergency. For the lower leg, the two-incision, four-compartment fasciotomy is the gold standard. A generous anterolateral incision (typically 15-20 cm) is made to release the anterior and lateral compartments, taking extreme care to identify and protect the superficial peroneal nerve as it exits the deep fascia. A second posteromedial incision, placed 2 cm posterior to the medial border of the tibia, is utilized to release the superficial and deep posterior compartments. The soleus bridge must be meticulously taken down to ensure complete decompression of the deep posterior compartment, which houses the posterior tibial vessels and nerve. The wounds are left open, covered with a negative pressure wound therapy (NPWT) device or sterile dressings, and planned for delayed primary closure or split-thickness skin grafting once the swelling subsides.
Complications, Incidence Rates, and Salvage Management
The management of polytrauma and open fractures is fraught with life-threatening and limb-threatening complications. The orthopaedic surgeon must maintain a high index of suspicion, employ aggressive prophylactic measures, and possess the technical repertoire to execute complex salvage procedures when complications arise.
Acute complications are primarily physiological and systemic. Fat Embolism Syndrome (FES) is a severe complication following long bone fractures, particularly of the femur and tibia. It presents classically with the triad of hypoxemia, neurological abnormalities, and a petechial rash. The incidence is significantly reduced by early fracture stabilization (ETC or DCO). Acute Respiratory Distress Syndrome (ARDS) is a manifestation of the systemic inflammatory response, characterized by non-cardiogenic pulmonary edema and refractory hypoxemia. Management is supportive, relying on lung-protective ventilation strategies in the ICU. Acute compartment syndrome, if missed or treated late (beyond 8 hours of ischemia), results in irreversible myonecrosis, Volkmann's ischemic contracture, and profound neurological deficits, frequently necessitating amputation.
Subacute and chronic complications are predominantly localized to the injured extremity. Deep infection and chronic osteomyelitis are the most dreaded complications of open fractures. Despite aggressive debridement and appropriate antibiotic prophylaxis, infection rates in severe open fractures (Gustilo Type III) can exceed 15-20%. Management requires a multidisciplinary approach involving radical surgical debridement of infected bone (often creating a critical-sized defect), prolonged targeted intravenous antibiotics guided by deep tissue cultures, and complex reconstruction techniques such as the Masquelet induced-membrane technique or distraction osteogenesis via Ilizarov frames.
Non-union and mal-union represent failures of the biological healing process or the mechanical construct. Hypertrophic non-unions, characterized by abundant callus formation but failure to bridge the fracture gap, indicate adequate biology but inadequate mechanical stability, requiring revision internal fixation. Atrophic non-unions, characterized by a lack of callus and tapering bone ends, indicate biological failure, necessitating decortication, rigid fixation, and the application of autologous bone graft (typically harvested from the iliac crest) or orthobiologics (e.g., BMP-2).
Comprehensive Complication and Salvage Matrix
| Complication | Estimated Incidence | Pathophysiology / Risk Factors | Salvage Management & Intervention Strategy |
|---|---|---|---|
| Deep Surgical Site Infection / Osteomyelitis | 2% (Closed) to >20% (Type IIIB Open) | Retained necrotic tissue, severe contamination, inadequate soft tissue coverage. | Radical repeat debridement, removal of loose hardware, local antibiotic delivery (cement spacers), systemic antibiotics, eventual soft tissue flap coverage. |
| Acute Compartment Syndrome | 2% - 9% (Tibial Diaphysis) | Increased pressure within a closed fascial space compromising microvascular perfusion. | Emergent 4-compartment fasciotomy. Delayed closure or split-thickness skin grafting once swelling resolves. |
| Aseptic Non-Union | 5% - 10% (Long Bones) | Inadequate mechanical stability (hypertrophic) or compromised biology/vascularity (atrophic). | Revision fixation (exchange nailing or plating). Autologous bone grafting, decortication, or application of orthobiologics (BMPs). |
| Fat Embolism Syndrome (FES) | 1% - 3% (Major Long Bone Trauma) | Marrow fat entering venous circulation, causing mechanical obstruction and biochemical endothelial damage. | Supportive ICU care, lung-protective mechanical ventilation, maintenance of hemodynamics. Prevention via early fracture stabilization. |
| Post-Traumatic Arthrosis | High in intra-articular fractures | Articular step-off > 2mm, cartilage necrosis, altered joint biomechanics. | Conservative management initially (injections, bracing). Definitive salvage via arthrodesis (joint fusion) or total joint arthroplasty. |
| Amputation (Mangled Extremity) | Variable (Dependent on severity) | Irreversible ischemia (>8 hrs), irreparable nerve injury, massive soft tissue/bone loss. | Formal amputation at the lowest viable functional level. Targeted muscle reinnervation (TMR) to prevent neuromas. Prosthetic fitting. |
Phased Post-Operative Rehabilitation Protocols
The rehabilitation of the polytraumatized patient is not a passive, delayed phase of care; it is an active, highly structured process that begins immediately upon admission to the intensive care unit. The ultimate goal is the restoration of pre-injury functional status, a process that requires months to years of dedicated multidisciplinary effort involving orthopaedic surgeons, physical therapists, occupational therapists, physiatrists, and psychological support teams.
The initial ICU Phase (Days 0-7) is focused on physiological optimization and the prevention of the complications of recumbency. Strict deep vein thrombosis (DVT) prophylaxis is initiated as soon as the bleeding risk is mitigated, utilizing low-molecular-weight heparin (LMWH) and mechanical sequential compression devices. Pulmonary toilet, incentive spirometry, and early upright positioning are critical to preventing ventilator-associated pneumonia and ARDS. From an orthopaedic standpoint, the focus is on maintaining joint mobility outside the zone of injury. Passive range of motion (ROM) exercises are initiated for uninjured joints to prevent contractures. For extremities stabilized with external fixators, meticulous pin-site care protocols are implemented to prevent superficial infections from tracking deep into the bone.
The Transition Phase (Weeks 1-4) typically coincides with the conversion of damage control external fixators to definitive internal fixation. Once definitive stability is achieved, the rehabilitation protocol shifts toward active and active-assisted range of motion. The weight-bearing status is strictly dictated by the fracture pattern, the quality of the host bone, and the biomechanical strength of the surgical construct. For rigidly fixed diaphyseal fractures utilizing locked intramedullary nails, early weight-bearing as tolerated is often encouraged to stimulate callus formation through cyclic axial loading. Conversely, complex periarticular fractures managed with plates and screws require a prolonged period of strict non-weight-bearing or touch-down weight-bearing (typically 8 to 12 weeks) to prevent catastrophic hardware failure or articular subsidence before biological healing occurs.
The Mobilization and Strengthening Phase (Months 1-6) focuses on restoring muscle mass, proprioception, and gait mechanics. Hydrotherapy is highly beneficial in the early stages, allowing for buoyancy-assisted range of motion and partial weight-bearing. Progressive resistance training is introduced as radiographic evidence of fracture consolidation appears. Occupational therapy plays a vital role in upper extremity trauma, focusing on fine motor skills, grip strength, and the performance of activities of daily living (ADLs).
The Long-Term Functional Phase (Months 6+) addresses the chronic sequelae of massive trauma. The orthopaedic surgeon must remain vigilant for the late development of post-traumatic arthrosis, chronic regional pain syndrome (CRPS), or delayed non-unions. Furthermore, the psychological impact of polytrauma cannot be overstated. A significant percentage of these patients develop post-traumatic stress disorder (PTSD), severe depression, and chronic anxiety. Routine screening and early referral to psychiatric and psychological support services are essential components of comprehensive orthopaedic trauma care, as untreated psychological morbidity is a primary predictor of poor physical functional recovery.
Summary of Landmark Literature and Clinical Guidelines
The evolution of orthopaedic trauma management is deeply rooted in rigorous clinical research and paradigm-shifting landmark studies. The modern orthopaedic surgeon must practice evidence-based medicine, utilizing these foundational texts to guide complex decision-making.
The classification and management of open fractures have been fundamentally altered by recent literature. While the Gustilo-Anderson classification remains ubiquitous, the Orthopaedic Trauma Association (OTA) 2010 Open Fracture Classification provides a more granular, objective, and reproducible system. By independently grading the Skin (approximable, non-approximable, degloving), Muscle (viable, localized necrosis, dead/loss of function), Arterial injury (none, without ischemia, with ischemia), Contamination (minimal, surface, embedded/high-risk), and Bone Loss, the OTA system offers superior prognostic value for predicting amputation risk and infection rates, guiding more precise surgical interventions.
The dogma of the "6-hour rule" for the debridement of open fractures has been thoroughly debunked by contemporary evidence. Landmark systematic reviews and massive retrospective analyses have definitively demonstrated that delaying surgical debridement up to 24 hours does not increase the risk of deep infection or non-union, provided that the patient receives early, appropriate intravenous antibiotics. This paradigm shift allows complex open fractures to be managed by dedicated, rested orthopaedic trauma teams during daylight hours, rather than by fatigued personnel in the middle of the night, thereby significantly improving the quality of the debridement and the overall surgical outcome.
The management of the wound itself was revolutionized by the Fluid Lavage of Open Wounds (FLOW) trial. This massive, multicenter randomized controlled trial definitively established that low-pressure irrigation is superior to high-pressure pulsatile lavage, and that the addition of castile soap provides no benefit over normal saline, and may indeed be deleterious to cellular viability. This study standardized the global approach to open fracture irrigation.
Antibiotic stewardship in open fracture management is governed by guidelines from the Eastern Association for the Surgery of Trauma (EAST) and the Surgical Infection Society. The critical determinant of success is the rapid administration of prophylactic antibiotics, ideally within 1 to 2 hours of injury. For Type I and II open fractures, a first-generation cephalosporin (e.g., Cefazolin) is standard. For Type III fractures, the addition of Gram-negative coverage (e.g., Ceftriaxone or Gentamicin) is indicated. High-dose Penicillin is reserved for specific high-risk environments (e.g., agricultural injuries with gross fecal contamination) to prevent Clostridium perfringens gas gangrene. Crucially, the duration of antibiotic therapy has been drastically shortened; current guidelines strongly advocate for the discontinuation of prophylactic antibiotics within 24 to 48 hours of definitive wound closure, as prolonged administration breeds multidrug-resistant organisms without reducing the incidence of surgical site infections.
Finally, the Lower Extremity Assessment Project (LEAP) study remains the definitive body of literature regarding the mangled extremity. This prospective, multicenter study evaluated patients with severe lower extremity trauma to determine the outcomes of limb salvage versus early amputation. The LEAP study famously demonstrated that, at long-term follow-up (2 to 7 years), there was no significant difference in functional outcomes, psychological distress, or return to work between patients who underwent successful limb salvage and those who underwent early amputation. This profound finding emphasizes that the decision to amputate or salvage must be highly individualized, considering not only the anatomical severity of the injury but also the patient's physiological reserve, socioeconomic support, and personal goals, reinforcing the art and science of orthopaedic trauma surgery.
