Muscle and Musculocutaneous Free Flaps: Principles and Surgical Techniques
Key Takeaway
Muscle and musculocutaneous free flaps are essential for reconstructing complex soft tissue defects and restoring functional neuromuscular units in the extremities. The latissimus dorsi flap offers robust coverage with a reliable thoracodorsal pedicle, while the lateral arm flap provides versatile fasciocutaneous tissue. This guide details the vascular anatomy, precise surgical harvest techniques, and postoperative microvascular monitoring protocols required for successful free tissue transfer in orthopaedic reconstructive surgery.
Comprehensive Introduction and Patho-Epidemiology
The advent of microvascular surgery and the subsequent evolution of free tissue transfer have fundamentally revolutionized the orthopaedic approach to complex extremity reconstruction. Historically, the management of massive soft tissue defects—particularly those associated with high-energy open fractures, extensive tumor resections, or chronic osteomyelitis—was limited to primary amputation or prolonged, often unsuccessful, attempts at secondary intention healing. Today, muscle and musculocutaneous free flaps serve as the cornerstone of the "reconstructive elevator," allowing surgeons to bypass the traditional reconstructive ladder and immediately provide robust, highly vascularized coverage to ischemic, infected, or structurally deficient recipient beds. This paradigm shift has dramatically improved limb salvage rates, functional outcomes, and patient quality of life.
The patho-epidemiology of defects requiring free tissue transfer is predominantly rooted in high-energy trauma, oncologic resection, and chronic infectious processes. In the realm of trauma, Gustilo-Anderson Type IIIB and IIIC open fractures represent the most frequent indications for microvascular muscle flaps. These injuries are characterized by extensive periosteal stripping, massive soft tissue avulsion, and a profound localized zone of injury that compromises the regional microcirculation. The resulting ischemic environment is highly conducive to bacterial colonization and biofilm formation, rendering local fasciocutaneous flaps inadequate or entirely unavailable. Muscle flaps, by virtue of their dense capillary networks and high oxygen delivery capacity, effectively obliterate dead space, deliver vital immunologic mediators (such as polymorphonuclear leukocytes and macrophages), and reverse the localized hypoxia that perpetuates chronic osteomyelitis.
Beyond traumatic soft tissue coverage, muscle free flaps are indispensable in the realm of Functional Muscle Transfer (FMT). The epidemiology of paralyzing conditions—ranging from devastating brachial plexus avulsions and Volkmann’s ischemic contractures to radical tumor extirpations—demands reconstructive solutions that replace irreparably damaged neuromuscular units. By transferring a muscle with its native motor nerve and meticulously coapting it to a functional recipient nerve, surgeons can restore dynamic function to an otherwise flail limb. The physiological behavior of these transferred tissues is highly predictable; non-reinnervated muscle flaps will undergo denervation atrophy, losing up to fifty percent of their initial bulk, which is often aesthetically advantageous in extremity reconstruction. Conversely, reinnervated functional transfers maintain their cross-sectional area and contractile properties, provided that tensioning and synergistic rehabilitation are optimally managed.
The selection between a pure muscle flap covered with a split-thickness skin graft versus a composite musculocutaneous flap requires a nuanced understanding of the defect's patho-anatomy. While musculocutaneous flaps provide native skin coverage, they can be excessively bulky and possess a propensity for shear forces at the subcutaneous interface. In contrast, a muscle flap with a skin graft contours impeccably to complex, three-dimensional extremity defects—such as the distal third of the tibia or the dorsal hand—and provides superior vascularity to the recipient bed. Understanding these fundamental principles, alongside the epidemiological drivers of complex tissue loss, is paramount for the reconstructive orthopaedic surgeon tasked with preserving limb and life.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of vascular anatomy and muscle biomechanics is the absolute prerequisite for successful microvascular tissue transfer. The foundational framework for understanding muscle flaps is the Mathes and Nahai classification, which categorizes muscles based on their pattern of vascular supply. This classification ranges from Type I (one vascular pedicle, e.g., tensor fascia lata) to Type V (one dominant pedicle and secondary segmental pedicles, e.g., latissimus dorsi). Understanding these vascular patterns dictates not only the harvest technique but also the safe limits of the skin paddle and the absolute length of the vascular pedicle available for microvascular anastomosis.
The latissimus dorsi, classified as a Type V muscle flap, remains the premier workhorse in orthopaedic reconstructive microsurgery. Originating from the posterior layer of the thoracolumbar fascia, the posterior iliac crest, and the lower three or four ribs, its expansive fan-like fibers converge superolaterally to insert on the inferior portion of the bicipital groove of the humerus. The dominant vascular supply is the thoracodorsal artery, a direct continuation of the subscapular artery, which itself branches from the third part of the axillary artery. The thoracodorsal artery enters the deep surface of the muscle approximately 8 to 12 centimeters distal to the humeral insertion. If dissected proximal to the circumflex scapular artery takeoff, the pedicle yields an exceptional vessel diameter of 1.5 to 3.0 millimeters and a length of up to 15 centimeters, making it highly amenable to microvascular anastomosis outside the zone of injury.
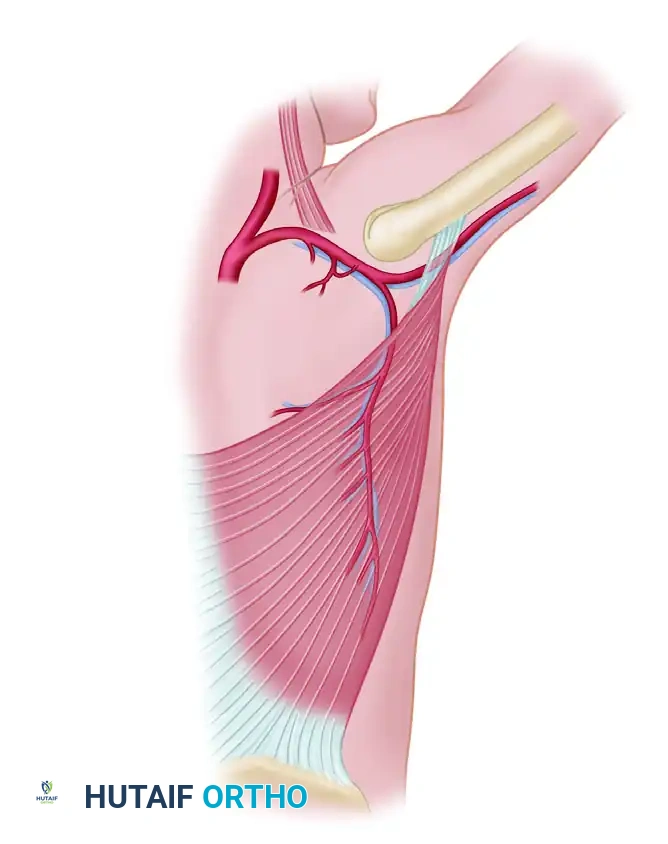
For defects requiring thinner, pliable, and potentially sensate tissue, the lateral arm free flap represents a highly versatile septocutaneous option. The vascular basis of this flap is the posterior radial collateral artery (PRCA), a terminal branch of the profunda brachii artery. The PRCA courses distally within the lateral intermuscular septum of the arm, sandwiched between the brachialis and brachioradialis anteriorly, and the triceps posteriorly. The flap can be harvested as a pure fasciocutaneous unit, or as a composite flap incorporating a segment of the lateral humerus or triceps tendon. Sensory innervation is robust, provided by the posterior cutaneous nerve of the arm and the posterior cutaneous nerve of the forearm, allowing for the restoration of protective sensibility in critical weight-bearing or tactile areas, such as the plantar foot or the palmar hand.
The biomechanics of muscle transfer—particularly in the context of Functional Muscle Transfer—require meticulous attention to the Blix curve, which defines the relationship between muscle length and active tension generation. A transferred muscle will only generate optimal contractile force if it is inset at its precise physiological resting length. If inset too loosely, the muscle operates on the ascending limb of the length-tension curve, resulting in profound weakness and inadequate excursion. If inset under excessive tension, it operates on the descending limb, leading to fibrosis, ischemia, and eventual failure of the neuromuscular unit. Furthermore, the surgeon must calculate the required excursion; the latissimus dorsi, for example, possesses an inherent excursion of approximately 8 to 10 centimeters, making it biomechanically ideal for replacing the biceps brachii for elbow flexion, or the extrinsic finger flexors in the forearm.
Exhaustive Indications and Contraindications
The decision to perform a microvascular muscle or musculocutaneous free flap must be predicated on a rigorous evaluation of the patient's systemic physiologic reserve, the precise nature of the local defect, and the availability of viable donor and recipient vessels. The indications for these complex procedures are broad but highly specific, encompassing the most challenging clinical scenarios encountered in orthopaedic trauma, oncology, and infection management.
| Category | Specific Clinical Scenarios | Rationale for Free Tissue Transfer |
|---|---|---|
| Trauma | Gustilo-Anderson Type IIIB/IIIC open fractures (especially distal 1/3 of tibia); Massive degloving injuries; Traumatic amputations requiring stump preservation. | Eradicates dead space; provides highly vascularized tissue to ischemic bone; covers exposed orthopaedic hardware, tendons, and neurovascular structures; facilitates primary bone healing. |
| Infection | Chronic osteomyelitis (Cierny-Mader Types III and IV); Infected non-unions; Septic arthritis with massive joint destruction. | Delivers high concentrations of systemic antibiotics and immune cells to the avascular focus; improves local tissue oxygen tension; allows for radical debridement of infected bone and soft tissue. |
| Oncology | Post-sarcoma resection defects; Radiation-induced tissue necrosis; Exposed endoprostheses following limb salvage surgery. | Replaces irradiated, fibrotic tissue with healthy, well-perfused muscle; provides massive bulk to fill post-extirpative dead space; protects massive metallic implants from exposure and secondary infection. |
| Functional Deficits | Brachial plexus avulsion injuries; Volkmann’s ischemic contracture; Chronic massive rotator cuff tears; Facial nerve palsy. | Restores dynamic motor function via Functional Muscle Transfer (FMT); replaces irreversibly fibrotic or denervated muscle groups; provides active joint stabilization. |
Despite their immense utility, free flaps are subject to strict contraindications. Absolute contraindications include profound systemic instability, such as irreversible hemorrhagic shock, severe uncorrected coagulopathy, or overwhelming systemic sepsis, where the physiological insult of a prolonged microvascular procedure would be life-threatening. Furthermore, the absence of viable recipient vessels—often secondary to severe peripheral arterial disease (PAD), extensive crush injury, or prior multilevel venous thrombosis—precludes free tissue transfer. In such cases, the surgeon must resort to pedicled flaps, cross-leg flaps, or ultimately, amputation.
Relative contraindications require careful multidisciplinary consideration. Advanced patient age alone is not a contraindication; however, the cumulative burden of medical comorbidities (e.g., poorly controlled diabetes mellitus, end-stage renal disease, severe cardiopulmonary compromise) significantly increases the risk of perioperative mortality and flap failure. Active tobacco use is a profound relative contraindication due to nicotine-induced peripheral vasospasm, endothelial dysfunction, and impaired microcirculatory flow. Most microsurgical centers require strict smoking cessation for a minimum of four to six weeks prior to elective free tissue transfer. Additionally, prior radiation therapy to the proposed donor site or extensive prior surgical dissection in the anticipated vascular territory may compromise the integrity of the donor pedicle, necessitating the selection of an alternative flap.
Pre-Operative Planning, Templating, and Patient Positioning
The success of a microvascular free flap is unequivocally determined long before the initial incision is made. Meticulous pre-operative planning, advanced imaging, and strategic patient positioning are critical to minimizing ischemic time, preventing intraoperative catastrophes, and ensuring optimal functional and aesthetic outcomes. The process begins with a comprehensive assessment of the recipient site, characterizing the true extent of the defect following anticipated radical debridement.
Vascular imaging of the recipient extremity is mandatory in the setting of high-energy trauma, severe peripheral vascular disease, or prior failed reconstructions. Computed Tomography Angiography (CTA) has largely replaced conventional catheter-based angiography as the gold standard for mapping the lower extremity arterial tree. CTA provides high-resolution, three-dimensional reconstructions that allow the surgeon to identify the zone of injury, assess the patency of the anterior tibial, posterior tibial, and peroneal vessels, and determine the optimal site for microvascular anastomosis. In cases where CTA is contraindicated due to severe renal impairment, Magnetic Resonance Angiography (MRA) or advanced duplex ultrasonography may be utilized. Concurrently, the donor site must be evaluated; handheld acoustic Doppler or color duplex ultrasonography is routinely employed to map the precise location of musculocutaneous perforators, ensuring they are safely captured within the designed skin paddle.
Templating the defect is a critical step that bridges the gap between the recipient and donor sites. Following radical debridement of the recipient bed, a three-dimensional template is created using sterile foil, surgical towels, or specialized foam. This template must account not only for the surface area of the skin defect but also for the volumetric requirements of the dead space. The template is then transferred to the donor site (e.g., the lateral thorax for a latissimus dorsi flap). The surgeon must orient the template to ensure that the vascular pedicle will easily reach the selected recipient vessels without tension, kinking, or torsion. The "lifeboat" principle must also be established during this phase; the surgical team must have a predetermined secondary reconstructive option (e.g., an alternative free flap or a pedicled flap) immediately available should the primary plan fail due to anatomical anomalies or intraoperative vascular injury.
Patient positioning is a highly orchestrated procedure designed to facilitate a simultaneous two-team approach, thereby drastically reducing total operative time and flap ischemia. For a latissimus dorsi harvest destined for a lower extremity defect, the patient is typically placed in a secure lateral decubitus position. A vacuum-activated beanbag, supplemented with kidney rests and an axillary roll, ensures rigid stability. The ipsilateral arm is prepped and draped free, allowing the donor-site surgeon to passively manipulate the shoulder to open the axilla and facilitate proximal pedicle dissection. Simultaneously, the recipient-site surgeon operates on the dependent or elevated lower extremity. Meticulous padding of all bony prominences and strict attention to neutral alignment of the cervical and lumbar spine are imperative to prevent catastrophic perioperative neuropathies or pressure-induced myonecrosis during these prolonged procedures.
Step-by-Step Surgical Approach and Fixation Technique
The execution of a microvascular free flap demands unparalleled surgical precision, combining aggressive orthopaedic debridement with delicate microsurgical tissue handling. The procedure is divided into four distinct phases: recipient site preparation, flap harvest, microvascular anastomosis, and final inset and fixation. The overarching goal is to minimize flap ischemia time while ensuring a mechanically stable, well-perfused reconstruction.
Recipient Site Preparation and Vessel Exposure:
The recipient site is first subjected to radical, oncologic-style debridement. All devitalized bone, fibrotic soft tissue, and infected material must be excised until punctate cortical bleeding (the "paprika sign") is observed. Following debridement, the recipient vessels are explored outside the zone of traumatic injury. For lower extremity defects, the posterior tibial or anterior tibial vessels are typically isolated. The perivascular adventitia is meticulously stripped under operating microscope magnification. The vessels are assessed for intimal damage, which manifests as a bruised, thickened, or delaminated vessel wall; anastomosis to damaged intima guarantees catastrophic thrombosis. Once healthy, pulsatile vessels are isolated, they are controlled with double-loop vessel loops and bathed in topical vasodilators (e.g., papaverine or verapamil) to prevent spasm.
Flap Harvest (Latissimus Dorsi Example):
With the patient in the lateral decubitus position, the skin paddle is incised, and the subcutaneous tissue is elevated off the latissimus fascia. The anterior border of the muscle is identified, and the areolar plane between the latissimus dorsi and the serratus anterior is bluntly developed. The thoracodorsal neurovascular bundle is identified on the deep surface of the muscle. The pedicle is traced proximally into the axilla, requiring the ligation of the serratus anterior branch and, if maximal length is needed, the circumflex scapular artery. The muscle is then divided from its inferior, posterior, and superior attachments. The humeral insertion is transected last. The flap is left attached solely by its vascular pedicle and allowed to perfuse for 20 minutes. Once the recipient site is fully prepared, the pedicle is ligated, and the flap is transferred to the defect.
Microvascular Anastomosis:
The flap is provisionally secured to the recipient bed using a few strategic tacking sutures to prevent inadvertent traction on the pedicle. Under the operating microscope, the arterial anastomosis is typically performed first to minimize warm ischemia time. An end-to-end or end-to-side anastomosis is performed using 8-0 or 9-0 nylon sutures in an interrupted fashion. The venous anastomosis follows; modern microsurgery heavily relies on mechanical venous coupling devices (e.g., Synovis couplers), which provide a rapid, highly reliable intima-to-intima coaptation and have been shown to significantly reduce venous thrombosis rates compared to hand-sewn techniques. Once the anastomoses are complete, the microvascular clamps are released. The surgeon must observe immediate, robust arterial pulsation within the pedicle, rapid capillary refill in the skin paddle or muscle belly, and brisk venous return without engorgement.
Flap Inset and Orthopaedic Fixation:
The final inset is critical to both the survival of the flap and the functional outcome of the limb. If underlying skeletal instability exists, orthopaedic fixation (typically an external fixator or low-profile internal plating) must be definitively applied prior to flap inset. The muscle is then draped over the hardware and bone, ensuring absolute obliteration of dead space. The muscle fascia is sutured to the adjacent healthy fascia of the recipient bed using interrupted absorbable sutures. Crucially, the inset must be completely tension-free; any compression over the vascular pedicle or tight closure of the overlying skin will lead to immediate venous congestion. If a pure muscle flap was harvested, a meshed split-thickness skin graft is applied directly to the raw muscle surface and secured with surgical staples. Closed suction drains are placed strategically beneath the flap, ensuring they do not cross or lie adjacent to the microvascular anastomoses.
Complications, Incidence Rates, and Salvage Management
Despite meticulous technique and advanced technology, microvascular free tissue transfer carries inherent risks. Complications can be broadly categorized into acute microvascular failures, subacute wound healing issues, and long-term donor or recipient site morbidities. The ability to rapidly recognize and aggressively manage these complications is the defining characteristic of a proficient microsurgeon.
| Complication | Estimated Incidence | Etiology and Clinical Presentation | Salvage Management and Intervention |
|---|---|---|---|
| Arterial Thrombosis | 1% - 3% | Usually secondary to technical error (suture catching back wall), intimal damage, or profound vasospasm. Presents as a pale, cool flap with absent capillary refill and loss of Doppler signal. | Immediate surgical emergency. Return to OR for re-exploration, thrombectomy, resection of the anastomotic site, and revision with a reversed interpositional vein graft (e.g., saphenous vein). |
| Venous Congestion | 2% - 5% | Caused by pedicle kinking, tight inset, hematoma compression, or venous coupler failure. Presents as a swollen, purple/blue flap with brisk, dark capillary refill and rapid bleeding upon pinprick. | Release tight sutures immediately at the bedside. If unresolved, return to OR for hematoma evacuation and anastomotic revision. Medicinal leeches (Hirudo medicinalis) may be used for temporary venous outflow relief. |
| Partial Flap Necrosis | 5% - 10% | Distal hypoperfusion, often seen in massive flaps where the distal tip extends beyond the reliable angiosome or perforator territory. | Demarcation allowed to occur over 1-2 weeks, followed by sharp debridement of necrotic tissue and secondary skin grafting or local tissue rearrangement. |
| No-Reflow Phenomenon | < 1% | Severe ischemia-reperfusion injury leading to microcirculatory collapse despite a patent macrovascular anastomosis. | Administration of systemic thrombolytics (tPA), intra-arterial vasodilators (verapamil, papaverine), and aggressive systemic hydration. Prognosis for flap survival is poor. |
| Donor Site Seroma | 10% - 15% | Common in latissimus dorsi harvests due to the massive dead space and disruption of extensive lymphatic networks in the axilla. | Prolonged use of closed suction drains. If drains are removed, serial percutaneous aspirations or re-insertion of a drain under ultrasound guidance. Sclerotherapy is rarely required. |
The critical window for microvascular failure is the first 48 to 72 hours postoperatively. Clinical monitoring remains the gold standard; however, adjunctive technologies such as implantable venous Doppler probes and Near-Infrared Spectroscopy (NIRS) have dramatically reduced the time to detection of vascular compromise. NIRS, in particular, provides real-time, continuous monitoring of regional tissue oxygen saturation (rStO2). A rapid drop of more than 20 points from baseline, or an absolute value below 30%, is highly sensitive for impending vascular occlusion and mandates immediate clinical correlation and potential re-exploration.
When re-exploration is required, the concept of "time is tissue" dictates the outcome. If arterial thrombosis is identified, the anastomosis must be aggressively resected back to healthy, uninjured intima. Simple thrombectomy is rarely sufficient, as the underlying intimal defect will inevitably propagate a new thrombus. The use of an interpositional vein graft—harvested from the ipsilateral greater saphenous vein or the lesser saphenous vein—is frequently necessary to bridge the resulting gap without tension. In cases of venous congestion that cannot be immediately revised surgically, the application of medicinal leeches (Hirudo medicinalis) provides powerful local anticoagulation via hirudin and active mechanical decongestion. Prophylactic antibiotics covering Aeromonas hydrophila (e.g., ciprofloxacin or trimethoprim-sulfamethoxazole) are absolutely mandatory when leech therapy is initiated to prevent devastating flap infections.
Phased Post-Operative Rehabilitation Protocols
The postoperative management of a patient following microvascular free tissue transfer is a highly structured, multidisciplinary endeavor. The rehabilitation protocol must balance the absolute necessity of protecting the fragile microvascular anastomoses with the orthopaedic imperatives of preventing joint contractures, mitigating deep vein thrombosis, and promoting early functional recovery. The protocol is generally divided into three distinct phases: the acute microvascular phase, the subacute mobilization phase, and the long-term functional integration phase.
Phase 1: Acute Microvascular Phase (Days 0 to 7)
The primary objective during the first week is flap survival. The patient is typically managed in a specialized microsurgical intensive care unit or step-down unit. The ambient room temperature is maintained above 24°C to prevent peripheral vasospasm. The reconstructed extremity is elevated slightly above the level of the heart to promote venous drainage, but strict precautions are taken to ensure the limb is immobilized in a neutral position, preventing any torsion or pressure over the pedicle. Core body temperature, hydration status, and urine output are rigorously optimized. Anticoagulation protocols vary, but a standard regimen includes daily low-dose aspirin (81 mg), subcutaneous prophylactic heparin or enoxaparin, and aggressive intravenous hydration. For lower extremity flaps, absolute bed rest is maintained for the first 5 to 7 days. Range of motion exercises are strictly limited to joints completely uninvolved with the flap or pedicle.
Phase 2: Subacute Mobilization and "Dangling" (Days 7 to 21)
Once the microvascular anastomoses have stabilized and the critical window for thrombosis has closed, the focus shifts to controlled mobilization. For lower extremity free flaps, the introduction of gravity dependency is the most critical hurdle. A structured "dangling protocol" is initiated to gradually condition the flap's microvasculature to venous hydrostatic pressure. On day 7, the extremity is wrapped in a light, non-compressive elastic bandage and allowed to hang dependent for 5 minutes. The flap is closely observed for signs of severe venous engorgement. If tolerated, the limb is elevated, and the dangling duration is incrementally increased by 5 minutes twice daily. By day 14, the patient should tolerate 30 to 45 minutes of dependency, allowing for the initiation of pivot transfers and partial weight-bearing with assistive devices, dictated by the underlying orthopaedic bony stability. Concurrently, aggressive physical therapy is initiated for the donor site to prevent adhesive capsulitis of the shoulder (in latissimus dorsi harvests) or elbow stiffness (in lateral arm harvests).
Phase 3: Long-Term Functional Integration (Weeks 3 to 12+)
The final phase of rehabilitation is tailored to the specific nature of the reconstruction. For standard coverage flaps, the focus is on progressive weight-bearing, gait training, and the transition to custom-molded orthotics or specialized footwear to protect the insensate or newly grafted tissue. Compression garments are frequently prescribed to manage chronic lower extremity edema and assist in contouring the bulky muscle flap. For Functional Muscle Transfers (FMT), this phase is profoundly complex. Reinnervation occurs at a rate of approximately 1 millimeter per day; thus, clinical signs of muscle contraction may not be evident for 3 to 6 months. During this waiting period, passive range of motion is critical to prevent joint contractures. Once trace active contraction is noted, biofeedback therapy, electrical stimulation, and targeted synergistic strengthening protocols are employed to train the brain to utilize the transferred muscle in its new biomechanical role. Maximum functional recovery following FMT often requires 18 to 24 months of dedicated, intensive rehabilitation.
Summary of Landmark Literature and Clinical Guidelines
The contemporary practice of microvascular free tissue transfer in orthopaedic surgery is deeply rooted in decades of rigorous clinical research and landmark publications. Understanding this literature is essential for evidence-based decision-making and optimal patient outcomes.
The foundational principles of timing in microvascular reconstruction were established by Marko Godina in his seminal 1986 publication. Godina demonstrated that early free flap coverage (within 72 hours of injury) of severe open lower extremity fractures resulted in dramatically lower rates of flap failure, infection, and non-union compared to delayed reconstruction. While modern damage-control orthopaedics and the advent of negative pressure wound therapy (NPWT) have slightly expanded this strict window, the "fix and flap" philosophy—advocating for definitive skeletal fixation and soft tissue coverage within the first 5 to 7 days—remains the gold standard supported by the British Orthopaedic Association (BOA) and the British Association of Plastic, Reconstructive and Aesthetic Surgeons (BAPRAS) joint guidelines.
The Lower Extremity Assessment Project (LEAP) study, a massive multicenter prospective cohort, fundamentally altered the debate between limb salvage and primary amputation. The LEAP study demonstrated that while successful limb salvage using free tissue transfer is highly achievable, the long-term functional outcomes and psychological impact at two and seven years are statistically comparable to early below-knee amputation. This landmark data underscores the necessity of shared decision-making; the technical ability to perform a microvascular muscle flap does not mandate its execution if the patient's long-term functional goals, socioeconomic support, and psychological resilience are better served by amputation and advanced prosthetics.
Regarding flap selection, the debate between muscle and fasciocutaneous flaps continues to evolve. Historically, muscle flaps (e.g., latissimus dorsi, rectus abdominis) were considered universally superior for infected beds and open fractures due to their high vascular density. However, recent comparative studies and meta-analyses have shown that modern perforator-based fasciocutaneous flaps (e.g., Anterolateral Thigh flap) achieve equivalent limb salvage and infection eradication rates in many extremity defects, while offering the advantages of reduced donor site morbidity and improved contouring without the need for skin grafting. Nevertheless, established clinical guidelines maintain that for massive cavitary defects, extensive areas of exposed orthopaedic hardware, and chronic Cierny-Mader Type IV osteomyelitis, the superior bulk and biological activity of a microvascular muscle flap remain unsurpassed.
