Mastering Trauma Principles: Damage Control Orthopaedics and Polytrauma Management

Key Takeaway
The management of polytrauma requires a multidisciplinary approach centered on rapid physiological stabilization and strategic fracture management. This guide details the critical transition from Early Total Care (ETC) to Damage Control Orthopaedics (DCO), emphasizing the mitigation of the systemic immune response syndrome (SIRS). It provides evidence-based protocols for soft-tissue classification, compartment syndrome evaluation, and the precise application of temporary external fixation to optimize patient survival and functional recovery.
Comprehensive Introduction and Patho-Epidemiology
The treatment of patients with multiple trauma requires highly specialized resources, multidisciplinary coordination, and rapid physiological assessment—capabilities that are fundamentally centralized within designated Level I and Level II trauma centers. The acute stabilization of long bone, pelvic, and spinal fractures must adhere to stringent, evidence-based trauma center protocols to mitigate mortality and morbidity. The centralization of trauma care has yielded dramatic epidemiological shifts over the past several decades. For instance, following the development of highly organized trauma systems globally, mortality from polytrauma plummeted significantly; historical data from Germany demonstrated a reduction in polytrauma mortality from 40% in 1972 to 18% in 1991. Similarly, in regionalized systems like San Diego County, overall mortality decreased from 26% to 8%, with concomitant drastic reductions in suboptimal assessment, delayed evaluation, and delayed treatment. Beyond mortality benefits, the length of hospital stay and the overall cost of treatment are significantly lower in patients triaged directly to trauma centers. Therefore, immediate referral to a dedicated trauma center remains the undisputed gold standard for the management of multiply-injured patients.

At the core of initial polytrauma management is the Advanced Trauma Life Support (ATLS) protocol, developed by the American College of Surgeons. This universal standard dictates a primary survey based on the ABCDE mnemonic: Airway protection with cervical spine control, Breathing and ventilation, Circulation with hemorrhage control, Disability (neurological status), and Exposure/Environmental control. However, an estimated 5% to 20% of patients with multiple trauma have injuries that are missed during the initial primary survey due to altered consciousness, profound hemodynamic instability, distracting injuries, or inadequate initial radiographs. This necessitates a formal, rigorous tertiary survey once the patient is physiologically stabilized. The initial physiological derangement following high-energy trauma is driven by massive tissue disruption, which activates cellular factors exerting profound systemic effects. This diffuse inflammatory reaction is clinically recognized as Systemic Inflammatory Response Syndrome (SIRS).
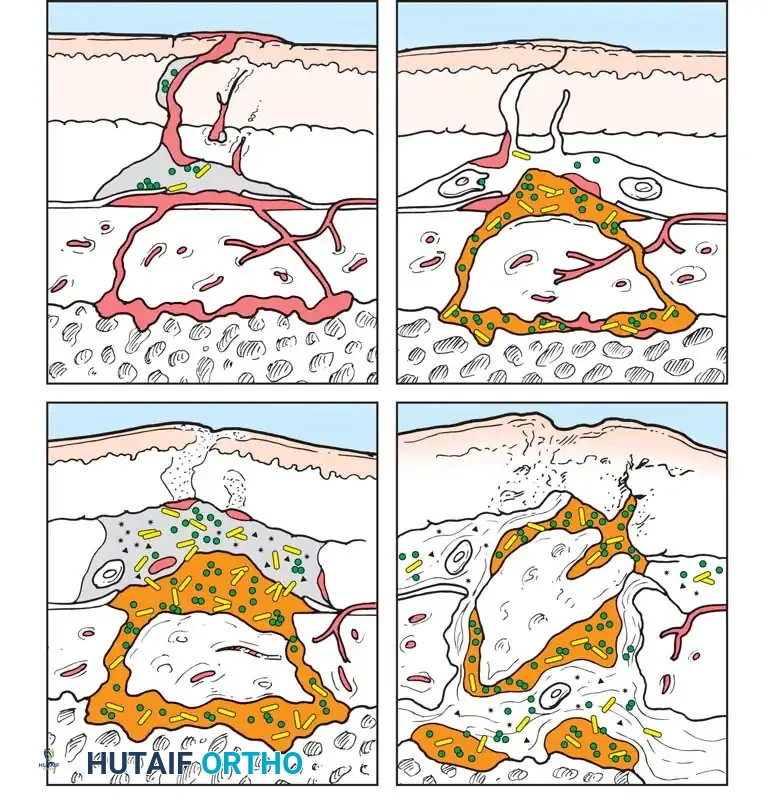
The pathophysiology of polytrauma is best understood through the paradigm of the "First Hit" and "Second Hit." The initial trauma serves as the "First Hit," priming the patient's innate immune system and triggering a massive release of inflammatory cytokines, most notably Interleukin-6 (IL-6), Interleukin-1 (IL-1), and Tumor Necrosis Factor-alpha (TNF-α). Polymorphonuclear neutrophils are sequestered in the pulmonary microvasculature, rendering the lungs highly susceptible to further insult. Subsequent prolonged surgical interventions, such as the definitive intramedullary nailing of bilateral femur fractures, act as a "Second Hit." The intramedullary reaming process releases marrow fat, micro-thrombi, and additional inflammatory mediators into the systemic circulation. In a physiologically exhausted patient, this "Second Hit" hyperactivates the primed immune system, leading to a catastrophic cytokine storm, endothelial damage, capillary leak syndrome, Acute Respiratory Distress Syndrome (ARDS), Multiple Organ Dysfunction Syndrome (MODS), and potentially death.
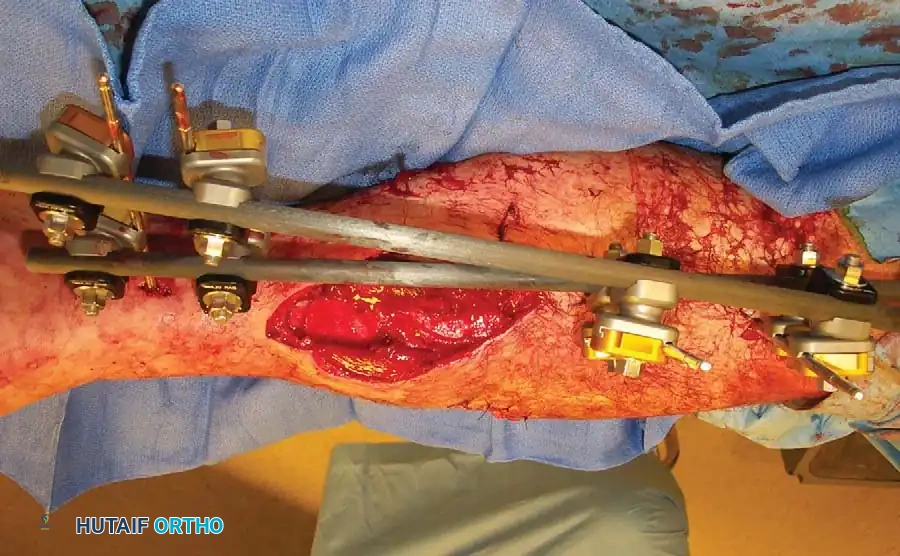
This profound understanding of the immune response catalyzed a paradigm shift in trauma orthopaedics. From the early 1990s, the prevailing philosophy was Early Total Care (ETC), which advocated for the definitive stabilization of all major fractures within the first 24 hours to reduce pulmonary complications. However, as the "Second Hit" phenomenon was elucidated, it became evident that ETC is severely detrimental to hemodynamically unstable or "borderline" patients. This realization birthed Damage Control Orthopaedics (DCO), a strategy involving the rapid, temporary immobilization of fractures—typically via external fixation—to obtain mechanical stability, control hemorrhage, and recover limb length, while strictly minimizing surgical time and physiological burden. Operative treatment for definitive fixation must never be undertaken if hemodynamic stabilization is not achieved, if life-threatening coagulopathy or acidosis persists, or if the patient requires escalating vasopressor support.
Detailed Surgical Anatomy and Biomechanics
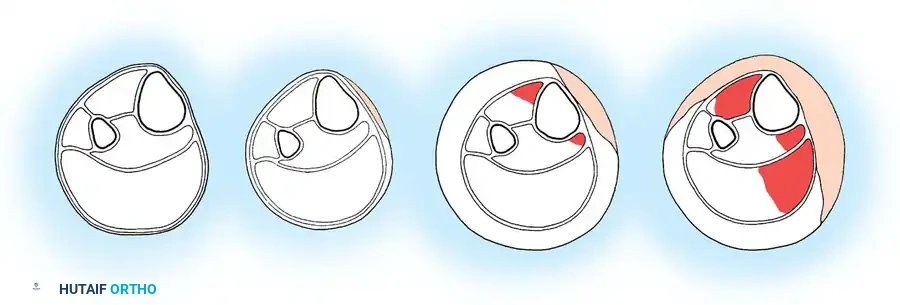
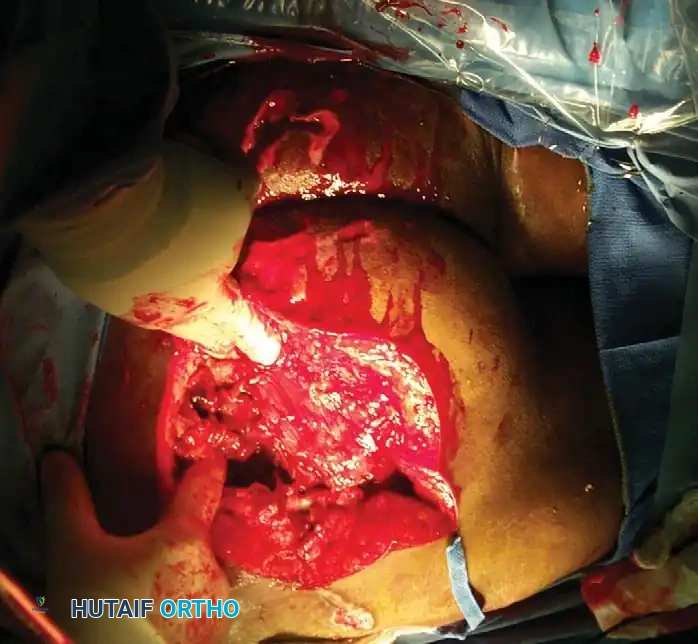
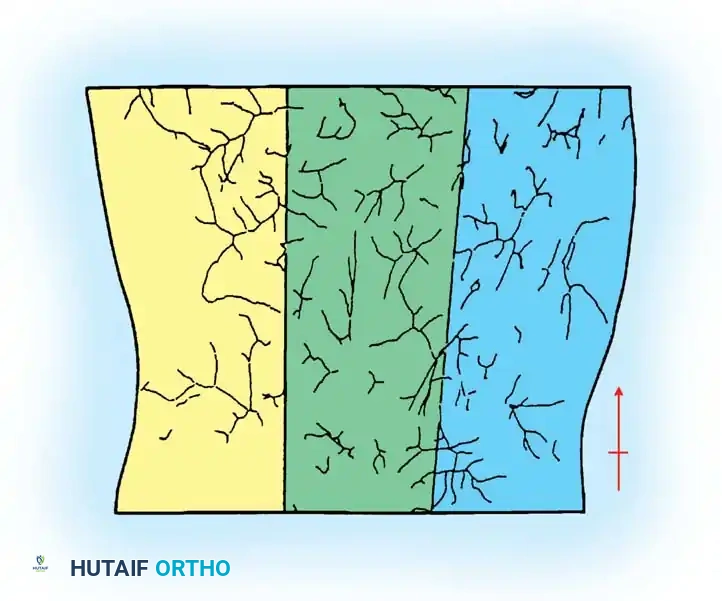
The successful execution of Damage Control Orthopaedics relies heavily on a profound understanding of cross-sectional surgical anatomy and the biomechanics of temporary fixation constructs. The soft-tissue envelope surrounding major long bones dictates not only the initial injury classification but also the safe corridors for external fixation pin placement. High-energy trauma imparts massive kinetic energy to this soft-tissue envelope, resulting in extensive microvascular thrombosis, periosteal stripping, and muscle necrosis. The degree of soft-tissue injury is the primary determinant of the bone's biological capacity to heal and its susceptibility to deep infection. Understanding the fascial compartments of the extremities is paramount; the leg contains four distinct compartments (anterior, lateral, deep posterior, and superficial posterior), while the thigh contains three, and the forearm contains three functional compartments. Edema and hemorrhage within these non-yielding fascial spaces rapidly elevate intracompartmental pressures, leading to microvascular compromise and ischemia.

To standardize the assessment of these complex injuries, the AO-ASIF and Tscherne classifications are universally utilized. The AO-ASIF classification provides a comprehensive framework for evaluating closed (IC) and open (IO) injuries. Closed injuries range from IC 1 (no skin lesion) to IC 5 (necrosis from contusion), encompassing severe closed degloving injuries known as Morel-Lavallée lesions (IC 4), where the subcutaneous tissue is sheared from the underlying deep fascia, creating a potential space filled with blood, lymph, and necrotic fat. Open injuries range from IO 1 (inside-out puncture) to IO 4 (full-thickness contusion, avulsion, and massive soft-tissue defect). The Tscherne classification for closed fractures further stratifies soft-tissue injury from Grade 0 (indirect violence, minimal damage) to Grade 3 (extensive contusion, crushing of skin, destruction of muscle, and high risk of compartment syndrome).

From a biomechanical perspective, the application of a damage control external fixator must prioritize maximum stability with minimal surgical time. The stiffness of an external fixation construct is governed by several biomechanical principles: the diameter of the Schanz pins, the distance between the pins and the fracture site, the distance between the longitudinal rod and the bone, and the number of planes utilized. Pin diameter is the most critical factor, as the bending stiffness of a pin is proportional to the fourth power of its radius ($r^4$). Therefore, utilizing a 5.0 mm or 6.0 mm pin in the femur significantly enhances construct rigidity compared to smaller diameters. However, pins must not exceed one-third of the bone's diameter to avoid creating a critical stress riser that could lead to iatrogenic fracture.
Furthermore, the anatomical placement of these pins must strictly respect "safe corridors" to avoid neurovascular injury and to prevent contamination of the future definitive fixation site. In the femur, pins are typically placed laterally or anterolaterally to avoid the medial neurovascular bundle (superficial femoral artery and vein). In the tibia, pins are placed on the anteromedial subcutaneous border. A critical biomechanical and biological consideration during pin insertion is the prevention of thermal necrosis. High-speed drilling without adequate cooling or the use of dull drill bits generates excessive heat, leading to ring sequestrum formation, aseptic loosening, and subsequent pin-tract infections. Thus, pre-drilling both cortices with a sharp bit through a tissue-protecting sleeve is mandatory.
Exhaustive Indications and Contraindications
The decision-making process between Early Total Care (ETC) and Damage Control Orthopaedics (DCO) is arguably the most critical juncture in polytrauma management. This decision must be driven by objective physiological parameters rather than the mere presence of fractures. Patients are broadly categorized into four physiological states: Stable, Borderline, Unstable, and In Extremis. Stable patients are candidates for ETC, where definitive intramedullary nailing or plate osteosynthesis can be safely performed. In Extremis and Unstable patients are absolute candidates for DCO, as any prolonged surgical intervention will precipitate an irreversible physiological collapse. The "Borderline" patient presents the greatest clinical challenge; these patients may appear transiently stable but possess a highly primed immune system capable of catastrophic decompensation upon the "Second Hit" of definitive surgery.
Indications for DCO include severe acid-base disturbances, coagulopathy, hypothermia, and massive transfusion requirements. The "Lethal Triad" of trauma—acidosis, hypothermia, and coagulopathy—is an absolute contraindication to definitive fracture care. Acidosis (pH < 7.25 or Base Excess < -5.0 mmol/L) indicates profound tissue hypoperfusion and anaerobic metabolism. Hypothermia (core temperature < 34°C) severely impairs enzyme kinetics, particularly those of the coagulation cascade, leading to refractory bleeding. Coagulopathy, often exacerbated by the consumption of clotting factors and hemodilution from crystalloid resuscitation, must be corrected before any definitive orthopaedic procedure. An elevated serum lactate (> 2.5 mmol/L) that fails to clear despite adequate fluid resuscitation is a highly sensitive indicator of occult hypoperfusion and mandates a DCO approach.
Contraindications to immediate definitive fixation also extend to local anatomical factors. Severe soft-tissue compromise, such as Tscherne Grade 3 closed injuries or Gustilo-Anderson Type IIIB/IIIC open fractures with massive contamination, preclude immediate internal fixation due to the exorbitant risk of deep infection and wound breakdown. In these scenarios, DCO allows for skeletal stabilization while facilitating serial debridements, soft-tissue recovery, and eventual flap coverage. Furthermore, the presence of an evolving compartment syndrome or a concomitant vascular injury requiring bypass grafting dictates the use of rapid external fixation to protect the vascular repair and allow unimpeded access to the soft tissues.
Decision Matrix for Polytrauma Management
| Parameter | Stable (ETC Indicated) | Borderline (Consider DCO) | Unstable / In Extremis (Absolute DCO) |
|---|---|---|---|
| Systolic Blood Pressure | > 100 mm Hg | 90 - 100 mm Hg | < 90 mm Hg (requires vasopressors) |
| Base Excess | > -2.0 mmol/L | -2.0 to -5.0 mmol/L | < -5.0 mmol/L |
| Serum Lactate | < 2.0 mmol/L | 2.0 - 2.5 mmol/L | > 2.5 mmol/L (non-clearing) |
| Coagulation (Platelets) | > 110,000 / µL | 90,000 - 110,000 / µL | < 90,000 / µL |
| Core Temperature | > 35° C | 34° - 35° C | < 34° C |
| Thoracic Trauma | None / Mild | Moderate (Multiple rib fx) | Severe (Bilateral contusions, PaO2/FiO2 < 200) |
| Transfusion Needs | < 2 Units PRBCs | 2 - 6 Units PRBCs | > 6 Units PRBCs (Massive Transfusion) |
Pre-Operative Planning, Templating, and Patient Positioning
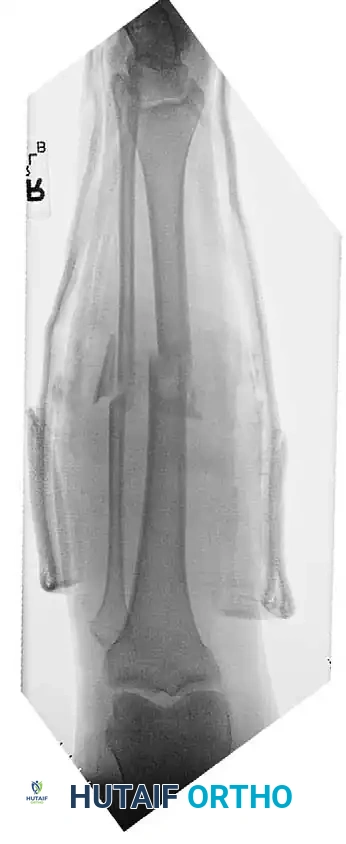
Pre-operative planning in the context of polytrauma is a dynamic, highly compressed process that begins in the trauma bay and continues seamlessly into the operating theater. Hemodynamic resuscitation is the absolute priority, guided by the principles of Damage Control Resuscitation (DCR), which emphasizes permissive hypotension, minimization of crystalloids, and the early, balanced administration of blood products (1:1:1 ratio of packed red blood cells, fresh frozen plasma, and platelets). While the trauma surgery and anesthesia teams optimize the patient's physiology, the orthopaedic surgeon must rapidly formulate a surgical plan that addresses all major skeletal injuries with maximum efficiency. This involves reviewing all available imaging, though in extremis patients may only have portable anteroposterior (AP) radiographs of the chest, pelvis, and affected extremities.

Patient positioning for DCO must facilitate rapid, multi-extremity access without the need for repositioning during the case. The patient is universally positioned supine on a fully radiolucent trauma table. This is critical to allow unimpeded access for the C-arm fluoroscope from the pelvis down to the bilateral lower extremities. Bumpers or sandbags may be used to elevate the ipsilateral hip for lateral access to the femur, but complex positioning devices (such as fracture tables with traction boots) are strictly avoided in the acute DCO setting, as they consume valuable time and limit access to other body regions (e.g., the abdomen for concurrent exploratory laparotomy).

Templating for external fixation is mental and anticipatory rather than strictly digital. The surgeon must select the appropriate pin sizes (typically 5.0 mm or 6.0 mm for the femur and tibia, 4.0 mm for the upper extremity) and determine the ideal pin locations to maximize construct stability while preserving the soft-tissue envelope for future definitive surgery. The entire limb, from the iliac crest to the toes, must be prepped and draped free. This wide sterile field allows for manual longitudinal traction, extensive soft-tissue debridement if open fractures are present, and the flexibility to extend the external fixation construct across joints (e.g., knee-spanning or ankle-spanning frames) if periarticular fractures or massive soft-tissue defects dictate such measures.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of Damage Control Orthopaedics must be swift, precise, and biologically respectful. When addressing a femoral shaft fracture in an unstable patient, the goal is to construct a rigid mono-lateral or bi-planar external fixator in under 30 minutes. The procedure begins with the identification of safe corridors. For the femur, half-pins are placed laterally or anterolaterally. A generous stab incision is made through the skin and iliotibial band. Blunt dissection using a hemostat is carried down to the bone to protect cutaneous nerves and prevent muscle entrapment. A drill sleeve is firmly seated against the near cortex. The bone is pre-drilled with a sharp drill bit, ensuring bicortical purchase while employing saline irrigation to prevent thermal osteonecrosis. The Schanz pins are then inserted manually or under low-speed power.
For the tibia, pins are placed on the anteromedial face (the subcutaneous border). Care must be taken to avoid the saphenous vein and nerve medially, and the anterior tibial neurovascular bundle laterally. Once a minimum of two pins are placed proximal and two pins distal to the fracture site, bar-to-pin clamps are applied and loosely connected with carbon fiber or radiolucent rods. An assistant applies strong longitudinal traction to restore limb length, correct rotational deformity, and align the mechanical axis under fluoroscopic guidance. Once acceptable alignment is achieved, the clamps are sequentially tightened. If additional stiffness is required, a delta frame configuration or a multi-planar construct can be rapidly assembled by adding an anterior rod connected to the primary construct.

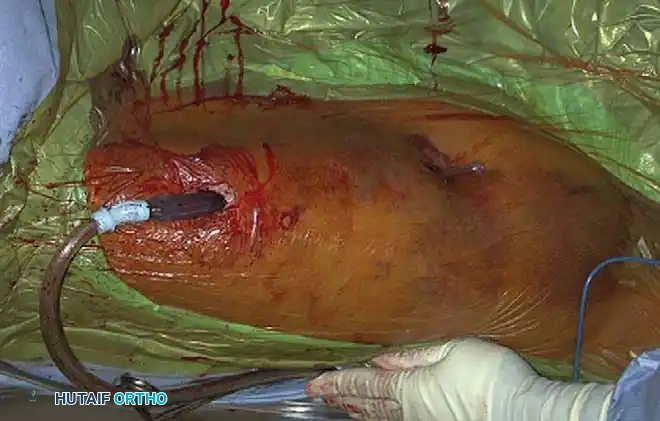
In the presence of open fractures, the DCO procedure must incorporate an aggressive, systematic debridement. Open fractures are surgical emergencies conceptualized as incomplete amputations. The primary goals are the prevention of infection and the removal of all devascularized tissue. The wound is extended longitudinally to allow thorough inspection. All necrotic skin, subcutaneous fat, and devitalized muscle (assessed by the "4 Cs": color, consistency, contractility, and capacity to bleed) are sharply excised. Bone fragments devoid of soft-tissue attachment are removed, and the medullary canal is irrigated with copious amounts of low-pressure normal saline. Following debridement, the wound is typically managed with a negative pressure wound therapy (NPWT) device to manage exudate and promote angiogenesis, bridging the patient to subsequent definitive coverage.
Concurrent with fracture stabilization, the surgeon must maintain a high index of suspicion for compartment syndrome, a catastrophic complication characterized by tissue pressures exceeding capillary perfusion pressure. Diagnosis in the obtunded polytrauma patient relies on objective compartment pressure monitoring. Irreversible muscle and nerve necrosis occurs if tissue pressures rise to within 30 mm Hg of the diastolic blood pressure (ΔP < 30 mm Hg). If this threshold is breached, an emergent four-compartment fasciotomy of the leg is mandatory. This is performed via dual incisions: a lateral incision to decompress the anterior and lateral compartments, and a medial incision to decompress the superficial and deep posterior compartments. The fascial releases must extend the entire length of the compartment to ensure complete decompression.

Complications, Incidence Rates, and Salvage Management
The management of polytrauma patients is fraught with severe, potentially life-threatening complications. These complications arise not only from the initial traumatic insult but also from the systemic inflammatory response and the necessary surgical interventions. One of the most critical systemic complications is Acute Respiratory Distress Syndrome (ARDS), which historically occurred in up to 38% of patients subjected to delayed definitive fixation, but has been significantly mitigated by the advent of DCO protocols. Multiple Organ Dysfunction Syndrome (MODS) remains a leading cause of late mortality in the ICU setting, driven by the unchecked cytokine storm and subsequent microvascular failure.

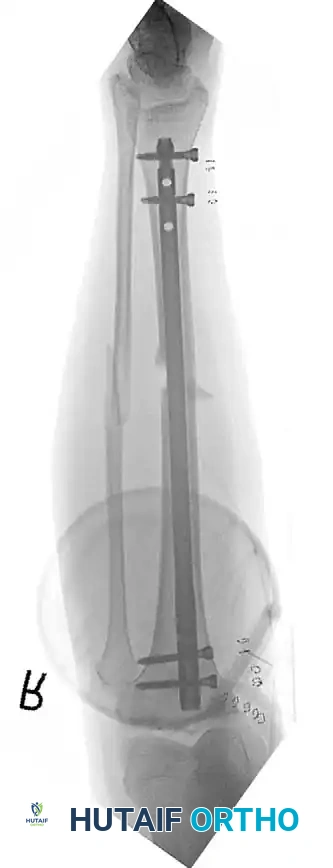
Locally, the use of temporary external fixation introduces the risk of pin-tract infections. Superficial pin-tract infections occur in approximately 10% to 15% of cases and are typically managed with oral antibiotics and aggressive local pin-site care. However, deep pin-tract infections with associated osteomyelitis or ring sequestrum necessitate immediate pin removal, aggressive over-reaming of the pin tract, and transition to skeletal traction or alternative fixation methods. The timing of conversion from external fixation to definitive intramedullary nailing is a subject of intense scrutiny. Landmark studies have demonstrated that if the conversion is performed within a strict 14-day window, the risk of deep intramedullary infection is not significantly higher than that of primary nailing. Delaying conversion beyond 14 days leads to an exponential increase in deep infection rates.
Missed injuries represent another significant complication in polytrauma care. Despite rigorous ATLS protocols, up to 20% of patients have injuries overlooked during the primary and secondary surveys. These most commonly include non-contiguous spinal fractures, subtle ligamentous injuries of the knee or foot, and upper extremity fractures. The implementation of a mandatory tertiary survey—a complete head-to-toe clinical and radiological re-evaluation performed 24 to 48 hours post-admission when the patient is awake and cooperative—is vital for identifying and salvaging these missed injuries before they result in chronic deformity or disability.
Common Complications and Salvage Strategies
| Complication | Incidence Rate | Pathophysiology / Risk Factors | Salvage Management / Prevention |
|---|---|---|---|
| ARDS / MODS | 5% - 15% | "Second Hit" phenomenon; massive cytokine release (IL-6, TNF-α); pulmonary micro-thrombi. | Adherence to DCO; avoidance of early IM reaming in borderline patients; lung-protective ventilation. |
| Pin-Tract Infection | 10% - 15% | Thermal necrosis during pin insertion; prolonged Ex-Fix duration (> 14 days); poor soft-tissue envelope. | Sharp drill bits with cooling; daily pin care; early conversion to IMN (< 14 days); over-reaming of infected tracts. |
| Deep Bone Infection | 2% - 5% | Open fractures (Gustilo IIIB/IIIC); delayed soft-tissue coverage; conversion to IMN after 14 days. | Aggressive serial debridements; early flap coverage (< 72 hrs); suppressive antibiotics; bone transport for massive defects. |
| Compartment Syndrome | 2% - 9% | Reperfusion injury; crush injuries (Tscherne Gr 2/3); delayed recognition in obtunded patients. | Continuous pressure monitoring (ΔP < 30); emergent 4-compartment fasciotomies; delayed primary closure. |
| Missed Injuries | 5% - 20% | Distracting injuries; altered sensorium (TBI, intubation); inadequate initial imaging. | Mandatory tertiary survey at 24-48 hours; low threshold for advanced imaging (CT/MRI) of symptomatic areas. |
Phased Post-Operative Rehabilitation Protocols
The post-operative management of a polytrauma patient treated with Damage Control Orthopaedics is highly protocolized and heavily dependent on multi-system physiological recovery. The rehabilitation protocol is divided into distinct, physiologically driven phases. The initial phase (Days 0-4) is the ICU Resuscitation Phase. During this period, the orthopaedic focus is strictly on maintaining the integrity of the external fixation constructs, monitoring for compartment syndrome, and assisting the intensivist team in clearing the patient's systemic physiological debt. Lactate clearance, normalization of base deficit, reversal of coagulopathy, and stabilization of core temperature are the primary endpoints. Mobilization is generally limited to passive range of motion of unaffected joints to prevent contractures and strict deep vein thrombosis (DVT) prophylaxis.
The second phase (Days 5-10) is the "Window of Opportunity." At this stage, the initial systemic inflammatory response has typically peaked and begun to subside. Interleukin-6 levels trend downward, and capillary leak resolves, allowing for diuresis of third-spaced fluids. If the patient meets the criteria for physiological stability, they are returned to the operating room for the conversion of temporary external fixators to definitive internal fixation (e.g., intramedullary nailing of the femur or tibia, plate osteosynthesis of periarticular fractures). This conversion must
Clinical & Radiographic Imaging Archive
