Classification & Management of Soft Tissue Injuries in Trauma

Key Takeaway
Soft tissue injury classification is paramount in orthopedic trauma, dictating surgical timing, fixation strategies, and limb salvage potential. Systems like the Gustilo-Anderson and Tscherne classifications provide prognostic value for infection and healing. Modern polytrauma management relies on these frameworks to transition between Early Total Care (ETC) and Damage Control Orthopaedics (DCO), optimizing patient survival and functional outcomes through staged interventions.
Comprehensive Introduction and Patho-Epidemiology
In the contemporary realm of operative orthopaedics, the paradigm has decisively shifted from a purely bone-centric approach to one that equally prioritizes the soft tissue envelope. The management of orthopaedic injuries, particularly in the context of high-energy trauma, has a profound effect on the patient’s ultimate functional recovery, limb salvage potential, and overall mortality. Just as the bony injury must be rigorously classified to adequately evaluate the fracture geometry and to validate results for comparative studies, trauma-associated soft tissue injuries must be meticulously evaluated and graded. The soft tissue envelope is not merely a passive covering; it is a dynamic, biologically active organ system that dictates the healing potential of the underlying osseous structures.
The degree of soft tissue compromise dictates the timing of surgical intervention, the choice between internal and external fixation, the necessity for complex soft tissue coverage (such as rotational or free tissue transfer), and the overall prognosis regarding deep infection, nonunion, and amputation. High-energy mechanisms, such as motor vehicle collisions, industrial crush injuries, and ballistic trauma, impart massive kinetic energy to the extremity. This energy transfer results in complex, comminuted fracture patterns that are invariably associated with severe periosteal stripping, muscle contusion, microvascular thrombosis, and gross contamination. Conversely, low-energy mechanisms, such as ground-level falls in the osteoporotic population, typically result in simple transverse or spiral fracture patterns with minimal soft tissue disruption, though the baseline microvascular status of the patient must still be considered.

Epidemiologically, open fractures occur at a rate of approximately 11.5 to 30.8 per 100,000 persons annually, with the tibial diaphysis being the most frequently involved anatomical site due to its precarious anteromedial subcutaneous location. The management of these injuries is further complicated in the multiply injured patient, where the initial trauma acts as a "first hit," triggering a massive systemic inflammatory response syndrome (SIRS). Early, definitive, and prolonged surgical interventions in this physiologically exhausted state can precipitate a "second hit," leading to acute respiratory distress syndrome (ARDS), multiple organ dysfunction syndrome (MODS), and death. This pathophysiological reality has birthed the concept of Damage Control Orthopaedics (DCO), which emphasizes rapid, temporary skeletal stabilization and hemorrhage control, delaying definitive reconstruction until the patient's physiological reserve has been restored.
Furthermore, the initial assessment of the soft tissue injury is often confounded by the evolving nature of soft tissue necrosis. The true extent of the "zone of injury" may not be fully apparent upon presentation in the emergency department. Microvascular thrombosis, progressive edema, and compartment syndrome can exacerbate initial tissue ischemia over the first 48 to 72 hours. Therefore, the classification of soft tissue injuries, whether using the Gustilo-Anderson system for open fractures or the Tscherne classification for closed injuries, must be viewed as a dynamic, iterative process. The final grading can only be accurately established in the operating theater following thorough surgical exploration and radical excisional debridement.
Detailed Surgical Anatomy and Biomechanics
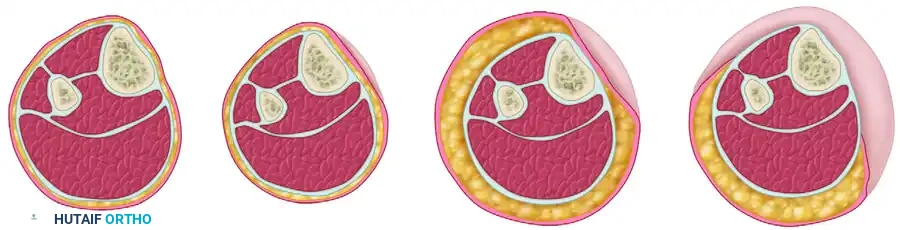
The soft tissue envelope of the extremities is a complex, multi-layered anatomical construct comprising the epidermis, dermis, subcutaneous adipose tissue, superficial and deep fascia, skeletal muscle, and periosteum. A comprehensive understanding of the vascular anatomy, specifically the angiosome concept detailed by Taylor and Palmer, is paramount for the orthopaedic trauma surgeon. Blood supply to the diaphysis of long bones is highly dependent on both the endosteal (medullary) and periosteal circulations. In the uninjured state, the endosteal system supplies approximately the inner two-thirds of the diaphyseal cortex, while the periosteal system supplies the outer one-third. However, in the presence of severe trauma, intramedullary nailing, or endosteal disruption, the periosteal blood supply becomes the critical determinant of cortical viability.


The morphology of a fracture serves as a direct historical record of the biomechanical energy imparted to the limb. The Orthopaedic Trauma Association (OTA) classification of long bone fractures categorizes bony injuries based on their morphology, functioning as an initial proxy for expected soft tissue damage. Simple fracture patterns typically result from lower-energy torsional or bending forces. In these injuries, the soft tissue hinge is often preserved, and the periosteum remains largely intact on the concave side of the bending force. This preservation allows for standard open reduction and internal fixation (ORIF) or intramedullary nailing without inducing extensive secondary soft tissue morbidity.


As the kinetic energy of the trauma increases, bending forces combined with axial loads create wedge or "butterfly" fragments. The degree of comminution correlates directly with the magnitude of periosteal stripping and local microvascular destruction. The soft tissue attachments to these intermediate fragments are often compromised, rendering them avascular. High-energy trauma results in complex, segmental fractures, severe comminution, or frank bone loss. These patterns are almost universally associated with profound soft tissue devitalization, a high risk of acute compartment syndrome, and the necessity for staged reconstructive protocols. The energy dissipates through the path of least resistance, causing explosive disruption of the surrounding muscle compartments, fascial tearing, and subcutaneous degloving (Morel-Lavallée lesions).


Biomechanically, the management of these complex fractures must respect the compromised biology. Traditional absolute stability constructs (e.g., lag screws and neutralization plates) require extensive soft tissue dissection, which can further devascularize already precarious fracture fragments, leading to iatrogenic nonunion and infection. Consequently, modern orthopaedic traumatology heavily favors relative stability constructs for diaphyseal and highly comminuted metaphyseal fractures. Techniques such as bridge plating, minimally invasive plate osteosynthesis (MIPO), and locked intramedullary nailing preserve the fracture hematoma and the remaining soft tissue attachments, fostering secondary bone healing via callus formation. The surgeon must meticulously balance the mechanical demands of the fracture with the biological needs of the soft tissue envelope.
Exhaustive Indications and Contraindications
The surgical decision-making process in orthopaedic trauma is heavily reliant on the accurate classification of the soft tissue injury. The Gustilo-Anderson classification, despite its well-documented inter-observer variability, remains the gold standard for guiding the management of open fractures. The indications for specific interventions are directly tied to these grades. Type I and Type II open fractures, characterized by wounds less than 1 cm and greater than 1 cm respectively, with minimal to moderate soft tissue contusion, are generally amenable to immediate or early definitive internal fixation following thorough debridement and irrigation. Intramedullary nailing for diaphyseal fractures in these categories is highly indicated, provided the physiological status of the patient permits.


Conversely, Type III open fractures represent high-energy injuries with massive contamination and severe soft tissue compromise, presenting distinct indications and strict contraindications. Type IIIA injuries, while featuring extensive lacerations, maintain adequate soft tissue coverage for the bone. Primary closure is often contraindicated due to the risk of trapping anaerobic bacteria and exacerbating edema; instead, delayed primary closure or split-thickness skin grafting is indicated after serial debridements. Type IIIB injuries are defined by inadequate local soft tissue coverage, necessitating rotational or free flap transfer. Immediate internal fixation with plates is generally contraindicated in Type IIIB injuries due to the prohibitive risk of deep infection; temporary external fixation is the treatment of choice. Type IIIC injuries involve an arterial injury requiring repair. The absolute indication here is immediate revascularization, often preceded by rapid external fixation to protect the vascular anastomosis.


The Tscherne classification provides equally critical indications for closed fractures. A Tscherne Grade 0 or 1 injury allows for standard timing of ORIF. However, Tscherne Grade 2 and Grade 3 injuries, characterized by deep contaminated abrasions, extensive muscle contusion, and severe subcutaneous degloving, are strong contraindications to immediate open surgical approaches through the compromised tissue. Incising through severely contused, edematous skin drastically increases the risk of wound dehiscence and deep infection. In these scenarios, the indication is to apply a spanning external fixator, elevate the limb, and wait for the "wrinkle sign" to appear—indicating the resolution of soft tissue edema—before proceeding with definitive internal fixation.
Summary of Soft Tissue Classifications and Surgical Indications
| Classification System | Grade / Type | Soft Tissue Characteristics | Primary Surgical Indications | Absolute/Relative Contraindications |
|---|---|---|---|---|
| Gustilo-Anderson | Type I | Clean wound < 1 cm, minimal contusion. | Immediate debridement, definitive internal fixation (IMN/ORIF). | Delayed fixation without biological rationale. |
| Gustilo-Anderson | Type II | Wound > 1 cm, moderate soft tissue damage. | Extended debridement, definitive internal fixation, possible delayed closure. | Primary closure under tension. |
| Gustilo-Anderson | Type IIIA | Extensive laceration, adequate bone coverage. | Serial debridements, temporary ex-fix or IMN, delayed primary closure. | Primary closure of highly contaminated wounds. |
| Gustilo-Anderson | Type IIIB | Extensive soft tissue loss, periosteal stripping. | Radical debridement, temporary ex-fix, flap coverage within 3-7 days. | Immediate plating; leaving bone exposed > 7 days. |
| Gustilo-Anderson | Type IIIC | Open fracture with arterial injury requiring repair. | Immediate temporary shunting, rapid ex-fix, vascular repair, fasciotomies. | Prolonged ischemia time (> 6 hours) without shunting. |
| Tscherne (Closed) | Grade 0 / 1 | Minimal to superficial soft tissue injury. | Standard timing for definitive internal fixation. | Unnecessary delay of definitive care. |
| Tscherne (Closed) | Grade 2 / 3 | Deep abrasion, extensive contusion, degloving. | Spanning external fixation, elevation, delay definitive ORIF until swelling resolves. | Incision through compromised, blistered skin. |
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning for severe soft tissue injuries begins at the trauma bay, adhering strictly to Advanced Trauma Life Support (ATLS) protocols. The initial assessment of the orthopaedic trauma patient must rapidly quantify the systemic physiological burden using established trauma scoring systems such as the Injury Severity Score (ISS), the Revised Trauma Score (RTS), or the Hanover Fracture Scale-97 (HFS-97). These metrics are vital for determining whether the patient is a candidate for Early Total Care (ETC) or requires Damage Control Orthopaedics (DCO). In the hemodynamically unstable patient, or the "borderline" patient with a severe chest injury, definitive prolonged internal fixation is contraindicated.


Once life-threatening injuries are addressed, meticulous evaluation of the soft tissue envelope is mandatory. The administration of early, appropriate intravenous antibiotics and tetanus prophylaxis is the single most critical step in reducing the incidence of infection in open fractures. Current guidelines dictate the administration of a first-generation cephalosporin for Gustilo Type I and II fractures, with the addition of an aminoglycoside or a third-generation cephalosporin for Type III injuries to cover Gram-negative organisms. High-dose penicillin is added if there is concern for clostridial contamination (e.g., agricultural injuries). Pre-operative imaging must include orthogonal radiographs of the entire injured segment, including the joints above and below. In high-energy trauma, particularly around the knee or in suspected Gustilo IIIC injuries, computed tomography angiography (CTA) is highly indicated to precisely map the vascular injury and plan the reconstructive or bypass approach.


Templating is an essential component of pre-operative planning, even when temporary external fixation is anticipated. The surgeon must anticipate the definitive implant to ensure that the placement of external fixation pins does not compromise the future surgical approach or the trajectory of intramedullary nails or plates. For instance, in a severe proximal tibia fracture requiring a spanning external fixator, the femoral pins should be placed anteriorly, and the tibial pins placed anteromedially, ensuring they remain entirely outside the future surgical incisions required for dual plating or intramedullary nailing.
Patient positioning in the operating room must facilitate both the orthopaedic stabilization and any necessary vascular or plastic surgical interventions. For complex lower extremity trauma, the patient is typically positioned supine on a radiolucent Jackson table or a flat table with a bump under the ipsilateral hip to correct external rotation. The entire limb, often up to the iliac crest, must be prepped and draped free to allow for extensive surgical approaches, harvesting of autologous bone graft, or procurement of vein grafts for vascular repair. A sterile tourniquet may be applied proximally but should remain uninflated unless life-threatening hemorrhage occurs, as assessing tissue viability during debridement relies heavily on observing active bleeding.
Step-by-Step Surgical Approach and Fixation Technique
The surgical management of severe soft tissue injuries and open fractures is predicated on the principle of radical excisional debridement. The objective is to convert a contaminated, necrotic wound into a clean, viable surgical bed. The surgeon must systematically evaluate and debride all tissue layers from superficial to deep. The skin edges should be sharply excised until healthy, bleeding dermal edges are encountered. Subcutaneous fat, which has poor vascularity and is highly susceptible to necrosis, must be aggressively resected if it appears contused or avulsed.


Assessment of skeletal muscle viability is arguably the most challenging aspect of the debridement process. The surgeon must rely on the classic "4 C's": Color, Consistency, Contractility, and Capacity to bleed. Muscle that is dark, mushy, fails to contract when stimulated with electrocautery, and does not bleed when cut must be radically excised. Retaining necrotic muscle provides an ideal nidus for anaerobic bacterial proliferation and subsequent deep infection. Bone fragments that are completely devoid of soft tissue attachments (cortical bone without periosteum) and are not critical for articular congruity should generally be removed, as they act as avascular sequestra.
Following radical debridement, thorough irrigation is performed to mechanically remove gross debris and reduce the bacterial bioburden. The landmark Fluid Lavage of Open Wounds (FLOW) trial demonstrated that normal saline is as effective as, if not superior to, castile soap or antibiotic solutions, and that low-pressure gravity flow is preferable to high-pressure pulsatile lavage, which can drive debris deeper into the medullary canal and damage delicate local microvasculature. Following irrigation, the surgical team should change gowns, gloves, and instruments before proceeding to skeletal stabilization to prevent cross-contamination.


Skeletal stabilization in the setting of severe soft tissue compromise (Gustilo IIIB/IIIC or Tscherne Grade 3) is most safely achieved with a spanning external fixator. The construct must provide absolute rigidity to protect the soft tissue envelope and any vascular anastomoses. Half-pins are placed well outside the zone of injury. Once the skeleton is stabilized, the soft tissue defect is managed. Primary closure is rarely indicated in high-energy open fractures. Instead, the application of Negative Pressure Wound Therapy (NPWT) has revolutionized the management of these wounds. NPWT reduces tissue edema, promotes angiogenesis, decreases the physical size of the wound, and provides a sterile barrier until definitive soft tissue coverage (e.g., a free latissimus dorsi or anterolateral thigh flap) can be performed. The consensus, pioneered by Godina, dictates that definitive flap coverage should ideally occur within 72 hours to 7 days post-injury to minimize the risk of nosocomial infection and flap failure.
Complications, Incidence Rates, and Salvage Management
The management of complex trauma with severe soft tissue injuries is fraught with high rates of complications. The most devastating of these include deep infection (osteomyelitis), fracture nonunion, acute compartment syndrome, flap necrosis, and ultimately, secondary amputation. The incidence of deep infection correlates directly with the severity of the soft tissue injury. Gustilo Type I fractures carry an infection rate of approximately 0-2%, Type II fractures 2-7%, Type IIIA fractures 7-15%, and Type IIIB/IIIC fractures can exhibit infection rates ranging from 10% to over 50% in various series.
Acute compartment syndrome is a surgical emergency that occurs when elevated pressure within a closed osteofascial compartment compromises local microcirculation, leading to muscle and nerve ischemia. It is highly associated with high-energy tibial shaft fractures, crush injuries, and vascular repairs (reperfusion injury). The diagnosis is primarily clinical, characterized by pain out of proportion to the injury, pain with passive stretch, and a tense compartment. When clinical diagnosis is equivocal, particularly in the obtunded polytrauma patient, continuous intra-compartmental pressure monitoring is indicated. A delta pressure (diastolic blood pressure minus compartment pressure) of less than 30 mmHg is an absolute indication for emergency four-compartment fasciotomies of the leg.
Salvage management for infected nonunions or massive bone defects resulting from severe open fractures requires complex, multidisciplinary reconstructive strategies. The Masquelet technique (induced membrane technique) involves radical debridement, placement of an antibiotic-impregnated polymethylmethacrylate (PMMA) cement spacer to induce a highly vascularized pseudosynovial membrane, followed 6 to 8 weeks later by spacer removal and massive autologous bone grafting. Alternatively, distraction osteogenesis utilizing the Ilizarov method allows for bone transport to bridge massive intercalary defects while simultaneously addressing soft tissue contractures and eradicating infection through continuous mechanical tension.
Complications and Salvage Strategies in Severe Soft Tissue Trauma
| Complication | Incidence / Risk Factors | Clinical Presentation | Salvage Management / Intervention |
|---|---|---|---|
| Acute Compartment Syndrome | 2-9% in tibial fractures; high in crush/vascular injuries. | Pain out of proportion, pain on passive stretch, tense compartments, paresthesia. | Emergent 4-compartment fasciotomy. Delayed primary closure or split-thickness skin grafting. |
| Deep Infection / Osteomyelitis | Gustilo I: <2%; Gustilo IIIB: 10-50%. | Erythema, purulent drainage, sinus tract formation, loosening of hardware. | Radical debridement, hardware removal (if unstable), antibiotic cement spacers, systemic culture-directed antibiotics. |
| Aseptic Nonunion | 5-15%; higher with severe periosteal stripping and bone loss. | Persistent pain at fracture site, lack of bridging callus on radiographs at 6-9 months. | Exchange nailing, autologous bone grafting (iliac crest or RIA), compression plating, optimization of host biology. |
| Flap Failure / Necrosis | 5-10% in free tissue transfers; related to vascular thrombosis or infection. | Demarcation of flap skin, loss of Doppler signal, venous congestion (bluish hue). | Emergent return to OR for microvascular exploration/thrombectomy. If unsalvageable, debridement and alternative flap or amputation. |
| Morel-Lavallée Lesion | Common in pelvic/trochanteric crush injuries. | Fluctuant mass, skin hypermobility, overlying skin necrosis. | Percutaneous drainage, sclerodesis, or open debridement with NPWT. Must be addressed prior to internal fixation. |
Phased Post-Operative Rehabilitation Protocols
The post-operative rehabilitation of a patient with a severe soft tissue injury and associated fracture is a prolonged, phased process requiring seamless coordination between orthopaedic surgeons, plastic surgeons, and physical therapists. The primary goal in the immediate post-operative phase (Days 0-14) is the protection of the soft tissue reconstruction and the prevention of deep vein thrombosis (DVT) and joint contractures. If a free flap or rotational flap has been performed, the limb is strictly elevated, and any external pressure on the pedicle is absolutely avoided. Weight-bearing is strictly non-weight-bearing (NWB), and range of motion (ROM) exercises are limited to joints distant from the zone of injury and flap coverage.
The intermediate phase (Weeks 2-6) begins once the soft tissue envelope demonstrates definitive viability and surgical incisions or skin grafts have healed. At this juncture, active and active-assisted ROM of the joints adjacent to the fracture is initiated to prevent arthrofibrosis. The progression of weight-bearing is dictated by the method of skeletal fixation and the morphological stability of the fracture. For diaphyseal fractures stabilized with a statically locked intramedullary nail, progressive partial weight-bearing may be initiated early. However, for complex periarticular fractures managed with bridge plating or external fixation, weight-bearing is typically delayed until radiographic evidence of early callus formation is observed.
The late rehabilitation phase (Weeks 6 to 12 and beyond) focuses on progressive mechanical loading, muscle strengthening, and functional restoration. The principles of Wolff's Law are utilized to stimulate bone remodeling; controlled axial loading is encouraged to promote fracture consolidation. Patients undergo intensive gait training, proprioceptive rehabilitation, and work-hardening programs. Psychological support is also paramount during this phase, as the incidence of post-traumatic stress disorder (PTSD) and clinical depression is exceptionally high among polytrauma patients who have sustained life-altering soft tissue and osseous injuries.
Summary of Landmark Literature and Clinical Guidelines
The modern management of soft tissue injuries in orthopaedic trauma is built upon a foundation of landmark clinical studies and evolving guidelines. The seminal work by Gustilo and Anderson in 1976, and its subsequent modification in 1984, remains the cornerstone for classifying open fractures and predicting infection risk. Despite valid criticisms regarding inter-observer reliability, it remains the universal language of orthopaedic traumatology. The Tscherne classification similarly revolutionized the appreciation of soft tissue compromise in closed injuries, emphasizing that severe crush injuries without a break in the skin carry morbidity comparable to high-grade open fractures.
The timing of soft tissue coverage was fundamentally altered by the work of Godina in 1986. His retrospective review demonstrated that early microsurgical reconstruction (within 72 hours) of complex extremity trauma resulted in significantly lower rates of flap failure, infection, and bone nonunion compared to delayed reconstruction. While modern advances in NPWT have slightly extended this window, the "Godina principle" of urgent soft tissue coverage remains a guiding tenet.
The Lower Extremity Assessment Project (LEAP) study provided critical insights into the long-term outcomes of limb salvage versus amputation in severe lower extremity trauma. The LEAP study found that at two years, and even at seven years post-injury, there was no significant difference in functional outcomes between patients who underwent successful limb salvage and those who underwent early amputation. This data is crucial when counseling patients with Gustilo Type IIIC injuries or massive Type IIIB injuries, highlighting that limb salvage is not always synonymous with functional salvage, and amputation should be viewed as a reconstructive option rather than a failure of care. Finally, the FLOW (Fluid Lavage of Open Wounds) trial provided high-level Level I evidence that low-pressure normal saline is the optimal irrigation solution, fundamentally changing emergency department and operating room protocols worldwide.
