Multiple Trauma: A Complete Guide to Multiple Injury Management
Key Takeaway
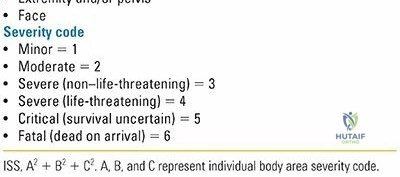
In this comprehensive guide, we discuss everything you need to know about Multiple Trauma: A Complete Guide to Multiple Injury Management. Multiple trauma multiple refers to severe injuries affecting more than one body system, characterized by an Injury Severity Score (ISS) greater than 18, often with hemodynamic instability or coagulopathy. Rapid, coordinated care within the "Golden Hour" significantly improves survival rates for these severely injured patients, as delayed treatment triples mortality risk.
Introduction and Epidemiology
High-velocity trauma remains the leading cause of death in the 18- to 44-year-old age group worldwide, presenting a profound challenge to both trauma systems and individual surgical providers. The economic burden and cost to the healthcare system for blunt trauma exceed those of any other disease category. While there is no single consensus definition, the polytrauma patient is classically defined by several critical parameters. The Berlin definition of polytrauma requires an Injury Severity Score (ISS) greater than 18, the presence of hemodynamic instability or coagulopathy on admission, and the involvement of more than one major organ system, such as the central nervous system (CNS), pulmonary, abdominal, or musculoskeletal systems.
Field Triage and Resuscitation Priorities
The initial management of the polytrauma patient begins in the prehospital setting. Field triage management priorities focus on the immediate preservation of life and the prevention of secondary injury. These priorities include the assessment of circulation and perfusion, aggressive hemorrhage control, safe patient extrication, shock management, preliminary fracture stabilization, and rapid patient transport.
Rapid transport of the severely injured patient to a designated Level I trauma center is essential for appropriate assessment and treatment. The concept of the "Golden Hour" dictates that a patient’s chance of survival diminishes rapidly after one hour, with a threefold increase in mortality for every 30 minutes of elapsed time without definitive care in the severely, multiply injured patient.
Trimodal Distribution of Trauma Deaths
Trauma deaths tend to occur in three distinct epidemiological phases, which dictate the focus of both public health initiatives and acute trauma care.
Immediate deaths occur at the scene or within minutes of the injury. This is usually the result of severe brain injury, high spinal cord disruption, or catastrophic disruption of the heart, aorta, or large vessels. These injuries are rarely salvageable and are most amenable to public health measures and primary prevention education, such as the enforcement of safety helmets and passenger restraints.
Early deaths occur minutes to a few hours after injury. These fatalities are usually the result of subdural or epidural hematomas, hemopneumothorax, splenic rupture, liver laceration, pelvic fractures, or multiple injuries associated with significant blood loss. These represent correctable injuries for which immediate, coordinated, definitive care at a Level I trauma center utilizing Advanced Trauma Life Support (ATLS) protocols is most beneficial.
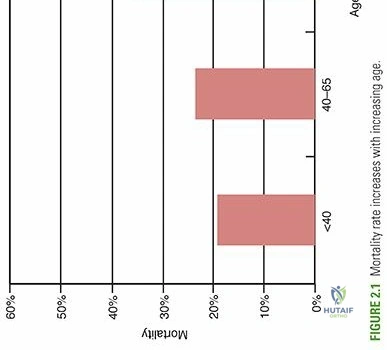
Late deaths occur days to weeks after the initial injury. Mortality in this phase is typically related to sepsis, pulmonary embolus, acute respiratory distress syndrome (ARDS), or multiple organ failure (MOF). The incidence of late mortality is heavily influenced by the initial resuscitation and the timing of surgical interventions. Mortality also demonstrates a direct correlation with increasing patient age, reflecting diminished physiological reserve in the elderly trauma population.
Surgical Anatomy and Biomechanics
Understanding the biomechanics of high-energy trauma and the surgical anatomy of major hemorrhage zones is critical for the orthopedic trauma surgeon. The transfer of kinetic energy to the human body dictates the pattern and severity of musculoskeletal and visceral injuries.
Energy Transfer and Injury Patterns
In blunt trauma, kinetic energy is transferred over a broad anatomical area, leading to compression, shearing, and deceleration injuries. The orthopedic surgeon must maintain a high index of suspicion for specific injury patterns based on the mechanism. For example, axial loading from a fall from a height frequently results in calcaneus fractures, tibial plateau fractures, and burst fractures of the thoracolumbar spine. Dashboard injuries in motor vehicle collisions transmit energy through the flexed knee, resulting in patella fractures, posterior hip dislocations, and posterior wall acetabular fractures.
Anatomy of Hemorrhage
The musculoskeletal system contains several major compartments capable of sequestering lethal volumes of blood. The pelvic ring is a critical anatomical zone in polytrauma. Disruption of the posterior pelvic ring expands the true pelvis volume, allowing massive retroperitoneal hemorrhage. Approximately 80 percent of pelvic bleeding is venous, originating from the presacral and prevesical venous plexuses, as well as the cancellous bone of the fractured pelvis. Arterial bleeding, comprising the remaining 20 percent, typically involves branches of the internal iliac artery, most commonly the superior gluteal artery or the internal pudendal artery.
Similarly, the fascial compartments of the thigh can accommodate up to 1.5 liters of extravasated blood per fractured femur. Bilateral femur fractures can therefore result in class III or IV hemorrhagic shock strictly from closed space bleeding, necessitating rapid anatomical restoration of length and volume through traction or external fixation.
Systemic Inflammatory Response
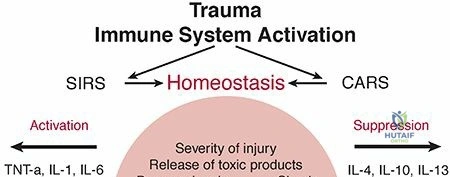
The biomechanical insult of polytrauma triggers a profound physiological response. The initial trauma causes a Systemic Inflammatory Response Syndrome (SIRS), characterized by the release of cytokines (IL-1, IL-6, TNF-alpha). This is closely followed by a Compensatory Anti-inflammatory Response Syndrome (CARS). The orthopedic principle of Damage Control Orthopedics (DCO) is predicated on the anatomical and physiological understanding that prolonged, definitive surgical procedures represent a "second hit" that can exacerbate SIRS, pushing the patient into ARDS and MOF.
Indications and Contraindications
The decision-making process in orthopedic polytrauma management revolves around the physiological status of the patient. The core debate is between Early Total Care (ETC) and Damage Control Orthopedics (DCO). More recently, the concept of Early Appropriate Care (EAC) has emerged, focusing on the resuscitation adequacy before definitive fixation.
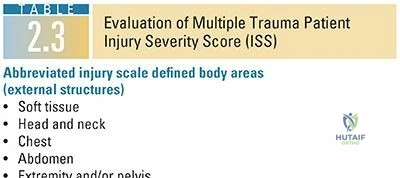
Physiological Classification of the Polytrauma Patient
Patients are classified into four physiological categories based on their response to initial resuscitation.
Stable patients have normal hemodynamics, no coagulopathy, and normal acid-base status. They are clear candidates for Early Total Care, including definitive intramedullary nailing of long bone fractures within the first 24 hours.
Borderline patients present the greatest clinical challenge. They may initially respond to resuscitation but possess underlying physiological derangements (e.g., elevated lactate, base deficit, hypothermia) that make them susceptible to deterioration during prolonged surgery.
Unstable patients remain hemodynamically labile despite aggressive resuscitation. They require strictly Damage Control Orthopedics.
In Extremis patients suffer from ongoing, uncontrolled hemorrhage and profound lethal triad parameters. They require immediate life-saving interventions, often strictly in the trauma bay or ICU, with surgical intervention limited to rapid hemorrhage control.
| Physiological Status | Clinical Parameters | Orthopedic Management Strategy |
|---|---|---|
| Stable | Systolic BP > 90 mmHg, Lactate < 2.0 mmol/L, Base Excess > -2, Normal Coagulation, Temp > 35°C | Early Total Care (ETC): Definitive fixation of all major fractures (e.g., IM nailing of femur) within 24 hours. |
| Borderline | Initial responder to fluids, Lactate 2.0-2.5 mmol/L, Base Excess -2 to -5.5, ISS 20-40, Multiple injuries | Early Appropriate Care (EAC) or DCO: Reassess after resuscitation. If parameters improve, proceed with ETC. If they worsen, pivot to DCO. |
| Unstable | Systolic BP < 90 mmHg despite fluids, Lactate > 2.5 mmol/L, Base Excess < -5.5, Coagulopathy present, Temp < 35°C | Damage Control Orthopedics (DCO): Rapid external fixation of long bones, pelvic binders/packing, hemorrhage control. |
| In Extremis | Ongoing massive hemorrhage, profound shock, Lactate > 8.0 mmol/L, severe coagulopathy, impending arrest | Life-Saving Interventions Only: Pelvic binder, immediate massive transfusion, REBOA, resuscitative thoracotomy. |
Pre Operative Planning and Patient Positioning
The trauma team is headed by the trauma general surgeon, who acts as the "captain of the ship" in prioritizing and directing patient care. The orthopedic consult is available to assess all musculoskeletal injuries, provide initial bony stabilization, and work in concert with the trauma general surgeons to treat shock and hemorrhage.
Advanced Trauma Life Support Principles
Resuscitation follows the strict ATLS algorithm of ABCDE Airway, Breathing, Circulation, Disability, Exposure.
Airway Control requires immediate inspection of the upper airway to ensure patency. Foreign objects should be removed, and secretions suctioned. A definitive airway (endotracheal or nasotracheal intubation) should be established as needed. The patient must be managed with strict cervical spine precautions. However, no patient should die from a lack of an airway because of concern over a possible cervical spine injury. Gentle maneuvers, such as manual in-line stabilization, allow for safe intubation without neurologic compromise.
Breathing involves the evaluation of ventilation and oxygenation. The most common reasons for ineffective ventilation after the establishment of an airway include malposition of the endotracheal tube, pneumothorax, and hemothorax. Tension pneumothorax is diagnosed clinically by tracheal deviation, unilateral absent breath sounds, tympany, and distended neck veins. Treatment requires immediate needle decompression (historically second intercostal space midclavicular line, now frequently updated to the fifth intercostal space anterior axillary line) followed by tube thoracostomy. Open pneumothorax, diagnosed by a sucking chest wound, is initially managed with an occlusive dressing taped on exactly three sides to allow a one-way flutter valve effect where air can exit the pleural space during exhalation but cannot enter during inhalation.
Circulation management focuses on hemorrhage control and restoration of intravascular volume. Massive Transfusion Protocols (MTP) should be initiated early, utilizing a 1 to 1 to 1 ratio of packed red blood cells, fresh frozen plasma, and platelets to prevent dilutional coagulopathy. Pelvic binders must be applied centered over the greater trochanters to reduce pelvic volume.
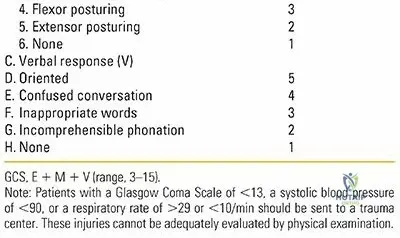
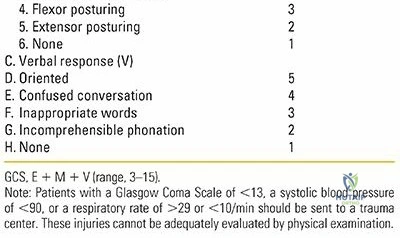
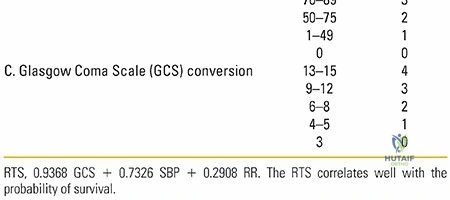
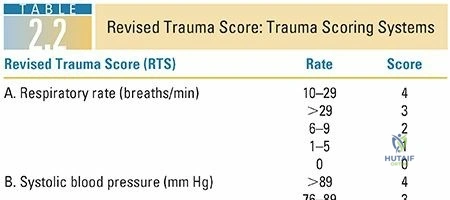
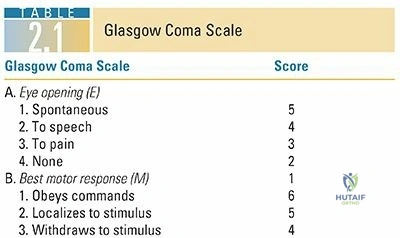
Disability assessment involves a rapid neurological evaluation using the Glasgow Coma Scale (GCS) and pupillary reflex testing. Exposure requires complete undressing of the patient to identify all injuries, followed immediately by the application of warm blankets and forced-air warming devices to prevent hypothermia.
Operating Room Setup for Damage Control
When a polytrauma patient is transferred to the operating room for damage control surgery, meticulous preoperative planning is essential. The room must be heated to prevent hypothermia. The patient should be positioned supine on a fully radiolucent trauma table. The surgical prep must be extensive, often encompassing the entire torso and bilateral lower extremities, to allow simultaneous access for laparotomy, pelvic stabilization, and long bone external fixation. Two or more surgical teams frequently operate concurrently to minimize total operative time.
Detailed Surgical Approach and Technique
The surgical technique in the acute polytrauma setting is defined by the principles of Damage Control Orthopedics. The goal is rapid, provisional stabilization of skeletal injuries to control hemorrhage, reduce pain, and facilitate nursing care, without inflicting a significant secondary physiological hit.
Damage Control Orthopedics Principles
DCO procedures should ideally be completed within 60 to 90 minutes. The primary targets for DCO are unstable pelvic ring disruptions, major long bone fractures (femur and tibia), and highly contaminated open fractures.
Pelvic Ring Stabilization
For hemodynamically unstable patients with mechanically unstable pelvic ring injuries (e.g., APC II/III or vertical shear patterns), immediate volume reduction is required. If a pelvic binder is insufficient, skeletal fixation is indicated.
Anterior external fixation is performed using either iliac crest pins or supra-acetabular pins. Supra-acetabular pin placement is biomechanically superior and allows better access for concurrent laparotomy. Through a small incision over the anterior inferior iliac spine (AIIS), the fascia is split, and the rectus femoris is retracted. Under fluoroscopic guidance (obturator oblique and iliac oblique views), a 5.0 mm or 6.0 mm Schanz pin is advanced between the inner and outer tables of the ilium, directed toward the posterior superior iliac spine.
In cases of severe posterior ring disruption with ongoing hemorrhage, a pelvic C-clamp may be applied. The pins are placed at the intersection of a line drawn along the longitudinal axis of the femur and a line drawn posteriorly from the anterior superior iliac spine. This targets the dense bone of the gluteus medius pillar, allowing massive compressive forces to be applied across the sacroiliac joints.
Long Bone External Fixation
Femur fractures in the unstable polytrauma patient are managed with rapid spanning external fixation rather than intramedullary nailing. The technique involves placing two 5.0 mm Schanz pins into the proximal femur (typically lateral to anterior to avoid the neurovascular bundle and future definitive surgical incisions) and two pins in the distal femur. A carbon fiber rod is used to connect the pins, restoring length, alignment, and rotation. This reduces the volume of the thigh compartment, tamponading further blood loss and reducing the systemic release of marrow fat and inflammatory mediators.
Similarly, tibial shaft fractures and periarticular fractures (e.g., tibial plateau, pilon) are managed with spanning external fixation. For a knee-spanning frame, pins are placed in the anterior diaphysis of the femur and the anteromedial face of the tibial shaft, connected by rigid rods to span the zone of injury.
Open Fracture Management and Compartment Syndrome
Highly contaminated open fractures require immediate aggressive debridement. All devitalized muscle, bone, and debris must be excised. The wound is typically left open and managed with negative pressure wound therapy (NPWT) or a sterile bead pouch.
The orthopedic surgeon must maintain a high index of suspicion for acute compartment syndrome, particularly in the setting of prolonged hypotension, reperfusion injury, or severe soft tissue crush. If compartment pressures are elevated (typically within 30 mmHg of diastolic blood pressure), emergent four-compartment fasciotomies of the leg or dual-incision fasciotomies of the forearm are mandatory.
Conversion to Definitive Fixation
The conversion from DCO to definitive fixation (e.g., exchange of an external fixator for an intramedullary nail) must be carefully timed. This typically occurs between days 5 and 10 post-injury, corresponding to the resolution of the systemic inflammatory response. The patient must demonstrate normalized physiological parameters, including a normal lactate, correction of coagulopathy, extubation or minimal ventilator settings, and a downward trend in inflammatory markers such as C-reactive protein (CRP) and Interleukin-6 (IL-6).
Complications and Management
The polytrauma patient is at extreme risk for a multitude of systemic and localized complications. The management of these complications requires a multidisciplinary approach involving orthopedic surgery, trauma surgery, and critical care medicine.
The Lethal Triad
The most immediate threat to the polytrauma patient is the "Lethal Triad" of hypothermia, acidosis, and coagulopathy. Hypothermia decreases the enzymatic activity of coagulation cascade proteins. Acidosis (pH < 7.2) further impairs coagulation and decreases myocardial contractility. Coagulopathy results from the consumption of clotting factors, dilution from crystalloid resuscitation, and hypothermia-induced dysfunction. Management requires aggressive rewarming, limitation of crystalloid fluids, administration of balanced blood products (MTP), and immediate cessation of surgery (Damage Control) until physiology is restored.
Systemic Complications
Fat Embolism Syndrome (FES) is a severe complication following long bone fractures, particularly when definitive fixation is delayed or performed in a borderline patient. It presents with a classic triad of hypoxemia, neurological abnormalities, and a petechial rash. Management is supportive, focusing on mechanical ventilation and maintenance of hemodynamics.
Acute Respiratory Distress Syndrome (ARDS) results from profound systemic inflammation and capillary leak in the lungs. It is characterized by bilateral pulmonary infiltrates and severe hypoxemia. Treatment involves lung-protective ventilation strategies and prone positioning.
| Complication | Incidence in Polytrauma | Pathophysiology / Risk Factors | Salvage Strategy and Management |
|---|---|---|---|
| Lethal Triad | 10-20% (Higher in ISS > 25) | Hypothermia, Acidosis, Coagulopathy driving irreversible shock. | Immediate DCO, massive transfusion protocol (1:1:1), active rewarming, correction of acidosis in ICU. |
| Fat Embolism Syndrome (FES) | 1-5% of long bone fractures | Release of marrow fat into venous circulation; biochemical degradation to toxic free fatty acids. | Supportive ICU care, mechanical ventilation, early stabilization of fractures to prevent further marrow embolization. |
| Acute Respiratory Distress Syndrome | 10-15% | Exaggerated SIRS response leading to alveolar-capillary membrane disruption. | Lung-protective ventilation (low tidal volume), permissive hypercapnia, prone positioning, diuresis. |
| Venous Thromboembolism (VTE) | Up to 60% without prophylaxis | Virchow's triad: endothelial injury, venous stasis, hypercoagulability post-trauma. | Early mechanical prophylaxis, chemical prophylaxis (LMWH) once bleeding risk resolves, IVC filter if anticoagulation contraindicated. |
| Multiple Organ Failure (MOF) | 10-20% | Prolonged hypoperfusion (first hit) followed by massive inflammatory response (second hit). | Aggressive early resuscitation, strict adherence to DCO principles, continuous renal replacement therapy (CRRT) if needed. |
Post Operative Rehabilitation Protocols
Rehabilitation of the polytrauma patient begins in the Intensive Care Unit (ICU) immediately following operative stabilization. The goals of early rehabilitation are the prevention of pulmonary complications, mitigation of muscle atrophy, and prevention of joint contractures.
Intensive Care Unit Management
Early mobilization is critical but must be balanced against the patient's physiological stability and the mechanical construct of their fracture fixation. In patients who have undergone Early Total Care with stable intramedullary fixation of long bones, early upright positioning and mobilization to a chair can significantly reduce ventilator days and ICU length of stay.
For patients managed with Damage Control Orthopedics, mobilization is often restricted by the presence of external fixators and the severity of their systemic illness. Range of motion exercises for non-immobilized joints should be initiated immediately by physical therapy.
Weight-bearing restrictions are dictated by the specific fracture patterns and fixation methods. Pelvic ring injuries may require protected weight-bearing for 6 to 12 weeks. Articular fractures managed with spanning external fixators require strict non-weight-bearing status until conversion to definitive internal fixation and subsequent bone healing.
Chemical thromboprophylaxis, typically with low-molecular-weight heparin (LMWH), should be initiated as soon as it is deemed safe by the trauma and surgical teams, usually within 24 to 48 hours of injury, provided there is no ongoing hemorrhage or unmanaged traumatic brain injury.
Summary of Key Literature and Guidelines
Clinical & Radiographic Imaging
