

Comprehensive Introduction and Patho-Epidemiology
End-stage tibiotalar arthrosis presents a complex reconstructive challenge that demands meticulous surgical planning and precise intraoperative execution. Unlike osteoarthritis of the hip and knee, which is predominantly primary or idiopathic in nature, primary osteoarthrosis of the ankle is relatively rare and often poorly understood in its exact etiology. The vast majority of cases encountered in the orthopedic foot and ankle clinic—approximately 70% to 80%—are strictly post-traumatic in origin. This post-traumatic degeneration typically stems from a history of intra-articular pilon fractures, rotational ankle fracture-dislocations complicated by malunion, or chronic lateral ankle instability that has led to progressive, asymmetric cartilage wear over decades.
The pathophysiology of post-traumatic ankle arthrosis is driven by acute mechanical cartilage injury followed by chronic abnormal joint kinematics. Impact loads sustained during the initial trauma cause immediate chondrocyte apoptosis and disruption of the extracellular matrix. Even with anatomic reduction of articular fractures, the altered contact mechanics and subtle residual incongruencies inevitably lead to elevated peak contact stresses. Over time, this mechanical overload initiates a cascade of inflammatory cytokines, matrix metalloproteinases, and progressive cartilage degradation, ultimately resulting in subchondral sclerosis, cyst formation, and debilitating pain.
Beyond post-traumatic etiologies, the orthopedic surgeon must be prepared to address end-stage ankle arthritis arising from systemic inflammatory arthropathies. Rheumatoid arthritis remains the most common inflammatory cause, though the incidence of severe tibiotalar destruction has decreased with the advent of modern disease-modifying antirheumatic drugs (DMARDs) and biologic therapies. Other systemic conditions, including hemochromatosis, crystalline arthropathies (gout and pseudogout), pigmented villonodular synovitis (PVNS), and hemophilic arthropathy, also contribute to the burden of disease. Furthermore, infectious etiologies such as sequelae of septic arthritis, and neuropathic destruction seen in Charcot neuroarthropathy, require highly specialized surgical algorithms.
The ultimate goal of an anterior ankle arthrodesis is to surgically obliterate the tibiotalar articulation, thereby providing a stable, durable, and pain-free platform for plantigrade ambulation. While total ankle arthroplasty (TAA) has seen significant advancements and expanded indications in recent years, ankle arthrodesis remains the gold standard, particularly for younger, high-demand patients, those with severe coronal or sagittal plane deformities, profound bone loss, or compromised soft tissue envelopes. By fusing the joint in an optimal biomechanical position, the surgeon sacrifices tibiotalar motion to restore overall limb function, relying on the transverse tarsal and subtalar joints to compensate for the loss of sagittal plane kinematics during the gait cycle.

Detailed Surgical Anatomy and Biomechanics
Osteology and Articular Geometry
The ankle joint, or tibiotalar joint, is a highly congruous, modified hinge joint formed by the complex articulation of the distal tibia, the fibula, and the talus. The tibial plafond represents the distal articular surface of the tibia, and its medial extension forms the medial malleolus. The plafond articulates primarily with the dorsal and medial aspects of the talar dome. In the sagittal plane, the plafond exhibits a slight posterior slope, which is critical for accommodating the talus during terminal dorsiflexion. In the coronal plane, the articular surface is typically oriented at an angle of 88 to 92 degrees relative to the mechanical axis of the tibial shaft, a metric that must be perfectly restored during arthrodesis to prevent eccentric loading of the hindfoot.
The fibula, articulating with the lateral facet of the talus, acts as a crucial lateral buttress for ankle stability. While biomechanical studies indicate that the fibula bears only about one-sixth of the axial load transmitted through the lower extremity, its contribution to the structural integrity of the ankle mortise is paramount. The lateral malleolus extends further distally than the medial malleolus, providing an essential bony block against excessive external rotation and valgus translation of the talus. During an anterior approach for arthrodesis, the fibula is generally left intact unless a transfibular approach or specific lateral deformity correction is dictated by the preoperative plan.
The talus is a unique, avascular-prone bone with approximately 60% of its surface covered by articular cartilage, lacking any direct muscular or tendinous attachments. Its superior articular surface, the trochlea, features a dual radius of curvature; it is significantly wider anteriorly than posteriorly. This trapezoidal geometry dictates that the ankle mortise is most stable in maximum dorsiflexion, where the wider anterior talus is wedged securely between the malleoli. During arthrodesis, the surgeon must carefully decorticate this dense subchondral bone without overly resecting the talar dome, as preserving talar height is critical to maintaining appropriate leg length and avoiding impingement of the malleoli on the calcaneus.



Ligamentous and Syndesmotic Complexes
Understanding the ligamentous anatomy is crucial when considering soft tissue releases for deformity correction prior to joint preparation. The distal tibiofibular syndesmosis is a robust fibrous joint formed by the anterior inferior tibiofibular ligament (AITFL), the interosseous membrane, the posterior inferior tibiofibular ligament (PITFL), and the transverse ligament. This complex binds the tibia and fibula together, allowing only minimal physiologic diastasis during terminal dorsiflexion. We must respect this complex during our anterior approach; iatrogenic injury or failure to address pre-existing syndesmotic widening can lead to a widened mortise, complicating graft placement and compromising the mechanical stability of the fusion construct.
Medially, the deltoid ligament complex provides primary resistance against valgus tilting and external rotation of the talus. It is composed of a superficial layer (tibionavicular, tibiocalcaneal, and superficial tibiotalar ligaments) and a deep layer (deep anterior and deep posterior tibiotalar ligaments). In cases of severe varus ankle arthritis, the deltoid ligament is often pathologically contracted. The surgeon must be prepared to perform a systematic medial release, sometimes requiring a separate medial incision, to allow the talus to be reduced into a neutral coronal alignment without placing excessive tension on the medial skin envelope.
Laterally, the lateral collateral ligament complex consists of the anterior talofibular ligament (ATFL), the calcaneofibular ligament (CFL), and the posterior talofibular ligament (PTFL). The ATFL is the primary restraint to anterior talar translation, while the CFL resists varus stress. In patients with post-traumatic arthritis secondary to chronic lateral instability, these structures are often attenuated or absent. Conversely, in long-standing valgus deformities, the lateral structures may be contracted, necessitating fractional lengthening or complete release to mobilize the talus and achieve a plantigrade foot position prior to definitive hardware fixation.



Anterior Neurovascular and Tendinous Anatomy
The anterior approach to the ankle navigates a highly concentrated zone of critical neurovascular and tendinous structures. The superficial peroneal nerve (SPN), a terminal branch of the common peroneal nerve, typically pierces the deep crural fascia in the distal third of the leg. It descends to supply sensation to the dorsum of the foot and toes. The SPN is highly variable in its arborization and frequently crosses the planned anterior longitudinal incision. Meticulous blunt dissection in the subcutaneous tissue is absolutely mandatory to identify, mobilize, and protect this nerve, as iatrogenic neuroma formation in this region is a profound source of postoperative morbidity.
Deep to the extensor retinaculum lies the deep neurovascular bundle, the most critical structure at risk during the anterior approach. This bundle consists of the deep peroneal nerve (DPN) and the anterior tibial artery, accompanied by its venae comitantes. The bundle traverses the anterior ankle joint capsule precisely between the tibialis anterior (TA) tendon and the extensor hallucis longus (EHL) tendon, or occasionally between the EHL and the extensor digitorum longus (EDL) tendons. The DPN provides motor innervation to the extensor digitorum brevis and supplies sensation to the first dorsal web space. Retraction of this bundle must be gentle and strictly lateralized to prevent traction neuropraxia or catastrophic vascular occlusion.
The tendinous anatomy dictates our surgical interval. The tibialis anterior (TA) is the largest and most medial tendon of the anterior compartment, functioning as a powerful dorsiflexor and invertor. It is enclosed within its own distinct synovial sheath. Immediately lateral to the TA is the extensor hallucis longus (EHL) tendon, which extends the great toe and assists in ankle dorsiflexion. Further lateral lies the extensor digitorum longus (EDL) and the peroneus tertius. The standard anterior approach utilizes the internervous and intertendinous interval between the TA and the EHL. Developing this interval allows direct, orthogonal access to the anterior capsule of the tibiotalar joint while permitting safe lateral retraction of the deep neurovascular bundle alongside the EHL and EDL.


Exhaustive Indications and Contraindications
Patient Selection and Clinical Evaluation
Before committing to surgical intervention, a comprehensive and exhaustive patient evaluation is non-negotiable. Patients typically present with a primary complaint of deep, aching, chronic pain localized to the anterior ankle joint line. This pain is characteristically exacerbated by weight-bearing activities, ambulation on uneven ground, and forced dorsiflexion (such as climbing stairs or walking up inclines). In early stages, the pain may be relieved by rest, but as the arthrosis progresses to end-stage disease, the pain often becomes constant, interfering with sleep and severely limiting the patient's activities of daily living. Associated symptoms frequently include chronic effusions, progressive stiffness, and a subjective feeling of instability or "giving way."
Clinical examination must assess the entire ipsilateral lower extremity, not merely the isolated ankle joint. Optimal limb alignment from the hip to the foot is absolutely essential; an ankle arthrodesis forfeits the limb's ability to compensate for any proximal or distal malalignment through the tibiotalar articulation. The surgeon must evaluate for genu varum or valgum, tibial torsion, and hindfoot alignment. Any significant concomitant hindfoot, midfoot, or forefoot malalignment (such as a rigid pes planovalgus or a cavovarus deformity) must be identified, as these may need to be addressed simultaneously or in a staged fashion to prevent eccentric loading and subsequent failure of the ankle fusion.
Range of motion (ROM) testing is critical, but the focus must extend beyond the ankle. While tibiotalar ROM will be intentionally obliterated, the ROM of the subtalar and transverse tarsal joints is paramount. A stiff, arthritic hindfoot combined with a fused ankle creates a functional tibiotalocalcaneal or pan-talar arthrodesis, severely limiting the foot's ability to accommodate uneven terrain and placing massive shear stresses on the midfoot and forefoot. If subtalar arthritis is clinically significant and symptomatic, the surgeon must consider either a primary tibiotalocalcaneal fusion or, if the patient meets criteria, a total ankle arthroplasty to preserve kinematics. Furthermore, a rigorous neurovascular exam documenting intact pulses, brisk capillary refill, and symmetric protective sensation (via Semmes-Weinstein monofilament testing) is mandatory prior to listing the patient for surgery.
Absolute and Relative Contraindications
While ankle arthrodesis is a highly successful procedure, strict adherence to contraindications is necessary to avoid catastrophic outcomes. Absolute contraindications include active, untreated local or systemic infection. Operating in the presence of active osteomyelitis or a septic joint invariably leads to hardware colonization, deep space infection, and potential limb loss. Another absolute contraindication is critical limb ischemia or profound peripheral vascular disease. Without adequate arterial inflow, the extensive soft tissue dissection and bone decortication required for fusion will fail to heal, leading to wound necrosis, nonunion, and amputation. Vascular surgery consultation and optimization are required if ischemic disease is suspected.
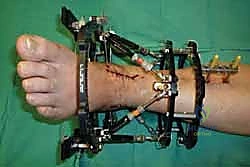
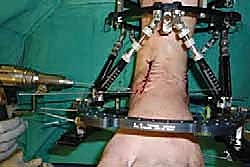
Relative contraindications require nuanced clinical judgment. Severe, uncontrolled peripheral neuropathy (most commonly diabetic) is a major risk factor for postoperative Charcot neuroarthropathy, hardware failure, and nonunion. While neuropathy is an absolute contraindication for total ankle arthroplasty, arthrodesis can be performed, provided the surgeon utilizes augmented fixation techniques (e.g., intramedullary nailing or robust multi-planar plating) and mandates a significantly prolonged period of non-weight-bearing immobilization. Similarly, active smoking is a profound relative contraindication. Nicotine induces microvascular vasoconstriction and inhibits osteogenesis, drastically increasing the rates of nonunion and wound dehiscence. Many academic centers mandate biochemical confirmation of smoking cessation (via serum or urine cotinine levels) prior to elective arthrodesis.
Other relative contraindications include severe osteopenia or osteoporosis, which compromises hardware purchase and structural stability. In such cases, the surgeon must plan for supplemental fixation, use of orthobiologics, or extended cast immobilization. Additionally, patients with profound cognitive impairment, severe psychiatric illness, or a documented history of medical non-compliance are poor candidates. The postoperative rehabilitation protocol following ankle arthrodesis is rigorous, requiring strict adherence to non-weight-bearing restrictions for several weeks. Inability to comply with these instructions virtually guarantees mechanical failure of the construct.
| Category | Specific Conditions | Surgical Implications & Management |
|---|---|---|
| Absolute Indications | End-stage post-traumatic OA, Rheumatoid Arthritis with severe deformity, Failed TAA, Paralytic deformities. | Primary indication for joint sacrifice to achieve stable, painless ambulation. |
| Absolute Contraindications | Active local/systemic infection, Critical limb ischemia, Non-reconstructable soft tissue envelope. | High risk of amputation. Requires infectious disease or vascular surgery intervention prior to any orthopedic consideration. |
| Relative Contraindications | Active smoking, Uncontrolled Diabetes/Neuropathy, Severe Osteoporosis, Medical non-compliance. | Mandates smoking cessation, augmented fixation (IM nails, heavy plates), prolonged NWB protocols, and stringent patient education. |


Pre-Operative Planning, Templating, and Patient Positioning
Diagnostic Imaging and Templating Protocols
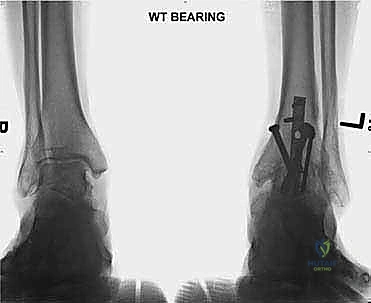
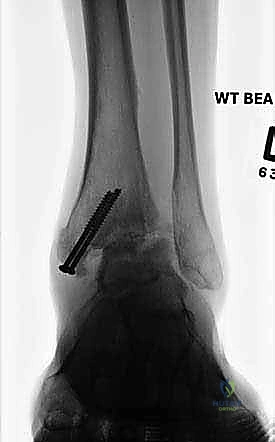
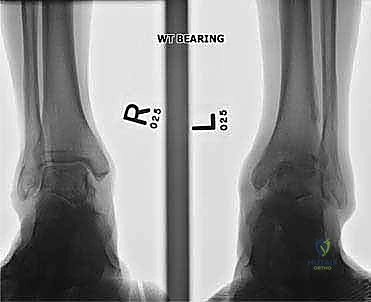
A comprehensive radiographic evaluation is the cornerstone of preoperative planning. Standard imaging must include weight-bearing anteroposterior (AP), lateral, and mortise views of the affected ankle. These plain films allow the surgeon to assess the degree of joint space narrowing, the presence and location of osteophytes, and the overall coronal and sagittal alignment of the tibiotalar joint. Additionally, weight-bearing AP, lateral, and oblique views of the foot are essential to evaluate the transverse tarsal and Lisfranc joints for concomitant arthrosis or deformity. A weight-bearing hindfoot alignment view (Saltzman view) is highly recommended to accurately quantify varus or valgus malalignment of the calcaneus relative to the tibial axis.
Advanced cross-sectional imaging is routinely utilized in modern orthopedic practice. A non-contrast Computed Tomography (CT) scan of the ankle and hindfoot is invaluable, particularly in cases of complex post-traumatic deformity or when substantial bone loss is suspected. The CT scan provides a high-resolution, three-dimensional map of the articular surfaces, allowing the surgeon to precisely localize subchondral cysts, areas of avascular necrosis, and the exact geometry of the deformity. This information dictates the necessity for structural bone grafting (autograft or allograft) and helps determine the optimal trajectory for fixation hardware. Magnetic Resonance Imaging (MRI) is less commonly required but is indicated if there is a high clinical suspicion of talar avascular necrosis or concurrent soft tissue pathology, such as unrecognized tendon ruptures.
Preoperative digital templating is a critical exercise that should not be bypassed. Utilizing the calibrated weight-bearing radiographs, the surgeon must template the expected bony resections required to achieve a neutral, plantigrade foot. The goal is to position the ankle in neutral dorsiflexion (0 degrees), 0 to 5 degrees of valgus, and 5 to 10 degrees of external rotation (matching the contralateral limb). Templating allows the surgeon to anticipate the size and length of the screws or plates required, the potential need for an Achilles tendon lengthening to achieve neutral dorsiflexion, and the exact location of the center of rotation of the ankle to prevent undesired anterior or posterior translation of the talus during final compression.

Patient Positioning and Anesthesia Considerations
Execution of a flawless anterior ankle arthrodesis begins with meticulous patient positioning. The patient is placed strictly supine on a standard radiolucent operating table. It is imperative that the plantar aspect of the operative foot is positioned at the absolute distal edge of the table. This positioning allows the surgeon unrestricted access to manipulate the foot and ankle through a full range of motion, facilitating deformity correction and the placement of posterior-to-anterior fixation if required. A bump or gel pad is placed under the ipsilateral hemipelvis to internally rotate the leg slightly, bringing the patella and the foot into a neutral, vertically oriented position. This prevents the natural tendency of the leg to externally rotate, which can disorient the surgeon and lead to malrotation of the final fusion construct.
Anesthesia for this procedure typically involves a multimodal approach to optimize intraoperative conditions and postoperative pain control. We routinely advocate for the use of a regional popliteal sciatic nerve block, often with a continuous catheter, combined with general anesthesia or deep sedation. The popliteal block provides profound, long-lasting analgesia to the foot and ankle while preserving motor function of the quadriceps, allowing for safe, early mobilization with crutches or a walker postoperatively. Because a proximal thigh tourniquet is utilized to maintain a bloodless surgical field, a supplemental femoral nerve block or an adequate depth of general anesthesia is required to mitigate tourniquet pain, which is not covered by the popliteal block alone.
The sterile prep and drape must be extensive. The entire lower extremity from the mid-thigh down to the toes is prepped with a chlorhexidine-based solution. The foot is draped free, allowing the surgeon to visually assess the alignment of the entire limb, from the tibial tubercle down to the second ray, during the critical stages of provisional fixation. A sterile tourniquet is typically not used; instead, a well-padded pneumatic thigh tourniquet is applied proximally. Prior to inflation, the limb is exsanguinated with an Esmarch bandage to ensure a pristine, bloodless field, which is absolutely critical for the precise identification of the delicate anterior neurovascular structures and the meticulous preparation of the articular surfaces.



Step-by-Step Surgical Approach and Fixation Technique
Incision, Exposure, and Neurovascular Protection
With the tourniquet inflated, the surgical approach commences with a longitudinal anterior midline incision. The incision is planned precisely, starting approximately 10 cm proximal to the tibiotalar joint line, located about 1 cm lateral to the palpable crest of the anterior tibia. This proximal extension is vital to allow adequate mobilization of the soft tissues without applying excessive tension to the skin edges. The incision is extended distally across the ankle joint, terminating just distal to the talonavicular joint. Sharp dissection is carried through the epidermis and dermis, immediately transitioning to meticulous blunt dissection in the subcutaneous fat to identify and protect the superficial peroneal nerve (SPN) and its arborizing branches.
Once the SPN is identified, isolated with a vessel loop, and gently retracted laterally, the deep crural fascia and the superior extensor retinaculum are incised longitudinally in line with the skin incision. The surgeon must now identify the critical surgical interval between the tibialis anterior (TA) tendon medially and the extensor hallucis longus (EHL) tendon laterally. The TA tendon sheath should ideally remain unviolated to prevent postoperative adhesions. Using blunt finger dissection or a Cobb elevator, the interval is developed down to the anterior capsule of the ankle joint.
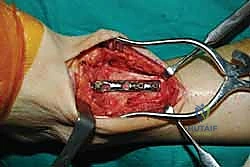
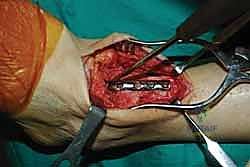
Deep to the EHL tendon lies the deep neurovascular bundle, comprising the deep peroneal nerve and the anterior tibial artery and veins. This bundle is mobilized as a single unit and retracted laterally along with the EHL and EDL tendons. We utilize a blunt, narrow Hohmann retractor placed carefully over the lateral shoulder of the talus to hold these structures out of harm's way. Medially, a second Hohmann retractor is placed around the medial malleolus to retract the TA tendon. This exposes the entire anterior capsule of the tibiotalar joint, which is then sharply excised to reveal the arthritic articular surfaces.




Articular Preparation and Deformity Correction
The success of an arthrodesis is entirely dependent on the meticulous preparation of the bony surfaces. The goal is to completely remove all remaining articular cartilage and dense, sclerotic subchondral bone down to healthy, bleeding, osteogenic cancellous bone, while preserving the complex congruent geometry of the joint. We begin by using a rongeur and sharp osteotomes to resect the large anterior tibial and talar osteophytes that typically block access to the joint space. A laminar spreader or a specialized joint distractor is then inserted into the joint to pry the tibia and talus apart, providing visualization of the posterior aspect of the joint.
Using a combination of sharp curettes, flexible osteotomes, and a high-speed burr, the cartilage is systematically denuded from the tibial plafond, the talar dome, and the medial and lateral gutters. It is critical to avoid aggressive flat-cut resections with a saw, as maintaining the native mortise-and-tenon geometry of the ankle provides immense intrinsic biomechanical stability. Once the cartilage is removed, the sclerotic subchondral bone must be penetrated. We employ a technique known as "fish-scaling" or "shingling," using a sharp osteotome to create multiple overlapping clefts in the bone, exposing the vascular marrow spaces. Alternatively, a 2.0 mm drill bit can be used to perform multiple subchondral perforations until punctate, petechial bleeding is observed upon tourniquet deflation.
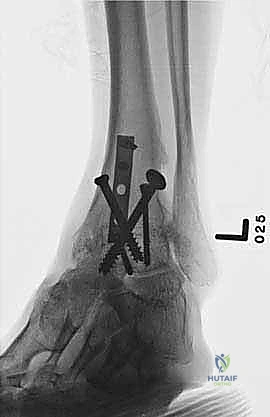
With the joint surfaces prepared, attention turns to deformity correction and alignment. If the patient has a rigid equinus contracture that prevents dorsiflexion to neutral, a percutaneous or open Achilles tendon lengthening (TAL) or gastrocnemius recession is performed at this stage. The foot is then manually manipulated into the optimal fusion position: 0 degrees of dorsiflexion (neutral), 0 to 5 degrees of hindfoot valgus, and external rotation that perfectly matches the contralateral limb (typically 5 to 10 degrees). The talus should be translated slightly posteriorly beneath the tibia to optimize the biomechanical lever arm of the Achilles tendon. Once perfect alignment is achieved clinically and verified fluoroscopically, the joint is provisionally fixed with two or three heavy (2.0 mm or 2.5 mm) Kirschner wires.

Clinical & Radiographic Imaging Archive














































Detailed Chapters & Topics
Dive deeper into specialized chapters regarding ankle-arthrodesis