Miniarthrotomy Ankle Arthrodesis: A Masterclass in Surgical Technique and Intraoperative Excellence

Key Takeaway
Join our masterclass on miniarthrotomy ankle arthrodesis. We'll meticulously cover patient selection, preoperative planning, precise intraoperative technique, comprehensive anatomical considerations, and essential pearls for achieving successful fusion in end-stage ankle arthritis, minimizing soft tissue disruption. This guide ensures fellows master every critical step.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to the operating theater and to this definitive masterclass on the miniarthrotomy technique for ankle arthrodesis. Today, we are tackling a procedure that represents a powerful, minimally invasive paradigm shift for the surgical management of end-stage ankle arthritis. Historically, ankle arthrodesis required extensive extensile surgical approaches, such as the transfibular or anterior expansile approaches, which inherently carried significant soft tissue morbidity, high rates of wound complications, and delayed healing. The miniarthrotomy technique, when executed with meticulous precision, offers excellent fusion rates that rival or exceed traditional open techniques while drastically reducing periosteal stripping and soft tissue trauma. Pay close attention to the nuances discussed herein, as we will walk through every critical step, from sophisticated preoperative planning to the final layered closure, emphasizing the biomechanical and biological principles that define successful outcomes.
To truly master this technique, one must first possess a profound understanding of the underlying pathology and the intricate epidemiology of ankle arthritis. Unlike the hip and knee, where primary osteoarthritis is the dominant etiology, the ankle joint is uniquely resistant to primary degenerative changes due to its highly congruent articular geometry and the distinct biological properties of its articular cartilage. Consequently, ankle arthritis is overwhelmingly posttraumatic in nature, accounting for approximately 70% to 80% of all cases. This typically follows intra-articular fractures (such as pilon or complex malleolar fractures), repetitive microtrauma from chronic lateral ligamentous instability, or neglected osteochondral lesions of the talus. The remaining cases comprise inflammatory arthritides (rheumatoid arthritis, seronegative spondyloarthropathies), neuropathic joint disease (Charcot arthropathy), and primary synovial disorders like pigmented villonodular synovitis.
The pathophysiology of end-stage ankle arthritis involves a relentless, progressive cascade of cartilage degradation, subchondral bone sclerosis, and the formation of hypertrophic marginal osteophytes. As the highly congruent tibiotalar joint space narrows, the natural kinematics of the ankle—which normally involve a complex combination of rolling and sliding motions—are severely disrupted. This mechanical degradation leads to profound functional impairment. Patients frequently develop compensatory gait mechanisms, most notably an obligatory external rotation of the hip during the stance phase, to bypass the painful heel-to-toe progression and limit stress across the arthritic tibiotalar articulation. Over time, this altered biomechanical chain can precipitate secondary pathology in the ipsilateral knee, hip, and lumbar spine.
Recent epidemiological literature rigorously underscores the debilitating nature of end-stage ankle arthritis, equating its physical and psychological impact to that of end-stage hip or kidney disease. These patients present with severe, unrelenting pain that profoundly interferes with activities of daily living, often reporting an obvious limp and a sensation of profound stiffness. Given the younger demographic often affected by posttraumatic ankle arthritis compared to primary hip or knee osteoarthritis, the socio-economic burden—measured in lost productivity and diminished quality of life—is immense. Therefore, offering a reliable, durable, and minimally morbid surgical solution via the miniarthrotomy arthrodesis is of paramount importance in the modern orthopedic surgeon's armamentarium.
Detailed Surgical Anatomy and Biomechanics
A flawless execution of the miniarthrotomy ankle arthrodesis demands an intimate, three-dimensional spatial awareness of the ankle's osseous architecture and its surrounding neurovascular envelope. The tibiotalar joint is a highly constrained, modified hinge joint. The osseous anatomy comprises the distal tibial plafond, the medial malleolus, the lateral malleolus (distal fibula), and the talar dome. The talar dome is wider anteriorly than posteriorly, a critical biomechanical feature that imparts intrinsic osseous stability when the ankle is in dorsiflexion. In the arthritic state, this anatomy is often distorted by massive anterior tibial and talar neck osteophytes, which mechanically block dorsiflexion and must be meticulously resected to restore anatomic alignment prior to fusion. Furthermore, the medial and lateral gutters—the articulations between the talus and the respective malleoli—must be thoroughly understood, as complete denudation of these surfaces is mandatory for a robust, multi-planar fusion mass.
The anterior neurovascular bundle is the most critical anatomic hazard during the anterior miniarthrotomy approach. The anterior tibial artery and the deep peroneal nerve descend into the foot coursing between the extensor hallucis longus (EHL) and the extensor digitorum longus (EDL) tendons at the level of the ankle joint. As they cross the anterior capsule, they are highly vulnerable to iatrogenic injury from aggressive retraction, errant osteotome placement, or uncontrolled burring. The deep peroneal nerve supplies sensation to the first web space and motor innervation to the extensor digitorum brevis; injury to this structure can result in painful neuromas and functional deficits. Maintaining strict subperiosteal dissection and utilizing protective retractors (such as malleable or Hohmann retractors) placed carefully inside the joint capsule are absolute prerequisites for safe execution.
Our surgical corridors for the miniarthrotomy technique rely on two precise vertical incisions that navigate safely between these critical structures. The medial incision is placed just medial to the anterior tibial (tibialis anterior) tendon. The primary structures at risk here are the saphenous vein and the saphenous nerve, which lie in the superficial subcutaneous tissue. The saphenous nerve provides sensation to the medial aspect of the foot and ankle, and its transection or traction injury is a frequent source of postoperative morbidity. Meticulous blunt dissection through the subcutaneous fat is required to identify and mobilize these structures. Deep to the retinaculum, the anterior tibial tendon is retracted laterally, providing direct access to the medial half of the tibial plafond, the medial gutter, and the medial talar dome.
The lateral surgical corridor is established via an incision placed immediately lateral to the peroneus tertius tendon. The anatomical hazard in this zone is the superficial peroneal nerve, which typically arborizes into the medial and intermediate dorsal cutaneous nerves proximal to the ankle joint. These branches cross the surgical field superficially and must be identified and protected. Deep dissection involves incising the extensor retinaculum and retracting the EDL and peroneus tertius tendons medially. This lateral window provides excellent visualization of the lateral half of the joint, the lateral gutter, and the syndesmosis. The convergence of these medial and lateral viewing portals allows the surgeon to cross-reference the joint preparation, ensuring no islands of cartilage remain on the central talar dome or tibial plafond.
Exhaustive Indications and Contraindications
The miniarthrotomy technique was initially conceptualized for a highly selected cohort of patients: those with end-stage ankle arthritis possessing minimal to no coronal plane deformity, negligible bone loss, and an absence of avascular necrosis (AVN). However, as surgical instrumentation has evolved and surgeon familiarity with the technique has grown, the indications have significantly expanded. Today, this procedure is broadly indicated for patients suffering from debilitating, end-stage tibiotalar arthritis that has proven recalcitrant to an exhaustive regimen of nonoperative management. This conservative trial must include, at a minimum, activity modification, aggressive use of nonsteroidal anti-inflammatory drugs (NSAIDs), targeted physical therapy, judicious use of intra-articular corticosteroid or biologic injections, and rigid immobilization via custom ankle-foot orthoses (AFOs) or rocker-bottom shoe modifications.
While the indications have broadened, strict adherence to biomechanical parameters regarding deformity is essential to prevent intraoperative frustration and postoperative failure. The miniarthrotomy approach is ideally suited for ankles with moderate deformities—specifically, varus or valgus malalignments measuring less than 10 to 15 degrees on weight-bearing radiographs. Deformities exceeding this threshold often require extensive soft tissue releases, structural bone grafting, or osteotomies of the malleoli that simply cannot be safely or effectively visualized through limited 2.5 cm incisions. Similarly, the technique is indicated for ankles with less than 25% anterior or posterior subluxation of the talus within the mortise. Talar subluxation beyond this limit indicates profound ligamentous incompetence and capsular contracture, necessitating a formal open approach to mobilize the joint and achieve anatomic reduction.
Contraindications to the miniarthrotomy ankle arthrodesis must be respected to mitigate catastrophic complications. Absolute contraindications include active or untreated deep infection of the ankle joint or surrounding soft tissues, severe peripheral vascular disease precluding wound healing, and profound neuroarthropathy (Charcot joint) with active fragmentation. In the setting of Charcot arthropathy, the lack of protective sensation and the compromised vascularity of the bone necessitate ultra-rigid fixation (often via circular external fixation or massive internal beams) and extensive bone grafting, which are not feasible via a mini-open approach. Furthermore, significant malalignment of the proximal tibia or femur that would result in a mechanically disadvantageous foot position post-fusion must be corrected prior to, or concomitantly with, the ankle arthrodesis.
Relative contraindications require nuanced clinical judgment. Avascular necrosis (AVN) of the talus is a prime example. If the AVN involves less than 25% of the talar body and the subchondral bone remains structurally intact, a miniarthrotomy approach may still be employed, often supplemented with biologic adjuvants like bone marrow aspirate concentrate (BMAC) or demineralized bone matrix (DBM). However, extensive talar AVN with collapse is a strong relative contraindication, often requiring a tibiotalocalcaneal (TTC) fusion or a massive structural allograft via an extensile approach. Similarly, severe osteoporosis is a relative contraindication, as the percutaneous screw fixation relied upon in this technique may fail to achieve adequate compression and purchase in osteopenic cancellous bone.
| Category | Miniarthrotomy Ankle Arthrodesis Criteria |
|---|---|
| Primary Indications | End-stage osteoarthritis, posttraumatic arthritis, inflammatory arthritis failing >6 months of conservative care. |
| Deformity Limits | Coronal plane deformity (varus/valgus) < 10-15 degrees; Sagittal subluxation < 25%. |
| Absolute Contraindications | Active local/systemic infection, severe peripheral arterial disease, active Charcot neuroarthropathy, uncorrectable proximal limb malalignment. |
| Relative Contraindications | Talar AVN > 25% of body, severe osteoporosis, massive cystic bone loss requiring large structural grafts, heavy active tobacco use. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the bedrock upon which a successful miniarthrotomy ankle arthrodesis is built. The process begins with a meticulous clinical examination. The surgeon must meticulously assess the soft tissue envelope, noting previous surgical scars, areas of compromised skin, and the presence of venous stasis changes. Vascular status is non-negotiable; palpable pedal pulses must be confirmed, and in any patient with a history of diabetes or vascular disease, an ankle-brachial index (ABI) and potentially arterial Doppler studies are mandatory. Neurologic examination must confirm intact protective sensation using a 5.07 Semmes-Weinstein monofilament. Crucially, the surgeon must differentiate primary ankle pain from adjacent hindfoot pathology. Because ankle arthritis often coexists with subtalar or transverse tarsal arthritis, diagnostic, fluoroscopically guided intra-articular injections of local anesthetic into the subtalar joint can be invaluable. Fusing the ankle while leaving a severely arthritic subtalar joint unaddressed is a guaranteed pathway to persistent postoperative pain and patient dissatisfaction.
Imaging evaluation begins with high-quality, bilateral, weight-bearing radiographs of the foot and ankle, including anteroposterior (AP), lateral, and mortise views. These plain films allow for the quantification of joint space narrowing, the assessment of coronal and sagittal plane deformities, and the identification of anterior impingement osteophytes.


When plain radiographs reveal significant subchondral cysts, suspected AVN, or complex multidirectional deformity, advanced imaging is required. A non-contrast Computed Tomography (CT) scan is the gold standard for defining the three-dimensional osseous architecture, mapping the exact size and location of subchondral cysts, and evaluating the integrity of the adjacent subtalar and talonavicular joints. If AVN is suspected but not clearly defined on CT, Magnetic Resonance Imaging (MRI) is utilized to assess the vascularity of the talar body.
Preoperative templating is a critical step that is too often overlooked. Using digital templating software on the weight-bearing lateral and AP radiographs, the surgeon should plan the optimal position of the ankle fusion: neutral dorsiflexion (0 degrees), 0 to 5 degrees of valgus, and 5 to 10 degrees of external rotation (matching the contralateral limb). Templating allows for the anticipation of the size and trajectory of the cannulated lag screws. Typically, we plan for two or three large-diameter (6.5 mm or 7.0 mm) partially threaded cannulated screws. The "home run" screw, traversing from the posterior tibia into the talar neck, is mechanically advantageous and should be templated to ensure it does not breach the subtalar joint. Anticipating the need for bone graft—whether local autograft harvested from the proximal tibia or distal radius, or allograft preparations—based on the volume of cystic voids seen on CT is essential for intraoperative efficiency.
Patient positioning in the operating room must be executed with precision to facilitate intraoperative fluoroscopy and accurate assessment of alignment. The patient is placed supine on a radiolucent operating table. A critical maneuver is the placement of a bump or rolled blanket under the ipsilateral buttock. The lower extremity naturally rests in external rotation; the bump internally rotates the leg to a neutral position, ensuring that the patella points directly toward the ceiling. This is vital because the patella serves as our primary proximal clinical landmark for setting the rotational alignment of the arthrodesis. The leg is prepped and draped freely above the knee to allow continuous visual access to the tibial crest and patella. While a thigh tourniquet is placed, we routinely do not inflate it unless visualization is severely compromised. Operating without a tourniquet allows the surgeon to visually confirm punctate bleeding from the subchondral bone—the ultimate biological confirmation of adequate joint preparation.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of the miniarthrotomy technique is an exercise in meticulous joint debridement and precise biomechanical fixation. We begin by delineating our surgical portals. The medial incision, approximately 2.5 to 3.0 cm in length, is centered over the medial joint line, strictly medial to the palpable anterior tibial tendon.


The skin is incised, and blunt dissection is utilized through the subcutaneous tissues to sweep the saphenous vein and nerve out of harm's way. The extensor retinaculum is incised longitudinally, and the anterior tibial tendon is retracted laterally. A vertical capsulotomy is then performed, exposing the medial aspect of the tibiotalar joint.

Simultaneously, the lateral incision is made just lateral to the peroneus tertius tendon, again measuring roughly 2.5 cm. Careful subcutaneous dissection identifies and protects the branches of the superficial peroneal nerve. The retinaculum is divided, the tendons are retracted medially, and a lateral capsulotomy is performed.


With both medial and lateral windows established, joint preparation commences. This is the most critical phase of the operation; any retained cartilage will act as a barrier to osteogenesis and result in a nonunion. We begin by resecting the anterior tibial and talar osteophytes using a combination of rongeurs and sharp osteotomes. This not only improves visualization but also removes the mechanical block to dorsiflexion, facilitating later reduction.


Next, using a series of straight and angled ring curettes, the remaining articular cartilage is systematically stripped from the tibial plafond and the talar dome.

Following curettage, a high-speed burr or an aggressive rasp is introduced to denude the subchondral bone plate.

The goal is not to remove large swaths of bone, which would shorten the limb and compromise stability, but to breach the sclerotic subchondral plate until healthy, bleeding cancellous bone is exposed. The medial and lateral gutters must be similarly debrided to ensure a maximal surface area for fusion. Finally, we use a 2.0 mm drill bit or a specialized microfracture awl to extensively fenestrate both the tibial and talar surfaces, releasing osteoprogenitor cells from the bone marrow.
Once the joint is thoroughly prepared and bleeding bone is confirmed, we proceed to deformity correction and provisional fixation. The foot is manually manipulated into the optimal fusion position: neutral sagittal alignment (0 degrees of dorsiflexion/plantarflexion), 0 to 5 degrees of hindfoot valgus, and external rotation matching the contralateral limb (typically 5 to 15 degrees).

Translational alignment is equally important; the talus should be translated slightly posteriorly beneath the tibia to optimize the biomechanical lever arm of the Achilles tendon. Once clinical alignment is achieved, two stout Steinmann pins or K-wires are driven across the joint to provisionally hold the reduction.

Intraoperative fluoroscopy (AP, lateral, and mortise views) is then meticulously reviewed to confirm perfect alignment and adequate bony apposition.
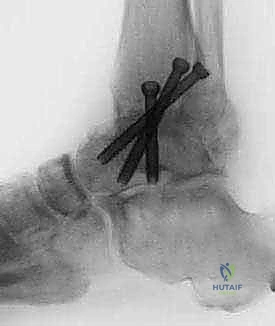
Definitive fixation is achieved using a construct of two or three large-diameter (6.5 mm or 7.0 mm) partially threaded cannulated lag screws. The precise configuration can vary based on surgeon preference and local anatomy, but a crossed-screw construct is biomechanically superior. The first guide pin is typically inserted from the medial tibia, proximal to the joint line, aiming distally and laterally into the lateral aspect of the talar body.


The second guide pin is placed from the lateral tibia, aiming medially into the medial talar body.


A third "home run" screw is highly recommended for maximal stability; this is placed from the posterior aspect of the distal tibia, aiming anteriorly and distally straight into the dense bone of the talar neck.

After confirming guide pin placement fluoroscopically, the near cortex is over-drilled, and the screws are inserted sequentially to generate massive interfragmentary compression across the arthrodesis site. If any small voids remain at the fusion interface, they are tightly packed with autologous bone graft or an osteoconductive allograft matrix prior to final screw tightening.
The wounds are thoroughly irrigated, and a meticulous, layered closure is performed, ensuring the extensor retinaculum is repaired to prevent tendon bowstringing.
