Anterior Cervical Discectomy and Fusion: An Intraoperative Masterclass
Key Takeaway
This masterclass on Anterior Cervical Discectomy and Fusion (ACDF) provides fellows with an immersive, step-by-step guide to this critical cervical spine procedure. We cover essential surgical anatomy, meticulous patient positioning, and detailed intraoperative execution, emphasizing optimal decompression and fusion techniques. Learn to navigate neurovascular risks, prepare endplates, and manage potential pitfalls for successful patient outcomes in cervical radiculopathy and myelopathy.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to the operating theater. Today, we embark on a comprehensive exploration of the Anterior Cervical Discectomy and Fusion, universally known as ACDF. Since its initial description by Smith and Robinson, and concurrently by Cloward in the 1950s, this procedure has evolved into the cornerstone surgical intervention for alleviating neural compression within the cervical spine. The ACDF is not merely a procedure of extirpation; it is an intricate exercise in structural restoration, meticulous neural decompression, and biomechanical stabilization. Mastery of this technique requires an appreciation of the delicate interplay between the cervical spine's neural elements and its dynamic, load-bearing architecture.
The pathophysiology of cervical spondylosis, the primary driver for this intervention, encompasses a predictable cascade of degenerative changes. It typically initiates with the desiccation and biochemical degradation of the intervertebral disc, specifically the nucleus pulposus. As the disc loses its hydrostatic properties, the annulus fibrosus is subjected to abnormal sheer and compressive forces, leading to micro-tears, bulging, and eventual loss of disc height. This collapse alters the kinematics of the entire motion segment, transferring aberrant loads to the uncovertebral and facet joints, which subsequently undergo hypertrophic arthrosis and osteophyte formation in a biological attempt to restabilize the segment.
Epidemiologically, cervical spondylosis is ubiquitous in the aging population, though it presents a wide spectrum of clinical manifestations. These degenerative changes can lead to neural impingement in two primary anatomic zones: the central spinal canal, resulting in cervical spondylotic myelopathy (CSM), or the lateral neural foramina, resulting in cervical radiculopathy. Radiculopathy typically manifests as a constellation of sharp, radiating pain, paresthesias, and motor weakness in a specific myotomal distribution. Conversely, myelopathy presents with more insidious, upper motor neuron signs, including gait instability, loss of fine motor dexterity, hyperreflexia, and in advanced cases, bowel or bladder dysfunction.
Understanding the distinction between soft disc herniations and hard spondylotic osteophytes is critical for operative planning. Soft disc herniations, often acute or subacute, involve the extrusion of nuclear material through an annular defect, directly compressing the neural elements. Hard discs, or osteophyte complexes, represent a chronic, calcified progression of the degenerative cascade. Furthermore, the ossification of the posterior longitudinal ligament (OPLL) presents a unique and challenging patho-epidemiological entity, particularly prevalent in East Asian populations, which can cause profound ventral cord compression. Differentiating these etiologies dictates not only the necessity of surgery but the specific nuances of the intraoperative decompression strategy.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel ever touches the skin, a profound, three-dimensional understanding of the regional anatomy is absolutely paramount. We are operating within a highly constrained, critical corridor, fraught with vital neurovascular and visceral structures. The anterior approach exploits a natural internervous and intermuscular plane, but straying even millimeters from the correct trajectory can result in catastrophic iatrogenic injury.
The Intervertebral Disc and Ligamentous Structures
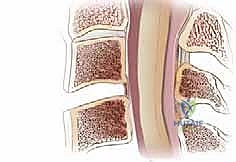
The intervertebral disc, our primary surgical target, is a complex, avascular structure composed of the tough, fibrous outer annulus fibrosus and the gelatinous, hydrophilic central nucleus pulposus. The annulus is composed of highly organized concentric lamellae of type I collagen, designed to resist tensile and torsional forces. The nucleus, rich in proteoglycans and type II collagen, acts as a shock absorber, distributing compressive loads across the vertebral endplates. It is intimately attached to the subchondral bone of the adjacent vertebral bodies via the cartilaginous endplates. Notably, the outermost rim of the vertebral endplate (the epiphyseal ring) lacks this direct cartilaginous attachment, creating a ring of exposed bone that is highly osteogenic and prone to forming the arthrotic spurs we frequently encounter.

Dorsally, defining the anterior boundary of the spinal canal, we encounter the posterior longitudinal ligament (PLL). This is a smooth, shiny, dense band of connective tissue that courses along the posterior surface of the vertebral bodies from the axis to the sacrum. In the cervical spine, it is distinctly double-layered; the deep layer spans single intervertebral segments, while the superficial layer spans multiple levels. The PLL is typically thickest centrally, providing a robust barrier against central disc herniations, but it dramatically thins laterally as it approaches the uncinate processes. This lateral attenuation explains the higher propensity for paracentral and foraminal disc herniations. Pathologic hypertrophy or ossification of this ligament (OPLL) is a major cause of ventral spinal cord compression and requires meticulous surgical management.
Anteriorly, the anterior longitudinal ligament (ALL) forms a wide, dense band, intimately associated with the anterior aspect of the intervertebral discs and vertebral bodies. It acts as a primary restraint against hyperextension. During our surgical exposure, the ALL must be sharply incised and elevated as subperiosteal flaps to expose the disc space and provide a bleeding bone bed for subsequent plate fixation. The careful elevation of the ALL and the underlying longus colli musculature is critical not only for exposure but for protecting the laterally situated sympathetic chain.


Uncovertebral Joints and Neural Foramina
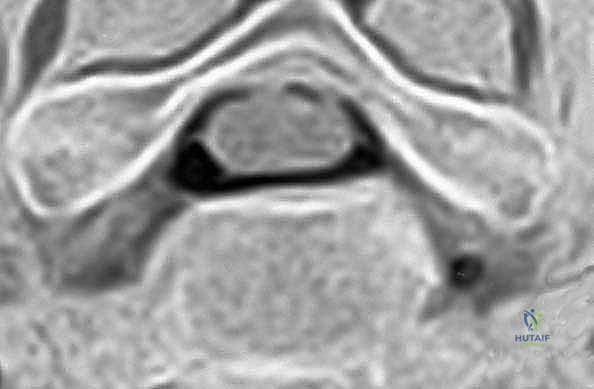
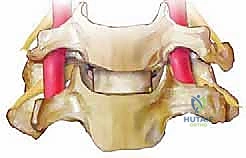
The uncovertebral joints, also known as the joints of Luschka, are critical anatomical and surgical landmarks in the cervical spine. These are posterolateral articulations formed between the uncinate processes—bony elevations on the superolateral margins of the inferior vertebral body—and the corresponding beveled inferolateral surfaces of the superior vertebral body. While not true synovial joints in early life, they develop synovial-like cavities due to the mechanical clefting of the lateral annulus over time. Spondylotic spurs commonly arise from these articulations, projecting medially into the spinal canal or laterally into the neural foramen, causing insidious impingement of the exiting nerve roots.
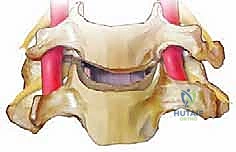
Each cervical spinal nerve is formed by the confluence of the dorsal (sensory) and ventral (motor) roots within the neural foramen. The spatial relationship here is highly specific: the ventral root lies immediately dorsal to the uncovertebral joint, making it highly susceptible to compression from uncinate osteophytes. Conversely, the dorsal root is situated ventral to the superior articular facet, making it vulnerable to facet arthrosis.
Crucially for the operating surgeon, the exiting nerve root leaves the spinal cord and traverses the foramen at approximately a 45-degree ventrolateral angle in the axial plane, and a slightly caudal trajectory in the sagittal plane. This exact 45-degree angulation is vital to visualize mentally during an anterior foraminotomy. When resecting the posterior uncinate process to decompress the root, the burr or curette must parallel this trajectory. Deviating too medially risks spinal cord injury, while deviating too laterally or anteriorly risks catastrophic injury to the vertebral artery.

Neurovascular Relationships and Surgical Corridors
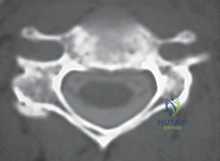
The vertebral artery represents the most feared vascular structure during anterior cervical surgery. It typically enters the transverse foramen at C6 and ascends vertically through the foramina up to C1. While working within the central confines of the posterior disc space during a standard decompression, the vertebral artery is generally safe, as it is located laterally, roughly at the level of the middle third of the vertebral body in the sagittal plane.
However, the margin of error is razor-thin. Depending on the specific cervical level and individual anatomical variations, the vertebral artery can be located as close as 5 mm from the medial border of the uncinate process. Furthermore, anatomical variations such as a medial loop or an aberrant entry level (e.g., entering at C5 or C7) are not uncommon. This proximity mandates extreme caution, copious visualization, and precise burr control when performing lateral decompression or uncovertebral osteophyte resection. The trajectory of our discectomy should always be strictly bounded by the medial borders of the uncinates, only widening posteriorly at the precise level of the nerve root to achieve thorough foraminal decompression while maintaining a safe distance from the artery.

Beyond the vertebral artery, the anterior approach requires navigation past several critical soft-tissue structures. The carotid sheath, containing the common carotid artery, internal jugular vein, and vagus nerve, must be carefully mobilized and retracted laterally. Medially, the visceral axis, comprising the trachea and esophagus, is retracted. The recurrent laryngeal nerve (RLN), which controls the vocal cords, is highly vulnerable. On the right side, its course is more variable and oblique, crossing from lateral to medial, making it theoretically more susceptible to stretch injury during right-sided approaches. On the left, it has a more predictable, vertical course within the tracheoesophageal groove. Additionally, the sympathetic trunk lies on the ventral surface of the longus colli muscle; aggressive lateral dissection or improper retractor placement can result in Horner's syndrome.


Exhaustive Indications and Contraindications
The decision to proceed with an ACDF must be grounded in a rigorous correlation of the patient's clinical presentation, physical examination findings, and advanced neuroimaging. Surgery is never indicated solely on the basis of abnormal imaging, as asymptomatic degenerative changes are highly prevalent in the general population. The primary goal of surgery is the relief of neural compression and the restoration of mechanical stability.
The most common indication for ACDF is cervical radiculopathy that has proven refractory to a comprehensive trial of nonoperative management, typically lasting 6 to 12 weeks. This nonoperative regimen should include targeted physical therapy, non-steroidal anti-inflammatory medications, oral corticosteroids, and potentially image-guided cervical epidural steroid injections. If the patient experiences persistent, debilitating radicular pain, or if there is evidence of progressive motor weakness in a specific myotome (e.g., progressive deltoid weakness from a C5 radiculopathy), surgical intervention is warranted.
Cervical spondylotic myelopathy (CSM) presents a more urgent indication. Unlike radiculopathy, the natural history of myelopathy is characterized by a stepwise, progressive neurological decline. Once clinical signs of spinal cord compression are evident—such as hyperreflexia, a positive Hoffman's sign, Babinski reflex, clonus, or objective gait disturbances—surgical decompression is indicated to halt the progression of the disease. ACDF is particularly well-suited for CSM when the compressive pathology is predominantly ventral and localized to the disc spaces (e.g., 1 to 3 levels).
Other indications include traumatic cervical instability, such as unilateral or bilateral facet dislocations, where the anterior approach allows for direct removal of the traumatized disc prior to reduction, preventing iatrogenic disc herniation into the canal. Anterior surgery is also indicated for the debridement and stabilization of cervical discitis/osteomyelitis, and for the resection of primary or metastatic ventral tumors.
| Indication Category | Specific Clinical Scenarios |
|---|---|
| Radiculopathy | Refractory pain > 6 weeks; Progressive motor deficit; Intractable pain failing injections. |
| Myelopathy | Clinical signs of cord compression (Hoffman, Babinski, gait issues); Ventral pathology. |
| Trauma | Facet dislocations (pre-reduction discectomy); Traumatic disc herniations with deficit. |
| Infection/Tumor | Ventral epidural abscess; Discitis/osteomyelitis; Ventral vertebral body tumors. |
| Contraindications | Absolute: Active systemic infection (unless targeted). Relative: Severe osteoporosis; Continuous OPLL > 3 levels (consider posterior); Isolated posterior compression (ligamentum flavum hypertrophy). |

Pre-Operative Planning, Templating, and Patient Positioning
Surgical success is largely dictated before the patient enters the operating room. Thorough preoperative planning minimizes intraoperative surprises, optimizes workflow, and maximizes patient safety. This begins with a meticulous review of all available imaging modalities.
Imaging and Diagnostic Studies
Plain radiographs (AP, lateral, flexion, and extension views) offer initial, critical insights into overall cervical alignment, sagittal balance, and dynamic instability. They allow for the assessment of disc height loss, the presence of anterior or posterior osteophytes, and congenital anomalies such as Klippel-Feil syndrome. Flexion-extension views are essential to rule out occult hypermobility or subluxation that might necessitate a more extensive fusion construct.
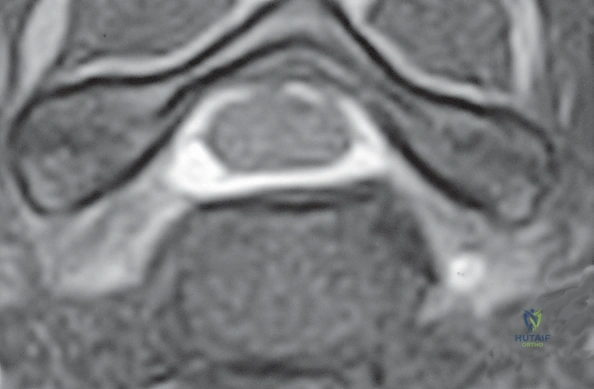
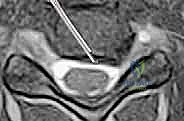
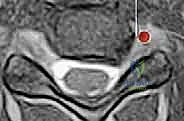
Magnetic Resonance Imaging (MRI) remains the gold standard modality for evaluating the soft tissues of the cervical spine. It provides exquisite detail of the spinal cord, nerve roots, intervertebral discs, and ligamentous structures. T2-weighted sagittal and axial images are paramount for identifying the exact level and laterality of neural compression, differentiating between soft disc herniations and intrinsic cord signal changes (myelomalacia), which correlate with a poorer prognosis for neurological recovery.

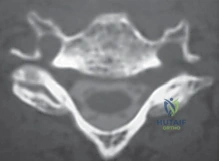
For patients with contraindications to MRI (e.g., incompatible pacemakers) or when the MRI fails to provide sufficient bony detail, a CT scan, often combined with a myelogram, is invaluable. CT provides outstanding resolution of the osseous anatomy, making it the superior modality for differentiating OPLL from soft disc herniation, and for evaluating the extent of uncovertebral and facet arthrosis. Furthermore, CT is critical for mapping the trajectory of the vertebral artery, identifying anomalies such as a tortuous V2 segment that might encroach medially into the surgical field.
Electromyography (EMG) and Nerve Conduction Studies (NCS) are useful adjuncts, particularly when the clinical picture is confounded by peripheral nerve entrapment syndromes (e.g., carpal or cubital tunnel syndrome) or when imaging findings do not perfectly correlate with the patient's symptoms. These neurodiagnostic tests can help isolate the exact level of radicular impairment and differentiate an acute radiculopathy from chronic, inactive nerve damage.


Patient Positioning and Setup
Proper patient positioning is a critical, highly specific step that facilitates exposure and dictates the ease of the entire procedure. The patient is placed supine on a radiolucent operating table. The head is carefully supported, typically resting on a foam doughnut or a specialized headrest, ensuring the occiput is protected from pressure necrosis.
A rolled towel or an intravenous fluid bag (a "bump") is placed transversely beneath the patient's scapulae. This maneuver allows the shoulders to fall posteriorly and facilitates a gentle extension of the cervical spine. This extension naturally opens the anterior disc spaces, making the surgical corridor more accessible. However, extreme caution must be exercised: the degree of intraoperative extension must never exceed the amount of extension the patient could tolerate preoperatively without exacerbating their neurological symptoms. In patients with severe, tight canal stenosis, hyperextension can induce a dynamic cord injury.


To ensure unimpeded fluoroscopic visualization of the lower cervical levels (C6, C7, T1), the patient's arms are tucked tightly at their sides. Broad adhesive tape is applied to the shoulders and pulled caudally, securing it to the foot of the bed. This depresses the clavicles and shoulders out of the radiographic trajectory. Before prepping, the C-arm is brought in to confirm that crystal-clear, true lateral and AP views of the target surgical levels can be obtained. If neuromonitoring (SSEP and MEP) is utilized, baseline signals are obtained after positioning but before the incision is made.
Step-by-Step Surgical Approach and Fixation Technique
With the patient optimally positioned and prepped, we begin the operative execution. The standard Smith-Robinson approach is utilized, providing a highly versatile, extensile window to the anterior cervical spine from C2 down to T2.
Incision, Dissection, and Exposure
The incision is typically planned in a transverse skin crease to optimize the cosmetic outcome. For a single or two-level ACDF, a transverse incision is sufficient; for three or more levels, an oblique longitudinal incision along the anterior border of the sternocleidomastoid (SCM) may be required. The level of the incision is estimated using palpable anatomical landmarks: the angle of the mandible (C2-C3), the hyoid bone (C3), the thyroid cartilage (C4-C5), and the cricoid cartilage (C6).

The skin and subcutaneous tissues are incised, and the platysma muscle is identified. The platysma is divided in line with the skin incision. Subplatysmal flaps are then developed superiorly and inferiorly using blunt and sharp dissection, which mobilizes the skin window and greatly enhances the deep exposure. The superficial cervical fascia is incised, and the avascular intermuscular plane between the sternocleidomastoid muscle (laterally) and the strap muscles (sternohyoid and sternothyroid, medially) is identified and developed using blunt finger dissection or Kittner dissectors.
Deepening the dissection, the carotid sheath is palpated. The sheath, containing the carotid artery laterally, must be gently mobilized and retracted laterally. The visceral axis, consisting of the trachea and esophagus, is retracted medially. Hand-held retractors (such as Army-Navy or Cloward retractors) are initially used to maintain this interval. The prevertebral fascia, which covers the longus colli muscles and the anterior longitudinal ligament, is now visible. It is sharply incised longitudinally in the midline. At this stage, a spinal needle is inserted into the presumed target disc space, and a lateral fluoroscopic image is taken to definitively confirm the correct surgical level.
Discectomy and Neural Decompression
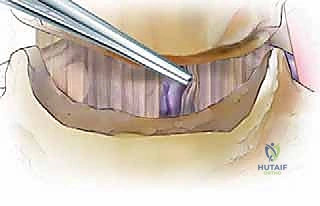
Once the level is confirmed, the medial borders of the longus colli muscles are elevated off the vertebral bodies bilaterally using a Bovie electrocautery and Cobb elevators. This exposes the full width of the anterior disc space and the uncinate processes laterally. Self-retaining retractors with toothed blades are carefully placed beneath the elevated longus colli muscles. Care must be taken to ensure the retractor blades are securely seated beneath the muscle bellies to prevent slippage and to protect the sympathetic chain and the esophagus.
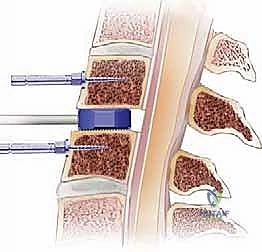
Caspar distraction pins are placed into the exact midline of the vertebral bodies superior and inferior to the target disc. A distractor is applied, and gentle, controlled distraction is utilized to open the disc space, restoring foraminal height and facilitating visualization. A radical annulotomy is performed using a #15 blade. The bulk of the intervertebral disc is then systematically removed using a combination of pituitary rongeurs, straight and angled curettes.
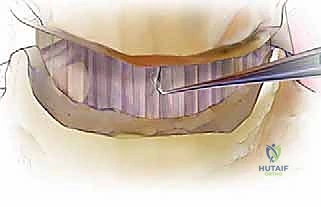
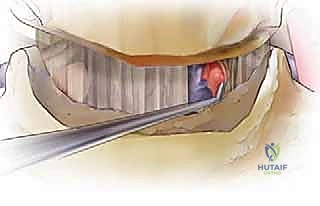
The decompression must proceed posteriorly until the posterior longitudinal ligament (PLL) is encountered. Using a high-speed burr (typically a 3mm or 4mm cutting burr, followed by a diamond burr), the cartilaginous endplates are decorticated, and any posterior osteophytes projecting from the superior or inferior vertebral bodies are thinned down until they can be fractured away from the dura using micro-curettes or Kerrison rongeurs. The decision to resect the PLL is dictated by the pathology; if a soft disc herniation has extruded behind the ligament, or if the ligament is hypertrophied and contributing to stenosis, it must be carefully elevated with a micro-hook and resected using a 1mm or 2mm Kerrison rongeur, fully exposing the underlying dura.
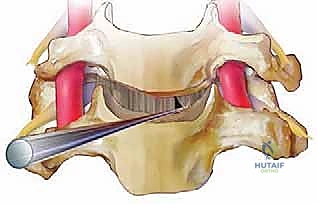
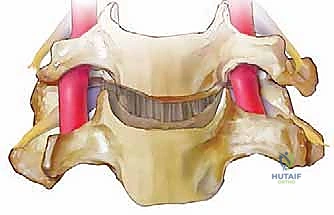
Bilateral foraminotomies are performed by following the uncinate processes posteriorly. The medial aspect of the uncinate is thinned with a burr and removed with a micro-Kerrison to unroof the neural foramen. The surgeon must maintain the critical 45-degree ventrolateral trajectory, hugging the posterior aspect of the uncinate to safely decompress the exiting nerve root while avoiding the vertebral artery located immediately lateral to the uncinate complex.
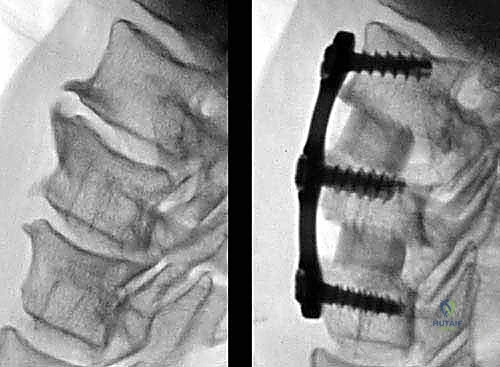
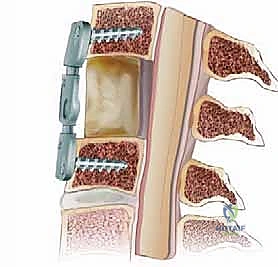
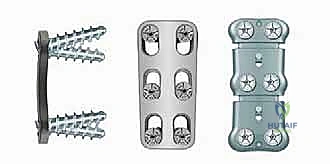
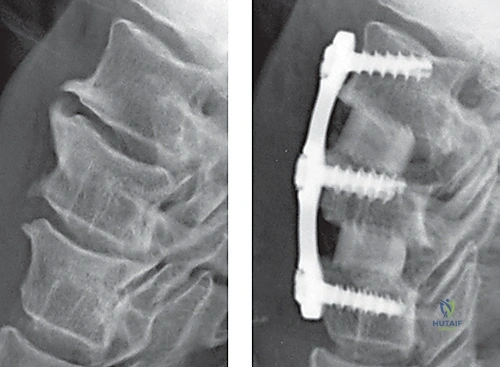
Interbody Grafting and Anterior Plating
With the spinal cord and nerve roots fully decompressed and pulsatile, attention turns to reconstruction. The cartilaginous endplates have been meticulously removed to expose bleeding subchondral bone, which is essential for arthrodesis. However, excessive burring must be avoided to prevent weakening the structural integrity of the endplate, which could lead
Clinical & Radiographic Imaging Archive