Anterior Approach for Open Reduction of Developmental Dysplasia of the Hip: A Masterclass

Key Takeaway
Join us in the OR for an immersive masterclass on the anterior approach for open reduction of developmentally dislocated hip (DDH). We'll meticulously dissect the anatomy, execute each surgical step with precision, and navigate potential pitfalls. This comprehensive guide ensures fellows gain a deep understanding of technique, rationale, and patient management for optimal outcomes in pediatric hip surgery.
Comprehensive Introduction and Patho-Epidemiology
Developmental dysplasia of the hip (DDH) represents one of the most profound challenges and rewarding pathologies managed by the pediatric orthopedic surgeon. The anterior approach for open reduction is not merely a technical exercise; it is a fundamental intervention designed to alter the natural history of a deteriorating joint, restoring a child's potential for normal biomechanical development and lifelong function. DDH is a complex spectrum disorder that affects the stability, morphology, and development of the hip joint, originating either in utero or manifesting postnatally. The pathology ranges from mild acetabular dysplasia and micro-instability to severe subluxation and frank, irreducible dislocation.
Understanding the underlying pathology and the natural history of the disease is paramount to achieving a successful outcome. The epidemiology of DDH reveals a multifactorial etiology, with genetic predispositions intertwining with mechanical factors. Risk factors such as female sex, breech presentation, oligohydramnios, and a positive family history are well documented. However, the absence of these risk factors does not preclude the diagnosis, necessitating high clinical vigilance. Untreated, the natural history of hip dysplasia with subluxation or dislocation is predictably poor, leading inexorably to early, debilitating degenerative joint disease. Clinical symptoms, typically pain and gait disturbances, can precede radiographic deterioration by a decade. Complete dislocation results in limb-length discrepancy, compensatory lumbar hyperlordosis, and adjacent joint degeneration.
Hips that are well-centered in childhood often demonstrate remarkable remodeling potential, showing improvement in acetabular dysplasia, though not always returning to absolute normative values. Conversely, radiologically eccentric hips typically do not improve and are destined for early osteoarthritis. In mature hips, a center-edge angle of Wiberg measuring less than 20 degrees strongly predicts the onset of symptomatic arthritis by the third or fourth decade of life. Therefore, the goal of open reduction is to achieve and maintain a concentric, stable reduction without excessive pressure, thereby providing the optimal mechanical environment for the acetabulum and proximal femur to remodel during the remaining years of skeletal growth.


Detailed Surgical Anatomy and Biomechanics
Embryology and Osseous Development
Surgical success in DDH hinges entirely on a profound appreciation of the delicate, evolving anatomy of the pediatric hip. In the first trimester, the joint structures begin as a single mass of scleroblastema, with the femoral head becoming cartilaginous by six weeks of gestation. By eight weeks, vascular invasion initiates enchondral ossification. The joint space itself develops through a process of programmed cell death and cleft formation between seven and eight weeks, and the basic joint structure is well apparent by week eleven. The proximal femur initially forms as a single chondroepiphysis. The ossific nucleus typically appears in infancy, between two and eight months of age. Side-to-side size discrepancies in its appearance can be normal, but delayed ossification is a hallmark of dysplasia.
A crucial biomechanical concept is the Heuter-Volkmann principle: a round, concentrically reduced femoral head serves as the primary mechanical stimulus for the acetabulum to develop its concave, spherical shape. Without this constant, concentric pressure, we observe the characteristic dysplastic changes. The acetabulum, which is a deep hemisphere in the first two trimesters, becomes shallower by birth, contributing to the inherent instability seen in neonates. An absent or chronically subluxated femoral head leads to a flat, egg-shaped acetabulum, a consistent finding in long-standing DDH. By eight years of age, the acetabular shape is largely determined, making surgical reduction significantly more challenging and often necessitating concomitant pelvic osteotomies.

Soft Tissue Obstacles to Reduction
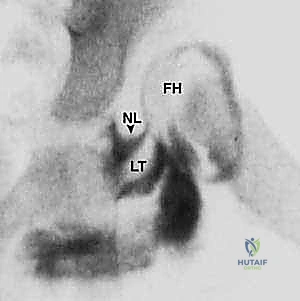
When performing an open reduction, the surgeon must systematically identify and address the anatomical blocks to concentric reduction. These obstacles are predictable and must be meticulously cleared. Extracapsularly, the primary deforming force is the contracted iliopsoas tendon, which creates an hourglass constriction of the joint capsule as it crosses anteriorly. Intracapsularly, the obstacles include a hypertrophic, elongated ligamentum teres, which occupies the depth of the acetabulum. The pulvinar, a pad of fibrofatty tissue at the base of the acetabulum, hypertrophies in the absence of the femoral head and must be excised.
The transverse acetabular ligament (TAL), which spans the acetabular notch inferiorly, often contracts and acts as a tension band, physically blocking the inferior descent of the femoral head into the true acetabulum. Finally, the acetabular labrum, which normally resembles an O-ring providing mechanical stability and proprioceptive feedback, can become inverted into the joint space. With chronic dislocation, an abnormally formed ridge of articular cartilage, termed the neolimbus, can develop at the edge of the acetabulum, acting as a significant barrier.
Vascular Anatomy and the Risk of Avascular Necrosis
The vascularity of the proximal femur is the most critical anatomical consideration during this procedure. The femoral head's blood supply in the pediatric patient is predominantly derived from the medial circumflex femoral artery (MCFA), with variable, lesser contributions from the lateral circumflex femoral artery (LCFA). These vessels form an extracapsular arterial ring at the base of the femoral neck, giving rise to the ascending retinacular arteries. These delicate vessels travel intracapsularly along the femoral neck to supply the chondroepiphysis.
Because the femoral head is an intra-articular, dome-shaped structure, this blood supply is exquisitely susceptible to iatrogenic injury. Excessive capsular stripping, particularly inferiorly and posteriorly, can directly transect these vessels. Furthermore, forceful reduction maneuvers or immobilization in extreme abduction (the "frog-leg" position) can cause mechanical tamponade of the retinacular vessels against the acetabular rim, leading to ischemia. Compromise of this blood supply results in avascular necrosis (AVN), a devastating complication that severely compromises the long-term outcome, leading to growth arrest, coxa breva, and premature osteoarthritis.


Exhaustive Indications and Contraindications
The decision to proceed with an anterior open reduction requires careful patient selection, timing, and an understanding of the limitations of conservative management. The anterior approach (Smith-Petersen) is the workhorse for DDH open reduction, offering excellent visualization of the anterior capsule, the iliopsoas tendon, and the entire acetabular rim, making it superior to the medial approach for older children or those requiring concomitant pelvic osteotomies.
| Parameter | Indications for Anterior Open Reduction | Contraindications for Anterior Open Reduction |
|---|---|---|
| Age | Typically 6 months to 3 years (often up to 8 years with concurrent bony procedures). | Infants < 6 months (unless teratologic or failed extensive closed management). |
| Prior Treatment | Failure of closed reduction and spica casting; failure of Pavlik harness. | Successful, stable closed reduction achievable without excessive force. |
| Pathology | Teratologic dislocations (e.g., Arthrogryposis, Spina Bifida) requiring early open reduction. | Active joint infection or untreated septic arthritis. |
| Anatomical Factors | Need for concomitant pelvic osteotomy (e.g., Salter, Pemberton) or femoral shortening. | Severe, uncorrected neuromuscular spasticity precluding postoperative stability. |
| Imaging | Interposed soft tissues (inverted labrum, hypertrophic pulvinar) identified on MRI/Arthrogram. | Medical comorbidities precluding safe general anesthesia. |
Pre-Operative Planning, Templating, and Patient Positioning
Comprehensive Clinical Evaluation
Before we even consider making an incision, meticulous preoperative planning is non-negotiable. Every newborn must receive a gentle, focused hip examination, including range of motion assessments and the Ortolani and Barlow maneuvers. An Ortolani-positive hip indicates a dislocation or subluxation that partially reduces with abduction—characterized by a distinct, palpable "clunk" as the femoral head relocates over the posterior acetabular rim. In older, walking-age children, the clinical picture shifts. Look for abnormal skin creases, though these are non-specific. Limited hip abduction in flexion is a highly reliable sign of a fixed deformity and adductor contracture.
A delay in walking is often the first indicator noted by parents. The Galeazzi sign, demonstrating apparent shortening of the thigh with the child supine and knees flexed, indicates a dislocated hip or a congenital short femur. A Trendelenburg gait, characterized by pelvic dipping on the contralateral side and a compensatory shoulder lurch, indicates mechanical insufficiency of the hip abductors due to the shortened lever arm of the dislocated hip. Always inspect the upper extremities, spine, and feet to rule out syndromic conditions.
Advanced Imaging and Diagnostic Studies
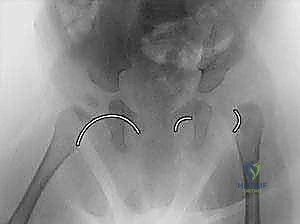
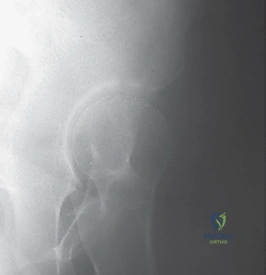
Imaging directly complements our clinical findings and dictates the surgical strategy. Ultrasound is the gold standard for infants up to six months of age, providing dynamic assessment of stability and morphological data (alpha and beta angles). Once the proximal femoral ossific nucleus appears, typically around four to six months, the anteroposterior (AP) radiograph becomes the primary modality. We meticulously evaluate the Shenton line—a continuous arch formed by the medial border of the femoral neck and the superior border of the obturator foramen. A break in this line indicates subluxation or dislocation. We also measure the acetabular index to quantify dysplasia.
Cross-sectional imaging, particularly MRI with or without intra-articular gadolinium, is increasingly utilized. It is unparalleled for visualizing non-ossified structures, assessing the condition of the articular cartilage, identifying an inverted labrum, and evaluating for early signs of osteonecrosis. Intraoperative arthrography is an essential adjunct. We utilize it immediately prior to incision to define the anatomical blocks to reduction, confirm the concentricity of any provisional reduction, and assess the dynamic stability of the joint.


Differential Diagnosis
Always consider alternative pathologies that can present with hip instability, leg length discrepancy, or a limp in the pediatric population. The differential diagnosis includes septic arthritis of the hip (which can lead to pathological dislocation and rapid joint destruction), proximal focal femoral deficiency (PFFD), congenital coxa vara, and neuromuscular dysplasia (such as that seen in cerebral palsy or myelomeningocele). Differentiating typical DDH from a teratologic dislocation is critical, as the latter is significantly more rigid, responds poorly to conservative measures, and requires earlier, more aggressive surgical intervention.
Patient Positioning and Setup
The patient is placed supine on a radiolucent operating table. A small bump is placed under the ipsilateral hemipelvis to elevate the operative side slightly, allowing the lower extremity to fall into natural external rotation, which aids in the initial dissection. The entire lower extremity, from the toes to the costal margin, must be prepped and draped free to allow for unrestricted manipulation of the hip during the reduction maneuvers and to facilitate intraoperative fluoroscopy. A sterile tourniquet is not typically used. The C-arm fluoroscopy unit is positioned to allow seamless AP and frog-leg lateral views of the pelvis without compromising the sterile field.
Step-by-Step Surgical Approach and Fixation Technique
The Incision and Superficial Dissection
The procedure begins with a meticulously planned "bikini line" incision, which offers superior cosmetic results compared to the traditional longitudinal Smith-Petersen incision, while providing equivalent deep exposure. The incision starts just inferior and lateral to the anterior superior iliac spine (ASIS) and follows the natural Langer's lines obliquely downward and medially. The subcutaneous tissues are divided in line with the incision. Hemostasis is achieved using electrocautery.
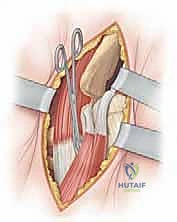
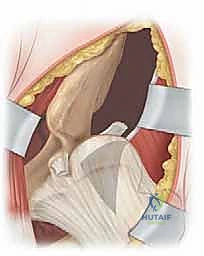
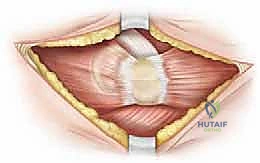
The superficial fascia is incised, and the interval between the sartorius muscle (innervated by the femoral nerve) and the tensor fasciae latae (TFL, innervated by the superior gluteal nerve) is identified. This is the classic Smith-Petersen internervous plane. Blunt dissection is utilized to separate these muscles. Extreme caution must be exercised at the proximal extent of this interval to identify and protect the lateral femoral cutaneous nerve (LFCN), which typically courses over or just medial to the sartorius. Retraction of the LFCN medially with the sartorius is generally preferred to prevent traction neurapraxia.

Deep Dissection and Iliopsoas Tenotomy
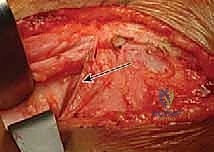
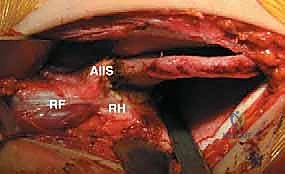
Deep to the sartorius and TFL, the rectus femoris muscle comes into view. The direct head of the rectus femoris originates from the anterior inferior iliac spine (AIIS), and the reflected head originates from the superior rim of the acetabulum. Both heads are identified, tagged with a non-absorbable suture, and transected near their origins to expose the underlying joint capsule. This step is crucial for adequate exposure of the anterior and superior acetabular rim.
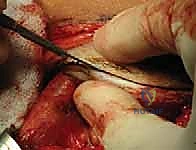
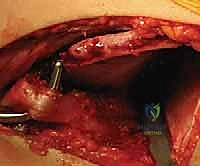
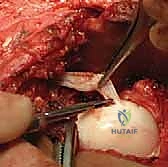
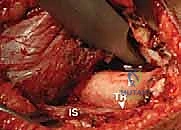
Next, we address the iliopsoas tendon. The hip is flexed, abducted, and externally rotated to bring the lesser trochanter and the iliopsoas tendon anteriorly. The tendon is identified as it crosses the anterior capsule. A blunt right-angle retractor is passed deep to the tendon to protect the medial structures, specifically the femoral nerve and vessels. The tendinous portion of the iliopsoas is then transected at the level of the pelvic brim, allowing the muscle belly to retract proximally. This fractional lengthening or tenotomy is a mandatory step; it eliminates the hourglass constriction of the capsule and significantly reduces the joint reaction forces post-reduction, mitigating the risk of AVN.

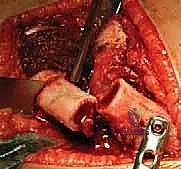
Capsulotomy and Clearing the Acetabulum
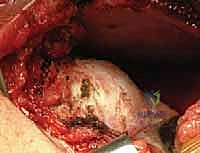
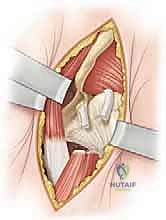
With the anterior capsule fully exposed, a capsulotomy is performed. An I-shaped or T-shaped incision is typical. The vertical limb is made parallel to the femoral neck, staying anterior to avoid the retinacular vessels located superiorly and inferiorly. The transverse limb is made parallel to the acetabular rim, leaving a small cuff of capsule attached to the rim for later repair. Stay sutures are placed in the capsular flaps.
Upon entering the joint, the obstacles to reduction must be systematically excised. The ligamentum teres is identified, grasped with a clamp, and excised at its base using electrocautery or scissors. The acetabulum is often filled with a hypertrophic pulvinar, which is meticulously removed using a pituitary rongeur or a curette, revealing the true medial wall (the teardrop on a radiograph). The transverse acetabular ligament (TAL) is identified at the inferior aspect of the acetabulum. If it is contracted and blocking the inferior seating of the femoral head, it is carefully incised radially. Finally, the labrum is inspected. An inverted labrum must be gently everted; it should rarely be excised, as it provides crucial stability and proprioception.
Reduction, Assessment of Stability, and Capsulorrhaphy
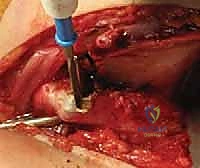
With the acetabulum cleared, the femoral head is gently reduced into the true acetabulum using a combination of traction, flexion, abduction, and internal rotation. Forceful manipulation must be strictly avoided. Once reduced, the stability of the joint is dynamically assessed. The "safe zone" of Ramsey is determined: this is the arc of motion between the angle of maximum abduction (limited by adductor tension) and the angle of adduction at which the hip subluxates or redislocates. If the safe zone is narrow, or if excessive internal rotation is required to maintain reduction, a concomitant femoral derotation osteotomy or a pelvic osteotomy (e.g., Salter innominate osteotomy) may be indicated.
If the reduction is stable and concentric, a meticulous capsulorrhaphy is performed. This is a critical step to eliminate capsular redundancy and provide anterior stability. The inferior capsular flap is advanced superiorly and medially, and the superior flap is brought inferiorly, creating a "vest-over-pants" imbrication. The repair must be tight enough to maintain reduction but not so tight as to restrict motion or compress the microvasculature. The rectus femoris is reattached to its origin, and the wound is closed in layers.


Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, open reduction of DDH carries significant risks. The surgeon must be prepared to identify and manage these complications promptly.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Prevention |
|---|---|---|---|
| Avascular Necrosis (AVN) | 5% - 15% | Injury to medial circumflex vessels; extreme abduction in spica cast; forceful reduction. | Prevention is key. Avoid extreme abduction (>50°). Kalamchi-MacEwen classification guides long-term management (e.g., trochanteric epiphysiodesis for overgrowth). |
| Redislocation / Subluxation | 2% - 8% | Incomplete clearing of acetabulum (missed inverted labrum, intact TAL); inadequate capsulorrhaphy; unrecognized bony dysplasia. | Immediate re-operation. Re-explore the joint, clear remaining obstacles, perform capsulorrhaphy, and consider concurrent pelvic/femoral osteotomy. |
| Nerve Injury (LFCN / Femoral) | 1% - 3% | Traction neurapraxia during retraction; direct transection during superficial dissection. | Careful dissection in the Smith-Petersen interval. Avoid excessive medial retraction of the sartorius/iliopsoas. Most are transient and resolve with observation. |
| Joint Stiffness | Variable | Prolonged immobilization; extensive capsular scarring; unrecognized chondrolysis. | Limit spica cast duration to the minimum necessary (typically 6-12 weeks). Encourage early, gentle range of motion upon cast removal. |
| Surgical Site Infection | < 1% | Contamination during surgery or via spica cast soiling. | Strict sterile technique. Meticulous spica cast care. Treat superficial infections with oral antibiotics; deep infections require urgent irrigation and debridement. |
Phased Post-Operative Rehabilitation Protocols
Immediate Post-Operative Immobilization: The Spica Cast
The immediate post-operative phase relies entirely on secure, well-molded immobilization to protect the capsulorrhaphy and maintain the concentric reduction while soft tissue healing occurs. While the patient is still under general anesthesia, a one-and-a-half or bilateral hip spica cast is applied. The position of the hip within the cast is of paramount importance. The hip is placed in the "human position" described by Salter: approximately 100 to 105 degrees of flexion, 40 to 50 degrees of abduction, and neutral rotation.
Crucially, the surgeon must actively avoid the "frog-leg" position (extreme abduction). Extreme abduction forces the femoral neck against the posterior acetabular rim, compressing the delicate retinacular vessels and drastically increasing the risk of avascular necrosis. The cast must be carefully molded over the greater trochanters to apply a gentle, medially directed force, further stabilizing the reduction. Post-operative imaging, typically a CT scan or an AP radiograph through the cast, is mandatory to confirm that the reduction has been maintained during the casting process.

Transition to Bracing and Long-Term Surveillance
The total duration of spica cast immobilization typically ranges from six to twelve weeks, depending on the child's age, the stability of the intraoperative reduction, and whether concomitant bony procedures were performed. A cast change under general anesthesia is often performed at the six-week mark to accommodate growth, assess stability, and ensure skin integrity.
Following the removal of the final spica cast, the child is transitioned to a rigid abduction orthosis (such as an Ilfeld or Atlanta brace) to be worn full-time, except for bathing, for an additional six to twelve weeks. This allows for the gradual return of joint motion while protecting against adduction and subluxation. Physical therapy is generally not required in young children, as normal play and mobility will naturally restore range of motion and muscle strength.
Long-term radiographic surveillance is absolute dogma in the management of DDH. Patients must be followed with serial AP pelvis radiographs annually or biannually until skeletal maturity. We meticulously monitor the development of the acetabular index, the center-edge angle, and the morphology of the femoral head to ensure ongoing favorable remodeling. Should residual acetabular dysplasia persist or become apparent as the child grows, secondary reconstructive procedures, such as a Pemberton or Dega osteotomy in the young child, or a periacetabular osteotomy (PAO) in the adolescent, must be considered to prevent the onset of early osteoarthritis.
Summary of Landmark Literature and Clinical Guidelines
The modern approach to the open reduction of DDH is built upon the foundational work of pioneers in pediatric orthopedics. Robert Salter’s seminal work in the 1960s revolutionized our understanding of the pathoanatomy of DDH and established the principles of concentric reduction and the
