Transfibular Ankle Arthrodesis: An Intraoperative Masterclass for End-Stage Arthritis

Key Takeaway
This masterclass provides a comprehensive, scrubbed-in guide to transfibular ankle arthrodesis for end-stage arthritis. We meticulously detail preoperative planning, patient positioning, and the step-by-step intraoperative execution, emphasizing critical anatomy, neurovascular protection, and precise joint preparation. Fellows will gain insights into surgical pearls, potential pitfalls, and comprehensive postoperative management for optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
End-stage ankle arthritis represents a profoundly debilitating clinical entity, characterized by the progressive, irreversible destruction of the articular cartilage between the tibial plafond and the talar dome. Unlike the hip and knee, where primary osteoarthritis predominates, the etiology of ankle arthritis is overwhelmingly post-traumatic. Epidemiological data suggests that up to seventy to eighty percent of end-stage ankle arthritides occur secondary to previous rotational ankle fractures, pilon fractures, or chronic lateral ligamentous instability. The remaining cohort comprises patients with systemic inflammatory arthritides (such as rheumatoid arthritis), neuropathic arthropathy (Charcot joint), post-infectious sequelae, and primary osteoarthritis, which is comparatively rare due to the unique biomechanical and biochemical properties of ankle articular cartilage.
The pathophysiological cascade of end-stage ankle arthritis involves not only the loss of hyaline cartilage but also profound alterations in the subchondral bone architecture. Patients develop dense subchondral sclerosis, expansive subchondral cysts, and hypertrophic marginal osteophytes that mechanically impinge during terminal ranges of motion. This structural degradation manifests clinically as intractable anterior ankle pain exacerbated by weight-bearing, a progressive loss of tibiotalar motion, and a characteristic antalgic gait. Patients frequently adopt a compensatory external rotation of the affected limb to bypass the sagittal plane stiffness of the tibiotalar joint, placing abnormal, asymmetrical stresses on the adjacent subtalar, talonavicular, and calcaneocuboid joints. Over time, this compensatory mechanism accelerates the degenerative cascade within the hindfoot and midfoot.
While total ankle arthroplasty (TAA) has experienced a renaissance over the past two decades—driven by significant advancements in implant design and instrumentation—ankle arthrodesis remains the undisputed gold standard for a substantial subset of patients. The transfibular approach to ankle arthrodesis, in particular, is an intraoperative workhorse. It offers unparalleled exposure to the tibiotalar joint, facilitates the correction of severe coronal and sagittal plane deformities, and provides a robust source of autogenous bone graft via the resected distal fibula. Arthrodesis is the preferred, and often necessary, intervention for younger, high-demand laborers, patients with profound bone loss or avascular necrosis, individuals with severe uncorrectable coronal plane deformities, and those with a history of deep joint infection or neuropathic arthropathy.
The primary objective of a transfibular ankle arthrodesis is to yield a stable, plantigrade, and painless foot that allows the patient to resume activities of daily living and moderate physical exertion. Achieving this requires meticulous preoperative planning, a profound understanding of periarticular anatomy, rigorous joint preparation, and biomechanically sound internal fixation. When executed with precision, the transfibular arthrodesis reliably eliminates tibiotalar pain and provides a durable, lifelong solution for end-stage joint destruction.
Detailed Surgical Anatomy and Biomechanics
A masterful execution of the transfibular approach demands an intimate understanding of the osseous, ligamentous, and neurovascular topography of the lateral ankle and hindfoot. The ankle joint is a highly constrained, intrinsically stable modified hinge joint. The osseous architecture consists of the trapezoidal talar dome articulating within the mortise formed by the tibial plafond, the medial malleolus, and the lateral malleolus. The articular cartilage of the ankle is notably thinner (approximately 1 to 2 mm) than that of the knee or hip, yet it withstands immense compressive forces—up to five times total body weight during the stance phase of gait. This high-load, low-surface-area biomechanical environment necessitates absolute precision when preparing the joint surfaces for arthrodesis, as any residual incongruity or malalignment will exponentially increase stress on the fixation construct and adjacent joints.
The ligamentous anatomy of the lateral ankle dictates the limits of our surgical exposure and must be managed deliberately. The syndesmotic complex, comprising the anterior inferior tibiofibular ligament (AITFL), the interosseous membrane, and the posterior inferior tibiofibular ligament (PITFL), binds the distal fibula to the tibia. During a transfibular approach, the AITFL and the distal interosseous membrane are meticulously incised to mobilize the fibula, while the PITFL is frequently preserved to act as a posterior hinge, protecting deeper structures. The lateral collateral ligamentous complex—specifically the anterior talofibular ligament (ATFL) and the calcaneofibular ligament (CFL)—must be sharply released from their fibular insertions to allow for complete reflection or resection of the distal fibula, thereby unlocking the lateral aspect of the tibiotalar joint.
Neurovascular preservation is the paramount safety concern during the superficial and deep dissection phases. The superficial peroneal nerve (SPN) is at highest risk during the anterior extension of the lateral incision. The SPN typically pierces the deep crural fascia in the anterolateral compartment approximately 10 to 12 centimeters proximal to the tip of the lateral malleolus, subsequently bifurcating into the intermediate and medial dorsal cutaneous nerves. The surgical flap must be elevated in a full-thickness manner, strictly subfascial or subperiosteal, to prevent iatrogenic transection or traction neuropraxia of these branches. Posteriorly, the sural nerve and the lesser saphenous vein course posterior to the lateral malleolus; these are protected by maintaining dissection anterior to the peroneal tendon sheath. The peroneal tendons (longus and brevis) lie within the retromalleolar groove and must be protected by elevating them en masse with the posterior soft tissue sleeve during fibular mobilization.
Biomechanically, the position of the arthrodesis is the single most critical determinant of long-term clinical success. The universally accepted optimal position for an ankle fusion is neutral dorsiflexion (0 degrees), 0 to 5 degrees of hindfoot valgus, and 5 to 10 degrees of external rotation (matching the contralateral limb). Furthermore, the talus should be translated slightly posteriorly relative to the longitudinal axis of the tibia. This posterior translation restores the normal lever arm of the Achilles tendon, reducing the energy expenditure required for toe-off during the gait cycle. Fusing the ankle in plantarflexion (equinus) is a catastrophic error, leading to a vaulting gait, severe genu recurvatum, and accelerated midfoot arthritis. Similarly, varus malalignment locks the transverse tarsal joints, resulting in a rigid, painful lateral column overload.
Exhaustive Indications and Contraindications
The decision to proceed with an ankle arthrodesis via a transfibular approach requires a nuanced evaluation of the patient's pathology, functional demands, and systemic health. While highly successful, it is an irreversible, joint-sacrificing procedure. Patient selection must be rigorous, balancing the reliable pain relief of a fusion against the inevitable loss of tibiotalar motion and the subsequent biomechanical toll on adjacent joints.
Below is a comprehensive breakdown of the indications and contraindications for transfibular ankle arthrodesis.
| Category | Specific Conditions | Clinical Rationale and Considerations |
|---|---|---|
| Absolute Indications | End-Stage Post-Traumatic Arthritis | The most common indication. Patients with severe cartilage loss, unremitting pain, and failure of all conservative modalities (bracing, injections, NSAIDs). |
| Severe Coronal/Sagittal Deformity | Arthrodesis allows for powerful deformity correction (e.g., severe varus/valgus) that would preclude the use of a total ankle arthroplasty. | |
| Neuropathic Arthropathy (Charcot) | TAA is absolutely contraindicated in Charcot joints. Arthrodesis, often utilizing robust multi-planar fixation or intramedullary nails, is required for stability. | |
| Paralytic Deformity / Drop Foot | In cases of permanent neuromuscular compromise, fusion provides a stable, plantigrade foot, eliminating the need for rigid AFO bracing. | |
| Failed Total Ankle Arthroplasty | A salvage procedure for aseptic loosening, subsidence, or periprosthetic joint infection (following a staged eradication protocol). | |
| Relative Indications | Avascular Necrosis of the Talus | If AVN involves >50% of the talar body, isolated ankle fusion may fail. Tibiotalocalcaneal (TTC) fusion or massive allograft reconstruction may be required. |
| Inflammatory Arthritides | Patients with RA often have multi-joint involvement. While TAA is an option, severe bone osteopenia or deformity may necessitate arthrodesis. | |
| Absolute Contraindications | Active Deep Joint Infection | Surgery must be staged. An infected joint cannot be acutely fused with internal hardware. An antibiotic spacer and IV antibiotics must precede definitive fusion. |
| Severe Peripheral Arterial Disease | Inadequate vascular inflow (ABI < 0.4, absent pulses) guarantees wound necrosis and nonunion. Revascularization by vascular surgery is mandatory prior to orthopedic intervention. | |
| Medically Unstable Patient | Patients unable to tolerate general or regional anesthesia, or those with severe cardiopulmonary disease precluding the stress of surgery and rehabilitation. | |
| Relative Contraindications | Severe Adjacent Joint Arthritis | Pre-existing severe subtalar or talonavicular arthritis will be exacerbated by isolated ankle fusion. A TTC or pantalar fusion should be strongly considered. |
| Active Tobacco Use | Smoking increases the nonunion rate by up to 400%. Elective arthrodesis should be delayed until the patient has ceased smoking for a minimum of 4-6 weeks, confirmed by cotinine levels. | |
| Poor Soft Tissue Envelope | Prior severe trauma with thin, adherent, or grafted skin over the lateral malleolus may preclude a standard transfibular approach, necessitating an anterior or posterior approach. |
Pre-Operative Planning, Templating, and Patient Positioning
The foundation of a successful transfibular ankle arthrodesis is laid long before the patient enters the operating theater. Preoperative planning begins with a meticulous physical examination, focusing on the soft tissue envelope, neurovascular status, and the flexibility of adjacent joints. The surgeon must manually assess the subtalar joint; if subtalar motion is already severely restricted or painful, an isolated ankle fusion will likely fail to provide complete pain relief, and an extended fusion must be discussed with the patient.
Radiographic evaluation is the cornerstone of surgical planning. Standard weight-bearing anteroposterior (AP), mortise, and lateral radiographs of the ankle and foot are mandatory. The AP and mortise views allow the surgeon to assess coronal plane alignment (varus/valgus deformity) and the extent of medial or lateral bone loss. The lateral view is critical for evaluating sagittal alignment, anterior/posterior translation of the talus, and the presence of anterior osteophytes that must be resected. Furthermore, a computed tomography (CT) scan is highly recommended, if not essential, for all end-stage ankle arthritis cases. CT provides exquisite, three-dimensional detail of subchondral cysts, areas of avascular necrosis, and the true extent of bone stock available for hardware purchase. It also allows for a definitive assessment of the subtalar and transverse tarsal joints.
Preoperative templating involves determining the optimal trajectory and length of the fixation hardware. The standard construct for a transfibular arthrodesis utilizes two to three large-fragment (6.5 mm or 7.3 mm) cannulated, partially threaded cancellous screws. The "home run" screw is templated to pass from the posterior aspect of the distal tibia, across the arthrodesis site, and into the dense bone of the anterior talar neck. A second screw is templated from the medial malleolus into the lateral aspect of the talar body. If the fibula is to be retained as an onlay biological plate, additional cortical screws will be templated to secure the fibula to the tibia and talus. The surgeon must mentally rehearse the sequence of deformity correction, joint preparation, and screw placement to ensure an efficient intraoperative workflow.
Patient positioning is critical for optimal exposure and intraoperative fluoroscopy. The patient is placed supine on the operating table. A substantial bump—typically a thick blanket roll or a specialized foam wedge—is placed beneath the ipsilateral hip. This bump internally rotates the operative extremity, bringing the lateral malleolus perfectly perpendicular to the floor and allowing the surgeon direct, unhindered access to the lateral aspect of the ankle. A well-padded thigh tourniquet is applied to provide a bloodless surgical field, which is absolutely essential for identifying neurovascular structures and ensuring complete cartilage removal. The C-arm fluoroscopy unit is brought in from the contralateral side of the table. Before prepping and draping, the surgeon must verify that perfect AP, mortise, and lateral fluoroscopic images can be obtained without obstruction from the table pedestal or the contralateral leg.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of the transfibular approach requires a methodical, stepwise progression, prioritizing soft tissue respect, aggressive joint preparation, and rigid biomechanical fixation.
Incision and Deep Dissection
The approach begins with a generous curvilinear incision over the lateral aspect of the ankle. The incision starts approximately 8 to 10 centimeters proximal to the distal tip of the fibula, centered over the posterior half of the fibular shaft. It extends distally, following the contour of the fibula, and gently curves anteriorly toward the base of the fourth metatarsal, terminating just past the sinus tarsi. This length is not excessive; it is necessary to create thick, full-thickness fasciocutaneous flaps that minimize tension on the skin edges during retraction.

Using a scalpel, the incision is carried straight down through the dermis and subcutaneous fat to the level of the deep crural fascia. Meticulous hemostasis is achieved with electrocautery. The anterior flap is developed by elevating the tissue directly off the deep fascia. It is during this anterior dissection that the superficial peroneal nerve is at greatest risk. The surgeon must avoid plunging blindly into the subcutaneous fat; instead, blunt dissection with a periosteal elevator or a sponge is utilized to sweep the soft tissues anteriorly, taking the nerve with the flap.
Once the deep fascia over the fibula is exposed, a longitudinal incision is made directly over the periosteum of the lateral fibula. Anteriorly, the anterior compartment musculature is elevated subperiosteally off the fibula and the anterior interosseous membrane. Posteriorly, the peroneal tendon sheath is identified and carefully elevated subperiosteally from the retromalleolar groove, protecting the tendons and the more posterior sural nerve.
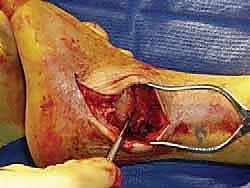
Fibular Osteotomy and Joint Exposure
With the distal fibula circumferentially exposed, the osteotomy is performed. The level of the osteotomy is typically 3 to 5 centimeters proximal to the tibiotalar joint line. Using an oscillating saw, an oblique cut is made from proximal-lateral to distal-medial. This obliquity prevents a sharp, prominent lateral bony spike that could cause postoperative hardware or soft tissue irritation.

Once the osteotomy is complete, a robust bone hook or a Lewin clamp is placed on the distal fibular fragment. The fragment is retracted laterally, placing the remaining ligamentous attachments under tension. The anterior talofibular ligament (ATFL), calcaneofibular ligament (CFL), and the anterior inferior tibiofibular ligament (AITFL) are sharply transected. The distal fibula can now be completely excised and passed to the back table to be morselized for autogenous bone graft, or it can be pedicled posteriorly on the PITFL to be used later as a vascularized lateral onlay graft. Excision of the fibula dramatically opens the lateral aspect of the tibiotalar joint, providing unparalleled visualization of the tibial plafond and talar dome.

Joint Preparation and Deformity Correction
The success of the arthrodesis hinges entirely on the quality of joint preparation. A fusion will not occur across retained cartilage or fibrous tissue. A combination of osteotomes, curettes, and a high-speed burr is used to systematically denude the articular cartilage from the tibial plafond, the talar dome, and the medial malleolar articular facet. The goal is to remove all hyaline cartilage down to bleeding subchondral bone while preserving the native contour of the joint. Aggressive, flat saw cuts should be avoided, as they shorten the limb, decrease the surface area for fusion, and inherently destabilize the construct by removing the intrinsic stability of the mortise.
Once the cartilage is removed, the sclerotic subchondral bone must be addressed. Dense, eburnated bone has poor vascularity and will inhibit cross-trabecular healing. The surgeon utilizes a sharp osteotome to perform "fish-scaling" or "shingling" of the subchondral surfaces, creating a textured, bleeding bed. Furthermore, a 2.0 mm or 2.5 mm drill bit is used to make multiple perforations into the subchondral bone of both the tibia and talus, penetrating into the vascular cancellous bone. This technique, known as subchondral drilling or microfracture, releases pluripotential marrow elements and osteoprogenitor cells into the arthrodesis site.
With the joint prepared, the deformity is corrected, and the ankle is provisionally reduced into the optimal position: neutral dorsiflexion, 0-5 degrees of valgus, and 5-10 degrees of external rotation, with slight posterior translation of the talus. This position is provisionally held using heavy, smooth Steinmann pins driven across the joint. Intraoperative fluoroscopy is mandatory at this stage to confirm absolute perfection in alignment in all three planes before definitive fixation is applied.
Definitive Internal Fixation
Rigid internal fixation is achieved using large-fragment cannulated screws. The primary screw, often termed the "home run" screw, provides the most robust biomechanical stability. A guide pin is inserted from the posterolateral aspect of the distal tibia, passing distally, anteriorly, and medially across the center of the arthrodesis site, and terminating in the dense bone of the anterior talar neck.

A second guide pin is placed from the medial malleolus, directing it distally and laterally into the central body of the talus. If a third screw is deemed necessary for rotational stability, it is typically placed from the anterolateral tibia into the posterior talar body. The screw lengths are measured, the near cortices are overdrilled to achieve a lag effect, and the appropriately sized 6.5 mm or 7.3 mm partially threaded screws are inserted over the guide pins. As the screws are tightened, the surgeon must visually confirm compression across the arthrodesis site.

If the fibula was retained as an onlay graft, its medial surface is decorticated, and it is secured to the lateral aspect of the tibia and talus using fully threaded cortical screws, bridging the fusion site and providing a massive lateral biological plate. Any remaining voids within the arthrodesis site are densely packed with the morselized cancellous bone graft harvested from the excised fibula or proximal tibia. The wound is copiously irrigated, a suction drain is optionally placed, and the soft tissues are closed in multiple layers, ensuring a tension-free skin closure.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, ankle arthrodesis carries a distinct complication profile. The surgeon must be acutely aware of these potential pitfalls, aggressively mitigate risk factors preoperatively, and possess the armamentarium to manage them if they arise.
| Complication | Estimated Incidence | Etiology and Risk Factors | Salvage and Management Strategy |
|---|---|---|---|
| Nonunion / Delayed Union | 5% - 10% | Smoking (highest risk), diabetes, inadequate joint preparation, poor fixation stability, infection, AVN of talus. | Prolonged immobilization, bone stimulators. If symptomatic, requires revision arthrodesis with structural bone grafting (iliac crest), rigid plate fixation, or transition to a TTC fusion. |
| Malunion | 3% - 8% | Intraoperative technical error, inadequate fluoroscopic evaluation, loss of fixation postoperatively. | Equinus or varus malunions are poorly tolerated. Requires revision surgery, often involving corrective osteotomies through the fusion mass and complex re-fixation. |
| Wound Dehiscence / Infection | 2% - 5% | Poor soft tissue envelope, excessive flap tension, diabetes, peripheral vascular disease, early postoperative dependency. | Superficial: Oral antibiotics, local wound care. Deep: Emergent surgical debridement, hardware removal (if loose), IV antibiotics, placement of antibiotic spacer, staged revision. |
| Adjacent Joint Arthritis | 30% - 50% (Long-term) | Biomechanical overload of the subtalar and talonavicular joints due to the loss of tibiotalar sagittal motion. | Initial conservative management (bracing, NSAIDs, injections). Definitive management requires extension of the fusion to include the symptomatic joints (e.g., subtalar arthrodesis). |
| Hardware Prominence / Pain | 10% - 15% | Prominent screw heads, especially over the medial malleolus or anterior tibia, irritating overlying soft tissues or tendons. | Once solid radiographic union is confirmed (typically >6-9 months), symptomatic hardware can be safely removed in a minor outpatient procedure. |
| Nerve Injury (SPN/Sural) | 1% - 3% | Iatrogenic transection, aggressive retraction, or entrapment in scar tissue during the surgical approach. | Prevention is key. If a neuroma develops, management includes gabapentinoids, local injections, or surgical neuroma excision and burying the nerve stump into muscle or bone. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following a transfibular ankle arthrodesis is a marathon, not a sprint. The biological process of achieving cross-trabecular bony union across the tibiotalar joint requires absolute mechanical stability and strict adherence to weight-bearing restrictions. Premature weight-bearing is the leading cause of construct failure and nonunion.
Phase 1: Immediate Postoperative Period (Weeks 0-2)
Immediately following surgery, the patient is placed in a well-padded, sterile compressive dressing and a rigid posterior plaster splint with a U-splint component to lock the ankle in neutral. The primary goals during this phase are wound healing, edema control, and pain management. The patient is strictly non-weight-bearing (NWB) on the operative extremity. Crutches, a walker, or a knee scooter are mandatory. The patient is instructed to elevate the limb strictly above the level of the heart for 23 hours a day to minimize swelling, which is the primary driver of wound dehiscence. Deep vein thrombosis (DVT) prophylaxis is initiated based on patient risk stratification.
Phase 2: Early Healing Phase (Weeks 2-6)
At the two-week mark, the patient returns to the clinic for suture removal and a wound check. If the incision is healing appropriately, the patient is transitioned into a total contact cast or a locked, rigid controlled ankle motion (CAM) boot. The patient remains strictly non-weight-bearing. Radiographs are obtained to verify that the hardware and alignment remain stable, though evidence of bony bridging will not yet be visible. The patient may begin gentle, active range of motion of the toes and isometric strengthening of the proximal musculature (quadriceps, hamstrings, gluteals) to prevent profound atrophy.
Phase 3: Progressive Weight-Bearing (Weeks 6-12)
At six weeks postoperatively, the critical clinical and radiographic assessment occurs. AP, mortise, and lateral radiographs are scrutinized for early signs of trabecular bridging across the arthrodesis site and the absence of hardware lucency. If clinical signs (lack of pain at the surgical site) and radiographic signs of early union are present, the patient is permitted to begin progressive weight-bearing in the CAM boot. This typically starts with 25% partial weight-bearing using crutches, advancing by 25% each week until full weight-bearing in the boot is achieved. Physical therapy is formally initiated to focus on gait mechanics, proprioception, and strengthening of the entire lower extremity kinetic chain.
Phase 4: Maturation and Return to Activity (Weeks 12+)
By the 10 to 12-week mark, definitive radiographic union is typically confirmed. Once solid fusion is achieved, the patient is gradually weaned from the CAM boot into a supportive, stiff-soled athletic shoe, often supplemented with a rocker-bottom modification or a solid ankle cushion heel (SACH) to facilitate the rollover phase of gait. Physical therapy intensifies, focusing on maximizing the function of the adjacent midfoot and hindfoot joints and returning the patient to their baseline occupational and recreational activities. Maximum medical improvement and final gait adaptation may take up to 12 to 18 months postoperatively.
Summary of Landmark Literature and Clinical Guidelines
The evolution of ankle arthrodesis is deeply rooted in the orthopedic literature, transitioning from highly morbid, open procedures with prolonged casting to the modern era of rigid internal fixation and early mobilization. Historically, Charnley pioneered the concept of compression arthrodesis using external fixators, demonstrating that mechanical compression significantly enhanced the biological fusion rate. However, external fixation was fraught with pin tract infections and poor patient compliance.
The paradigm shifted dramatically with the advent of rigid internal fixation. Landmark biomechanical studies in the 1980s and 1990s established the superiority of crossed-screw constructs. A seminal study by Holt et al. demonstrated that a two-screw construct provided significantly greater torsional and bending stiffness compared to single-screw or staple techniques. Further refinement by Mann and others popularized the use of the "home run" screw from the posterior tibia into the talar neck, which capitalizes on the densest bone available for thread purchase.
Modern clinical guidelines, supported by the American Orthopaedic Foot & Ankle Society (AOFAS), universally recommend joint-sparing, meticulous cartilage preparation (avoiding flat saw cuts) and rigid internal fixation with large-fragment screws or anatomic plating systems. Recent meta-analyses comparing ankle arthrodesis to total ankle arthroplasty (such as those by Zaidi et al. and the Canadian Orthopaedic Foot and Ankle Society) consistently demonstrate that while TAA provides superior sagittal motion and potentially protects adjacent joints, arthrodesis remains unparalleled in its ability to provide definitive pain relief with a lower rate of major reoperation in the medium to long term. The literature firmly supports the transfibular approach as a highly reliable technique, yielding fusion rates exceeding 90% in appropriately selected patients, solidifying its status as a foundational procedure in the orthopedic foot and ankle
