AAOS Orthopedic MCQs (Set 3): Shoulder, Elbow & Wrist Trauma | 2005 Board Review
Key Takeaway
This high-yield question set for the AAOS/ABOS exams focuses on common upper extremity pathologies. Questions cover the diagnosis, classification, and management of shoulder girdle injuries, elbow fractures, and specific wrist conditions. It is an essential resource for candidates preparing for orthopedic board certifications and residency exams.
AAOS Orthopedic MCQs (Set 3): Shoulder, Elbow & Wrist Trauma | 2005 Board Review
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 42-year-old woman with a long-standing history of rheumatoid arthritis undergoes total shoulder arthroplasty for persistent pain that has failed to respond to nonsurgical management. Intraoperative radiographs reveal an oblique, minimally displaced fracture of the greater tuberosity. Based on these findings, what is the best course of action?
Explanation
Question 2
A 13-year-old gymnast has had recurrent right elbow pain for the past year. She denies any history of trauma. Rest and anti-inflammatory drugs have failed to provide relief. Examination reveals no localized tenderness and only slight loss of both flexion and extension (10 degrees). What is the most likely diagnosis?
Explanation
Question 3
The incidence of ipsilateral phrenic nerve blockade after an interscalene block approaches
Explanation
Question 4
What is the most consistent finding regarding glenohumeral kinematics in patients with symptomatic tears of the rotator cuff?
Explanation
Question 5
A 28-year-old man sustained numerous injuries in an accident including a dislocation of the elbow and a severe closed head injury that resulted in unconsciousness. The elbow was reduced in the emergency department. After 1 month of rehabilitation, the patient reports pain and stiffness. A radiograph is shown in Figure 23. Management should now consist of
Explanation
Question 6
A 52-year-old man has had right shoulder pain in the deltoid region that increases at night for the past 2 months. He denies any history of trauma. Examination reveals mild tenderness over the greater tuberosity, and the Neer and Hawkins impingement signs are positive. AP and outlet lateral radiographs are shown in Figures 24a and 24b. Initial management should consist of
Explanation
Question 7
A 70-year-old woman is brought to the emergency department with a two-part greater tuberosity fracture with an anterior subcoracoid dislocation. One day after successful closed reduction, examination reveals marked swelling of the involved arm, forearm, and hand, as well as large amounts of "weeping" serous fluid but no obvious lacerations. The fingers are warm and pink, and the pulses are normal distally with good refill. Edema is present. There is no pain with passive and active motion of the elbow, wrist, and fingers. What is the next most appropriate step in management?
Explanation
Question 8
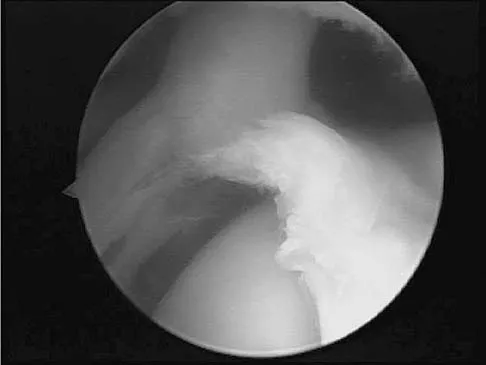
A baseball pitcher has intractable posterior and superior shoulder pain. The arthroscopic view seen in Figure 25 shows no Bankart or Hill-Sachs lesion and a negative drive-through sign. There are no signs of ligamentous laxity, but active compression and anterior slide tests are positive. Treatment should consist of
Explanation
Question 9
With increasing abduction in the scapular plane, maintaining neutral rotation, contact area, and contact pressure per unit area between the humeral head and glenoid follows what pattern if the total load across the joint is held constant?
Explanation
Question 10
A 21-year-old patient has had pain and a marked decrease in active and passive shoulder motion after having had a seizure 2 months ago as the result of alcohol abuse. Current AP and axillary radiographs and a CT scan are shown in Figures 26a through 26c. Management should consist of
Explanation
Question 11
Which of the following ligaments are the primary static restraints to inferior translation of the arm when the shoulder is in 0 degrees of abduction and neutral rotation?
Explanation
Question 12
A 44-year-old man who sustained an elbow dislocation 3 months ago now reports pain and restricted elbow motion. Radiographs are shown in Figures 27a and 27b. Management should consist of
Explanation
Question 13
A 67-year-old man who underwent humeral head arthroplasty for a four-part fracture 6 months ago reports that he is still unable to actively elevate his arm. Rehabilitation after surgery consisted of a sling with passive range-of-motion exercises for 2 weeks and then progressed to active-assisted and strengthening exercises at 3 weeks. Radiographs are shown in Figures 28a and 28b. What is the primary cause of his inability to elevate the arm?
Explanation
Question 14
Initial postoperative management after repair of an acute rotator cuff tear includes
Explanation
Question 15
A 34-year-old woman reports constant midlateral arm pain after sustaining minimal trauma to the shoulder. Radiographs and a biopsy specimen are shown in Figures 29a and 29b. What is the most likely diagnosis?
Explanation
Question 16
A 25-year-old professional baseball pitcher reports a 4-month history of gradually increasing medial elbow pain that occurs during the late cocking and acceleration phases of throwing. The pain occasionally refers distally along the ulnar aspect of the forearm. He denies any weakness; however, he notes occasional paresthesias. A nerve conduction velocity study demonstrates increased latency across the cubital tunnel. Management consisting of 6 weeks of rest and rehabilitation fails to provide relief as the symptoms returned when he resumed throwing. What is the best course of action?
Explanation
Question 17
What artery provides the only direct vascularizaton to both the intraneural and extraneural blood supply of the ulnar nerve just proximal to the cubital tunnel?
Explanation
Question 18
A 56-year-old man underwent right total shoulder arthroplasty 2 months ago. Recently while reaching with his shoulder in a flexed and adducted position, he noted shoulder pain and afterwards he could not externally rotate his arm. An axillary radiograph is shown in Figure 30. What is the most likely cause of this problem?
Explanation
Question 19
A 70-year-old man seen in the emergency department has had left shoulder pain and a fever of 101.5 degrees F (38.6 degrees C) for the past 3 days. He denies any history of trauma. Examination reveals tenderness anterosuperiorly and at the posterior glenohumeral joint line. He has very limited range of motion (passive and active). Laboratory studies show a WBC count of 12,000/mm3 and an erythrocyte sedimentation rate of 48 mm/h. Initial management should consist of
Explanation
Question 20
A 40-year-old man who is an avid weight lifter has had chronic pain in the proximal anterior shoulder for the past year. He denies any history of trauma. Examination reveals tenderness at the intertubercular groove, a positive speed test, and a positive Neer impingement sign. Nonsurgical management has failed to provide relief, and he is now considering surgery. Arthroscopic findings in the glenohumeral joint are shown in Figure 31. Based on these findings, treatment should consist of
Explanation
Question 21
A 59-year-old man reports moderate shoulder pain and very restricted range of motion after undergoing humeral arthroplasty for osteoarthritis 1 year ago. An AP radiograph is shown in Figure 32. Management should now consist of
Explanation
Question 22
A 70-year-old woman has a preoperative anterior interscalene block prior to undergoing a total shoulder arthroplasty. After seating her in the beach chair position, she becomes acutely hypotensive. What is the most likely cause for the hypotension?
Explanation
Question 23
What structure is considered the single most important soft-tissue restraint to anterior-posterior stability of the sternoclavicular joint?
Explanation
Question 24
A 35-year-old man has atraumatic painless limited elbow motion. Radiographs are shown in Figures 33a and 33b. What is the most likely diagnosis?
Explanation
Question 25
A 64-year-old man who underwent total shoulder arthroplasty 4 weeks ago is making satisfactory progress in physical therapy, but his therapist notes limitations in external rotation to neutral. A stretching program is started, and the patient suddenly gains 90 degrees of external rotation but now reports increased pain and weakness. What is the best course of action?
Explanation
Question 26
A 24-year-old man falls on an outstretched hand and sustains a proximal pole scaphoid fracture. Which of the following best describes the blood supply to the proximal pole of the scaphoid and its clinical implication?
Explanation
Question 27
A 35-year-old woman falls from a ladder and sustains a 'terrible triad' injury of the elbow. Which of the following describes the standard sequence of surgical reconstruction to restore elbow stability?
Explanation
Question 28
A 40-year-old man sustains a closed spiral fracture of the middle third of the humerus. On initial exam, neurological function is intact. Immediately following a closed reduction and splinting, he loses active wrist and finger extension and sensation in the first dorsal web space. What is the most appropriate next step in management?
Explanation
Question 29
A 78-year-old woman with severe osteoporosis presents with a 4-part proximal humerus fracture after a mechanical fall. The humeral head is entirely devoid of soft tissue attachments, and the tuberosities are comminuted. What is the preferred surgical treatment to maximize functional outcome and pain relief in this patient?
Explanation
Question 30
A 30-year-old man presents with a highly comminuted, un-reconstructable radial head fracture and severe ipsilateral wrist pain following a fall. Examination reveals distal radioulnar joint (DRUJ) instability. If the radial head is excised and not replaced, which of the following complications is most likely to occur?
Explanation
Question 31
A 25-year-old man sustains a traumatic injury to his right forearm. Radiographs demonstrate a fracture of the distal third of the radial shaft with associated dorsal displacement of the distal ulna. Which of the following is the most appropriate definitive management?
Explanation
Question 32
Which of the following is considered an absolute indication for operative fixation of an acute midshaft clavicle fracture?
Explanation
Question 33
A 32-year-old male presents with persistent wrist pain following a hyperextension injury 6 weeks ago. Radiographs show a widened scapholunate interval of 4 mm and a "cortical ring sign" of the scaphoid. What does the cortical ring sign indicate?
Explanation
Question 34
A 22-year-old gymnast falls on an outstretched arm and sustains a Type I (Hahn-Steinthal) capitellum fracture. Which of the following best describes this fracture pattern?
Explanation
Question 35
According to the Bado classification, which of the following characterizes a Type I Monteggia lesion?
Explanation
Question 36
A 28-year-old man presents to the emergency department after a motorcycle accident. His wrist is grossly deformed, and he reports numbness in his thumb, index, and middle fingers. Radiographs reveal a volar dislocation of the lunate with the capitate lying dorsally. Which nerve is most commonly injured in this scenario?
Explanation
Question 37
A 45-year-old male bodybuilder feels a sudden "pop" in his anterior elbow while performing heavy bicep curls. He presents with weakness in forearm supination and elbow flexion. During an anatomic repair of the distal biceps tendon using a single-incision anterior approach, which nerve is at greatest risk of iatrogenic injury?
Explanation
Question 38
A 35-year-old woman undergoes tension-band wiring for a transverse, non-comminuted olecranon fracture. What is the most common complication associated with this specific surgical technique?
Explanation
Question 39
A 35-year-old man falls on an outstretched hand and sustains the injury shown in
. The injury includes a posterior elbow dislocation, radial head fracture, and coronoid fracture. During operative management, what is the most appropriate sequence of repair?

Explanation
Question 40
A 28-year-old man presents with chronic wrist pain after an untreated injury 5 years ago. Radiographs shown in
demonstrate a scaphoid nonunion advanced collapse (SNAC). Which of the following articulations is typically preserved the longest in the natural history of a SNAC wrist?

Explanation
Question 41
When evaluating a displaced 4-part proximal humerus fracture for the risk of avascular necrosis, which of the following provides the primary arterial supply to the humeral head?
Explanation
Question 42
Which of the following is considered an absolute indication for operative fixation of an acute midshaft clavicle fracture?
Explanation
Question 43
A 55-year-old woman is treated in a cast for a minimally displaced distal radius fracture. Six weeks later, she notes a sudden inability to extend her thumb at the interphalangeal joint. What is the most likely etiology of this complication?
Explanation
Question 44
A 24-year-old professional baseball player complains of hypothenar wrist pain and paresthesias in his small finger after a forceful swing. A carpal tunnel view radiograph is shown in
. He is diagnosed with a hook of hamate fracture. What is the most definitive surgical treatment to allow earliest return to professional sports?

Explanation
Question 45
After closed reduction of a simple posterior elbow dislocation, the elbow is stable in pronation but subluxates when extended in supination. This finding indicates insufficiency of which of the following structures?
Explanation
Question 46
A 22-year-old motorcyclist is brought in after a high-speed collision. He has an entirely flail, pulseless upper extremity. Radiographs shown in
demonstrate significant lateral displacement of the scapula. What is the most critical immediate step in management?

Explanation
Question 47
A 30-year-old man falls onto his extended wrist. Lateral radiographs shown in
reveal a dorsal perilunate dislocation. Which of the following nerve injuries is most commonly associated with this specific trauma?
Explanation
Question 48
A 45-year-old woman presents with elbow pain after a fall. Imaging shown in
reveals a fracture of the capitellum involving the lateral trochlear ridge. Which surgical approach is most appropriate for direct visualization and fixation of this specific fracture pattern?

Explanation
Question 49
A 62-year-old woman undergoes volar locked plating for a distal radius fracture. Postoperatively, she develops flexor pollicis longus (FPL) tenosynovitis. What technical error is the most likely cause of this complication?
Explanation
Question 50
A 19-year-old college football player sustains an acute anterior shoulder dislocation. MRI confirms an anterior labral tear (Bankart lesion). If he is treated nonoperatively with a sling, what is his approximate risk of recurrent instability?
Explanation
Question 51
During surgical management of a 'terrible triad' injury of the elbow, after fixing the coronoid and replacing the radial head, the elbow remains unstable in extension. What is the next most appropriate step?
Explanation
Question 52
A 22-year-old man falls on an outstretched hand and presents with anatomic snuffbox tenderness. Radiographs are negative, but MRI confirms a nondisplaced fracture of the proximal pole of the scaphoid. The blood supply placing this region at high risk for avascular necrosis originates primarily from which vessel?
Explanation
Question 53
A 65-year-old woman is evaluated 6 months after volar locked plating of a distal radius fracture. She now presents with a new-onset inability to actively flex the interphalangeal joint of her thumb. What is the most likely etiology?
Explanation
Question 54
A 55-year-old woman presents with a severely displaced 4-part proximal humerus fracture after a fall. Examination reveals profound weakness in active arm abduction and numbness over the lateral aspect of the shoulder. Which nerve is most likely injured?
Explanation
Question 55
A 25-year-old cyclist sustains a completely displaced midshaft clavicle fracture with 2.5 cm of shortening. Compared to nonoperative management, what is the primary advantage of open reduction and internal fixation (ORIF) for this specific injury pattern?
Explanation
Question 56
A 7-year-old boy falls from the monkey bars. Radiographs demonstrate a fracture of the ulnar shaft with an anterior dislocation of the radial head (Bado Type I Monteggia variant). What is the preferred initial management?
Explanation
Question 57
A 30-year-old man is involved in a motorcycle crash. His wrist is grossly swollen, and he has numbness in the median nerve distribution. A lateral wrist radiograph demonstrates that the lunate maintains its normal articulation with the distal radius, but the capitate is displaced dorsally. What is the diagnosis?
Explanation
Question 58
A 40-year-old man sustains a severe traction injury to his right arm. Examination reveals massive swelling around the shoulder girdle and absent radial and ulnar pulses. Radiographs show extreme lateral displacement of the scapula. What is the most critical next step in management?
Explanation
Question 59
An 82-year-old community-dwelling woman with severe osteoporosis presents with a highly comminuted, intra-articular distal humerus fracture. She is a low-demand patient but requires her arms for basic transfers. What is the most appropriate surgical intervention?
Explanation
Question 60
A 35-year-old man presents to the ER after a grand mal seizure. His shoulder is locked in internal rotation. An AP radiograph shows a 'lightbulb sign.' What is the most common associated bony defect in this injury pattern?
Explanation
Question 61
A 28-year-old man suffers a severe fall on an outstretched hand, resulting in a comminuted radial head fracture, diffuse forearm pain, and distal radioulnar joint (DRUJ) tenderness. If the radial head is surgically excised without replacement, what is the most likely complication?
Explanation
Question 62
A 40-year-old woman falls onto her outstretched hand and presents with lateral elbow pain. A lateral elbow radiograph demonstrates a 'double arc' sign. What specific type of injury does this radiographic finding represent?
Explanation
Question 63
A 50-year-old man with a chronic, untreated scapholunate ligament tear presents with progressive wrist pain. Radiographs show joint space narrowing exclusively at the radioscaphoid articulation. As Scapholunate Advanced Collapse (SLAC) progresses to Stage III, which articulation is typically affected next?
Explanation
Question 64
A 5-year-old boy presents with a completely displaced extension-type III supracondylar humerus fracture. His hand is pale and pulseless. Following closed reduction and percutaneous pinning in the OR, the hand immediately becomes pink and well-perfused, but the radial pulse remains unpalpable. What is the most appropriate next step?
Explanation
Question 65
A 45-year-old weightlifter feels a sudden 'pop' in his anterior elbow during a heavy deadlift. Examination reveals a positive hook test. He undergoes a single-incision anterior approach for distal biceps tendon repair. What is the most common complication associated with this specific surgical approach?
Explanation
Question 66
A 32-year-old man sustains a Galeazzi fracture. After achieving anatomic open reduction and internal fixation of the radius, intraoperative assessment reveals the distal radioulnar joint (DRUJ) remains unstable in supination. What is the most appropriate next step in management?
Explanation
Question 67
During open reduction and internal fixation of a midshaft clavicle fracture, the surgeon inadvertently plunges the drill bit deep to the clavicle and the subclavius muscle. Which neurovascular structure is at greatest risk of direct injury in this immediate anatomic region?
Explanation
Question 68
A 35-year-old woman undergoes ORIF for a Mason Type II radial head fracture with a mechanical block. To avoid hardware impingement on the proximal radioulnar joint during forearm rotation, plates must be placed within the radial head 'safe zone.' Which clinical landmarks define this safe zone?
Explanation
Question 69
A 28-year-old manual laborer presents with chronic wrist pain 5 years after an untreated scaphoid fracture. Radiographs demonstrate a scaphoid nonunion with advanced radioscaphoid and capitolunate osteoarthritis, while the radiolunate joint is preserved. What is the most appropriate surgical treatment?
Explanation
Question 70
A 35-year-old man sustains a 'terrible triad' injury of the elbow. Intraoperatively, the coronoid fracture is fixed, the comminuted radial head is replaced, and the lateral ulnar collateral ligament (LUCL) is repaired. During range of motion testing, the elbow remains persistently unstable and subluxates in 30 degrees of extension. What is the next most appropriate step?
Explanation
Question 71
A 65-year-old woman sustains a 4-part proximal humerus fracture and undergoes shoulder hemiarthroplasty. Which of the following technical factors is most critical for restoring forward elevation and predicting a good long-term functional outcome?
Explanation
Question 72
A 28-year-old motorcycle rider presents with severe wrist pain after a crash. Radiographs reveal a volar dislocation of the lunate. The rest of the carpus remains aligned with the radius. What is the most commonly associated nerve injury with this specific pattern?
Explanation
Question 73
A 40-year-old woman falls on an outstretched hand and sustains a comminuted, unfixable Mason type III radial head fracture combined with distal radioulnar joint instability (Essex-Lopresti lesion).
What is the most appropriate management of the radial head?
Explanation
Question 74
A 32-year-old man undergoes superior plating for a completely displaced midshaft clavicle fracture. Postoperatively, he notes a localized area of numbness over the anterosuperior aspect of his chest wall, directly inferior to the surgical incision. Which nerve was most likely injured during the exposure?
Explanation
Question 75
An 82-year-old woman with advanced osteoporosis presents with a severely comminuted intra-articular distal humerus fracture (AO/OTA type 13-C3). She lives independently but uses a walker. Which surgical treatment provides the most reliable early return to function while minimizing the risk of reoperation for fixation failure?
Explanation
Question 76
A 55-year-old woman undergoes volar locked plating for a displaced distal radius fracture. Six months later, she presents with a sudden, painless inability to actively flex the interphalangeal joint of her thumb.
What is the most likely cause of this complication?
Explanation
Question 77
A 19-year-old football player presents with shortness of breath, dysphagia, and a choking sensation after a direct blow to the medial aspect of his shoulder. Plain radiographs of the shoulder and clavicle are inconclusive. What is the most appropriate next diagnostic step?
Explanation
Question 78
A 7-year-old boy falls from the monkey bars and sustains a Bado Type I Monteggia fracture equivalent. What is the classic anatomic deformity seen in a typical Bado Type I injury?
Explanation
Question 79
During open reduction and internal fixation of a Galeazzi fracture-dislocation in a 30-year-old man, the distal radius is anatomically plated. Intraoperative evaluation reveals that the distal radioulnar joint (DRUJ) remains grossly unstable in supination. What is the most appropriate next step in management?
Explanation
Question 80
A 45-year-old woman falls on her outstretched hand and sustains a coronal shear fracture of the distal humerus. The fracture fragment includes the capitellum and a significant medial extension that encompasses most of the trochlea. What is the correct classification for this fracture pattern?
Explanation
Question 81
A 34-year-old man presents with a high-energy multitrauma including a displaced scapular neck fracture. Which of the following radiographic parameters is an accepted indication for operative fixation of the scapula?
Explanation
Question 82
According to the O'Driscoll classification of coronoid fractures, an isolated fracture of the anteromedial facet of the coronoid is pathognomonic for which specific instability pattern of the elbow?

Explanation
Question 83
A 50-year-old man sustains a highly comminuted, high-energy distal radius fracture. Two hours later in the emergency department, he complains of severe, progressively worsening pain and numbness in his thumb, index, and middle fingers. Passive extension of his fingers causes excruciating pain out of proportion to the injury. What is the most urgent intervention?
Explanation
Question 84
A 45-year-old woman sustains a nondisplaced distal radius fracture treated in a short arm cast. Six weeks later, after cast removal, she suddenly loses the ability to actively extend the interphalangeal joint of her thumb. What is the most likely diagnosis?
Explanation
Question 85
A 35-year-old man falls from a height and sustains a 'terrible triad' injury to his elbow. When proceeding with operative management, what is the most accepted sequence of surgical repair to restore elbow stability?
Explanation
Question 86
Which of the following factors most significantly increases the risk of avascular necrosis and nonunion following a scaphoid fracture?
Explanation
Question 87
A 40-year-old woman presents with elbow pain after a fall on an outstretched hand. The lateral radiograph reveals a 'double arc' sign. Which of the following is the most likely diagnosis?
Explanation
Question 88
A 30-year-old manual laborer sustains a comminuted radial head fracture, wrist pain, and distal radioulnar joint (DRUJ) instability. If the radial head is excised and not replaced, what is the most likely long-term complication?
Explanation
Question 89
Which of the following scenarios is considered an absolute indication for operative internal fixation of a Galeazzi fracture?
Explanation
Question 90
According to Hertel's criteria, which of the following radiographic findings is the strongest predictor of humeral head ischemia in the setting of a proximal humerus fracture?
Explanation
Question 91
A 6-year-old child sustains an extension-type Monteggia fracture-dislocation. Which of the following neurological deficits is most commonly associated with this injury?
Explanation
Question 92
A 22-year-old cyclist sustains a midshaft clavicle fracture. Which of the following is a widely accepted relative indication for open reduction and internal fixation?
Explanation
Question 93
In the setting of an acute perilunate dislocation, what neurological complication is most frequently encountered on initial presentation?
Explanation
Question 94
A 5-year-old boy falls from monkey bars and sustains a significantly displaced extension-type supracondylar humerus fracture with posteromedial displacement. Which nerve is at the greatest risk of injury?
Explanation
Question 95
During surgical exposure for a comminuted intra-articular distal humerus fracture via an olecranon osteotomy, what is the ideal configuration of the osteotomy to maximize stability upon repair?
Explanation
Question 96
A 30-year-old man presents to the emergency department following a high-speed motor vehicle collision. Radiographs reveal an isolated, minimally displaced fracture of the scapular body. What is the most appropriate initial management?
Explanation
Question 97
A 19-year-old rugby player presents with severe medial chest pain, shortness of breath, and dysphagia after being tackled. Examination reveals a depression at the medial end of the clavicle. What is the most crucial next step in management?
Explanation
Question 98
Following a closed reduction of a simple posterolateral elbow dislocation in a 40-year-old male, the elbow is noted to be stable in pronation and flexion but subluxates in full extension. What is the best rehabilitation protocol?
Explanation
Question 99
A 28-year-old active manual laborer complains of ulnar-sided wrist pain 6 months after a nonoperatively treated distal radius fracture. Radiographs show a shortened, dorsally angulated distal radius with DRUJ incongruity. What is the most appropriate definitive surgical intervention?
Explanation
Question 100
A 28-year-old man falls onto his shoulder and is diagnosed with a Type V acromioclavicular (AC) joint injury. Which of the following best describes the anatomic disruption characteristic of this injury type?
Explanation
None
