AAOS Sports Medicine MCQs (Set 1): Knee, Shoulder & Ankle Injuries | Board Review

Key Takeaway
This high-yield question set (Set 1) for the AAOS/ABOS/OITE exams focuses on essential Sports Medicine topics. It covers diagnosis and management of knee ligamentous injuries, shoulder instability, and meniscal pathology. Ideal for board preparation and enhancing clinical knowledge in orthopedic sports medicine.
AAOS Sports Medicine MCQs (Set 1): Knee, Shoulder & Ankle Injuries | Board Review
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 22-year-old college baseball pitcher reports the recent onset of anterior and posterosuperior shoulder pain in his throwing shoulder. Examination shows a 15-degree loss of internal rotation, tenderness over the coracoid, and a positive relocation test. Radiographs are normal, and an MRI scan without contrast shows no definitive lesions. A rehabilitation program is prescribed. Which of the following regimens should be initially employed?
Explanation
Question 2
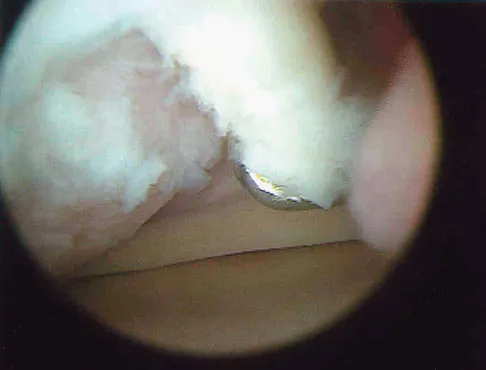
A 28-year-old professional football player reports painless loss of ankle motion after sustaining a "severe" ankle sprain 12 months ago. A mortise radiograph is shown in Figure 1. Surgical treatment should be reserved for which of the following conditions?
Explanation
Question 3
The most common mechanism of injury to the triangular fibrocartilage complex (TFCC) involves
Explanation
Question 4
The force generated by a muscle is most highly dependent on its
Explanation
Question 5
A 31-year-old woman has increasing pain and tightness in her right knee, with occasional stiffness and recurrent hemorrhagic effusions. MRI scans are shown in Figures 2a and 2b. What is the most likely diagnosis?
Explanation
Question 6
A 30-year-old elite marathon runner reports chronic pain over the lateral aspect of the distal right leg and dysesthesia over the dorsum of the foot with active plantar flexion and inversion of the foot. Examination reveals a tender soft-tissue fullness approximately 10 cm proximal to the lateral malleolus. The pain is exacerbated by passive plantar flexion and inversion of the ankle. There is also a positive Tinel's sign over the site of maximal tenderness. There is no motor weakness, and deep tendon reflexes are normal. Radiographs and MRI of the leg are normal. What is the next most appropriate step in management?
Explanation
Question 7
A 21-year-old soccer player reports pain and is unable to straighten his knee following an acute injury during a game. He is unable to continue to play. An MRI scan is shown in Figure 3. What is the next most appropriate step in management?
Explanation
Question 8
When performing an inside-out lateral meniscal repair, capsule exposure is provided by developing the
Explanation
Question 9
A 50-year-old man reports left shoulder pain and weakness after undergoing a lymph node biopsy in his neck 2 years ago. Examination reveals winging of the left scapula. Electromyography shows denervation of the trapezius. Surgical treatment for this condition involves
Explanation
Question 10
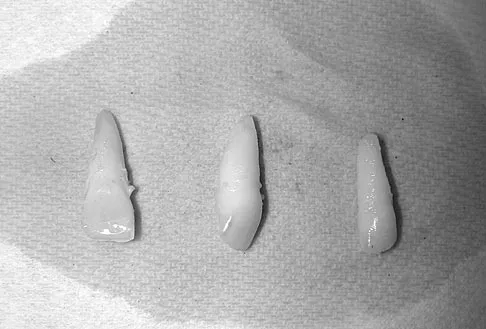
A 15-year-old female field hockey player sustains a blow to the mouth from a hockey stick. Three front teeth are knocked out and shown in Figure 4. In addition to calling a dentist immediately, what is the next best step in management?
Explanation
Question 11
Commotio cordis is best treated with
Explanation
Question 12
Which of the following is considered an advantage of arthroscopic distal clavicle excision compared with open distal clavicle excision?
Explanation
Question 13
A 40-year-old woman reports the atraumatic onset of severe knee pain and swelling after undergoing an uncomplicated elective cholecystectomy 1 week ago. She denies any history of diabetes mellitus or HIV but has had occasional episodes of mild knee pain and swelling that have always responded to nonsteroidal anti-inflammatory drugs. Radiographs are shown in Figures 5a and 5b. A knee aspiration yields a WBC count of 35,000/mm3. The aspirate should also yield which of the following findings?
Explanation
Question 14
What is the maximum acceptable amount of divergence of the interference screw in the femoral tunnel from the bone plug of a bone-patellar tendon-bone graft in anterior cruciate ligament (ACL) reconstruction before pull-out strength is statistically decreased?
Explanation
Question 15
A 21-year-old professional ballet dancer reports a painful popping sensation over her right hip joint. Examination reveals that symptoms are reproduced with hip flexion and external rotation. Which of the following studies will best confirm the diagnosis?
Explanation
Question 16
The posterior circumflex artery provides blood supply to what portion of the proximal humerus?
Explanation
Question 17
Use of prophylactic knee bracing in contact sports participants results in which of the following?
Explanation
Question 18
A 22-year-old college football player reports shortness of breath and dyspnea after a tackle. Examination reveals tachypnea, tachycardia, the trachea is shifted to the right, and there are decreased breath sounds on the left lung fields. The first line of treatment on the field should be
Explanation
Question 19
Anabolic steroid use has which of the following effects on serum lipoprotein levels?
Explanation
Question 20
A 20-year-old professional female jockey who is wearing a helmet is thrown from her horse. What is the most likely location of her injury?
Explanation
Question 21
A 62-year-old man with a long history of right shoulder pain and weakness is scheduled to undergo hemiarthroplasty. Based on the radiographs shown in Figures 6a through 6c, what preoperative factor will most affect postoperative functional outcome?
Explanation
Question 22
Which of the following complications is more likely with an inside-out repair technique compared to an all-inside techniques for a medial meniscus tear?
Explanation
Question 23
Figure 7 shows the CT scan of a 22-year-old professional baseball pitcher who has had elbow pain for the past 6 months despite rest from throwing. Management should consist of
Explanation
Question 24
A 17-year-old football player is injured during a play and reports abdominal pain that is soon followed by nausea and vomiting. What organ has most likely been injured?
Explanation
Question 25
A 15-year-old high school soccer player collides with an opponent and is unconscious when the trainer arrives on the field. He is conscious within 15 seconds, breathing appropriately, and denies any headache, neck pain, or nausea. It is his first head injury. Provided that the athlete is free of symptoms, when should he be allowed to return to athletic activity?
Explanation
Question 26
A 65-year-old man presents with chronic right shoulder pain and an inability to actively elevate his arm above 60 degrees. Passive elevation is preserved. MRI shows a massive, retracted tear of the supraspinatus and infraspinatus with Goutallier stage 4 fatty infiltration. What is the most appropriate definitive surgical management?
Explanation
Question 27
A 24-year-old male undergoes anterior cruciate ligament (ACL) reconstruction using a bone-patellar tendon-bone (BPTB) autograft. Compared to hamstring autograft, BPTB autograft has a higher incidence of which of the following postoperative complications?
Explanation
Question 28
A 28-year-old soccer player sustains an ankle injury resulting from forceful inversion and dorsiflexion. MRI reveals an osteochondral lesion of the talus. Based on the mechanism of injury, where is this lesion most likely located?
Explanation
Question 29
A 45-year-old manual laborer presents with persistent anterior shoulder pain. MRI arthrogram reveals a Type II SLAP tear. Nonoperative management has failed. What is the most appropriate surgical intervention to minimize the risk of postoperative stiffness and maximize functional return?
Explanation
Question 30
A 30-year-old male presents with a multi-ligamentous knee injury following a high-energy trauma. Physical examination reveals an abnormal dial test at both 30 and 90 degrees of knee flexion. Which of the following nerve injuries is most commonly associated with this specific structural injury pattern?
Explanation
Question 31
An 18-year-old football player sustains a syndesmotic "high" ankle sprain. Which of the following mechanisms of injury is most classically responsible for this pathology?
Explanation
Question 32
During diagnostic arthroscopy for chronic anterior shoulder instability, the surgeon identifies an impaction fracture of the anteroinferior glenoid rim with an associated disruption of the adjacent articular cartilage and labrum. What is the standard eponymous term for this lesion?
Explanation
Question 33
A 42-year-old female experiences a sudden "pop" in her posterior knee while squatting. MRI reveals a posterior root tear of the medial meniscus. If left untreated, this injury biomechanically behaves most similarly to which of the following?
Explanation
Question 34
A 35-year-old recreational athlete sustains an acute Achilles tendon rupture. He discusses nonoperative versus operative management with his orthopedic surgeon. What does current high-level evidence indicate regarding functional rehabilitation (nonoperative) versus surgical repair?
Explanation
Question 35
A 24-year-old overhead throwing athlete complains of deep shoulder pain during the late cocking phase of throwing. MRI arthrography reveals a Type II SLAP tear. Which of the following mechanisms is most responsible for this specific injury pattern in the overhead athlete?
Explanation
Question 36
When counseling a 19-year-old female collegiate soccer player regarding anterior cruciate ligament (ACL) reconstruction, she asks about the differences between bone-patellar tendon-bone (BPTB) and hamstring autografts. Compared to hamstring autografts, BPTB autografts are associated with a higher incidence of:
Explanation
Question 37
A 25-year-old rugby player sustains an inversion and plantarflexion injury to his ankle. Which osteochondral lesion of the talus is most characteristically associated with this specific mechanism?
Explanation
Question 38
A 21-year-old collegiate linebacker presents with recurrent anterior shoulder instability. CT scan indicates 25% anterior glenoid bone loss. What is the most appropriate definitive management?
Explanation
Question 39
A 26-year-old male undergoes ACL reconstruction and a concurrent peripheral longitudinal tear of the medial meniscus is repaired. The healing rate of this meniscal repair is enhanced compared to an isolated meniscal repair primarily due to:
Explanation
Question 40
A 35-year-old recreational athlete sustains an acute Achilles tendon rupture. In comparing surgical versus functional nonoperative management, surgical repair is historically associated with:
Explanation
Question 41
A 28-year-old tennis player exhibits a Glenohumeral Internal Rotation Deficit (GIRD) of 30 degrees compared to the contralateral side. Her total arc of motion is symmetric. Initial management should consist of:
Explanation
Question 42
During a posterolateral corner (PLC) reconstruction of the knee, the surgeon must be acutely aware of the anatomy to avoid iatrogenic injury. Which nerve is at the greatest risk during the surgical approach and lateral dissection for a PLC reconstruction?
Explanation
Question 43
A 20-year-old gymnast experiences patellar instability. The medial patellofemoral ligament (MPFL) is deemed incompetent. The femoral footprint of the MPFL (Schöttle's point) is anatomically located:
Explanation
Question 44
A 29-year-old male sustains an isolated posterior cruciate ligament (PCL) tear after a dashboard injury. If nonoperative management is chosen, physical therapy should primarily focus on strengthening which muscle group to restrict posterior tibial translation?
Explanation
Question 45
A 31-year-old volleyball player complains of isolated painless weakness in external rotation of his dominant shoulder. Examination reveals infraspinatus atrophy but normal supraspinatus strength. MRI is most likely to show a cyst in which location?
Explanation
Question 46
A 22-year-old football player sustains a multiligamentous knee injury. Physical examination demonstrates >10 degrees of increased external tibial rotation compared to the contralateral knee at both 30 degrees and 90 degrees of knee flexion. This finding indicates injury to the:
Explanation
Question 47
Which of the following physical examination tests is the most sensitive and specific for diagnosing an acute high ankle (syndesmotic) sprain?
Explanation
Question 48
A 19-year-old collegiate soccer player undergoes anterior cruciate ligament (ACL) reconstruction using a bone-patellar tendon-bone (BPTB) autograft. She successfully returns to sport at 9 months. Which of the following is the most commonly reported long-term complication associated with this specific graft choice compared to hamstring autografts?
Explanation
Question 49
A 16-year-old high school football player sustains a first-time traumatic anterior shoulder dislocation. Closed reduction is performed in the emergency department. If this patient is treated nonoperatively, which of the following is the most significant risk factor for recurrent instability?
Explanation
Question 50
A 23-year-old lacrosse player sustains an inversion and external rotation injury to his ankle. Examination reveals tenderness over the anterior inferior tibiofibular ligament (AITFL) and a positive squeeze test. Non-weight-bearing radiographs appear normal. What is the most appropriate next step to evaluate for syndesmotic instability?
Explanation
Question 51
A 52-year-old female presents with sudden onset medial knee pain after stepping down from a curb. She denies mechanical locking but reports an audible "pop." MRI demonstrates a radial tear at the attachment of the medial meniscus posterior horn with meniscal extrusion. If left untreated, this injury most predictably leads to:
Explanation
Question 52
A 45-year-old recreational tennis player has persistent anterior shoulder pain. MRI confirms a Type II SLAP (Superior Labrum Anterior to Posterior) tear. After failing 6 months of conservative management, surgical intervention is planned. Evidence suggests that which of the following produces the most reliable clinical outcomes and highest return to sport in this age group?
Explanation
Question 53
A 35-year-old male sustains an acute Achilles tendon rupture playing basketball. He is debating between operative and nonoperative management. Recent level I evidence indicates that when an early functional rehabilitation protocol is employed, nonoperative management is associated with:
Explanation
Question 54
A 28-year-old male is diagnosed with an isolated Grade II posterior cruciate ligament (PCL) tear following a dashboard injury. He is prescribed a physical therapy program. To optimize dynamic stabilization of the knee, the rehabilitation protocol should heavily emphasize strengthening of which muscle group?
Explanation
Question 55
A 15-year-old female requires medial patellofemoral ligament (MPFL) reconstruction for recurrent patellar instability. Anatomic femoral graft placement is critical to avoid anisometry. Radiographically, the anatomic femoral origin of the MPFL (Schöttle's point) is located:
Explanation
Question 56
A 30-year-old manual laborer sustains a Grade III acromioclavicular (AC) joint separation. If surgical reconstruction is eventually required, an understanding of the coracoclavicular ligaments is essential. Which of the following describes the anatomic orientation of these ligaments?
Explanation
Question 57
A 24-year-old female presents with chronic ankle pain. Imaging shows an osteochondral lesion of the talus.
Regarding the typical characteristics of talar dome osteochondral lesions, which statement is true?
Explanation
Question 58
A 26-year-old male sustains a high-energy knee dislocation (KD-III). Upon reduction in the trauma bay, his foot is warm and pink, but his ankle-brachial index (ABI) is calculated at 0.7. What is the most appropriate next step in management?
Explanation
Question 59
A 21-year-old collegiate baseball pitcher presents with vague posterior shoulder pain. Physical exam reveals a Glenohumeral Internal Rotation Deficit (GIRD) of 25 degrees compared to the contralateral side, with a total arc of motion deficit of 15 degrees. What is the most appropriate initial treatment?
Explanation
Question 60
During an ACL reconstruction, the surgeon evaluates the two functional bundles of the anterior cruciate ligament. Which of the following accurately describes the anatomy and biomechanics of the ACL bundles?
Explanation
Question 61
A 22-year-old gymnast presents with snapping over the lateral aspect of her ankle following a severe dorsiflexion-inversion injury. Exam reveals subluxation of the peroneal tendons over the lateral malleolus with resisted active dorsiflexion and eversion. This condition is primarily caused by an injury to which structure?
Explanation
Question 62
A 25-year-old cyclist falls directly onto his shoulder and sustains a completely displaced, midshaft clavicle fracture. Which of the following fracture characteristics is the most accepted absolute or relative indication for open reduction and internal fixation?
Explanation
Question 63
A 12-year-old boy presents with vague, activity-related anterior knee pain. Radiographs reveal a juvenile osteochondritis dissecans (JOCD) lesion. What is the most common anatomic location for this lesion?
Explanation
Question 64
A 32-year-old male bodybuilder feels a "pop" in his anterior chest wall while performing a heavy bench press. He presents with bruising and loss of the axillary fold. MRI confirms a pectoralis major tendon rupture. Which portion of the muscle-tendon unit is most commonly injured in this scenario?
Explanation
Question 65
A 19-year-old runner sustains an acute inversion ankle sprain. In the emergency department, anterior drawer testing is positive. Which ligament is the primary restraint to anterior translation of the talus in the ankle mortise when the foot is in plantarflexion?
Explanation
Question 66
A 40-year-old male undergoes knee arthroscopy for a 1.5 cm symptomatic focal chondral defect on the medial femoral condyle. A microfracture procedure is performed. The tissue that eventually fills this defect is histologically characterized by:
Explanation
Question 67
A 68-year-old male presents with chronic right shoulder pain and the inability to actively raise his arm above 60 degrees. Passive range of motion is full. Radiographs show a high-riding humeral head with acromiohumeral articulation (Hamada grade 3). What is the most appropriate surgical intervention?
Explanation
Question 68
A 19-year-old female soccer player sustains a non-contact knee injury. Which of the following is considered a primary anatomic risk factor for anterior cruciate ligament (ACL) rupture in female athletes?
Explanation
Question 69
A 24-year-old competitive rugby player presents with recurrent anterior shoulder instability. CT scan shows a 25% anterior glenoid bone loss. Which of the following is the most appropriate surgical treatment?
Explanation
Question 70
During a minimally invasive repair of an acute Achilles tendon rupture, the surgeon places percutaneous sutures in the proximal stump. Which of the following structures is at greatest risk of iatrogenic injury during this step?
Explanation
Question 71
A 50-year-old patient sustains a medial meniscus posterior root tear. Biomechanical studies have demonstrated that this injury alters knee contact pressures most similarly to which of the following conditions?
Explanation
Question 72
A 21-year-old collegiate baseball pitcher presents with vague posterior shoulder pain during the late cocking phase of throwing. Examination shows increased external rotation and a 25-degree loss of internal rotation compared to the contralateral side. What is the primary pathologic mechanism of this condition?
Explanation
Question 73
A 25-year-old hockey player sustains a rotational ankle injury. The external rotation stress test is positive.
Which ligament is typically the first to tear in a syndesmotic injury?
Explanation
Question 74
A 16-year-old female sustains an acute lateral patellar dislocation. She is scheduled for medial patellofemoral ligament (MPFL) reconstruction. The normal anatomic femoral origin of the MPFL is located:
Explanation
Question 75
A 45-year-old manual laborer has a massive, retracted, and irreparable posterosuperior rotator cuff tear. He has intact subscapularis function and severe external rotation weakness. Which of the following is the most appropriate surgical intervention to restore active external rotation?
Explanation
Question 76
A 32-year-old runner presents with deep ankle pain. MRI reveals an osteochondral lesion of the talus. Compared to anterolateral lesions, posteromedial talar dome lesions are characteristically:
Explanation
Question 77
A 28-year-old male is brought to the emergency department after a motorcycle accident with a grossly unstable knee (KD-III). His ankle-brachial index (ABI) is 0.8. What is the most appropriate next step in management?
Explanation
Question 78
During an anatomic reconstruction of the coracoclavicular (CC) ligaments for a chronic Type V acromioclavicular joint separation, the surgeon must recreate the conoid and trapezoid ligaments. Which of the following correctly describes the normal anatomy of these ligaments?
Explanation
Question 79
A 22-year-old basketball player complains of a snapping sensation at the posterolateral ankle when cutting. Examination reveals subluxation of the peroneal tendons over the lateral malleolus with resisted active dorsiflexion and eversion. What is the primary pathomechanical defect in this condition?
Explanation
Question 80
A 25-year-old professional soccer player has a symptomatic 3.5 cm² full-thickness chondral defect on the weight-bearing surface of the medial femoral condyle. Which of the following treatments provides the most durable long-term hyaline-like cartilage repair for a lesion of this size?
Explanation
Question 81
A 45-year-old recreational tennis player has a symptomatic Type II SLAP tear that has failed conservative management. Current literature suggests that compared to primary SLAP repair, primary biceps tenodesis in this age group will likely result in:
Explanation
Question 82
A 30-year-old male sustains a dashboard injury to his knee. Examination reveals a posterior sag sign and a posterior drawer test showing 8 mm of posterior tibial translation with a firm endpoint. There is no other ligamentous laxity.
What is the recommended initial management?

Explanation
Question 83
A 21-year-old collegiate pitcher undergoes evaluation for internal impingement. Which of the following capsuloligamentous structures is most likely contracted, contributing to glenohumeral internal rotation deficit (GIRD) in this athlete?
Explanation
Question 84
A 26-year-old soccer player undergoes an anterior cruciate ligament (ACL) reconstruction using a bone-patellar tendon-bone autograft. Six months postoperatively, she reports persistent stiffness and restricted knee flexion. What is the most common cause of technical failure leading to loss of flexion in ACL reconstruction?
Explanation
Question 85
A 22-year-old rugby player sustains an external rotation injury to his right ankle. Evaluation reveals a syndesmotic sprain. During the sequential failure of the distal tibiofibular syndesmosis from this mechanism, which structure is typically injured first?
Explanation
Question 86
A 25-year-old male presents with recurrent anterior shoulder instability. Imaging and diagnostic arthroscopy reveal an anteroinferior glenoid bone loss of 28%. Which of the following procedures is most appropriate to restore stability and minimize recurrence in this patient?
Explanation
Question 87
A 31-year-old man sustains an acute traumatic knee dislocation following a motorcycle collision. After closed reduction, his Ankle-Brachial Index (ABI) is 0.85. What is the most appropriate next step in management?
Explanation
Question 88
A 45-year-old recreational basketball player experiences a "pop" in his posterior ankle followed by weakness in plantar flexion. He is diagnosed with an acute Achilles tendon rupture. If he elects to undergo open surgical repair, which of the following is the most commonly reported significant complication compared to nonoperative management?
Explanation
Question 89
A 50-year-old male presents with acute onset of medial joint line pain in his knee after a deep squat. MRI reveals a medial meniscus posterior root tear with 4 mm of meniscal extrusion. Biomechanically, this injury is most similar to which of the following conditions?
Explanation
Question 90
A 24-year-old cyclist falls directly onto the point of his shoulder. Radiographs demonstrate a Type V acromioclavicular (AC) joint injury. Which of the following ligaments must be reconstructed to reliably restore superior-inferior stability of the clavicle?
Explanation
None
