Upper Extremity Orthopedic MCQs (Set 2): Shoulder, Elbow, Wrist & Hand | ABOS & AAOS Board Review
Key Takeaway
This high-yield question set (Set 2) for AAOS, ABOS, and OITE exams focuses on comprehensive upper extremity orthopedics. It features MCQs covering common pathologies of the shoulder, elbow, wrist, and hand, including fractures, dislocations, and nerve entrapments, essential for board preparation.
Upper Extremity Orthopedic MCQs (Set 2): Shoulder, Elbow, Wrist & Hand | ABOS & AAOS Board Review
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
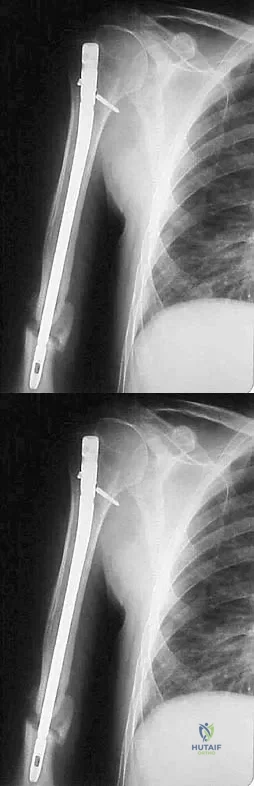
A 31-year-old man sustained a closed injury to his arm in a motor vehicle accident 16 months ago. Treatment of the fracture consisted of intramedullary nailing of the humerus. He now reports pain with minimal activities. Clinical examination and laboratory studies suggest no signs of infection. Radiographs are seen in Figures 12a through 12c. Treatment should now consist of
Explanation
Question 2
A well-developed college football player reports swelling and a heaviness in the arm after lifting weights. Examination reveals that distal pulses are normal and equal in both arms. A venogram is shown in Figure 13. What is the most likely cause of this condition?
Explanation
Question 3
Figure 14 shows the AP radiograph of a patient who underwent prosthetic arthroplasty 8 years ago and has now become symptomatic again over the past 18 months. A WBC count and erythrocyte sedimentation rate are within normal limits, and aspiration of the glenohumeral joint yields a negative Gram stain and cultures. Which of the following procedures will most likely provide the best pain relief and function?
Explanation
Question 4
A 52-year-old woman reports the sudden onset of intense pain in the right shoulder. She denies any history of injury or previous shoulder problems. At a 2-week follow-up examination, she notes that the pain has decreased, but she now has severe weakness of the external rotators and abductors. Her cervical spine and remaining shoulder examination are otherwise unremarkable. Radiographs of the shoulder and neck are normal. What is the most likely diagnosis?
Explanation
Question 5
What is the most commonly reported complication following elbow arthroscopy?
Explanation
Question 6
When an acute infection of a total elbow arthroplasty is managed with irrigation and debridement, which of the following organisms is associated with the highest risk of persistent infection?
Explanation
Question 7
A professional baseball player has had intermittent, mild shoulder pain for the past 2 years. Nonsurgical management has consisted of anti-inflammatory drugs. Examination reveals atrophy of the infraspinatus muscle but not the supraspinatus. There is weakness in external rotation with the arm at his side but not at 90 degrees of abduction. He has no weakness or pain with resisted abduction. Electromyography confirms an isolated lesion of the suprascapular nerve branch to the infraspinatus. He is otherwise neurologically intact. An MRI scan of the shoulder shows no cysts but confirms atrophy of the infraspinatus muscle. What is the next most appropriate step in management?
Explanation
Question 8
A 66-year-old woman who requires a cane for ambulation now notes increasing difficulty in using the cane after undergoing total elbow arthroplasty 3 months ago. AP and lateral radiographs are shown in Figures 15a and 15b. What is the most likely diagnosis?
Explanation
Question 9
The mother of a healthy 8-month-old boy reports that her son refuses to use his left arm. Examination reveals that the arm hangs limp at his side in an adducted and internally rotated position, and the affected shoulder subluxates posteriorly. Passive external rotation measures 15 degrees. Management should consist of
Explanation
Question 10
During shoulder motion with the elbow controlled in a brace, electromyographic studies of the supraspinatus show significant activity with all range-of-motion testing. Concurrent electromyographic studies of the long head of the biceps will most likely show
Explanation
Question 11
A right-handed 24-year-old professional baseball player injured his left shoulder 6 weeks ago when he dove forward and landed hard with the arm extended. He reports that the shoulder "slipped out" and "went back in." The shoulder did not need to be reduced. He now reports deep pain in the front of the shoulder when batting on either side and is hesitant to raise his left arm up over his head to catch a ball. Examination reveals no obvious deformities of the shoulder and a somewhat guarded, limited range of motion in all planes. Provocative tests for the rotator cuff and labrum are equivocal. MRI scans are shown in Figures 16a and 16b. What is the best course of action?
Explanation
Question 12
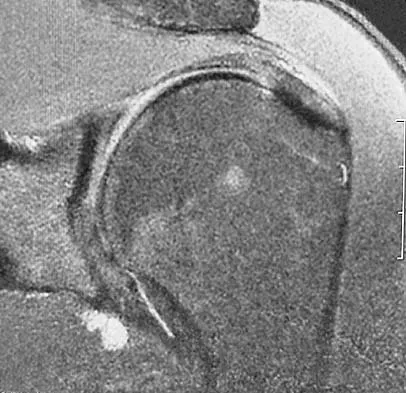
A 35-year-old woman dislocated her right shoulder in a fall from a step stool several months ago. She now reports several painful recurrences. Examination reveals anterior and inferior apprehension that reproduces her symptoms. An MRI scan is shown in Figure 17. Management should consist of
Explanation
Question 13
A 20-year-old man sustained an injury to his arm during a tug-of-war contest. An MRI scan is shown in Figure 18. What is the most likely diagnosis?
Explanation
Question 14
When the elbow is extended and an axial load is applied, what percent of stress distribution occurs across the ulnohumeral and radiohumeral articular surface, respectively?
Explanation
Question 15
Which of the following is most frequently associated with heterotopic ossification about the shoulder?
Explanation
Question 16
A 55-year-old woman with a 15-year history of systemic lupus erythematosus has had left shoulder pain for the past 3 months. She reports that the pain has grown progressively worse over the past few months, and her shoulder function is severely limited. She is presently being treated with azathioprine and has used corticosteroids in the past. AP and axillary radiographs are shown in Figures 19a and 19b, and MRI scans are shown in Figures 19c and 19d. Which of the following forms of management will yield the most predictable pain relief and return of shoulder function?
Explanation
Question 17
A 45-year-old man sustains an acute closed posterolateral elbow dislocation. The elbow is reduced, and examination reveals that the elbow dislocates posteriorly at 35 degrees with the forearm placed in supination. What is the best course of action?
Explanation
Question 18
Figure 20 shows the MRI scan of a 20-year-old athlete who has a painful shoulder. This pathology is most commonly seen in
Explanation
Question 19
Figure 21 shows the radiograph of an 18-year-old man who was brought to the emergency department with shoulder pain following a rollover accident on an all-terrain vehicle. Examination reveals a fracture with massive swelling; however, the skin is intact and not tented over the fracture. Based on these findings, initial management should consist of
Explanation
Question 20
A 55-year-old man reports increasing weakness in his arms that has progressed to his lower limbs, resulting in frequent tripping and falling. Examination reveals weakness in shoulder abduction and external and internal rotation bilaterally. Fasciculation is noted. He also has weakness in elbow flexion and extension bilaterally, and his grip strength is diminished. An electromyogram and nerve conduction velocity studies show decreased amplitude of compound motor action potential, slightly slowed motor conduction velocity, and denervation signs with decreased recruitment in all extremities. The sensory study is normal. Based on these findings, what is the most likely diagnosis?
Explanation
Question 21
Which of the following positions of immobilization has been shown to best approximate the anterior labrum against the glenoid rim following anterior dislocation of the shoulder?
Explanation
Question 22
What is the most common complication following arthroscopic capsular release in a patient with adhesive capsulitis of the shoulder?
Explanation
Question 23
What is the most common complication following surgical fixation of a distal humeral fracture?
Explanation
Question 24
A 16-year-old female swimmer reports several episodes of atraumatic glenohumeral instability that occur with different arm positions. Examination reveals generalized ligamentous laxity and a positive sulcus sign, and her shoulder can be subluxated both anteriorly and posteriorly. Initial management should consist of
Explanation
Question 25
A 13-year-old boy has a mild deformity of the left sternoclavicular joint after being involved in a rollover accident while riding an all-terrain vehicle. Examination in the emergency department reveals that he is hemodynamically stable, and his neurovascular examination is normal. The CT scan shown in Figure 22 was obtained because radiographs were inconclusive. Management should consist of
Explanation
Question 26
A 45-year-old mechanic presents with chronic radial-sided wrist pain. Imaging shows a scaphoid waist nonunion with radioscaphoid and capitolunate arthritis. The radiolunate joint is entirely spared. What is the most appropriate surgical treatment?
Explanation
Question 27
A 35-year-old weightlifter undergoes a single-incision anterior repair of a distal biceps tendon rupture using suture anchors. Postoperatively, he exhibits weakness in thumb and finger extension, but normal wrist flexion. Wrist extension is weak and deviates radially. Which nerve was most likely injured during the procedure?
Explanation
Question 28
A 22-year-old rugby player has recurrent anterior shoulder instability. CT scan demonstrates 25% glenoid bone loss and a large, engaging Hill-Sachs lesion. What is the most appropriate definitive management?
Explanation
Question 29
A 28-year-old carpenter sustains a laceration to the volar index finger at the proximal phalanx, completely dividing the FDP and FDS tendons. He undergoes primary 6-strand core repair. Which rehabilitation protocol provides the best combination of tendon glide and prevention of rupture?
Explanation
Question 30
Six weeks after closed reduction and casting of a nondisplaced distal radius fracture, a 65-year-old woman presents with the sudden inability to actively extend her thumb interphalangeal joint. What is the most appropriate surgical management?
Explanation
Question 31
A 42-year-old woman undergoing hemodialysis for end-stage renal disease presents with severe, bilateral carpal tunnel syndrome that has failed conservative management. During open carpal tunnel release, thick, brownish tenosynovial tissue is noted. What is the most likely composition of this tissue?
Explanation
Question 32
A 45-year-old man falls on an outstretched hand and sustains a "terrible triad" injury of the elbow. Which of the following is the standard recommended sequence of surgical reconstruction?
Explanation
Question 33
A 72-year-old woman with rotator cuff tear arthropathy and pseudoparalysis undergoes a reverse total shoulder arthroplasty (RTSA). Which of the following muscles provides the primary motive force for active elevation postoperatively?
Explanation
Question 34
The spiral cord in Dupuytren's disease causes central and superficial displacement of the digital neurovascular bundle, placing it at high risk during fasciectomy. Which of the following normal anatomical structures is NOT a component of the spiral cord?
Explanation
Question 35
A 30-year-old manual laborer presents with dorsal wrist pain. Radiographs show sclerosis and fragmentation of the lunate, with a negative ulnar variance of 3 mm. There is no radiocarpal arthritis. What is the most appropriate initial surgical intervention?
Explanation
Question 36
A 6-year-old boy sustains a Bado Type I Monteggia fracture-dislocation. Closed reduction of the ulna fracture is achieved and stabilized with an intramedullary wire, but the radial head remains anteriorly dislocated. What is the most appropriate next step in management?
Explanation
Question 37
A 45-year-old construction worker falls from a ladder and sustains an elbow dislocation. Radiographs reveal a posterior elbow dislocation associated with a radial head fracture and a coronoid fracture. During surgical reconstruction of this 'terrible triad' injury, what is the standard sequence of repair?
Explanation
Question 38
A 24-year-old man presents with a 9-month history of wrist pain after a fall. MRI shows a scaphoid nonunion with avascular necrosis (AVN) of the proximal pole. What is the most appropriate surgical management?
Explanation
Question 39
A 72-year-old female presents with chronic right shoulder pain and pseudoparalysis, unable to actively elevate her arm past 40 degrees. Radiographs show severe glenohumeral arthritis with superior migration of the humeral head articulating with the acromion. Which procedure provides the most predictable improvement in function?
Explanation
Question 40
A 45-year-old manual laborer presents with persistent shoulder pain. MRI confirms a Type II SLAP tear. After failing conservative management, surgical intervention is planned. To minimize the risk of post-operative stiffness and reoperation in this demographic, what is the preferred procedure?
Explanation
Question 41
A 30-year-old man sustains a closed midshaft humerus fracture. Initial examination shows intact radial nerve function. A closed reduction is performed, and a coaptation splint is applied. Immediately after reduction, the patient is unable to extend his wrist or fingers. What is the most appropriate next step?
Explanation
Question 42
A 35-year-old carpenter has central dorsal wrist pain. Radiographs reveal sclerosis and a coronal fracture of the lunate, without carpal collapse (Lichtman Stage IIIa). Ulnar variance is neutral. What is the most appropriate joint-leveling procedure to unload the lunate?
Explanation
Question 43
A 42-year-old male undergoes a two-incision surgical repair of a distal biceps tendon rupture. Compared to a single-incision anterior approach, the two-incision technique carries a historically higher risk of which of the following complications?
Explanation
Question 44
A 25-year-old cyclist sustains a displaced fracture of the distal third of the clavicle. Radiographs show superior displacement of the medial fragment, while the coracoclavicular (CC) ligaments remain attached to the distal fragment. What is the recommended management?
Explanation
Question 45
Following a primary repair of a Zone II flexor digitorum profundus (FDP) laceration in the index finger, which post-operative rehabilitation protocol most reliably decreases adhesion formation while protecting the repair?
Explanation
Question 46
A 65-year-old patient presents with a highly comminuted olecranon fracture that exits distal to the coronoid process (trans-olecranon fracture-dislocation pattern). What is the most appropriate method of internal fixation?
Explanation
Question 47
A 28-year-old male sustained a wrist hyperextension injury 3 weeks ago. Radiographs demonstrate a scapholunate interval of 4mm and a 'signet ring' sign of the scaphoid. What is the most appropriate surgical intervention?
Explanation
Question 48
An 80-year-old female with severe osteoporosis presents with a closed 4-part proximal humerus fracture. The humeral head is completely split into two segments and is displaced from the glenoid. What is the most appropriate surgical treatment?

Explanation
Question 49
A 50-year-old male with severe cubital tunnel syndrome presents with intrinsic muscle atrophy and clawing of the small and ring fingers. He previously underwent a simple in-situ ulnar nerve release 2 years ago, with initial relief followed by recurrence. What is the most appropriate next surgical step?
Explanation
Question 50
A 22-year-old competitive rugby player presents with recurrent anterior shoulder instability. A 3D CT scan reveals 28% bone loss of the anterior/inferior glenoid. Which surgical procedure is most appropriate?
Explanation
Question 51
A 40-year-old manual laborer presents with Stage II SLAC (Scapholunate Advanced Collapse) wrist. Radiographs show osteoarthritis at the radioscaphoid joint, but the radiolunate and midcarpal joints are spared. If he desires a motion-preserving salvage procedure, which of the following is acceptable?
Explanation
Question 52
A 45-year-old manual laborer presents with a massive, irreparable posterosuperior rotator cuff tear. Examination reveals an intact subscapularis and deltoid, but he has significant weakness in active external rotation and forward elevation. Which of the following tendon transfers is the most appropriate surgical treatment to restore function?
Explanation
Question 53
A 35-year-old male falls on an outstretched hand and sustains a 'terrible triad' injury to the elbow. Operative management is planned. Following a standard deep-to-superficial surgical approach, what is the accepted sequence of structural repair to restore elbow stability?
Explanation
Question 54
A 55-year-old man presents with chronic wrist pain and weakness. Radiographs demonstrate scapholunate advanced collapse (SLAC) stage III, defined by capitatolunate arthritis with a preserved radiolunate joint. Which of the following is the most appropriate surgical management?
Explanation
Question 55
A 25-year-old rugby player presents with an inability to actively flex the distal interphalangeal (DIP) joint of his ring finger after grabbing an opponent's jersey. Radiographs reveal a large bony avulsion fragment volar to the DIP joint. According to the Leddy-Packer classification, what type of flexor digitorum profundus (FDP) avulsion is this?
Explanation
Question 56
A 22-year-old competitive rugby player with a history of recurrent anterior shoulder dislocations undergoes advanced imaging. A 3D CT scan reveals a 28% anterior glenoid bone defect. What is the most appropriate definitive surgical intervention?
Explanation
Question 57
A 42-year-old bodybuilder feels a 'pop' in his anterior elbow while doing heavy biceps curls. MRI confirms a complete distal biceps tendon rupture. If a single anterior incision technique is chosen for the repair, which nerve is at the highest risk of iatrogenic injury?
Explanation
Question 58
A 65-year-old woman with advanced rheumatoid arthritis presents with a massive, irreparable rotator cuff tear, severe glenohumeral osteoarthritis, and pseudoparalysis of the shoulder. Physical exam confirms an intact and functioning deltoid muscle.
Which of the following is the most appropriate definitive management?

Explanation
Question 59
A 28-year-old gymnast presents with chronic ulnar-sided wrist pain. Examination reveals a positive foveal sign. MRI arthrogram demonstrates a peripheral tear of the triangular fibrocartilage complex (TFCC) with an avulsion from the fovea of the ulna. This corresponds to which Palmer classification, and what is the preferred treatment?
Explanation
Question 60
During the surgical management of a distal radius fracture with a volar locking plate, the surgeon ensures the plate is placed proximal to the watershed line. This anatomic guideline is primarily utilized to prevent which of the following complications?
Explanation
Question 61
A 30-year-old male sustains a Bennett fracture. Radiographs show a fracture at the base of the thumb metacarpal where the volar ulnar intra-articular fragment retains its anatomic position. The metacarpal shaft is displaced proximally, dorsally, and radially. Which muscle is the primary deforming force responsible for this characteristic shaft displacement?
Explanation
Question 62
A patient with a severe ulnar nerve transection at the level of the elbow initially presents with weakness of intrinsic hand muscles but minimal clawing of the ring and small fingers. Three months following nerve repair at the elbow, pronounced clawing of these digits develops. This phenomenon is known as:
Explanation
Question 63
A 35-year-old male sustains a closed diaphyseal fracture of the humerus. On initial evaluation, he is unable to actively extend his wrist or fingers. He undergoes closed reduction and functional bracing. At 12 weeks, there is no clinical or electromyographic (EMG) evidence of radial nerve recovery. What is the most appropriate next step in management?
Explanation
Question 64
A 40-year-old patient with Kienböck's disease is evaluated radiographically. Images reveal lunate sclerosis and fragmentation, fixed scaphoid rotation, and established osteoarthritis in the capitolunate joint. According to the Lichtman classification, this is Stage IV Kienböck's. Which of the following procedures is contraindicated in this setting?
Explanation
Question 65
A 19-year-old collegiate baseball pitcher presents with medial elbow pain during the late cocking phase of throwing. MRI arthrogram confirms a high-grade ulnar collateral ligament (UCL) tear. During UCL reconstruction (e.g., using the docking technique), the graft is primarily designed to replicate which specific structure?
Explanation
Question 66
A 50-year-old diabetic female presents with a locking thumb that is refractory to corticosteroid injections. During surgical release of the A1 pulley, the surgeon must be particularly careful to protect a nerve that courses obliquely over the flexor sheath near the metacarpophalangeal flexion crease. Which nerve is this?
Explanation
Question 67
A 28-year-old cyclist sustains a mid-shaft clavicle fracture after going over the handlebars.
According to established orthopedic guidelines, which of the following is considered an ABSOLUTE indication for acute operative fixation of a clavicle fracture?
Explanation
Question 68
A 68-year-old osteoporotic woman sustains a displaced 3-part proximal humerus fracture. Open reduction and internal fixation with a locking plate is planned. To maximize biomechanical stability and prevent postoperative varus collapse of the humeral head, which of the following must be achieved intraoperatively?
Explanation
Question 69
A 24-year-old male sustains a posterior elbow dislocation. After closed reduction, the elbow is stable in 90 degrees of flexion but immediately subluxates when extended with the forearm in supination. This specific pattern of instability indicates insufficiency of which of the following structures?
Explanation
Question 70
A 32-year-old carpenter suffers a clean guillotine amputation of his index finger at the level of the proximal phalanx. Replantation is attempted. To maximize venous outflow and ensure the best survival rate of the replanted digit, what is the optimal ratio of veins to arteries that should be anastomosed?
Explanation
Question 71
A 26-year-old chef sustains a deep laceration to the volar aspect of his index finger over the middle phalanx, cleanly transecting both the FDS and FDP tendons (Zone II). Primary repair is planned. According to biomechanical studies, the strength of the flexor tendon repair is most directly proportional to which of the following factors?
Explanation
Question 72
A 72-year-old woman presents with chronic right shoulder pain and an inability to raise her arm above the horizontal plane. Physical examination reveals active forward elevation to 40 degrees and passive elevation to 150 degrees. Radiographs demonstrate superior migration of the humeral head with articulation against the acromion
. Which of the following is the most appropriate surgical treatment?
Explanation
Question 73
A 35-year-old man presents with chronic wrist pain and stiffness 2 years after a fall. Imaging reveals a scaphoid nonunion with radioscaphoid arthritis and preservation of the midcarpal joint. The proximal pole of the capitate demonstrates no arthritic changes. Which of the following procedures is most appropriate?
Explanation
Question 74
A 42-year-old woman falls on an outstretched hand and sustains a "terrible triad" injury of the elbow. Which of the following structures is the primary restraint to posterolateral rotatory instability (PLRI) and must be meticulously repaired or reconstructed during surgery?
Explanation
Question 75
A 28-year-old carpenter presents with acute finger pain, swelling, and a flexed posture of the index finger 48 hours after a penetrating injury. Which of the following is NOT one of Kanavel's cardinal signs of acute suppurative flexor tenosynovitis?
Explanation
Question 76
A 21-year-old collegiate wrestler has experienced multiple anterior shoulder dislocations. A recent CT scan indicates 30% anterior glenoid bone loss. What is the most appropriate surgical intervention to prevent recurrent instability?
Explanation
Question 77
A 29-year-old construction worker complains of progressive dorsal wrist pain. Radiographs reveal sclerosis and fragmentation of the lunate without carpal collapse. Measurements demonstrate 3 mm of negative ulnar variance. What is the most appropriate surgical treatment?
Explanation
Question 78
A 45-year-old man complains of elbow pain and a "clunking" sensation when pushing himself out of a chair. On examination, a positive pivot-shift test of the elbow is elicited. Which mechanism of injury is most commonly associated with this specific condition?
Explanation
Question 79
A 32-year-old woman undergoes primary repair of a lacerated flexor digitorum profundus (FDP) tendon in Zone II. To optimize healing and minimize adhesions, which of the following postoperative rehabilitation protocols is most strongly supported by current evidence?
Explanation
Question 80
A 38-year-old bicyclist falls directly onto his shoulder. Clinical examination and standing X-rays demonstrate a Type V acromioclavicular (AC) joint separation, with the distal clavicle elevated 150% above the acromion. Which ligaments are completely disrupted in this injury pattern?
Explanation
Question 81
A 62-year-old woman presents with debilitating pain at the base of her right thumb. Examination shows a positive grind test. Radiographs demonstrate severe joint space narrowing and osteophytes at the trapeziometacarpal joint, but the scaphotrapezial joint is spared. Following failed conservative management, what is the gold standard surgical treatment?
Explanation
Question 82
A 44-year-old weightlifter sustained an acute complete distal biceps tendon rupture and underwent surgical repair using a two-incision technique. Postoperatively, he has profound restriction of forearm pronation and supination but full elbow flexion and extension. What is the most likely complication responsible for his restricted motion?
Explanation
Question 83
A 26-year-old male falls from a height and presents with a markedly swollen and painful wrist. The lateral radiograph demonstrates the "spilled teacup" sign with the lunate displaced volarly. During physical examination, which nerve distribution should be most meticulously evaluated?
Explanation
Question 84
A 55-year-old woman presents with a 6-month history of progressive, severe, global loss of both active and passive shoulder range of motion. She denies any preceding trauma. Which of the following systemic conditions is most strongly associated with the development and refractoriness of her most likely diagnosis?
Explanation
Question 85
A 72-year-old female presents with severe right shoulder pain and an inability to actively elevate her arm above 40 degrees. Radiographs demonstrate superior migration of the humeral head with an acromiohumeral distance of 3 mm. Examination reveals intact deltoid function but positive lag signs. What is the most appropriate surgical treatment?
Explanation
Question 86
A 42-year-old male presents with a "terrible triad" injury of the elbow following a fall onto an outstretched hand. When performing the surgical reconstruction, what is the most widely accepted sequence of repair?
Explanation
Question 87
A 45-year-old male presents with chronic wrist pain and a history of a scaphoid fracture 15 years ago. Radiographs demonstrate advanced radioscaphoid arthritis and scaphocapitate arthritis, but the radiolunate joint is completely spared (SNAC Stage III). What is the most appropriate definitive surgical intervention?
Explanation
Question 88
A 28-year-old carpenter lacerates the volar surface of his index finger over the middle phalanx (Zone II). A primary flexor tendon repair is planned. To safely implement an early active motion protocol postoperatively, what is the minimum recommended number of core strands across the repair site?
Explanation
Question 89
A 21-year-old collegiate rugby player with a history of multiple recurrent anterior shoulder dislocations undergoes evaluation. A CT scan with 3D reconstruction reveals a 28% anterior glenoid bone loss. What is the most appropriate surgical intervention?
Explanation
Question 90
A 35-year-old bodybuilder feels a sudden pop in his anterior elbow during a heavy bicep curl. The hook test is positive. The surgeon utilizes a single-incision anterior approach to repair the distal biceps tendon. Which of the following nerves is at highest risk of iatrogenic injury with this specific approach?
Explanation
Question 91
A 26-year-old male falls from a ladder onto an outstretched hand. An AP radiograph of the wrist reveals a "piece of pie" sign, while the lateral radiograph demonstrates a "spilled teacup" sign. Which nerve is most commonly acutely injured in this specific clinical setting?
Explanation
Question 92
During a regional fasciectomy for severe Dupuytren's disease, the surgeon carefully dissects a spiral cord to avoid neurovascular injury. How does the spiral cord typically displace the digital neurovascular bundle?
Explanation
Question 93
A 30-year-old right-hand-dominant construction worker sustains a Type III acromioclavicular (AC) joint separation following a direct blow to the shoulder. What is the most widely accepted initial management for this patient?
Explanation
Question 94
A 45-year-old female sustains a coronal shear fracture of the capitellum that extends medially to include the majority of the trochlea (McKee modification Type IV). Open reduction and internal fixation with headless compression screws is planned. What is the most common complication following surgical management of this injury?
Explanation
Question 95
A 24-year-old gymnast complains of ulnar-sided wrist pain and clicking. Examination reveals severe distal radioulnar joint (DRUJ) instability in both supination and pronation. MRI confirms a foveal avulsion of the triangular fibrocartilage complex (TFCC). What is the primary biomechanical function of the foveal attachment of the TFCC?
Explanation
None
