Hip Dislocations: Understanding Causes, Risks, & Outcomes
Key Takeaway
This article provides essential research regarding Hip Dislocations: Understanding Causes, Risks, & Outcomes. **Hip dislocations hip** are severe injuries where the femoral head separates from the acetabulum. These high-energy traumas, often from motor vehicle accidents, primarily affect 16-40-year-old males. Posterior dislocations are most prevalent, with common complications including sciatic nerve injury, femoral head osteonecrosis, and posttraumatic arthritis.
Introduction and Epidemiology
Traumatic hip dislocations represent true orthopedic emergencies that demand rapid assessment, precise imaging, and immediate reduction to mitigate devastating long-term sequelae such as femoral head osteonecrosis and posttraumatic arthritis. The hip is an inherently stable ball-and-socket joint; therefore, dislocation requires substantial high-energy trauma. Consequently, up to 50 percent of patients sustain concomitant fractures elsewhere at the time of hip dislocation, necessitating a comprehensive Advanced Trauma Life Support evaluation.
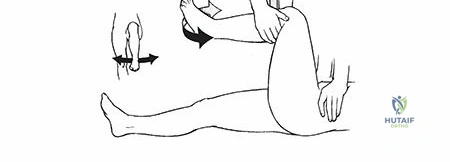
The majority of hip dislocations occur in 16- to 40-year-old males involved in motor vehicle collisions. Almost all posterior hip dislocations result from motor vehicle accidents, classically described as a "dashboard injury" where an axial load is applied to a flexed, adducted knee. Unrestrained motor vehicle accident occupants are at a significantly higher risk for sustaining a hip dislocation than passengers wearing a restraining device.
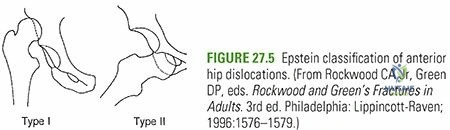
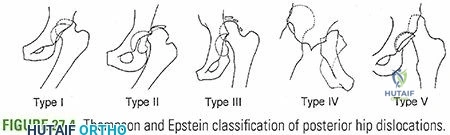
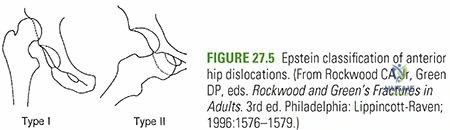
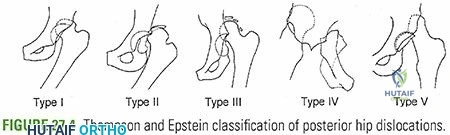
Directionally, traumatic dislocations are classified primarily into posterior and anterior variants. Anterior dislocations constitute 10 to 15 percent of traumatic dislocations of the hip, typically resulting from forced abduction and external rotation. Posterior dislocations account for the remaining 85 to 90 percent.
The clinical outcomes following hip dislocations are heavily influenced by the severity of the initial trauma and the time to reduction. The incidence of femoral head osteonecrosis ranges between 2 percent and 17 percent of patients, with the risk increasing significantly if reduction is delayed beyond six hours. Furthermore, 16 percent of patients develop posttraumatic arthritis, often secondary to unrecognized chondral damage, impaction fractures, or retained intra-articular loose bodies. Sciatic nerve injury is present in 10 to 20 percent of posterior dislocations, typically presenting as a peroneal nerve division palsy due to the anatomical vulnerability of the laterally positioned peroneal fibers within the sciatic sheath.
Pathomechanics of Dislocation
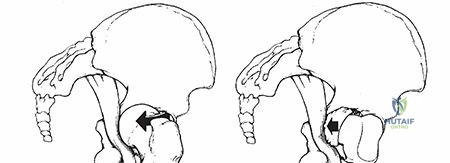
The position of the hip at the moment of impact dictates the direction of the dislocation and the associated bony injuries. In posterior dislocations, if the hip is flexed and adducted, a simple dislocation without an acetabular fracture is common. If the hip is in neutral adduction or slight abduction, the femoral head is driven into the posterior wall of the acetabulum, frequently resulting in a fracture-dislocation. Anterior dislocations are subdivided into superior (pubic) and inferior (obturator) types, depending on the degree of hip flexion at the time of the abduction/external rotation force.
Surgical Anatomy and Biomechanics
A profound understanding of the osseous, ligamentous, and vascular anatomy of the hip is imperative for executing safe reduction maneuvers, determining surgical approaches, and anticipating complications.
Osteology and Articular Geometry
The hip articulation has a highly congruent ball-and-socket configuration with stability conferred by both bony and ligamentous restraints. The acetabulum is formed from the confluence of the ischium, ilium, and pubis, which meet at the triradiate cartilage during skeletal immaturity. The hemispherical femoral head articulates with the lunate surface of the acetabulum.
Approximately 40 percent of the femoral head is covered by the bony acetabulum at any position of hip motion. The effect of the fibrocartilaginous labrum is to deepen the acetabulum, increasing the surface area of the joint by 22 percent and its volume by 33 percent. This creates a suction seal that enhances joint stability through negative intra-articular pressure and distributes compressive loads across the articular cartilage.
Capsuloligamentous Restraints
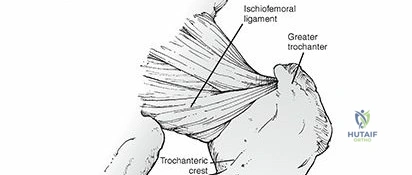
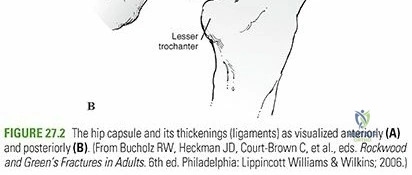
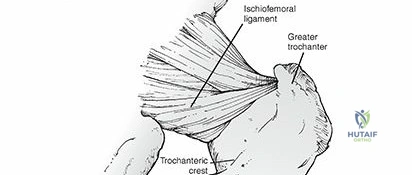
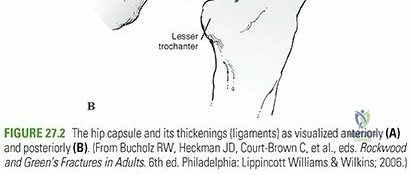
The hip joint capsule is formed by thick longitudinal fibers supplemented by much stronger ligamentous condensations that run in a spiral fashion. These include the iliofemoral, pubofemoral, and ischiofemoral ligaments.
The iliofemoral ligament, or the Y-ligament of Bigelow, is the strongest ligament in the human body. It originates from the anterior inferior iliac spine and inserts along the intertrochanteric line, preventing excessive hip extension and external rotation. The pubofemoral ligament limits extension and abduction, while the ischiofemoral ligament, located posteriorly, tightens during internal rotation. Because these ligaments spiral around the femoral neck, they become taut in extension, driving the femoral head firmly into the acetabulum, and relax in flexion, which is the position of greatest vulnerability for posterior dislocation.
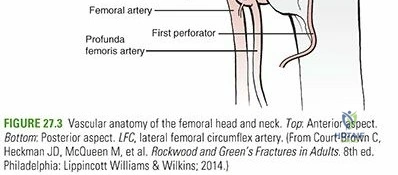
Vascular Anatomy
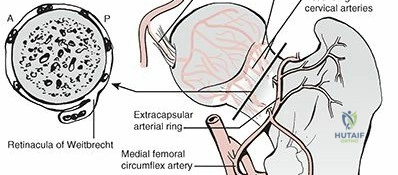
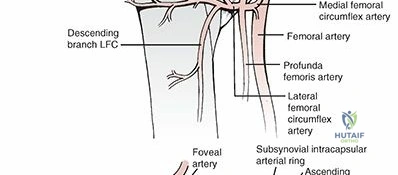
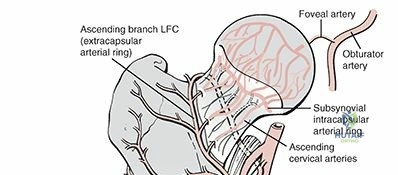
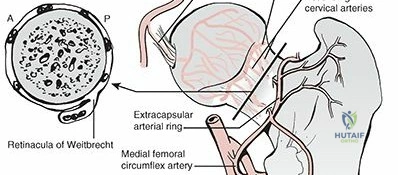
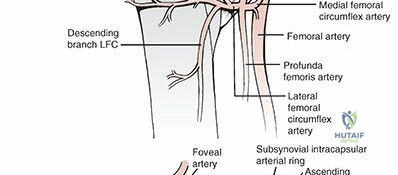
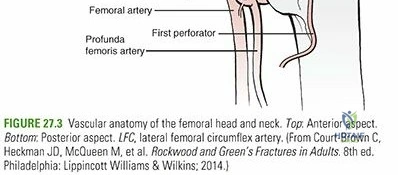
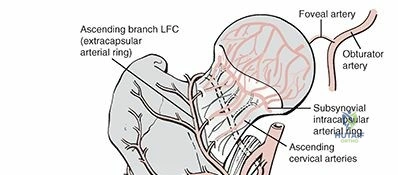
The vascular supply to the proximal femur is the most critical anatomical consideration in hip trauma, as disruption leads to avascular necrosis. The main vascular supply to the femoral head originates from the medial and lateral femoral circumflex arteries, which are typically branches of the profunda femoris artery.
An extracapsular vascular ring is formed at the base of the femoral neck. From this ring, ascending cervical branches (retinacular vessels) pierce the hip joint capsule at the level of its distal insertion. These branches ascend along the femoral neck beneath the synovial reflection and enter the bone just inferior to the articular cartilage of the femoral head. The lateral epiphyseal artery, a terminal branch of the medial femoral circumflex artery, provides the majority of the blood supply to the weight-bearing dome of the femoral head.
The artery of the ligamentum teres, a branch of the obturator artery, contributes a variable but generally minor blood supply to the epiphyseal region of the femoral head. In adults, this vessel is often insufficient to maintain femoral head viability if the retinacular vessels are disrupted during a traumatic dislocation.
Neurologic Proximity
The sciatic nerve exits the pelvis through the greater sciatic foramen, typically emerging inferior to the piriformis muscle. It descends posterior to the short external rotators (superior gemellus, obturator internus, inferior gemellus, and quadratus femoris). In posterior hip dislocations, the displaced femoral head or associated posterior wall acetabular fracture fragments can stretch, compress, or lacerate the sciatic nerve.
Indications and Contraindications
The management of traumatic hip dislocations is dictated by the reducibility of the joint, the concentricity of the reduction, and the presence of associated fractures. Closed reduction under procedural sedation or general anesthesia is indicated as the first-line treatment for almost all acute, simple hip dislocations and should be performed emergently.
Open reduction is indicated when closed reduction fails, when there is an associated displaced femoral neck fracture, or when post-reduction imaging reveals a non-concentric joint due to incarcerated intra-articular fragments (such as osteochondral loose bodies, labrum, or capsule).
Operative Versus Non Operative Management
| Management Strategy | Indications | Contraindications |
|---|---|---|
| Emergent Closed Reduction | Acute simple posterior or anterior dislocation; hemodynamically stable patient; absence of ipsilateral femoral neck fracture. | Ipsilateral displaced femoral neck fracture; delayed presentation (> 24 hours) where open reduction is preferred to clear joint. |
| Open Reduction (Posterior Approach) | Irreducible posterior dislocation; non-concentric reduction; incarcerated intra-articular fragment; associated posterior wall acetabular fracture requiring fixation; sciatic nerve palsy developing after closed reduction. | Anterior dislocation requiring direct anterior visualization (relative contraindication). |
| Open Reduction (Anterior Approach) | Irreducible anterior dislocation; incarcerated anterior structures (e.g., buttonholing through capsule); associated anterior femoral head fracture (Pipkin). | Posterior dislocation with posterior wall fracture. |
| Surgical Dislocation (Ganz) | Complex Pipkin fractures; extensive labral or chondral pathology requiring 360-degree visualization of the femoral head. | Severe hemodynamic instability; critically ill polytrauma patient requiring damage control. |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning begins with a systematic trauma evaluation. Life-threatening injuries must be addressed prior to focusing on the extremity, though reducing a dislocated hip is considered a crucial part of the secondary survey to prevent irreversible ischemia to the femoral head.
Imaging Modalities
Initial imaging includes an anteroposterior radiograph of the pelvis. In a posterior dislocation, the femoral head appears smaller than the contralateral side and is displaced superiorly and laterally to the acetabulum. In an anterior dislocation, the femoral head appears larger and is displaced inferiorly and medially.
Following any reduction attempt, a post-reduction AP pelvis radiograph is mandatory to confirm concentric reduction. Subsequently, a fine-cut computed tomography scan of the pelvis with sagittal and coronal reconstructions must be obtained. The CT scan is the gold standard for identifying incarcerated osteochondral fragments, subtle marginal impaction, and associated acetabular or femoral head fractures that were obscured on plain radiographs.
Anesthesia and Positioning
For closed reduction, deep procedural sedation with muscle relaxation in the emergency department is often sufficient. If the patient is already being transported to the operating room for other life-saving interventions, reduction under general anesthesia with complete neuromuscular blockade is preferred to minimize iatrogenic chondral damage during the maneuver.
Positioning for closed reduction typically involves the patient lying supine on a firm stretcher or operating table. For open reduction via a posterior approach (Kocher-Langenbeck), the patient is placed in the lateral decubitus position or prone, depending on surgeon preference and associated pelvic ring injuries. The lateral decubitus position allows for excellent visualization of the posterior column and posterior wall. For an anterior approach (Smith-Petersen or Watson-Jones), the patient is positioned supine on a radiolucent flat table, often with a bump under the ipsilateral hip.
Detailed Surgical Approach and Technique
The technical execution of hip reduction, whether closed or open, requires strict adherence to biomechanical principles to avoid iatrogenic fracture of the femoral neck or further vascular compromise.
Closed Reduction Maneuvers
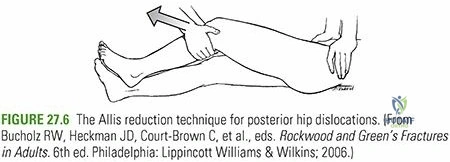
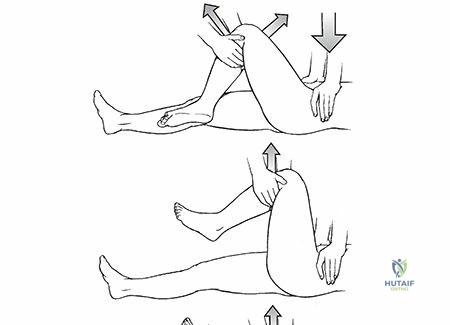
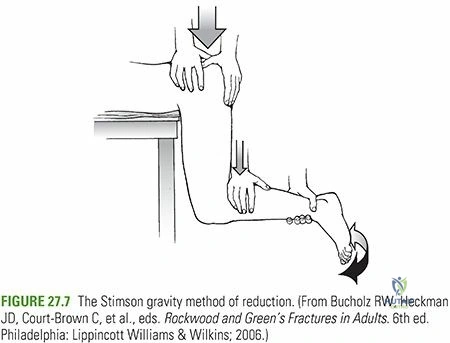
Several techniques exist for the closed reduction of posterior hip dislocations. The core principle involves in-line traction, flexion to 90 degrees, and gentle internal-to-external rotation to navigate the femoral head over the posterior acetabular rim.
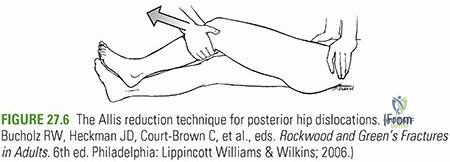
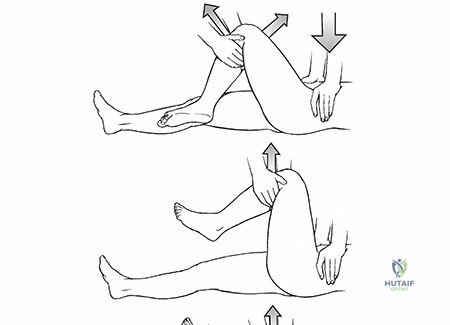
- Allis Maneuver: The patient is supine. The surgeon stands over the patient, flexing the hip and knee to 90 degrees. An assistant provides counter-traction by applying downward pressure on the anterior superior iliac spines. The surgeon applies steady upward axial traction in line with the femur, coupled with gentle internal and external rotation.
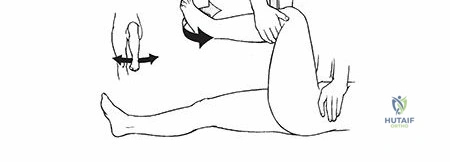
- Captain Morgan Technique: The patient is supine. The surgeon places their flexed knee under the patient's flexed knee. By plantarflexing their own ankle, the surgeon uses their calf as a fulcrum to apply a strong, controlled upward force behind the patient's proximal tibia, combined with manual traction.
- East Baltimore Lift: Requires two providers. The patient is supine. The providers stand on opposite sides of the bed, placing their arms under the patient's flexed calf and resting their hands on each other's shoulders. They simultaneously stand up, applying upward traction, while a third provider stabilizes the pelvis.
For anterior dislocations, the reduction maneuver involves in-line traction with the hip in slight flexion and abduction, followed by gentle internal rotation and adduction to lever the head back into the acetabulum.
Open Reduction via Posterior Approach
When closed reduction fails, the Kocher-Langenbeck approach is the workhorse for posterior dislocations.
- Incision and Superficial Dissection: A curvilinear incision is made centered over the greater trochanter. The fascia lata is incised in line with the skin, and the gluteus maximus is split bluntly along the direction of its fibers.
- Nerve Identification: The sciatic nerve is systematically identified, usually exiting beneath the piriformis. It must be protected throughout the procedure, often by maintaining the hip in slight extension and knee in flexion to reduce tension.
- Deep Dissection: The short external rotators (piriformis, superior gemellus, obturator internus, and inferior gemellus) are tagged and tenotomized near their insertion on the greater trochanter. They are reflected posteriorly over the sciatic nerve to act as a protective cushion. The quadratus femoris is typically left intact to preserve the ascending branch of the medial femoral circumflex artery, which runs in close proximity to its superior border.
- Capsulotomy and Reduction: A T-shaped or I-shaped capsulotomy is performed. The joint is inspected, and any incarcerated labrum, capsule, or osteochondral fragments are meticulously excised or repaired. The femoral head is then reduced under direct vision using manual traction and a bone hook on the greater trochanter if necessary.
- Closure: The capsule is repaired if possible, and the short external rotators are reattached to their trochanteric insertion via transosseous drill holes to restore dynamic stability.
Open Reduction via Anterior Approach
For irreducible anterior dislocations, a Smith-Petersen approach is utilized.
- Internervous Plane: The approach exploits the internervous plane between the femoral nerve (sartorius and rectus femoris) and the superior gluteal nerve (tensor fasciae latae and gluteus medius).
- Superficial Dissection: An incision is made from the anterior half of the iliac crest to the anterior superior iliac spine, extending distally. The interval between the sartorius and tensor fasciae latae is developed.
- Deep Dissection: The lateral femoral cutaneous nerve is identified and protected. The interval between the rectus femoris and gluteus medius is developed. The ascending branch of the lateral femoral circumflex artery is identified and ligated.
- Capsulotomy: The reflected head of the rectus femoris is elevated off the capsule. An anterior capsulotomy is performed, exposing the dislocated femoral head. The obstructing structures (often the capsule or iliopsoas tendon) are cleared, and the hip is reduced.
Complications and Management
The complication profile following a hip dislocation is substantial, necessitating rigorous follow-up and patient counseling.
Avascular Necrosis and Neurologic Injury
| Complication | Incidence | Pathophysiology and Management Strategy |
|---|---|---|
| Avascular Necrosis (Osteonecrosis) | 2% to 17% | Caused by disruption of the medial femoral circumflex artery or prolonged intra-articular hypertension. Risk increases exponentially if reduction is delayed > 6 hours. Monitored via serial radiographs and MRI. Management ranges from core decompression in early stages to total hip arthroplasty for structural collapse. |
| Posttraumatic Arthritis | 16% to 20% | Secondary to initial chondral impact, retained loose bodies, or altered joint biomechanics from associated fractures. Managed conservatively with NSAIDs and injections initially; ultimately may require total hip arthroplasty. |
| Sciatic Nerve Palsy | 10% to 20% | Most common in posterior dislocations. Typically involves the peroneal division. If a deficit is present pre-reduction, closed reduction is performed, and the nerve is observed. If a deficit develops post-reduction, immediate surgical exploration is indicated to rule out nerve entrapment within the joint. |
| Heterotopic Ossification | Up to 40% (post-op) | Formation of bone in periarticular soft tissues, more common following open reduction. Prophylaxis with Indomethacin or single-fraction localized radiation therapy is utilized in high-risk patients. |
| Recurrent Dislocation | < 2% | Rare in pure dislocations without substantial posterior wall deficiency. If recurrent, evaluation for massive capsular incompetence, labral avulsion, or unrecognized bony defects is required. |
Post Operative Rehabilitation Protocols
Rehabilitation following a hip dislocation must balance the need for early mobilization to prevent deep vein thrombosis and stiffness with the necessity of protecting the healing capsuloligamentous structures.
Phase Based Recovery
In the immediate post-reduction phase, patients are typically placed on restricted weight-bearing protocols. For simple dislocations without associated fractures, touch-down weight-bearing or partial weight-bearing with crutches or a walker is maintained for four to six weeks.
Range of motion restrictions are dictated by the direction of the initial dislocation. For a posterior dislocation, patients are instructed to adhere to posterior hip precautions: avoiding hip flexion past 90 degrees, adduction across the midline, and extreme internal rotation for a minimum of six weeks. Conversely, following an anterior dislocation, anterior precautions are instituted, restricting extreme extension and external rotation.
Routine radiographic surveillance is conducted at two weeks, six weeks, three months, six months, and annually thereafter. Magnetic resonance imaging may be considered at the three-to-six-month mark if the patient develops persistent groin pain, to evaluate for early osteonecrosis before radiographic collapse occurs.
Summary of Key Literature and Guidelines
The foundational literature in orthopedic traumatology emphasizes the critical nature of time in the management of hip dislocations. Classical studies have demonstrated that reduction within six hours significantly decreases the rate of avascular necrosis. The Advanced Trauma Life Support guidelines reinforce that while life-saving measures take precedence, the reduction of a dislocated hip is an urgent priority in the secondary survey.
Furthermore, contemporary literature highlights the indispensable role of post-reduction computed tomography. Plain radiographs have been shown to miss up to 30 percent of intra-articular loose bodies and subtle marginal impaction fractures. Therefore, an algorithmic approach incorporating emergent closed reduction, mandatory post-reduction CT imaging, and selective open reduction for non-concentric joints or associated fractures remains the gold standard in academic orthopedic practice. Utilizing these evidence-based protocols ensures the optimization of joint preservation and the minimization of long-term morbidity in this challenging patient population.
Clinical & Radiographic Imaging