Bernese Periacetabular Osteotomy: A Masterclass in Hip Preservation

Key Takeaway
This masterclass details the Bernese Periacetabular Osteotomy (PAO) for hip dysplasia. Fellows will learn comprehensive anatomy, meticulous preoperative planning, and granular intraoperative execution from a surgeon's perspective. We cover neurovascular risks, precise osteotomy techniques, and essential pearls for successful acetabular reorientation, aiming to prevent arthrosis and restore hip function.
Comprehensive Introduction and Patho-Epidemiology
Welcome, esteemed colleagues and fellows, to the operating theater and to this definitive exploration of hip preservation. Today, we are undertaking a comprehensive analysis of the Bernese Periacetabular Osteotomy (PAO), an exceptionally sophisticated, joint-preserving procedure primarily indicated for the treatment of symptomatic acetabular dysplasia. Introduced by Reinhold Ganz and his colleagues at the University of Bern in 1988, this procedure fundamentally revolutionized the approach to the young, active patient suffering from structural hip instability. This is not merely a technical surgical exercise; it is an intricate biomechanical art form dedicated to restoring the physiological kinematics of the hip joint, thereby preventing or significantly delaying the onset of debilitating coxarthrosis.
We must fundamentally understand that hip dysplasia, particularly developmental dysplasia of the hip (DDH), represents the most common anatomical etiology of secondary coxarthrosis, frequently leading to total hip arthroplasty (THA) far too early in a patient's life cycle. Extensive longitudinal studies, such as the landmark epidemiological work by Murphy et al., have demonstrated a stark, undeniable correlation: patients presenting with a lateral center-edge angle (LCEA) of less than 16 degrees almost invariably develop symptomatic osteoarthritis by the age of 65. Our ultimate objective with the Bernese PAO is to surgically liberate and realign the congruous, albeit spatially maloriented, dysplastic acetabulum. By doing so, we normalize joint contact pressures, providing profound and often indefinite symptom relief for appropriately selected patients, even those exhibiting early-stage, radiographically evident arthrosis.


The Bernese PAO distinguishes itself distinctly from legacy pelvic osteotomies—such as the Salter innominate osteotomy, the Pemberton osteotomy, and the classical triple osteotomy—by meticulously preserving the structural integrity of the posterior column of the pelvis. This is a critical, defining anatomical distinction. By leaving the posterior column intact, we inherently minimize pelvic ring instability, negate the need for postoperative spica casting, and allow for a far more robust, multiplanar reorientation of the acetabular fragment. We achieve this remarkable feat through a highly precise, reproducible sequence of five interconnected osteotomies, each specifically designed to liberate the acetabulum while maintaining its vital posterior connection to the sacroiliac joint and preserving its delicate endosteal and periosteal blood supply.
Furthermore, the patho-epidemiology of dysplasia extends beyond simple lateral uncoverage. The dysplastic acetabulum is frequently shallow, anteverted, and deficient anteriorly, leading to a pathological mechanical environment characterized by chronic edge-loading, labral hypertrophy, and eventual chondral delamination. The PAO directly addresses this by allowing the surgeon to medialize the hip center of rotation—thereby reducing the joint reaction force lever arm—while simultaneously providing superior and anterior coverage. This profound alteration in the mechanical environment halts the vicious cycle of chondral degradation, shifting the paradigm from inevitable joint replacement to lifelong joint preservation.
Detailed Surgical Anatomy and Biomechanics
Osteology and Topographical Landmarks
Before we even consider making an incision, a profound, three-dimensional understanding of the critical bony and neurovascular structures of the hemipelvis is an absolute prerequisite. The acetabulum, our primary surgical target, is a hemispherical cavity nestled precisely at the confluence of the ilium, ischium, and pubis, supported by the robust anterior and posterior columns of the pelvis. In the setting of DDH, the most common area of bony deficiency is typically located anteriorly and laterally, leading to inadequate structural coverage of the femoral head and subsequent anterolateral instability.
Important bony landmarks dictate the precise trajectory of our osteotomies. The iliopectineal eminence marks the medialmost extent of the acetabulum and serves as a crucial reference point for our superior pubic ramus osteotomy, ensuring we do not inadvertently enter the joint medially. The infracotyloid groove, located just distal to the inferior lip of the acetabulum, is the precise anatomical site for our anterior ischial osteotomy. The anterosuperior iliac spine (ASIS) and anteroinferior iliac spine (AIIS) are prominent landmarks that guide our superficial and deep dissections, often requiring partial osteotomy or meticulous soft-tissue reflection to facilitate access to the true pelvis.
The apex of the greater sciatic notch and the ischial spine are critical posterior landmarks. The sciatic notch guides the superior iliac cut, while the ischial spine indicates the medial extent of the posterior column. The posterior column itself is triangular in cross-section, being thickest immediately posterior to the acetabulum and tapering as it approaches the sciatic notch. Consequently, the optimal plane for the posterior column osteotomy is angled obliquely to the medial cortex and perpendicular to the lateral cortex of the ischium, allowing for a safe, controlled cut that avoids the articular surface.


Neurovascular Considerations and Biomechanical Principles
Navigating the neurovascular landscape during a PAO demands unwavering vigilance. The lateral femoral cutaneous nerve (LFCN) courses highly variably over or through the iliac crest and sartorius origin; it is acutely vulnerable during the superficial dissection and ASIS osteotomy, and its protection is paramount to avoid debilitating meralgia paresthetica. Deep within the pelvis, the obturator nerve and artery are at risk during the superior pubic ramus osteotomy. The use of precisely placed blunt retractors within the obturator foramen is essential to shield these structures from the oscillating saw or osteotome.
Perhaps the most critical vascular structure is the medial femoral circumflex artery (MFCA), the primary blood supply to the femoral head. The MFCA is located in perilous proximity to the obturator externus tendon. By strictly staying proximal to this tendon during the ischial osteotomy, we protect the MFCA and prevent catastrophic avascular necrosis of the femoral head. Posteriorly, the sciatic nerve lies intimately close to the posterior aspect of the ischium. Deep, uncontrolled penetration during the ischial or posterior column osteotomies poses a significant risk of iatrogenic sciatic nerve palsy.
Biomechanically, the dysplastic hip is a system in failure. The lack of lateral and anterior coverage drastically reduces the contact area between the femoral head and the acetabular dome. According to the formula Pressure = Force / Area, a decreased contact area leads to exponentially elevated joint contact stresses. This chronic edge-loading overwhelms the hoop stresses of the acetabular labrum, leading to labral tearing, chondral delamination, and the formation of subchondral cysts. The PAO biomechanically neutralizes this by lateralizing and anteriorizing the acetabular roof, massively increasing the surface area for load transmission, medializing the center of rotation to decrease the abductor lever arm requirement, and ultimately normalizing intra-articular contact pressures.
Exhaustive Indications and Contraindications
Patient Selection Criteria
The success of the Bernese PAO is inextricably linked to rigorous, uncompromising patient selection. The ideal candidate is a symptomatic adolescent or young adult (typically between 14 and 40 years of age) with radiographically confirmed acetabular dysplasia and closed triradiate cartilage. The primary physiological constraint is not strictly chronological age, but rather the degree of preoperative arthrosis, the quality of the articular cartilage, and the presence of medical comorbidities that might favor total hip arthroplasty.
A comprehensive clinical history must evaluate the onset, duration, and specific character of the hip pain. Pain localized to the groin that is exacerbated by activity, prolonged sitting, or pivoting is classic for intra-articular pathology secondary to dysplasia. Mechanical symptoms such as catching, clicking, or a sensation of "giving way" strongly suggest concomitant labral tears or chondral flaps. We must also rigorously screen for previous hip disorders (such as Legg-Calvé-Perthes disease or slipped capital femoral epiphysis), neuromuscular conditions (like cerebral palsy or Charcot-Marie-Tooth disease), and systemic skeletal dysplasias, as these fundamentally alter the surgical approach and expected outcomes.

The physical examination must be exhaustive. Gait analysis often reveals a compensated Trendelenburg gait, indicative of chronic abductor fatigue or mechanical disadvantage due to a lateralized center of rotation. Range of motion assessment frequently demonstrates increased hip flexion and internal rotation due to anterior acetabular uncoverage. Specific provocative tests, such as the Anterior Apprehension Test and the Anterior Impingement Test (FADIR), are critical for identifying symptomatic anterior instability and secondary femoroacetabular impingement (FAI), respectively.

Indication and Contraindication Matrix
To systematize the decision-making process, we adhere strictly to established clinical and radiographic parameters. The following table delineates the absolute and relative indications and contraindications for the Bernese PAO.
| Category | Parameters & Conditions | Rationale / Clinical Context |
|---|---|---|
| Absolute Indications | Symptomatic DDH (LCEA < 20°), Closed triradiate cartilage, Tonnis Grade 0 or 1 OA. | Ideal mechanical environment for preservation; cartilage is viable enough to sustain long-term joint survival post-realignment. |
| Relative Indications | Mild to moderate retroversion, Tonnis Grade 2 OA in a young patient (< 30 yrs), Perthes-like deformities. | Requires careful patient counseling regarding the potential for earlier conversion to THA; PAO serves as a "buying time" procedure. |
| Absolute Contraindications | Tonnis Grade 3 OA (bone-on-bone), Open triradiate cartilage, Inflammatory arthropathies (e.g., Rheumatoid Arthritis). | Cartilage is irreparably damaged; realignment will not relieve pain. Open cartilage risks growth arrest and catastrophic pelvic deformity. |
| Relative Contraindications | Age > 45 years, Obesity (BMI > 35), Significant osteopenia, "Hinge abduction" on dynamic radiographs. | Higher complication rates, technically demanding mobilization, and poor potential for cartilage remodeling. Hinge abduction indicates incongruency that PAO may exacerbate. |
Pre-Operative Planning, Templating, and Patient Positioning
Advanced Imaging and Radiographic Templating
The blueprint for a successful PAO is drawn long before the patient enters the operating suite. Our preoperative imaging protocol is exhaustive. Standard radiography must include a weight-bearing anteroposterior (AP) view of the pelvis to assess the Lateral Center-Edge Angle of Wiberg (normal > 25°), the Tönnis Acetabular Roof Angle (normal 0-10°), and the presence of a crossover sign indicative of cranial retroversion. A False Profile view of the affected hip is mandatory to evaluate the Anterior Center-Edge Angle of Lequesne and de Seze (normal > 20°), quantifying the degree of anterior uncoverage.



Furthermore, we routinely obtain AP views in maximal abduction and internal rotation (the von Rosen view). This dynamic assessment is paramount; it evaluates joint congruency and helps us visualize the potential spherical appearance of the hip after acetabular reorientation. Importantly, it helps identify "hinge abduction," a phenomenon where the laterally subluxated femoral head hinges on the lateral acetabular rim rather than reducing into the true acetabulum. The presence of true hinge abduction is a strong relative contraindication to a standard PAO, often necessitating a concurrent proximal femoral valgus-producing osteotomy or steering the surgeon toward salvage procedures.
Modern preoperative planning relies heavily on advanced cross-sectional imaging. Computed Tomography (CT) scans with three-dimensional (3D) reconstructions are invaluable for precisely assessing the volumetric amount and multiplanar direction of correction required. Magnetic Resonance Imaging (MRI), specifically utilizing radial sequences centered on the femoral head neck axis, allows for detailed assessment of the articular cartilage and labrum. Advanced techniques like Delayed Gadolinium-Enhanced MRI of Cartilage (dGEMRIC) provide a biochemical map of glycosaminoglycan concentration, offering a superior preoperative predictor of long-term PAO outcomes by identifying mechanically compromised, yet macroscopically intact, cartilage.

Operating Room Setup and Patient Positioning
Optimal patient positioning and operating room setup are critical for executing the complex geometry of the PAO safely. The patient is placed strictly supine on a fully radiolucent operating table. This is non-negotiable, as it allows for completely unrestricted, orthogonal fluoroscopic access throughout the entirety of the procedure. We utilize a C-arm fluoroscopy unit, positioned on the contralateral side of the operative hip, capable of swiftly providing AP, ilio-oblique, obturator-oblique, and false profile views.
The operative extremity is prepared and draped entirely free. The sterile field must extend superiorly to the costal margin, posteriorly to at least the posterior third of the iliac crest, and medially across the midline to the umbilicus. This extensive exposure ensures we have ample, unhindered access for both the anterior and deep medial aspects of our dissection, as well as the necessary trajectory for our osteotomes and fixation pins.
For perioperative pain management and to minimize the requirement for systemic narcotics, we routinely advocate for the placement of an epidural catheter prior to induction. This is typically maintained until postoperative day two or three. Concurrently, a Foley catheter is placed to decompress the bladder, minimizing the risk of iatrogenic injury during the deep pelvic dissection and superior pubic ramus osteotomy. Controlled hypotensive anesthesia is often employed to minimize blood loss from the highly vascular cancellous bone of the pelvis.
Step-by-Step Surgical Approach and Fixation Technique
The Surgical Approach and Deep Dissection
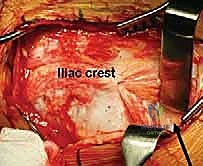
We standardly employ the longitudinal anterior Smith-Petersen approach, which provides unparalleled direct access to the anterior pelvis. While a transverse "bikini" (ilioinguinal) incision offers a superior cosmetic result, it can severely restrict access to the deep anterior ischium, particularly in muscular or obese patients. The skin incision begins slightly proximal and lateral to the ASIS, extending distally along the interval between the tensor fasciae latae (TFL) and the sartorius.

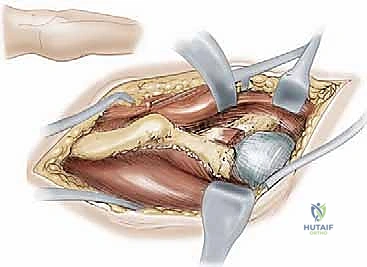
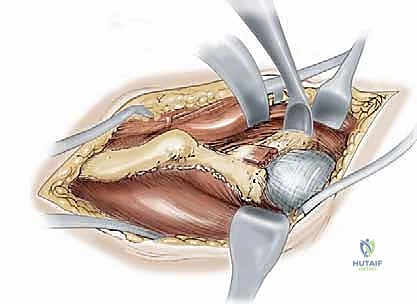
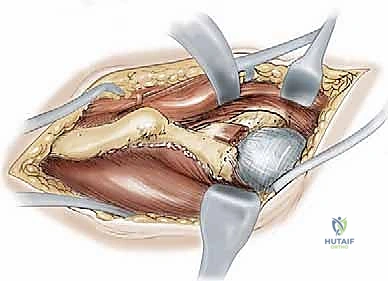
During the superficial dissection, meticulous identification and protection of the lateral femoral cutaneous nerve (LFCN) are paramount. The fascia over the TFL is incised, and the interval between the TFL and the sartorius/rectus femoris is developed. The ASIS is often managed via a thin wafer osteotomy, leaving the sartorius and inguinal ligament attached, which facilitates later repair and prevents avulsion. Deep dissection involves elevating the iliacus muscle subperiosteally from the inner table of the ilium, exposing the pelvic brim, the quadrilateral plate, and extending posteriorly toward the greater sciatic notch.
Simultaneously, the outer table of the ilium is exposed by elevating the abductor musculature (gluteus medius and minimus) just enough to visualize the supra-acetabular region and the capsule. The rectus femoris origin at the AIIS is identified; the direct head is typically preserved, while the reflected head may be released to expose the superior joint capsule. Blunt retractors (such as a Hohmann or a specialized Ganz retractor) are carefully placed over the pelvic brim and into the obturator foramen to protect the neurovascular bundle during the subsequent osteotomies.
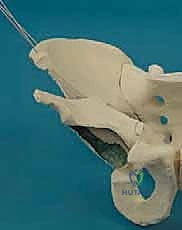
The Five Interconnected Osteotomies
The hallmark of the Bernese PAO is the sequence of five precise osteotomies.
1. The Anterior Ischial Osteotomy: This is arguably the most technically demanding cut. Working through the interval medial to the psoas tendon, a specialized angled osteotome is guided down the quadrilateral plate to the infracotyloid groove. The cut is made approximately 1.5 cm distal to the acetabular articular surface, directed posteriorly and slightly laterally, intentionally stopping short of complete cortical disruption to protect the sciatic nerve posteriorly and the MFCA laterally.
2. The Superior Pubic Ramus Osteotomy: A blunt retractor protects the obturator nerve and vessels. Using an oscillating saw or osteotome, the superior pubic ramus is cut obliquely, just medial to the iliopectineal eminence. This cut must be complete to allow for fragment mobilization.



- The Supra-acetabular Iliac Osteotomy: Using an oscillating saw, a transverse cut is made across the ilium, originating just inferior to the ASIS and terminating 1 to 2 cm short of the pelvic brim, directing the cut toward the apex of the greater sciatic notch.
- The Posterior Column (Retroacetabular) Osteotomy: This cut connects the medial aspect of the supra-acetabular cut to the posterior aspect of the ischial cut. Using a long, straight osteotome driven down the quadrilateral plate, the cut is angled approximately 120 degrees from the iliac cut, passing completely within the posterior column, remaining extra-articular, and crucially leaving the posterior cortex of the posterior column intact for pelvic stability.



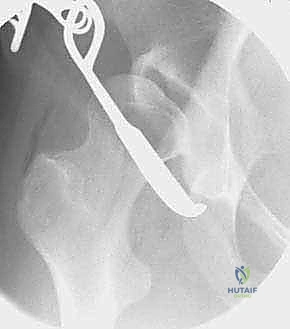
- The Final Liberation: A specialized bone hook or a heavy Schanz pin is placed into the supra-acetabular region of the fragment. With controlled, deliberate force, the remaining intact bone bridges (specifically the posterior ischial cortex) are fractured, fully mobilizing the acetabular fragment.
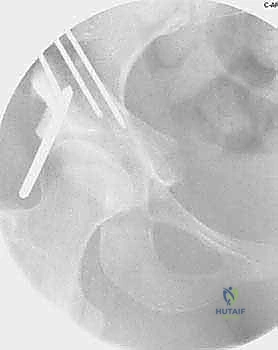
Reorientation and Definitive Fixation
Once liberated, the acetabular fragment is highly mobile. Using the Schanz pin as a joystick, the acetabulum is reoriented to achieve the preoperatively templated coverage. Typically, this involves anterior and lateral rotation (extension and abduction of the fragment) and medialization of the hip center. The fragment is temporarily held with long Kirschner wires.

Intraoperative fluoroscopy is absolutely critical at this juncture. AP, false profile, and ilio-oblique views are obtained to confirm the correction of the LCEA, normalization of the Tönnis angle, and restoration of anterior coverage without inducing iatrogenic retroversion or femoroacetabular
Clinical & Radiographic Imaging Archive