Miller MD et al: Essential Surgical Approaches to the Upper Extremity
Key Takeaway
Discover the latest medical recommendations for Miller MD et al: Essential Surgical Approaches to the Upper Extremity. The anterior (deltopectoral) approach is a primary surgical method for accessing the shoulder joint. It establishes an interval between the deltoid and pectoralis major muscles, facilitating exposure of the clavipectoral fascia, subscapularis, and proximal humerus. This approach, as described by miller md et al, involves mobilizing the cephalic vein and potentially dividing the subscapularis for deep joint access.
Introduction and Epidemiology
Surgical approaches to the upper extremity form the foundational basis of operative orthopedics, requiring a profound understanding of complex regional anatomy, neurovascular relationships, and internervous planes. The primary objective of any surgical approach is to provide adequate exposure of the osseous and soft tissue structures while minimizing iatrogenic trauma to the surrounding neurovascular bundles. The upper extremity is particularly unforgiving in this regard, given the dense concentration of critical nerves and vessels traversing narrow anatomical corridors.

Epidemiologically, upper extremity trauma accounts for a significant proportion of orthopedic surgical volume. Proximal humerus fractures represent approximately 5% to 6% of all adult fractures, with an increasing incidence in the aging osteoporotic population. Distal radius fractures are even more prevalent, constituting up to 17% of all fractures evaluated in emergency departments. The surgical management of these injuries, alongside elective procedures such as arthroplasty and tumor resection, demands a versatile armamentarium of surgical exposures.

The utilization of true internervous planes—corridors between muscles innervated by different peripheral nerves—is a core principle in orthopedic surgery. Dissection through an internervous plane ensures that the involved muscles remain innervated, preserving postoperative motor function. However, not all approaches utilize true internervous planes; some rely on muscle-splitting techniques or internodal planes where the risk of denervation is mitigated by specific anatomic characteristics, such as the proximal innervation of the deltoid or the dual innervation of the brachialis.

The historical evolution of upper extremity surgical approaches is deeply rooted in the pioneering work of anatomists and surgeons such as Arnold K. Henry and Stanley Hoppenfeld. Their meticulous cadaveric dissections established the safe zones and extensile exposures that remain the gold standard today. The modern orthopedic surgeon must synthesize this classical anatomical knowledge with contemporary techniques, including minimally invasive plate osteosynthesis and arthroscopically assisted fracture reduction, to optimize patient outcomes.

Understanding the epidemiology of upper extremity pathology is essential for anticipating the surgical approaches most frequently required in clinical practice. Beyond fractures, compressive neuropathies such as carpal tunnel syndrome and cubital tunnel syndrome necessitate precise surgical decompression. Furthermore, the rising incidence of primary osteoarthritis and rotator cuff arthropathy has led to an exponential increase in total shoulder arthroplasty and reverse total shoulder arthroplasty, procedures that rely heavily on the deltopectoral and anterolateral approaches.

Surgical Anatomy and Biomechanics
A rigorous comprehension of upper extremity anatomy is paramount for safe surgical dissection. The upper extremity is broadly divided into the shoulder girdle, brachium, elbow, antebrachium, and wrist. Each segment presents unique anatomical challenges and neurovascular hazards.

Shoulder Girdle Anatomy
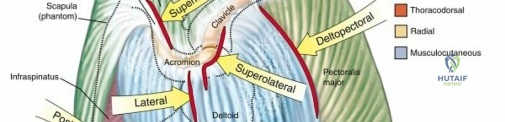
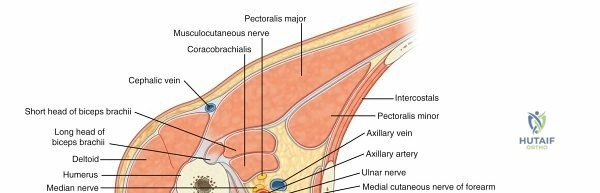
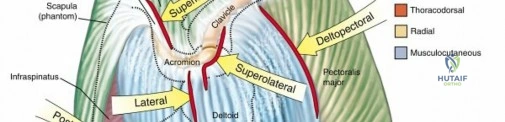
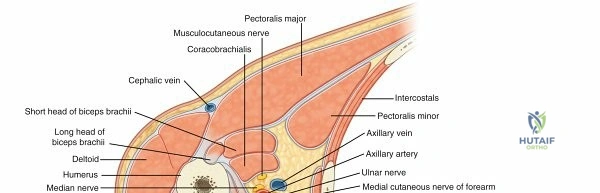
In the shoulder, the deltopectoral interval represents the standard workhorse approach. The superficial boundary is defined by the deltoid, innervated by the axillary nerve, and the pectoralis major, innervated by the medial and lateral pectoral nerves. The cephalic vein, a critical superficial landmark, courses within this interval and drains into the axillary vein after piercing the clavipectoral fascia. Deep to this interval lies the conjoint tendon, comprising the coracobrachialis and short head of the biceps, and the subscapularis.

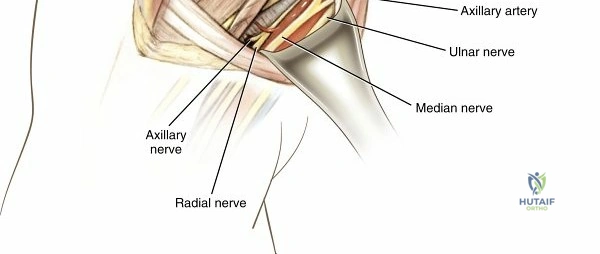
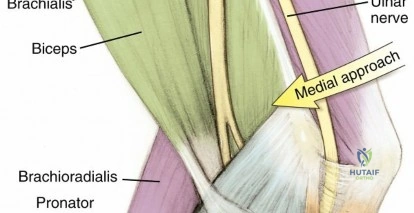
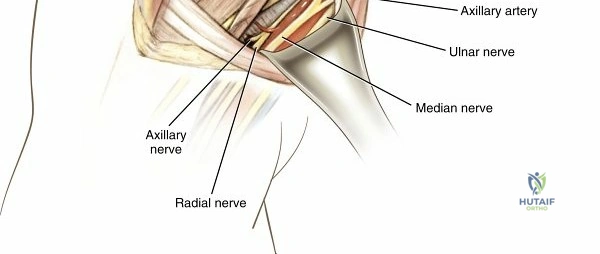
The axillary nerve is the primary structure at risk during shoulder approaches. It traverses the quadrangular space posteriorly but wraps anteriorly around the surgical neck of the humerus, typically 5 to 7 centimeters distal to the lateral acromion. This makes it highly susceptible to injury during distal extension of the deltopectoral approach or during lateral deltoid-splitting approaches. The musculocutaneous nerve enters the coracobrachialis approximately 5 to 8 centimeters distal to the coracoid process, dictating the safe zone for medial retraction of the conjoint tendon.

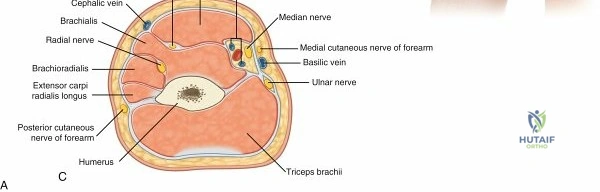
Brachium Anatomy
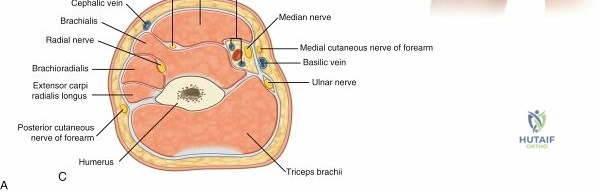
The brachium is defined by the anterior and posterior compartments, separated by the medial and lateral intermuscular septa. The radial nerve spirals from posterior to anterior along the spiral groove of the humerus, piercing the lateral intermuscular septum approximately 10 centimeters proximal to the radiocapitellar joint. This distinct anatomical course dictates the safe zones for both anterior and posterior humeral approaches.
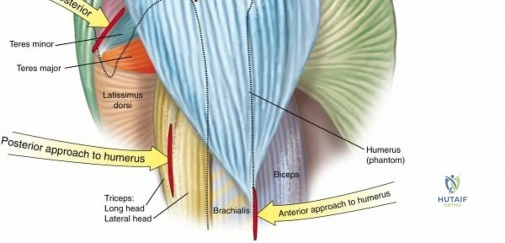

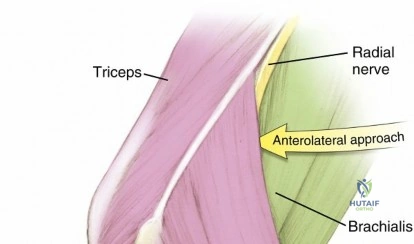
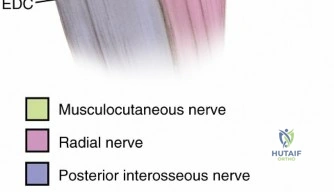
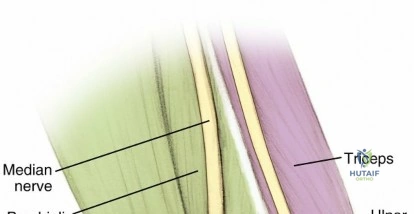
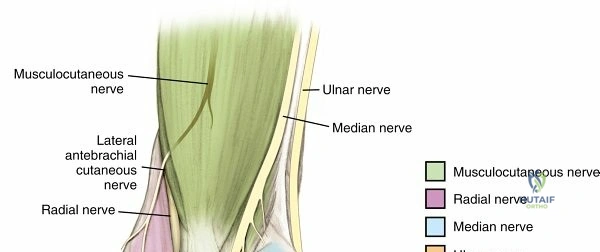
The brachialis muscle is uniquely innervated by both the musculocutaneous nerve medially and the radial nerve laterally. This dual innervation provides a safe longitudinal split for the anterolateral approach to the distal humerus, allowing extensive exposure of the humeral shaft without denervating the muscle. Posteriorly, the triceps brachii is innervated by the radial nerve, which gives off branches to the medial, lateral, and long heads before entering the spiral groove.


Elbow and Antebrachium Anatomy
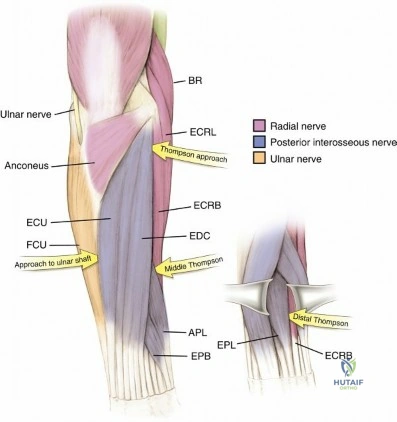
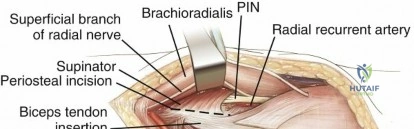
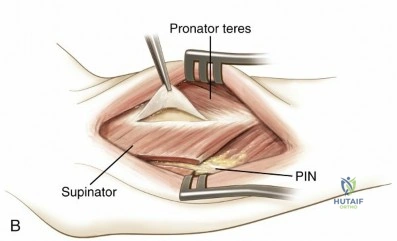
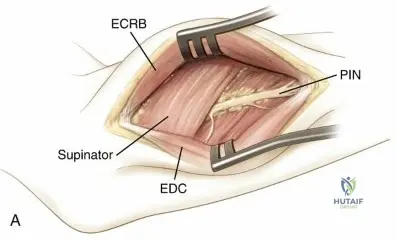
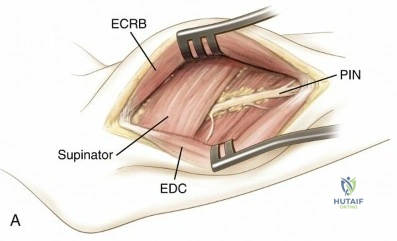
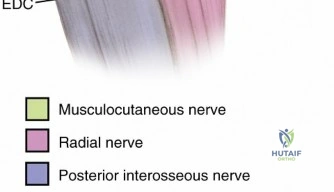
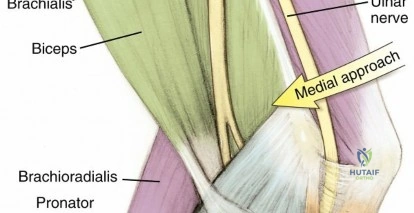
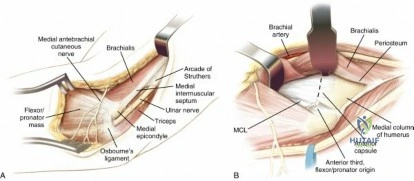
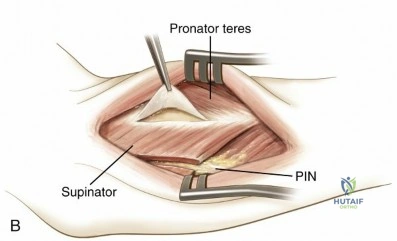
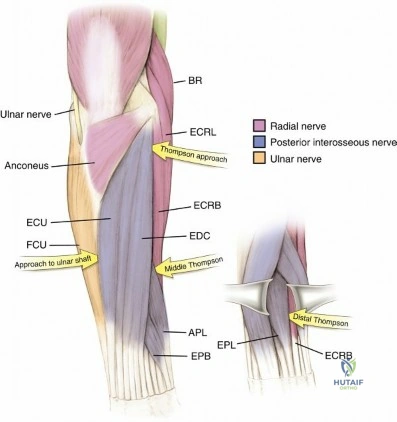
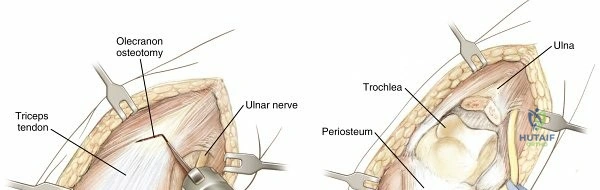
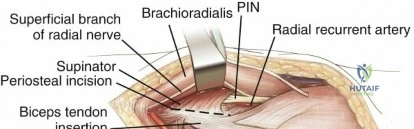
The elbow joint is a highly congruent ginglymoid joint. The ulnar nerve courses posterior to the medial epicondyle within the cubital tunnel, making it vulnerable during medial approaches or hardware placement for distal humerus fractures. Laterally, the radial nerve bifurcates into the superficial sensory branch and the deep posterior interosseous nerve anterior to the radiocapitellar joint. The posterior interosseous nerve then courses through the supinator muscle, crossing the proximal radius and defining the safe zone for proximal radius exposures.

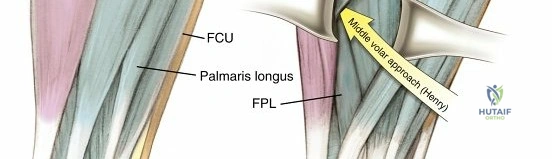
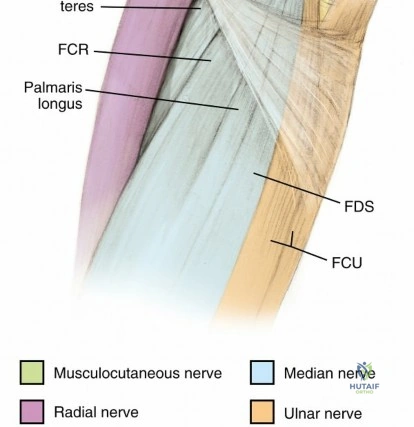
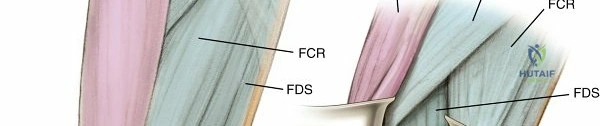
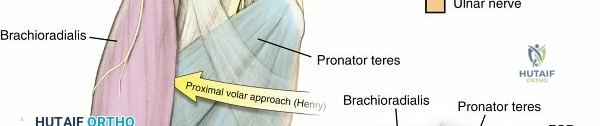
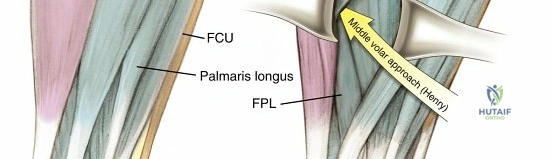
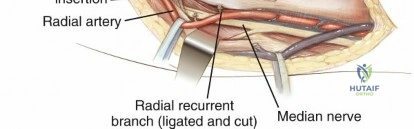
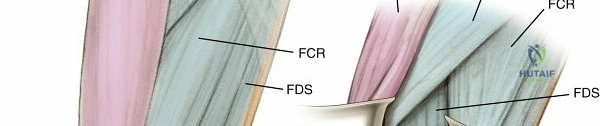
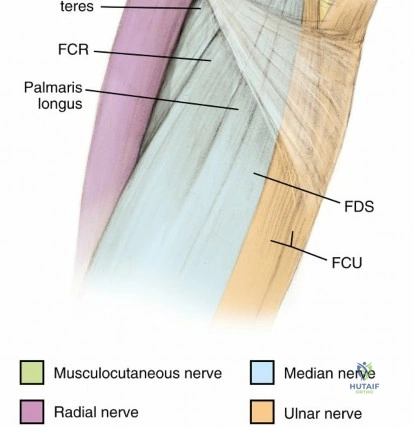
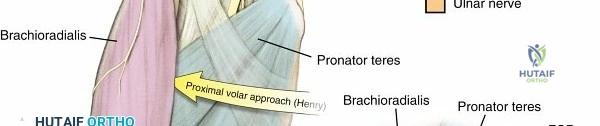
In the forearm, the volar compartment is supplied primarily by the median and ulnar nerves, while the dorsal compartment is supplied by the radial nerve. The classic volar approach of Henry utilizes the internervous plane between the brachioradialis, innervated by the radial nerve, and the pronator teres or flexor carpi radialis, innervated by the median nerve. This provides an extensile exposure to the entire volar radius.

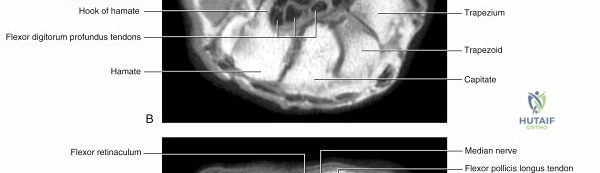
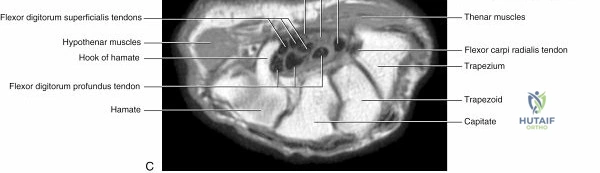
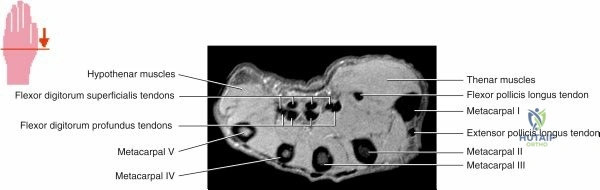
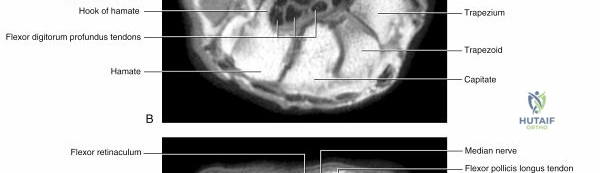
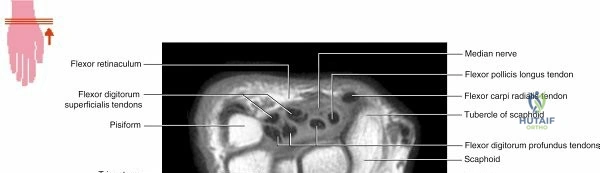
Wrist and Hand Anatomy
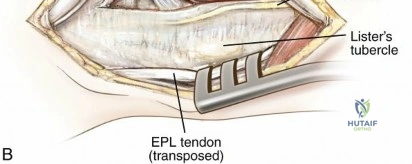
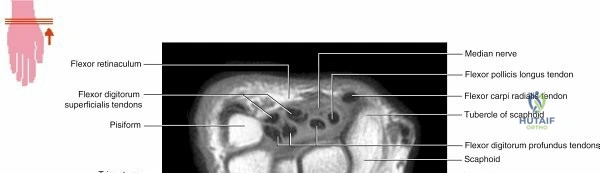
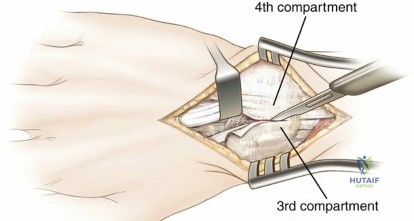
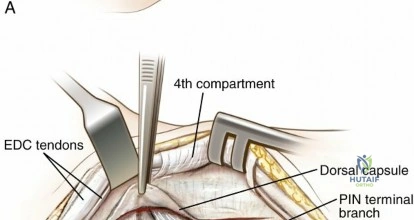
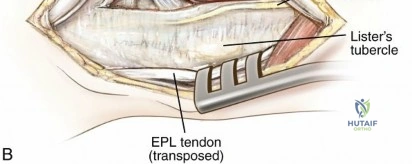
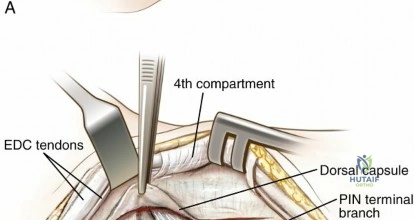
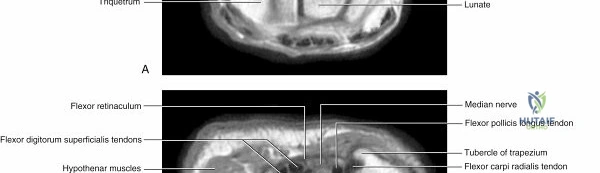
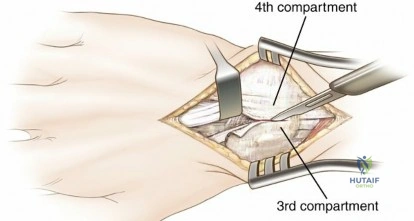
The distal radius and carpus present a complex array of tendons, nerves, and vessels. The volar aspect is characterized by the flexor tendons traversing the carpal tunnel alongside the median nerve. The flexor carpi radialis sheath is the standard landmark for the volar approach to the distal radius. Dorsally, the extensor tendons are divided into six distinct compartments by the extensor retinaculum. The dorsal approach to the wrist typically utilizes the interval between the third compartment, containing the extensor pollicis longus, and the fourth compartment, containing the extensor digitorum communis and extensor indicis proprius.

Indications and Contraindications
The selection of a surgical approach is dictated by the specific pathology, the required extent of exposure, the patient's soft tissue envelope, and the surgeon's familiarity with the regional anatomy. A poorly chosen approach can lead to inadequate reduction, inability to place appropriate fixation, and devastating neurovascular complications.
For proximal humerus fractures, the deltopectoral approach is the gold standard for arthroplasty and most cases of open reduction and internal fixation. However, for isolated greater tuberosity fractures or complex valgus-impacted patterns requiring direct lateral plate application, a deltoid-splitting approach may be indicated. The primary contraindication to a deltoid-splitting approach is the need for extensile distal exposure, which risks axillary nerve transection.


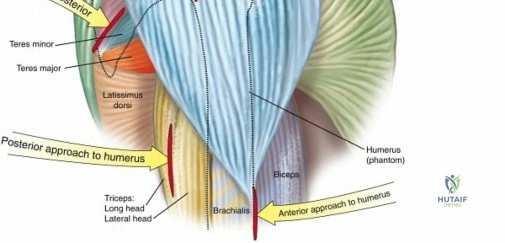
Humeral shaft fractures can be approached anteriorly or posteriorly. The anterolateral approach is excellent for proximal and middle third fractures, utilizing the internervous plane between the biceps and brachialis proximally, and splitting the brachialis distally. The posterior approach is indicated for distal third humeral shaft fractures, particularly those associated with radial nerve palsies requiring exploration, as it provides direct visualization of the radial nerve in the spiral groove.


Operative vs Non Operative Management
| Pathology | Operative Indications | Non-Operative Indications | Preferred Surgical Approach |
|---|---|---|---|
| Proximal Humerus Fracture | Displaced 3-part or 4-part fractures, head-splitting, fracture-dislocations | Minimally displaced, high surgical risk, non-ambulatory | Deltopectoral or Deltoid-splitting |
| Humeral Shaft Fracture | Open fractures, vascular injury, floating elbow, unacceptable alignment | Acceptable alignment (<20° anterior bowing, <30° varus/valgus, <3cm shortening) | Anterolateral or Posterior |
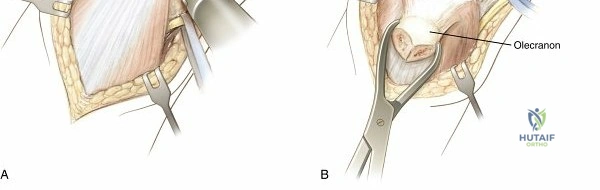
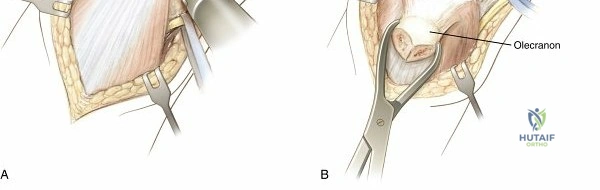
| Distal Humerus Fracture | Displaced intra-articular fractures, supracondylar nonunions | Undisplaced fractures in elderly/low-demand patients | Posterior (Olecranon osteotomy or TRAP) |
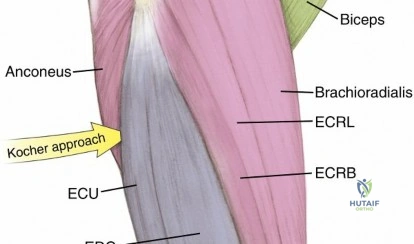
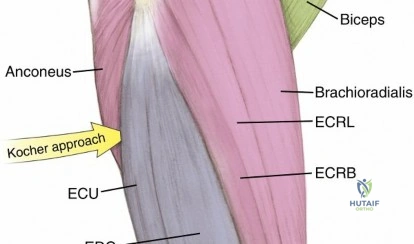
| Radial Head Fracture | Mechanical block to motion, >30% articular involvement, >2mm displacement | Minimally displaced, no mechanical block | Lateral (Kocher or Kaplan) |
| Both Bone Forearm Fracture | Displaced diaphyseal fractures in adults (almost all require ORIF) | Undisplaced fractures (rare in adults), pediatric plastic deformation | Volar Henry (Radius) + Direct Ulnar |
| Distal Radius Fracture | Volar comminution, >2mm articular step-off, >10° dorsal tilt, significant shortening | Undisplaced, stable post-reduction, low functional demand | Volar FCR approach |
Contraindications to specific approaches often revolve around prior surgical incisions, active localized infection, or compromised soft tissue envelopes. For instance, a patient with a prior volar wrist laceration and severe scarring may require a dorsal approach for a distal radius fracture to avoid inadvertent injury to the median nerve or flexor tendons embedded in scar tissue.
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is a non-negotiable prerequisite for successful upper extremity surgery. This begins with appropriate imaging. Standard orthogonal radiographs are mandatory. For complex intra-articular fractures of the proximal humerus, distal humerus, or distal radius, fine-cut computed tomography with three-dimensional reconstructions is essential to understand fracture morphology, articular comminution, and the location of specific fracture fragments.

Shoulder Positioning Strategies
Patient positioning for shoulder surgery generally involves either the beach chair position or the lateral decubitus position. The beach chair position is preferred for the deltopectoral and deltoid-splitting approaches, particularly for arthroplasty and fracture fixation. It allows for an anatomic orientation of the shoulder, easy conversion to an open procedure if performed arthroscopically, and unobstructed fluoroscopic access. The head and neck must be meticulously secured to prevent cervical spine hyperextension or lateral flexion, which can cause brachial plexus traction injuries.

The lateral decubitus position is frequently utilized for arthroscopic stabilization procedures and posterior approaches to the shoulder. It provides excellent visualization of the glenohumeral joint through longitudinal traction. Care must be taken to pad all bony prominences, particularly the common peroneal nerve at the fibular neck and the axilla of the dependent arm to prevent compressive neuropathies.
Humerus and Elbow Positioning
For the anterolateral approach to the humerus, the patient is positioned supine with the arm extended on a radiolucent hand table. A sterile tourniquet may be applied high on the brachium, though it is often omitted for proximal extensions. For the posterior approach to the humerus and elbow, the lateral decubitus or prone position is preferred. The arm is draped free over a post or padded mayo stand, allowing for elbow flexion to 90 degrees, which relaxes the triceps and facilitates exposure of the distal humerus.

Forearm and Wrist Positioning
Forearm and wrist procedures are almost universally performed with the patient in the supine position, with the operative extremity abducted onto a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. Exsanguination with an Esmarch bandage is performed prior to tourniquet inflation, typically to 250 mmHg or 100 mmHg above systolic blood pressure. The fluoroscopy unit should be positioned parallel to the hand table, entering from either the head or foot of the table depending on surgeon preference and anesthesia access.

Detailed Surgical Approach and Technique
The mastery of surgical technique requires an intimate knowledge of superficial landmarks, deep internervous planes, and the specific sequence of dissection. The following sections detail the essential surgical approaches to the upper extremity.
The Deltopectoral Approach
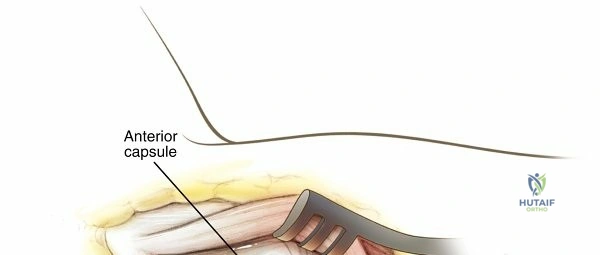
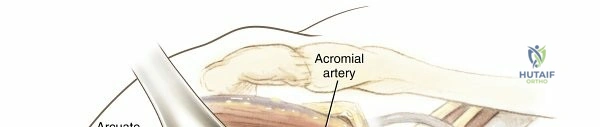
The deltopectoral approach is the primary exposure for the anterior shoulder. The incision begins at the tip of the coracoid process and extends distally and laterally along the deltopectoral groove toward the deltoid tuberosity. The superficial dissection identifies the cephalic vein, which is typically retracted laterally with the deltoid to preserve its major venous tributaries, though medial retraction is acceptable if lateral tributaries are sparse.

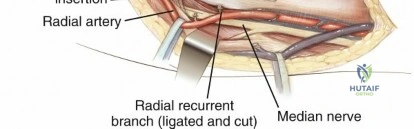
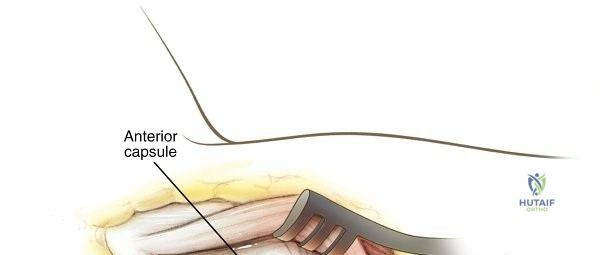
Deep dissection involves incising the clavipectoral fascia lateral to the conjoint tendon. The conjoint tendon is retracted medially. Care must be taken not to place retractors too deep medially to avoid injury to the musculocutaneous nerve. The subscapularis tendon is identified and can be managed via tenotomy, peel, or lesser tuberosity osteotomy depending on the procedure. The anterior humeral circumflex artery and vein, located at the inferior border of the subscapularis, must be identified and ligated to prevent troublesome bleeding.


The Anterolateral Approach to the Humerus
This approach provides excellent access to the proximal and middle thirds of the humeral shaft. The incision follows the lateral border of the biceps brachii. The superficial internervous plane lies between the biceps brachii (musculocutaneous nerve) and the brachioradialis (radial nerve) distally. Proximally, the plane is between the deltoid (axillary nerve) and the pectoralis major (pectoral nerves).

Deep dissection requires splitting the brachialis muscle longitudinally. Because the brachialis receives dual innervation, splitting the muscle along its midline preserves innervation to both halves. The lateral half acts as a protective cushion for the radial nerve. The periosteum is incised to expose the humeral shaft. Distal extension requires careful identification and protection of the radial nerve as it pierces the lateral intermuscular septum.

The Posterior Approach to the Humerus
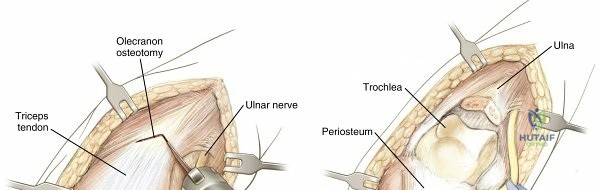
Indicated for distal third humeral shaft fractures, the posterior approach utilizes a midline longitudinal incision over the posterior arm. The superficial dissection exposes the triceps fascia. The deep exposure can be achieved via a triceps-splitting or a triceps-sparing (paratricipital) technique.
In the triceps-splitting approach, the long and lateral heads of the triceps are separated. The radial nerve and profunda brachii artery must be systematically identified in the spiral groove. The nerve crosses from medial to lateral along the posterior humerus. Once identified, it is mobilized with a vessel loop. The medial head of the triceps is then split longitudinally down to the bone to expose the distal humerus.


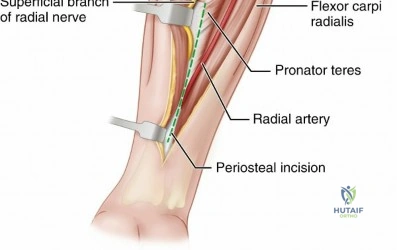
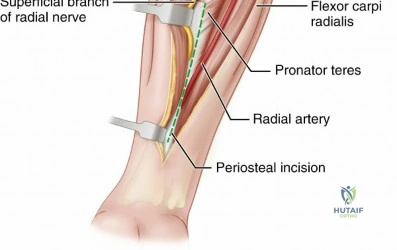
The Volar Henry Approach to the Radius
The volar approach of Henry provides extensile exposure to the entire volar surface of the radius. The incision extends from the biceps tendon distally to the radial styloid. The superficial internervous plane is between the brachioradialis (radial nerve) and the pronator teres/flexor carpi radialis (median nerve).