Essential Surgical Approaches: Upper Extremity by Miller MD et
Key Takeaway
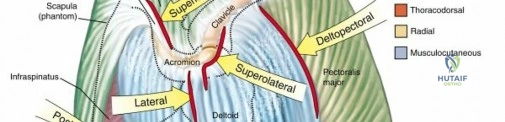
For anyone wondering about Essential Surgical Approaches: Upper Extremity by Miller MD et, The anterior (deltopectoral) approach is a surgical technique to access the shoulder joint. It utilizes the interval between the deltoid and pectoralis major muscles, protecting nerves like the axillary. This approach, consistent with principles taught by miller md et al., exposes the clavipectoral fascia, subscapularis, and proximal humerus, providing direct access for surgical intervention.
Introduction and Epidemiology
Surgical approaches to the upper extremity form the foundational bedrock of orthopedic trauma and reconstructive surgery. Mastery of these approaches requires an intimate understanding of cross-sectional anatomy, internervous planes, and neurovascular relationships. The primary objective of any surgical approach is to provide adequate exposure of the osseous and articular structures while minimizing iatrogenic soft tissue trauma, preserving vascular supply, and protecting critical peripheral nerves.


The epidemiology of upper extremity injuries dictates the frequency with which these approaches are utilized. Proximal humerus fractures account for approximately 5% of all fractures, with an increasing incidence in the aging osteoporotic population, frequently necessitating the deltopectoral or anterolateral deltoid-splitting approaches. Humeral shaft fractures represent 1-3% of all fractures, managed via anterolateral or posterior approaches depending on the fracture morphology and associated radial nerve pathology. Distal humerus, elbow, and forearm fractures (including Monteggia, Galeazzi, and both-bone forearm fractures) require precise utilization of approaches such as the Kocher, Kaplan, Henry, and Thompson intervals to restore complex articular mechanics and rotational kinematics.

The selection of an approach is dictated by the specific pathology, the need for proximal or distal extension, and the presence of prior incisions. True internervous planes—intervals between muscles innervated by different peripheral nerves—allow for extensile exposure without denervating the mobilized musculature. This concept, popularized by Henry and Hoppenfeld, remains the gold standard for atraumatic surgical dissection in the upper extremity.
Surgical Anatomy and Biomechanics
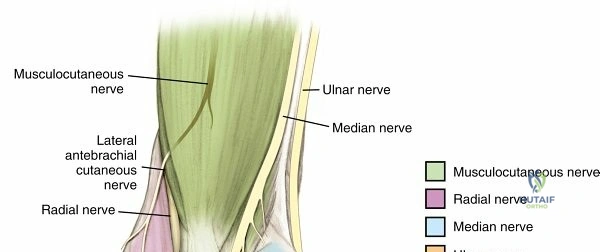
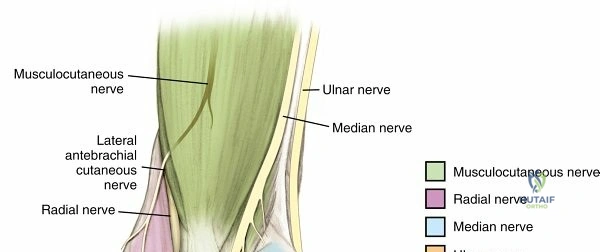
The upper extremity is functionally designed to position the hand in space, requiring a complex interplay of the shoulder girdle, elbow hinge, and radioulnar rotational axes. Surgical anatomy is best understood through the lens of the brachial plexus and its terminal branches, as these structures dictate the safe zones for dissection.
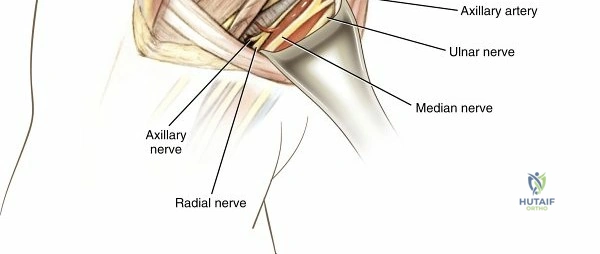
Shoulder and Proximal Humerus Anatomy
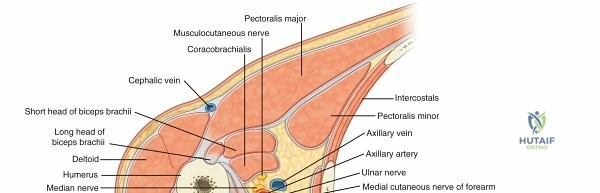
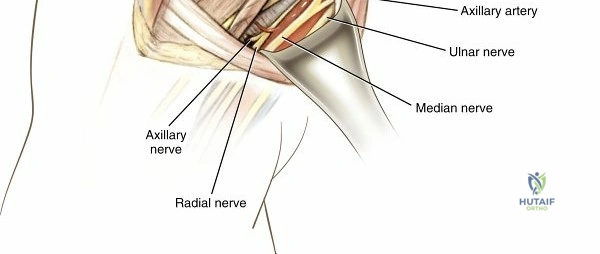
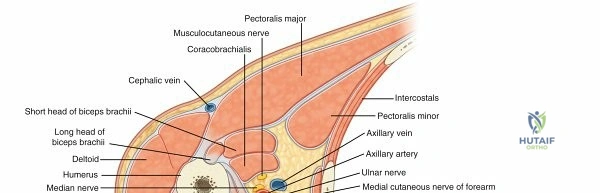
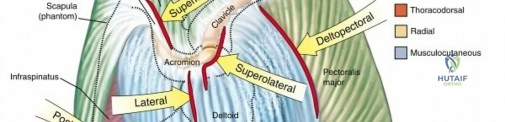
The deltoid (axillary nerve) and pectoralis major (medial and lateral pectoral nerves) form the primary anterior internervous plane. Deep to this, the clavipectoral fascia envelops the coracobrachialis and short head of the biceps (conjoint tendon). The axillary nerve traverses the quadrangular space, coursing transversely approximately 5 to 7 cm distal to the lateral acromial edge, creating a critical risk zone during lateral deltoid-splitting approaches. The anterior humeral circumflex artery (AHCA) and its venae comitantes form a leash of vessels marking the inferior border of the subscapularis.
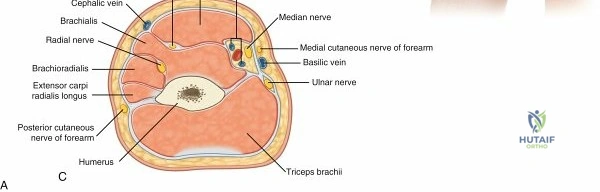
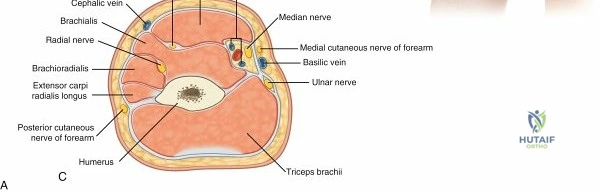
Humeral Shaft and Radial Nerve Kinematics
The radial nerve spirals around the posterior humerus, passing from medial to lateral through the triangular interval, lying directly on the periosteum in the spiral groove. It pierces the lateral intermuscular septum approximately 10 cm proximal to the radiocapitellar joint to enter the anterior compartment. Posterior approaches must account for the radial nerve and the profunda brachii artery, which dictate the limits of triceps splitting versus triceps sparing (paratricipital) techniques.


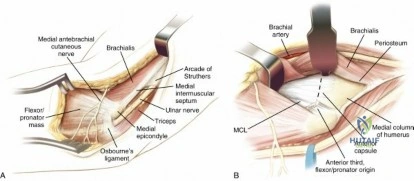
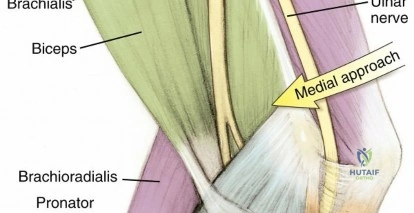
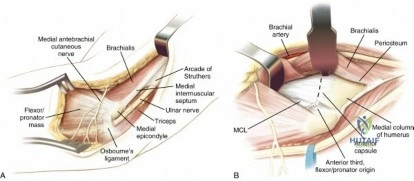
Elbow and Forearm Anatomy
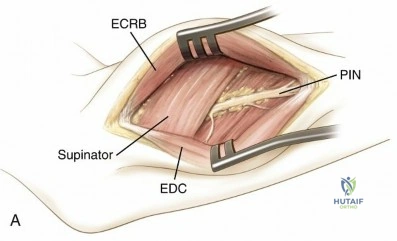
The elbow joint relies on the structural integrity of the medial ulnar collateral ligament (MUCL) and the lateral collateral ligament (LCL) complex. Approaches to the elbow must preserve these ligamentous origins. In the forearm, the axis of pronation and supination runs from the center of the radial head to the fovea of the distal ulna. The posterior interosseous nerve (PIN) enters the supinator arcade (arcade of Frohse) and is highly vulnerable during proximal radius exposures. Forearm supination translates the PIN laterally and anteriorly, moving it away from the surgical field during the volar Henry approach.

Indications and Contraindications
The selection of a surgical approach is dictated by fracture morphology, the necessity for articular visualization, the planned implant, and the patient's soft tissue envelope.
| Pathology | Non-Operative Indications | Operative Indications (Approach Selected) |
|---|---|---|
| Proximal Humerus Fracture | Minimally displaced, stable patterns; high surgical risk patients. | Displaced 3- or 4-part fractures, head-splitting patterns (Deltopectoral or Deltoid-splitting). |
| Humeral Shaft Fracture | <20° anterior angulation, <30° varus/valgus, <3 cm shortening. | Open fractures, vascular injury, floating elbow, bilateral humerus fractures (Anterolateral or Posterior). |
| Distal Humerus Fracture | Non-displaced extra-articular fractures in low-demand patients. | Displaced intra-articular fractures (Posterior approach with olecranon osteotomy or triceps-sparing). |
| Radial Head Fracture | Mason Type I or minimally displaced Type II without mechanical block. | Mason Type III, mechanical block to rotation, associated instability (Kocher or Kaplan). |
| Both-Bone Forearm Fracture | Pediatric incomplete fractures (greenstick/torus) with acceptable alignment. | Displaced fractures in adults, Monteggia/Galeazzi variants (Volar Henry for radius, Subcutaneous for ulna). |
Contraindications
Absolute contraindications to specific approaches include active soft tissue infection directly overlying the planned incision and severe soft tissue compromise (e.g., severe degloving or fracture blisters) that precludes safe wound closure. Relative contraindications involve pre-existing nerve palsies where an approach might jeopardize the only remaining functional nerve supply to a compartment, or prior incisions that dictate a modified approach to prevent skin bridge necrosis.
Pre Operative Planning and Patient Positioning
Thorough preoperative planning involves orthogonal radiographs and, frequently, computed tomography (CT) with 3D reconstructions for intra-articular fractures of the shoulder, elbow, and wrist. Templating software is utilized to determine plate length, screw trajectory, and the necessity for structural allografts or arthroplasty components.


Positioning Strategies
- Beach Chair Position: Ideal for the anterior deltopectoral approach. The patient is elevated 30-45 degrees. The arm must be completely free to allow for extension, abduction, and rotation, which are critical for mobilizing the proximal humerus and relaxing the deltoid.
- Lateral Decubitus: Utilized for posterior shoulder approaches or arthroscopic procedures. Requires careful padding of the axilla to prevent brachial plexus neuropraxia.
- Supine with Hand Table: Standard for anterolateral humerus, anterior elbow, forearm, and wrist approaches. A sterile tourniquet is typically applied to the proximal arm.
- Lateral or Prone: Preferred for posterior approaches to the humeral shaft and distal humerus. The arm is draped over a radiolucent post or resting on a Mayo stand. Prone positioning allows for excellent visualization of the posterior column of the distal humerus but requires meticulous airway and ocular protection.



Detailed Surgical Approach and Technique
Shoulder Approaches
Anterior Deltopectoral Approach
This is the workhorse approach for proximal humerus fractures, shoulder arthroplasty, and anterior instability procedures.
* Superficial Interval: Deltoid (axillary nerve) and Pectoralis major (medial and lateral pectoral nerves).
* Dissection: The incision is made from the coracoid process extending distally toward the deltoid tuberosity. The interval is marked by the cephalic vein. The vein is mobilized laterally with the deltoid or medially with the pectoralis major depending on surgeon preference and venous tributary anatomy (preserving the vein laterally is often preferred to maintain deltoid venous drainage).
* Deep Dissection: Retracting the deltoid laterally and the pectoralis medially exposes the clavipectoral fascia. This fascia is incised lateral to the conjoint tendon. The conjoint tendon is retracted medially, taking care to avoid vigorous retraction which can cause neuropraxia to the musculocutaneous nerve (which enters the coracobrachialis 5-8 cm distal to the coracoid).
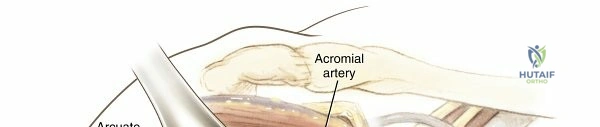
* Articular Access: The subscapularis and proximal humerus are exposed. The inferior border of the subscapularis is demarcated by the anterior humeral circumflex vessels (the "leash of Henry"). For joint access, the subscapularis is incised longitudinally, tenotomized, or elevated via a lesser tuberosity osteotomy.



Lateral Deltoid-Splitting Approach
Utilized for open reduction internal fixation (ORIF) of greater tuberosity fractures and proximal humerus fractures utilizing locked plating.
* Interval: Split within the anterior and middle thirds of the deltoid (both axillary nerve). This is not a true internervous plane.
* Dissection: Incision extends distally from the lateral acromion. The deltoid is split bluntly for no more than 5 cm to avoid the axillary nerve, which courses transversely deep to the muscle. A stay suture is often placed at the distal apex of the split to prevent inadvertent distal propagation and nerve transection.


Posterior Shoulder Approach
- Superficial Interval: Split deltoid (axillary nerve).
- Deep Interval: Infraspinatus (suprascapular nerve) and Teres minor (axillary nerve).
- Dissection: Used for posterior glenoid fractures and posterior instability. The deltoid is detached from the spine of the scapula or split in line with its fibers. The deep interval exposes the posterior capsule.


Humerus Approaches
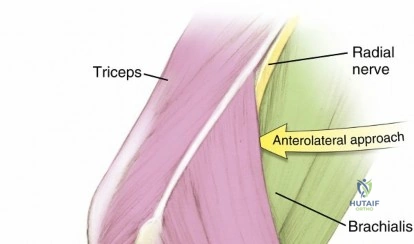
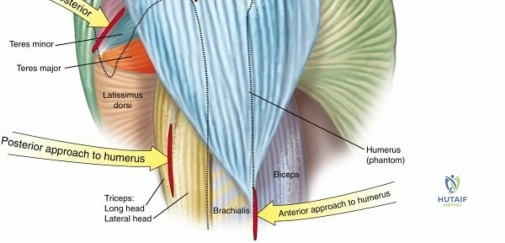
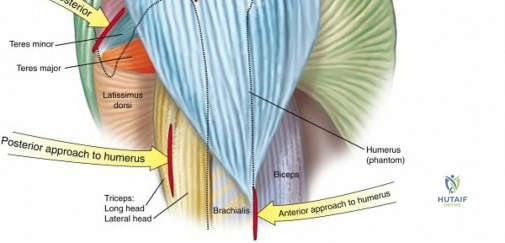
Anterolateral Approach
Can be utilized for the entire humeral shaft.
* Proximal Interval: Deltoid and Pectoralis major.
* Middle/Distal Interval: Lateral to the biceps (musculocutaneous nerve) and splitting the brachialis.
* Dissection: The brachialis has dual innervation (musculocutaneous medially, radial laterally). Splitting the brachialis longitudinally provides a safe, extensile approach to the anterior humeral shaft. The radial nerve is protected within the lateral half of the brachialis muscle belly.

Posterior Humerus Approach
Ideal for mid-to-distal third humeral shaft fractures.
* Interval: Triceps splitting or triceps sparing.
* Dissection (Triceps Splitting): Incision midline over the posterior arm. The interval between the lateral and long heads of the triceps is developed. Deep to this, the medial head of the triceps is split longitudinally to expose the posterior humerus. The radial nerve and profunda brachii vessels must be identified as they cross the posterior humerus from medial to lateral in the spiral groove.
* Dissection (Triceps Sparing/Paratricipital): The entire triceps muscle is mobilized from the lateral and medial intermuscular septa, allowing visualization of the posterior humerus without violating the extensor mechanism.


Elbow Approaches
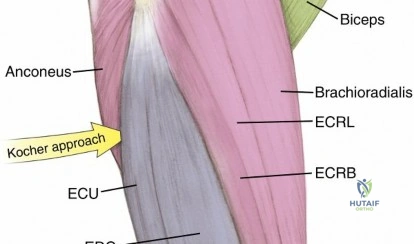
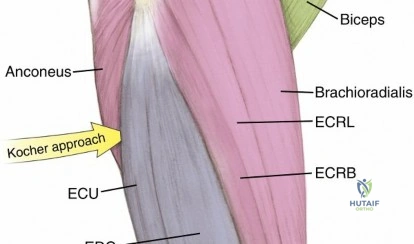
Posterolateral (Kocher) Approach
Standard approach for radial head fractures and lateral collateral ligament reconstruction.
* Interval: Anconeus (radial nerve) and Extensor Carpi Ulnaris (PIN).
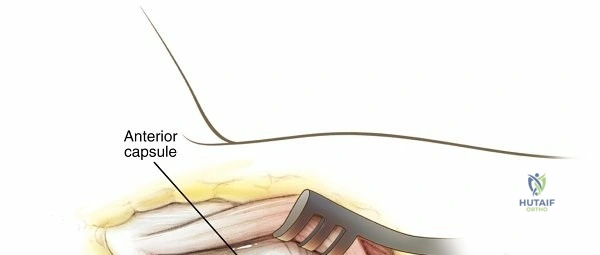
* Dissection: The origin of the anconeus and ECU is identified at the lateral epicondyle. The interval is developed distally. The capsule is incised anterior to the equator of the radial head to prevent iatrogenic injury to the LUCL (lateral ulnar collateral ligament), which inserts on the supinator crest of the ulna. The PIN lies within the supinator muscle belly distally and must be protected by keeping the forearm pronated during deep retraction.


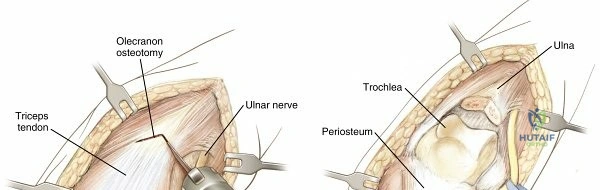
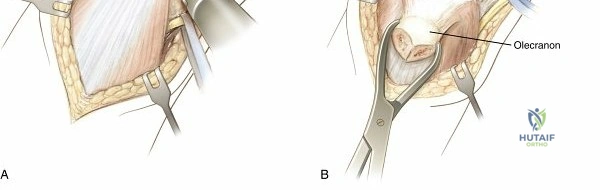
Posterior Elbow Approaches
Utilized for distal humerus intra-articular fractures.
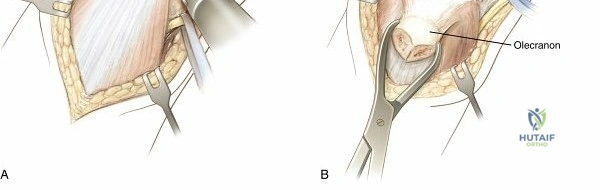
* Options: Olecranon osteotomy, Bryan-Morrey (triceps-sparing), or triceps-splitting. None of these possess a true internervous plane.
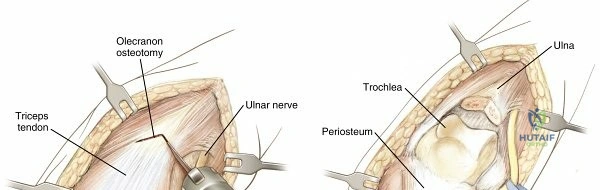
* Olecranon Osteotomy: Provides maximal articular exposure. A chevron osteotomy is performed bare-area of the sigmoid notch. The olecranon and attached triceps are reflected proximally. The ulnar nerve must be identified, mobilized, and protected throughout the procedure.

Forearm Approaches
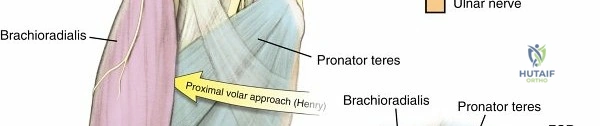
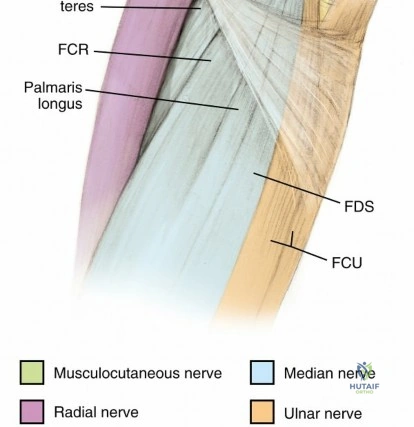
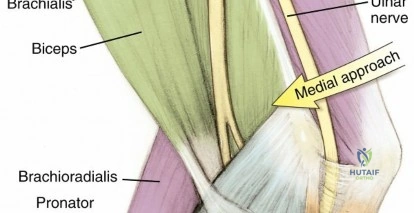
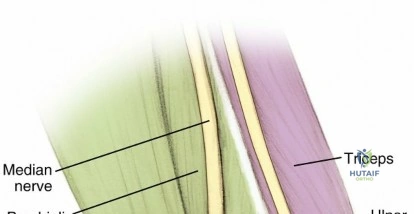
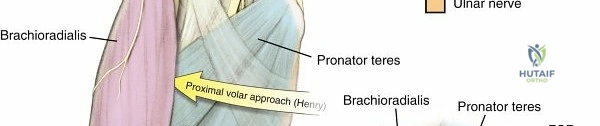
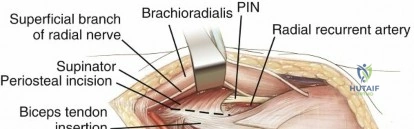
Anterior (Henry) Approach to the Radius
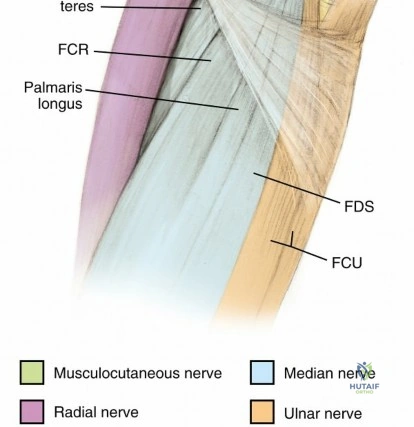
- Superficial Interval: Brachioradialis (radial nerve) and Pronator Teres/Flexor Carpi Radialis (median nerve).
- Deep Interval: Varies proximally to distally. Proximally, between the supinator (PIN) and pronator teres (median). Distally, between the brachioradialis and FCR.
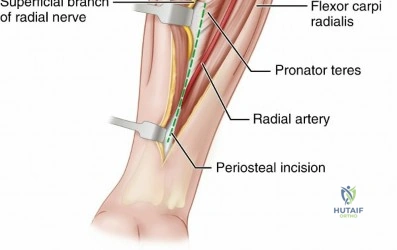
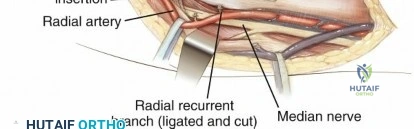
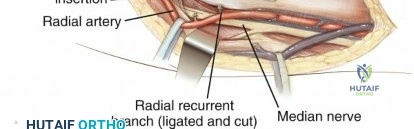
- Dissection: Incision follows a line from the biceps tendon to the radial styloid. The superficial fascia is incised. The radial artery is identified under the brachioradialis and mobilized medially. The superficial branch of the radial nerve runs on the undersurface of the brachioradialis and is retracted laterally. In the proximal third, the recurrent radial artery (leash of Henry) must be ligated. The supinator is elevated off the radius with the forearm fully supinated to protect the PIN.

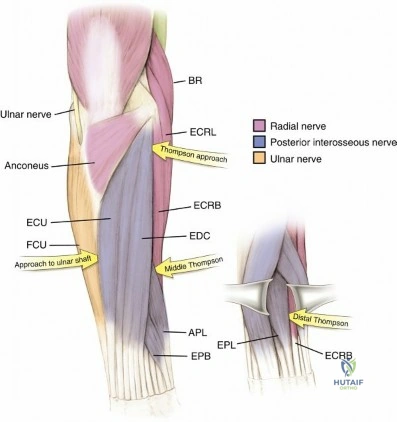
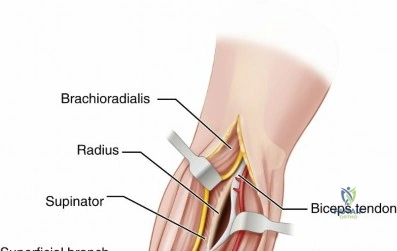
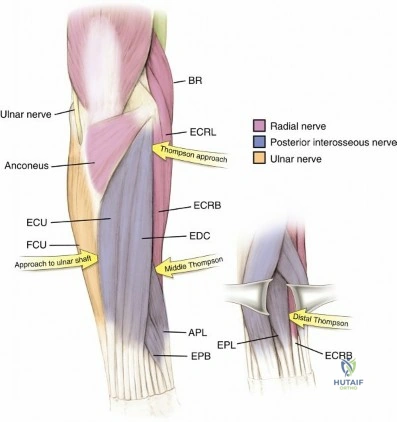
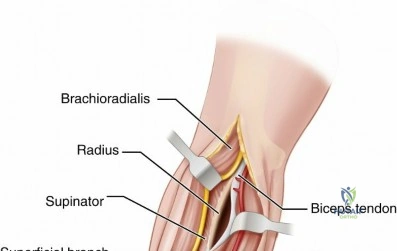
Posterior (Thompson) Approach to the Radius
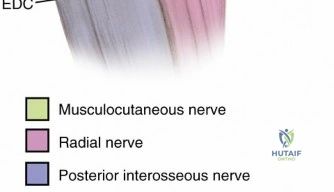
- Superficial Interval: Extensor Carpi Radialis Brevis (radial/PIN) and Extensor Digitorum Communis (PIN).
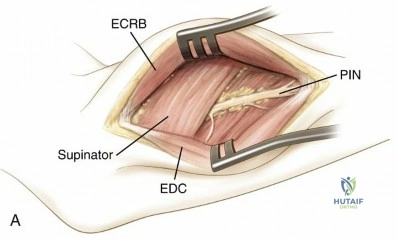
- Dissection: Used primarily for proximal and middle third radius fractures. The interval is developed to expose the supinator. The PIN must be directly visualized or safely bypassed by elevating the supinator from ulnar to radial.

Posterior Approach to the Ulna
- Interval: Extensor Carpi Ulnaris (PIN) and Flexor Carpi Ulnaris (ulnar nerve).
- Dissection: The ulnar shaft is subcutaneous. The approach is performed directly between the ECU and FCU. The periosteum is incised directly over the subcutaneous border of the ulna.

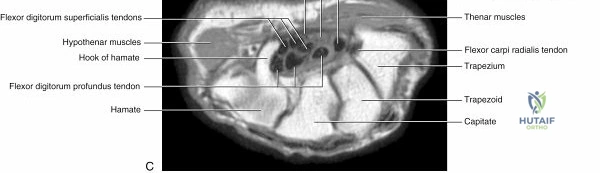
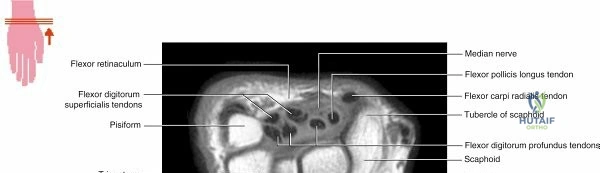
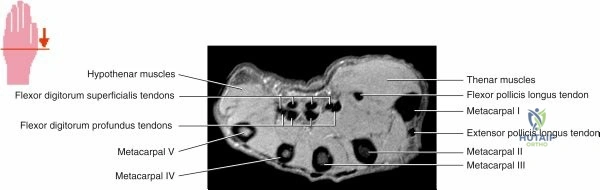
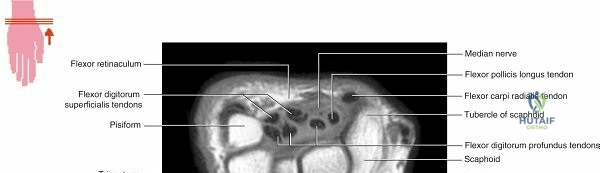
Wrist Approaches
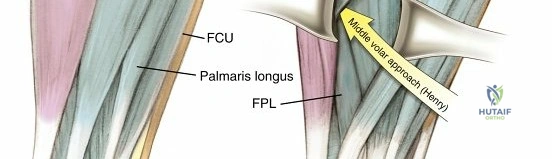
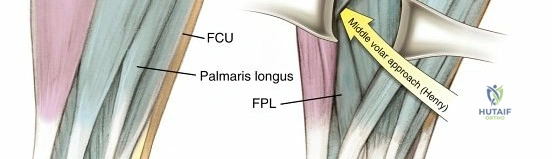
Volar (Distal Henry) Approach
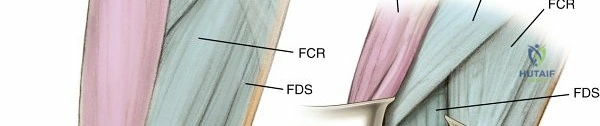
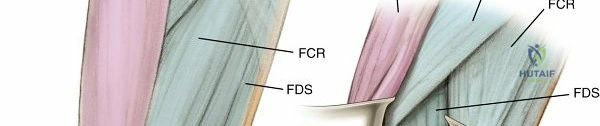
- Interval: FCR (median nerve) and Radial Artery.
- Dissection: Standard for distal radius fractures. The FCR sheath is opened, and the tendon is retracted ulnarly, protecting the median nerve. The floor of the FCR sheath is incised to expose the flexor pollicis longus (FPL) and the pronator quadratus (PQ). The PQ is elevated from its radial border (L-shaped incision) to expose the volar cortex of the distal radius.


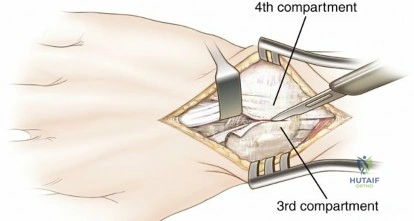
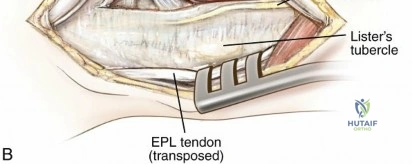
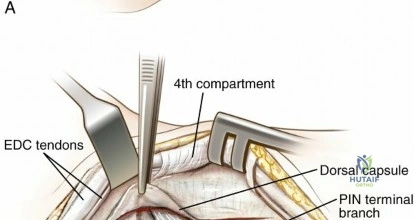
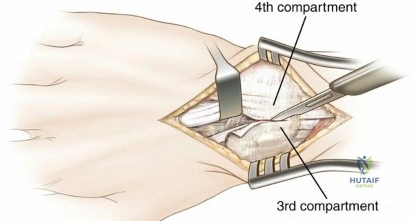
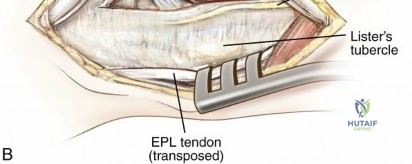
Dorsal Approach
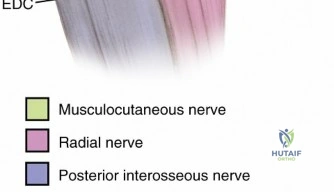
- Interval: Between the third (EPL) and fourth (EDC) extensor compartments.
- Dissection: Extensor retinaculum is incised. The EPL is mobilized from Lister's tubercle. The floor of the compartments is elevated to expose the dorsal radius and carpus. There is no true internervous plane here, as all structures are PIN
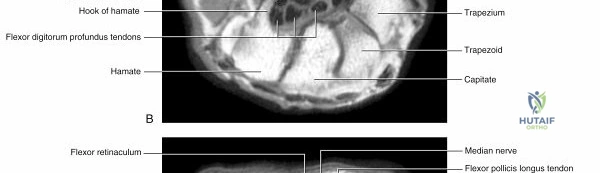
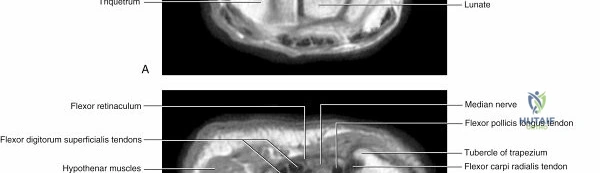
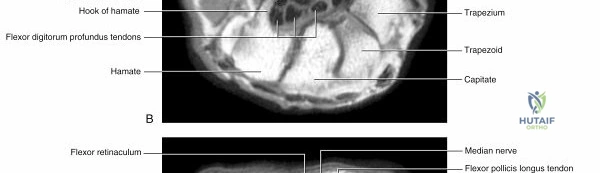
Clinical & Radiographic Imaging