Surgical Access: Mastering the Tibia's Surface & Fibula Approaches
Key Takeaway
Here are the crucial details you must know about Surgical Access: Mastering the Tibia's Surface & Fibula Approaches. Surgical approaches to the tibia include anterior and posterolateral for the shaft, and anterolateral, posteromedial, posterolateral, and posterior for the tibial plateau. The anterior approach is commonly used for the shaft due to its easy access to the subcutaneous surface of the tibia, offering direct surgical entry. This broad, accessible surface makes the tibia a frequent target for various surgical interventions.
Comprehensive Introduction and Patho-Epidemiology
The surgical management of tibial and fibular pathology represents a cornerstone of orthopedic trauma and reconstructive surgery. The tibia and fibula, while approximately equal in length, possess starkly contrasting structural characteristics and biomechanical functions. The tibia is a massive, weight-bearing monolith that transmits the vast majority of the axial stress generated during ambulation. Its broad, subcutaneous anteromedial surface renders it highly accessible to the surgeon but simultaneously exceptionally vulnerable to high-energy trauma and subsequent soft tissue compromise. Conversely, the fibula is a slender, strut-like bone that absorbs approximately one-sixth of the axial load. Its primary biomechanical mandate is the maintenance of ankle mortise stability and the provision of a robust origin for the complex musculature of the leg.
Epidemiologically, fractures of the tibial diaphysis are the most common long bone fractures encountered by orthopedic surgeons, often resulting from high-energy mechanisms such as motor vehicle collisions or significant falls. Proximal tibial articular fractures, encompassing the diverse spectrum of tibial plateau injuries, exhibit a bimodal distribution. High-energy mechanisms predominantly affect young males, often resulting in complex bicondylar fractures with severe soft tissue degloving. In contrast, low-energy falls typically inflict lateral depression or split-depression fractures in osteoporotic elderly populations. The sheer volume and complexity of these injuries necessitate an exhaustive understanding of the surgical corridors available to the operating surgeon.
Historically, the approach to the tibia and fibula was dictated by a philosophy of extensile exposure, prioritizing absolute anatomical reduction of the bone over the preservation of the soft tissue envelope. This paradigm frequently led to catastrophic complications, including wound dehiscence, deep infection, and refractory nonunions. Modern orthopedic surgery has undergone a radical paradigm shift toward soft tissue preservation, giving rise to minimally invasive percutaneous osteosynthesis (MIPO) and the strategic utilization of anatomically precise, limited-incision approaches. The modern surgeon must master not only the traditional extensile exposures but also these nuanced, tissue-sparing techniques to optimize patient outcomes.
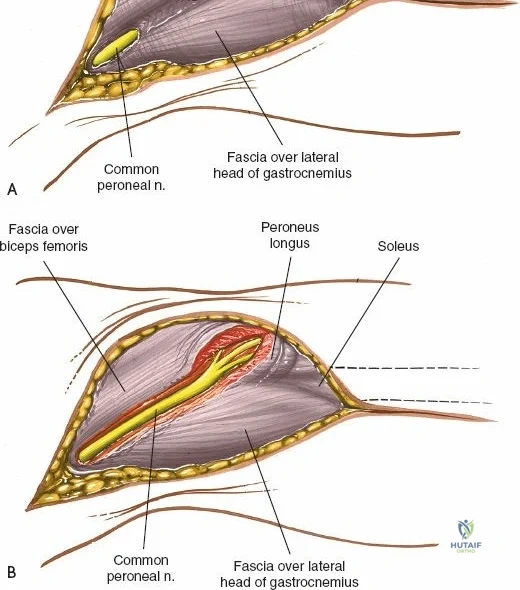
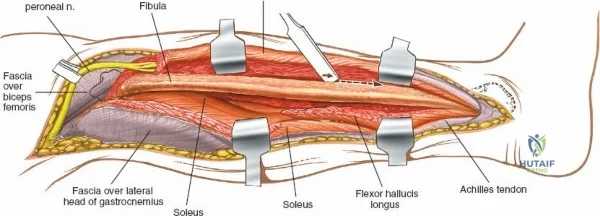
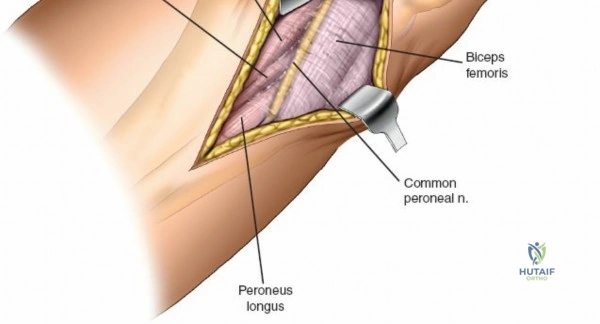
The decision-making process regarding surgical access is intrinsically linked to the personality of the fracture, the condition of the soft tissue envelope, and the planned method of fixation. Approaches to the fibular shaft, for instance, are notoriously complex due to the deep muscular encasement of the bone and the perilous winding of the common peroneal nerve around the fibular neck. Mastery of these approaches requires a profound, three-dimensional spatial awareness of the leg's neurovascular topography. This chapter serves as a definitive guide to navigating these complex surgical corridors, providing the orthopedic surgeon with the anatomical mastery required to execute these approaches safely and effectively.
Detailed Surgical Anatomy and Biomechanics
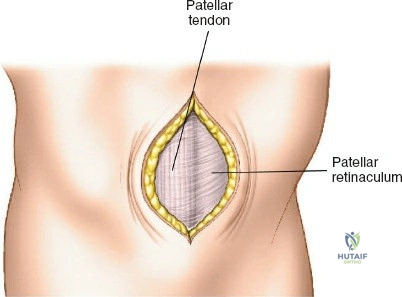
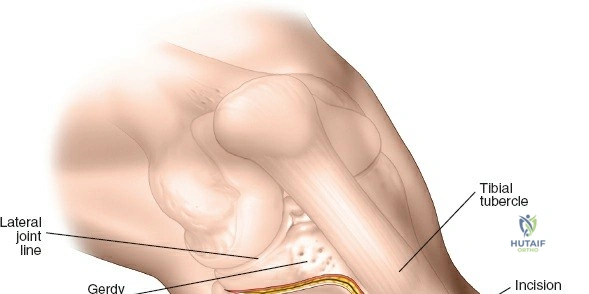
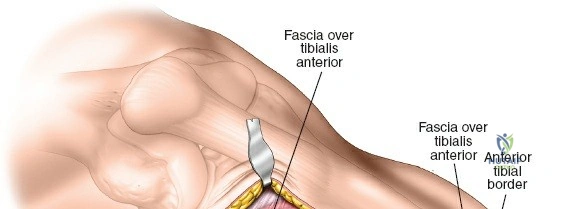
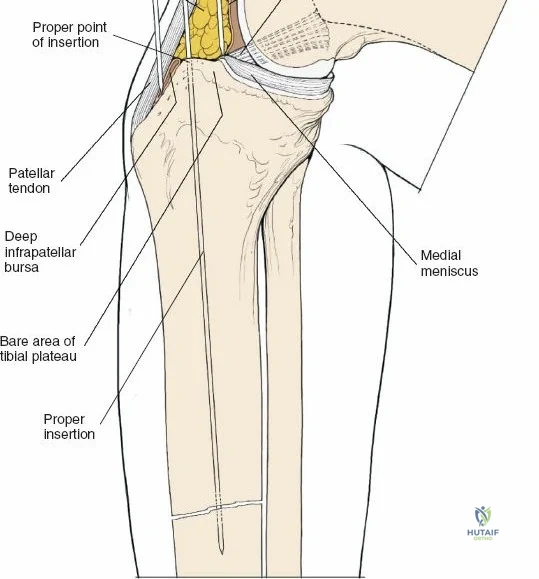
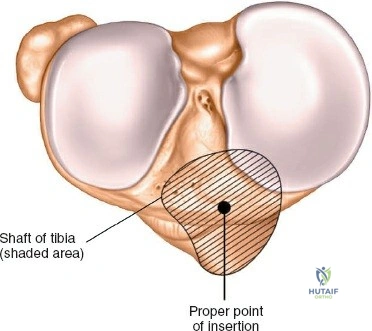
A profound comprehension of the osteology and regional anatomy of the leg is the absolute prerequisite for executing safe surgical approaches. The proximal tibia expands into the medial and lateral condyles, which form the tibial plateau. The medial plateau is larger, concave, and bears a greater proportion of the physiological load, whereas the lateral plateau is convex, smaller, and elevated relative to its medial counterpart. The intercondylar eminence serves as the crucial attachment site for the cruciate ligaments and menisci. Anteriorly, the tibial tubercle provides the insertion for the patellar tendon, while laterally, Gerdy’s tubercle serves as the insertion point for the iliotibial band.
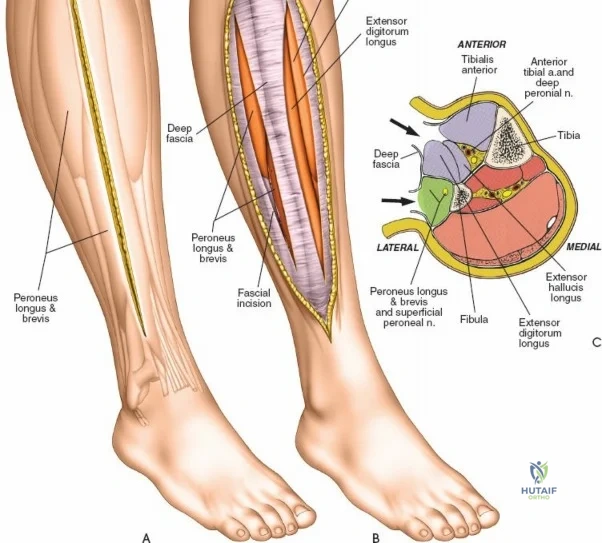
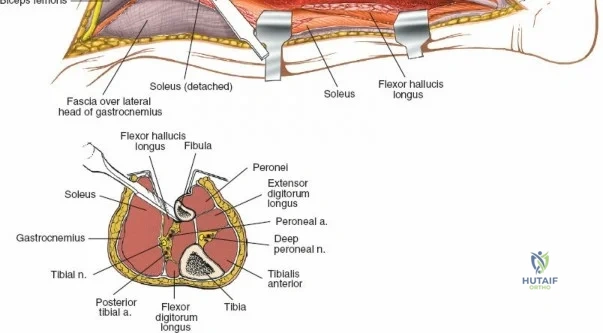
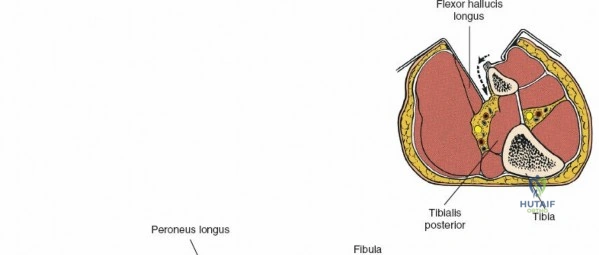
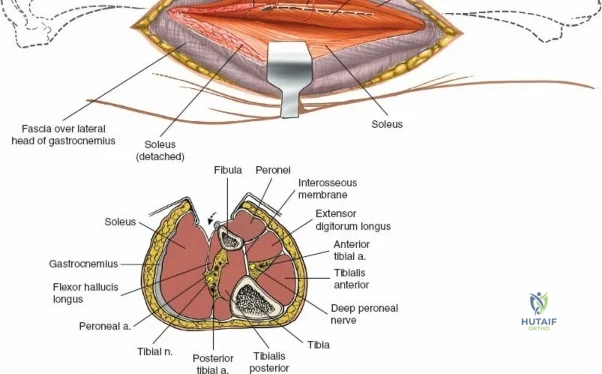
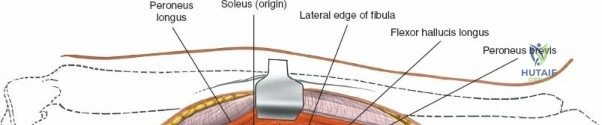
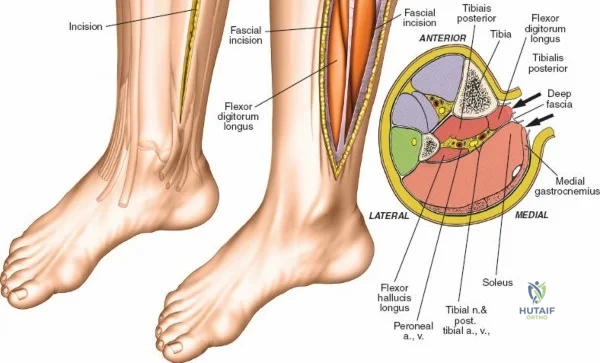
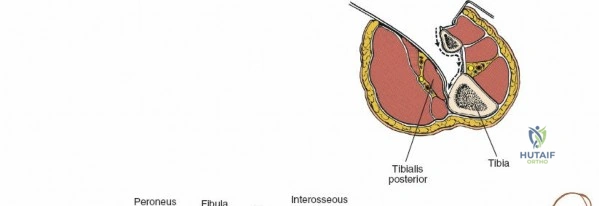
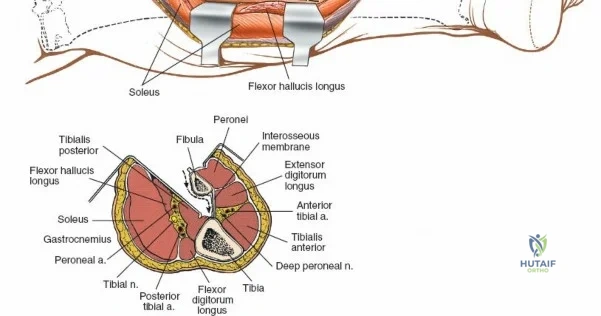
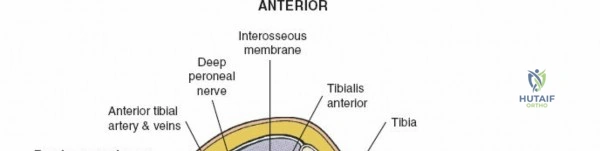
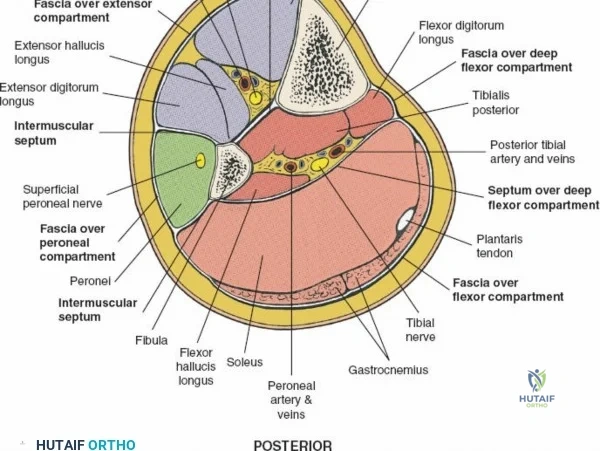
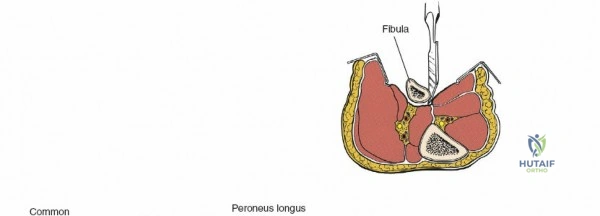
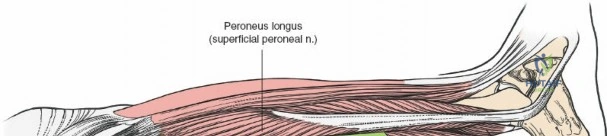
The leg is anatomically partitioned into four distinct fascial compartments: the anterior, lateral, superficial posterior, and deep posterior compartments. The anterior compartment houses the tibialis anterior, extensor hallucis longus, extensor digitorum longus, and peroneus tertius, all innervated by the deep peroneal nerve. The anterior tibial artery provides the vascular supply to this compartment. The lateral compartment contains the peroneus longus and brevis, innervated by the superficial peroneal nerve. The rigid fascial boundaries separating these compartments are unyielding, rendering the leg highly susceptible to acute compartment syndrome following trauma or reperfusion injury, necessitating emergent surgical decompression via dual-incision fasciotomies.
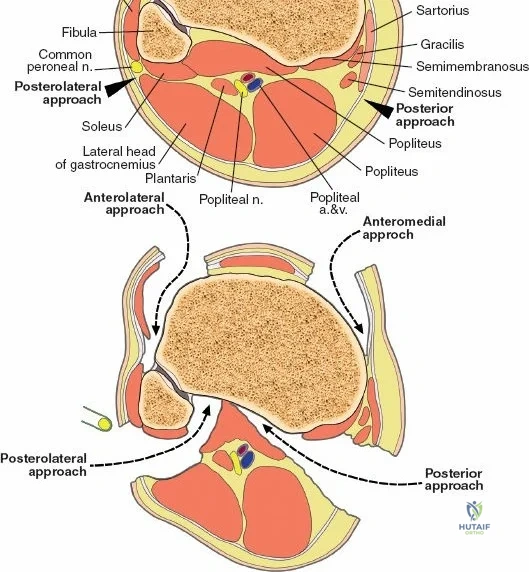
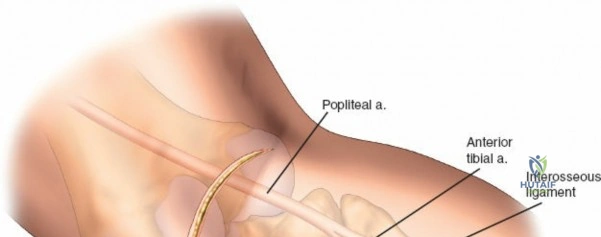
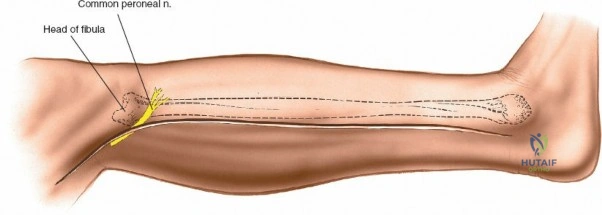
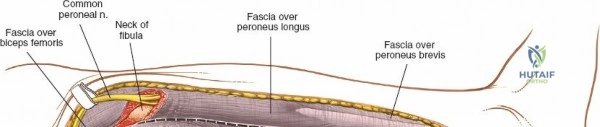
Neurovascular mapping is critical when dissecting the proximal tibia and fibula. The popliteal artery descends posterior to the knee joint, bifurcating at the distal border of the popliteus muscle into the anterior tibial artery and the tibioperoneal trunk. The anterior tibial artery courses anteriorly through the interosseous membrane, a vulnerable location during proximal tibial osteotomies or posterior approaches. The common peroneal nerve is arguably the most critical structure at risk during lateral approaches. It descends along the medial border of the biceps femoris, winds around the fibular neck subcutaneously, and pierces the peroneus longus muscle before dividing into its superficial and deep branches. Iatrogenic injury to this nerve results in devastating foot drop and loss of dorsal foot sensation.
Biomechanically, the tibia acts as the primary compressive strut of the lower extremity. During the gait cycle, the medial aspect of the tibia is subjected to significant compressive forces, while the anterolateral aspect experiences tensile forces. This biomechanical reality dictates the placement of internal fixation; tension band constructs or tension-side plating is generally preferred on the lateral side, whereas buttress plating is mandatory on the posteromedial aspect to prevent varus collapse. The fibula, while bearing less axial load, acts as a critical lateral buttress. Disruption of the proximal tibiofibular joint or the distal syndesmosis profoundly alters the contact mechanics of the knee and ankle, respectively, accelerating post-traumatic arthrosis if not anatomically restored.
Exhaustive Indications and Contraindications
The selection of a surgical approach to the tibia and fibula is dictated by a meticulous analysis of the fracture morphology, the integrity of the soft tissue envelope, and the physiological status of the patient. The anterolateral approach to the lateral tibial plateau is the undisputed workhorse for proximal tibial fractures. It provides excellent exposure for the open reduction and internal fixation of Schatzker Type I, II, and III fractures. Furthermore, it is heavily utilized for bone grafting procedures in the setting of delayed union or nonunion, the radical debridement of osteomyelitis, and the en bloc excision or biopsy of osseous neoplasms.
The posteromedial approach is specifically indicated for the visualization and buttress plating of the posteromedial shear fragment, a hallmark of high-energy Schatzker Type IV, V, and VI fractures. Accurate reduction of this fragment is paramount, as failure to do so inevitably leads to catastrophic varus collapse of the knee joint. The posterolateral and direct posterior approaches are reserved for highly specific fracture patterns involving the posterior column of the tibial plateau, where anterior approaches fail to provide adequate visualization or permit orthogonal hardware placement. Approaches to the tibial shaft are generally divided into the anterior approach, utilized for open plating or intramedullary nailing, and the posterolateral approach, which is an invaluable limb-salvage corridor used primarily for bone grafting of recalcitrant nonunions when the anterior skin is severely compromised.
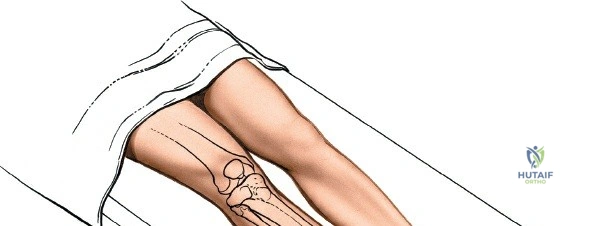
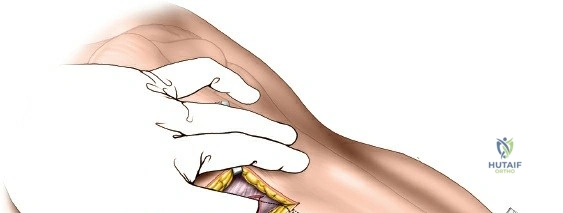
Contraindications to these approaches are primarily governed by the state of the soft tissues. Acute, high-energy trauma frequently results in massive edema, hemorrhagic fracture blisters, and incipient compartment syndrome. Incising through compromised, blistering skin is an absolute contraindication, as it exponentially increases the risk of wound necrosis and deep osseous infection. In such scenarios, a damage-control orthopedic strategy—spanning external fixation, elevation, and delayed definitive fixation—is mandatory. Surgery must be postponed until the soft tissue envelope demonstrates clear signs of recovery, typically indicated by the appearance of skin wrinkles (the "wrinkle sign") and the re-epithelialization of fracture blisters.
Relative contraindications include severe peripheral vascular disease, uncontrolled diabetes mellitus, and active local soft tissue infections. In patients with profound vasculopathy, extensive periosteal stripping during open approaches can devascularize the bone fragments, leading to atrophic nonunion. In these high-risk cohorts, minimally invasive percutaneous osteosynthesis (MIPO) or definitive management with circular external fixation (Ilizarov or Taylor Spatial Frame) may be the preferred, safer alternative.
| Approach | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Anterolateral (Plateau) | Schatzker I-III, Lateral column access, Tumor biopsy | Anterior skin blistering/necrosis, Active local infection | Severe peripheral vascular disease |
| Posteromedial (Plateau) | Schatzker IV-VI, Posteromedial shear fragments | Posterior soft tissue compromise, DVT in popliteal vein | Morbid obesity (positioning difficulty) |
| Posterolateral (Shaft) | Tibial nonunion, Anterior skin breakdown (limb salvage) | Normal anterior skin (unnecessary complexity) | Prior extensive lateral compartment trauma |
| Direct Posterior | Posterior column plateau fractures, Avulsion fractures | Popliteal artery injury requiring anterior access | Inexperience with popliteal neurovascular anatomy |
| MIPO (Distal Tibia) | Multifragmentary distal metaphyseal fractures | Need for absolute anatomical reduction of articular block | Severe osteoporosis (poor screw purchase) |
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning is the intellectual foundation of successful orthopedic trauma surgery. Standard orthogonal radiographs (anteroposterior and lateral) provide a baseline understanding of the fracture pattern. However, for complex tibial plateau and pilon fractures, high-resolution computed tomography (CT) with two-dimensional multiplanar reconstructions and three-dimensional surface rendering is absolute dogma. The CT scan allows the surgeon to map the fracture lines, identify the location of major articular depression, and delineate the presence of coronal plane fracture lines that dictate the necessity of posterior approaches.
Digital templating software must be utilized to select the optimal implant size, contour, and screw trajectory. The surgeon must anticipate the sequence of reduction, planning the placement of Schanz pins for joystick manipulation, the application of articulating tension devices, and the strategic positioning of independent lag screws prior to the application of the neutralization or buttress plate. In cases of significant metaphyseal comminution, the surgeon must plan for the harvest of autologous bone graft (typically from the iliac crest) or the availability of allograft/orthobiologics to fill metaphyseal voids and support the elevated articular surface.
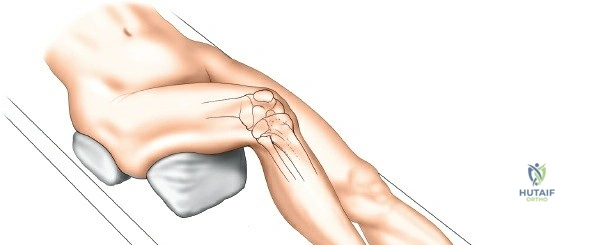
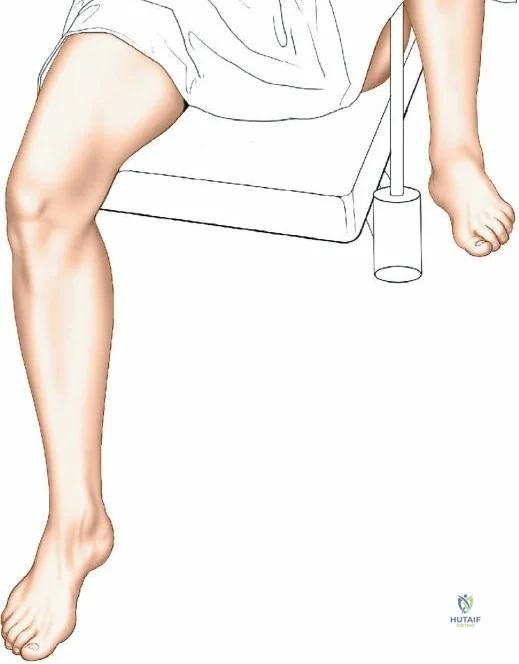
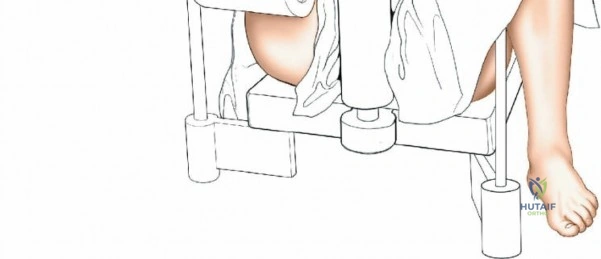
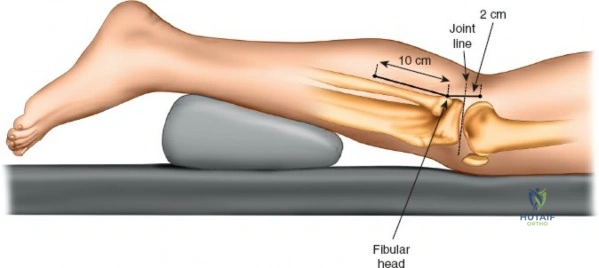
Patient positioning is a critical step that directly influences surgical exposure and ease of reduction. For the anterolateral approach to the tibial plateau and anterior approaches to the shaft, the patient is positioned supine on a fully radiolucent table. A firm, sterile-draped bump is placed beneath the ipsilateral hip to correct the natural external rotation of the lower extremity, ensuring the patella points directly toward the ceiling. A sterile triangle or a firm wedge is placed beneath the knee to maintain approximately 60 degrees of flexion. This flexion relaxes the gastrocnemius muscle, neutralizing its deforming force on the proximal tibia, and allows for dynamic manipulation of the joint during reduction.
For the posteromedial, posterolateral, and direct posterior approaches, the patient is typically placed in the prone position or the "floppy lateral" decubitus position. Prone positioning requires meticulous padding of all bony prominences, particularly the face, chest, and bilateral iliac crests, to prevent pressure necrosis. The arms are positioned on arm boards in less than 90 degrees of abduction to protect the brachial plexus. A pneumatic tourniquet is applied to the proximal thigh. Prior to inflation, the limb is exsanguinated by elevation for 3 to 5 minutes or by the tight application of an Esmarch bandage, ensuring a bloodless surgical field, which is critical for identifying the delicate articular margins and neurovascular structures.


Step-by-Step Surgical Approach and Fixation Technique
The Anterolateral Approach to the Lateral Tibial Plateau
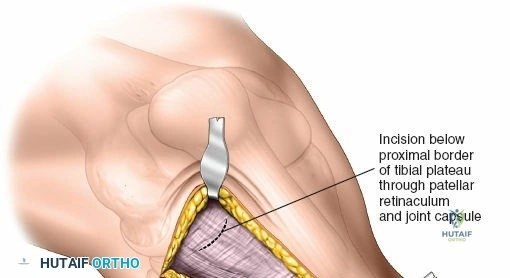
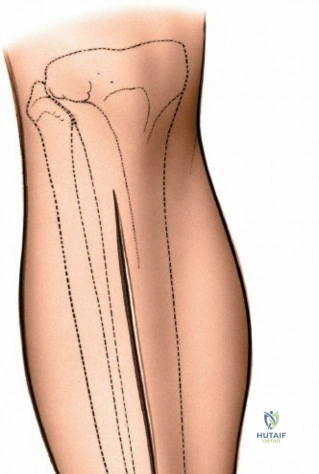
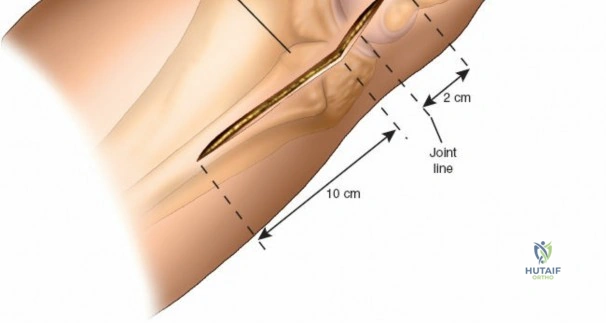
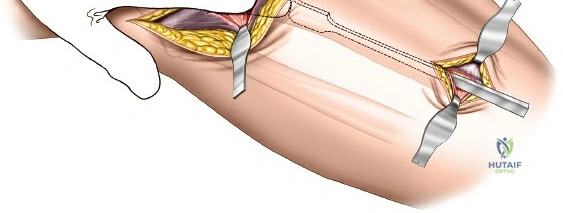
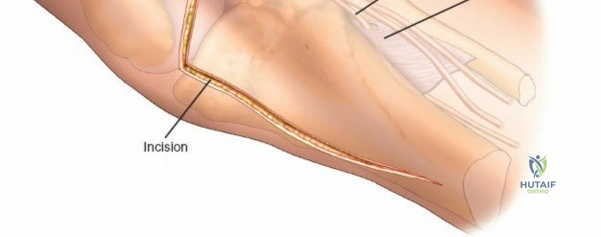
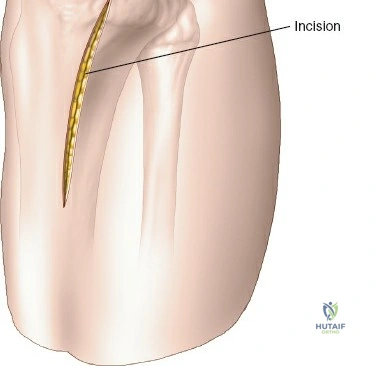
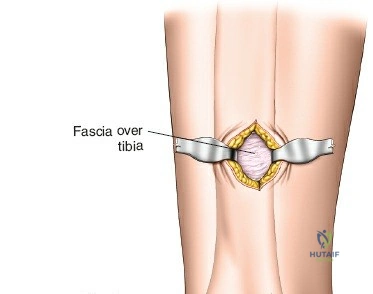
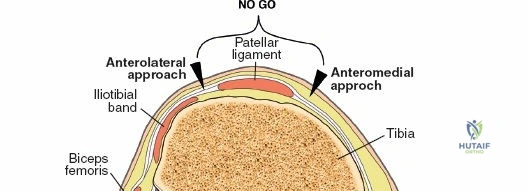
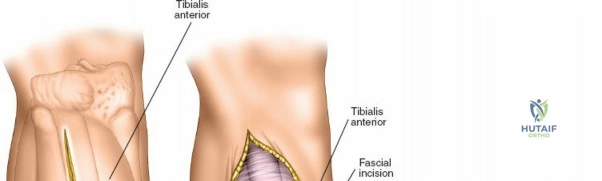
The anterolateral approach begins with the identification of key osseous landmarks: the anterior border of the tibial shaft, the lateral joint line, and Gerdy’s tubercle. An inverted L-shaped or gently curved "hockey stick" incision is utilized. The incision starts 2 to 3 cm proximal to the joint line, lateral to the patellar tendon, curves anteriorly over Gerdy’s tubercle, and extends distally parallel to, and approximately 1 cm lateral to, the anterior tibial crest. The deep fascial incision mirrors the skin incision. The dissection is strictly epiperiosteal; there is no true internervous plane, as the entire exposure lies within the territory of the deep peroneal nerve, which remains protected within the anterior compartment musculature.
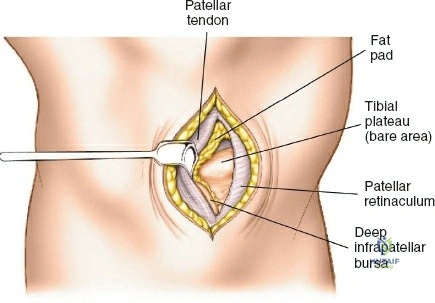
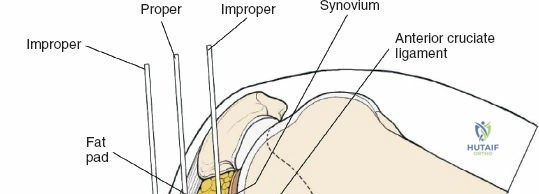
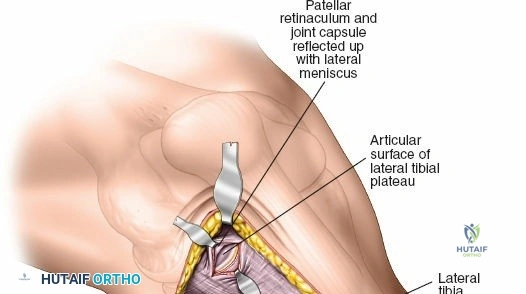
Superficial dissection involves elevating full-thickness fasciocutaneous flaps to preserve the subdermal vascular plexus. The knee joint capsule is incised transversely just inferior to the lateral meniscus. Meticulous care must be taken to avoid inadvertently transecting the meniscus. Deep dissection requires a submeniscal arthrotomy. The coronary ligaments anchoring the lateral meniscus to the tibia are sharply divided. The meniscus is elevated superiorly, and 1-0 PDS or Vicryl stay sutures are placed along its periphery. Upward traction on these sutures provides unparalleled visualization of the lateral articular surface. The anterior horn of the meniscus must remain firmly attached to prevent catastrophic destabilization of the meniscal root.
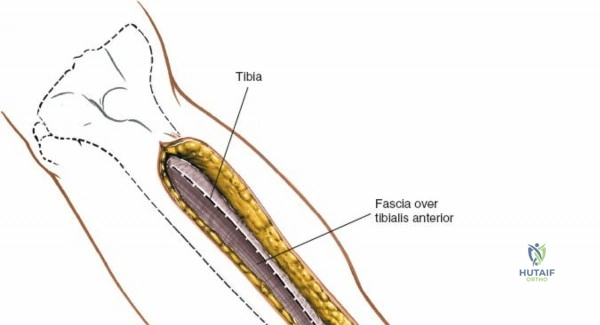
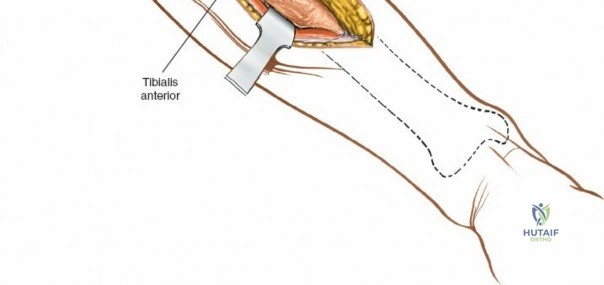
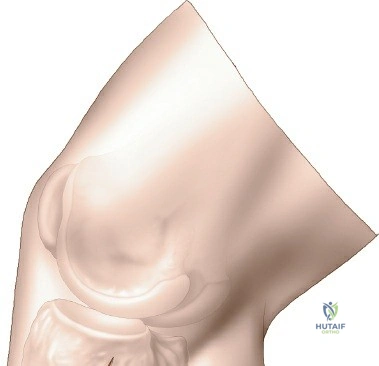
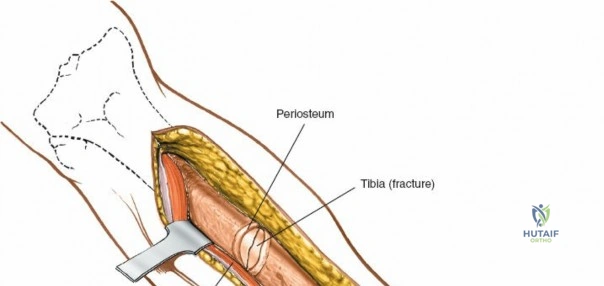
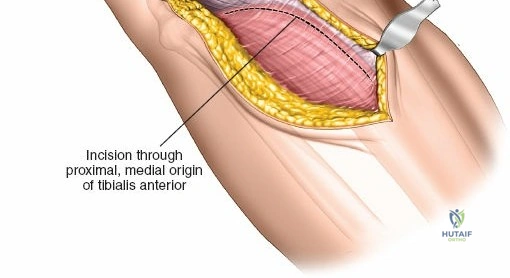
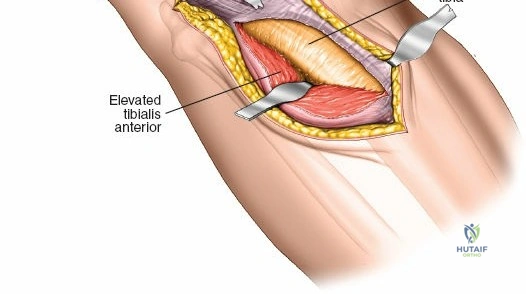
To expose the lateral metaphysis, the origin of the tibialis anterior muscle is sharply elevated from the proximal tibia using a Cobb elevator. The surgeon must work strictly within the plane between the periosteum and the muscle belly to minimize bleeding and protect the anterior tibial recurrent artery. If additional exposure is required, a femoral distractor can be applied with pins in the lateral femoral condyle and the distal tibial diaphysis. Applying varus stress and distraction opens the lateral compartment, allowing the surgeon to elevate depressed articular fragments using bone tamps, fill the resulting void with structural graft, and apply a lateral locking plate.
The Posteromedial Approach to the Proximal Tibia
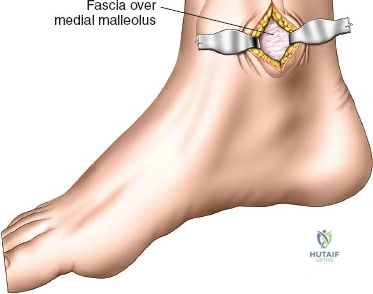
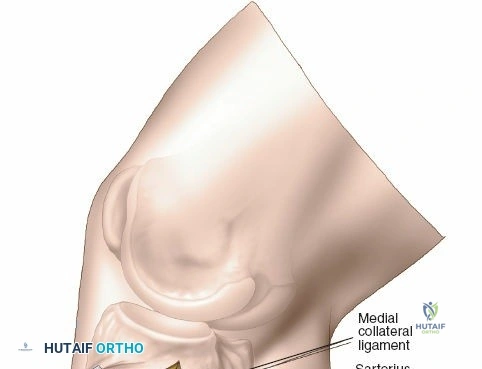
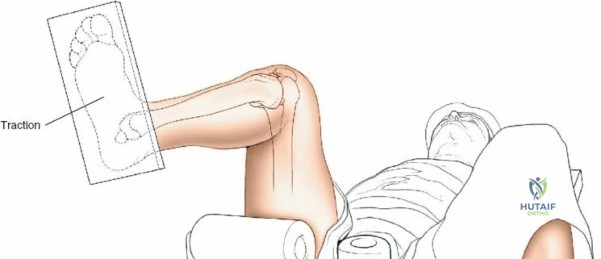
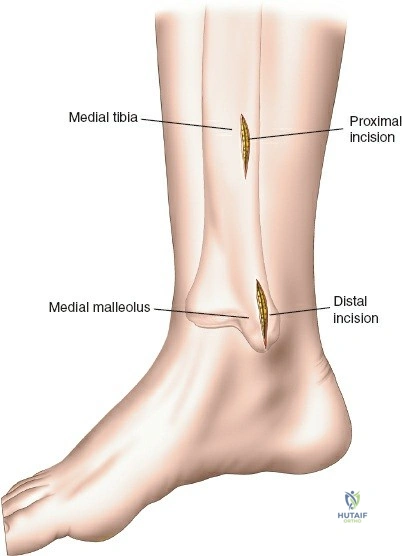
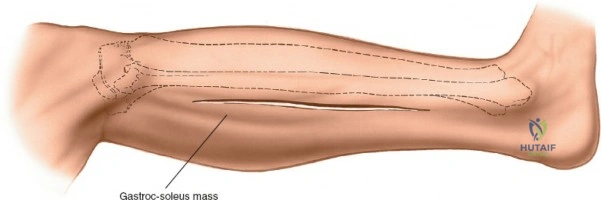
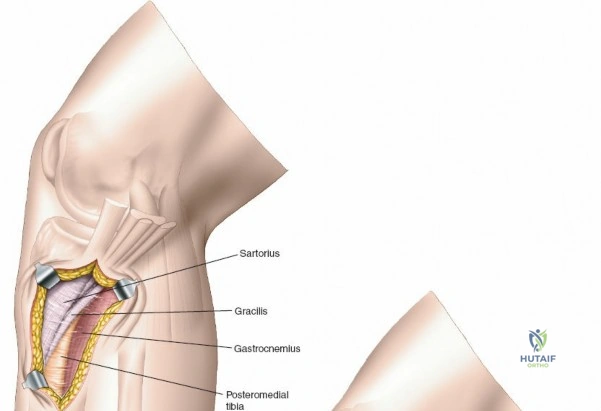
The posteromedial approach is essential for stabilizing the posteromedial shear fragment. The patient is typically positioned prone or supine with the leg externally rotated (figure-of-four position). A longitudinal incision is made along the posteromedial border of the proximal tibia, starting at the level of the joint line and extending distally. The great saphenous vein and the saphenous nerve lie in the superficial subcutaneous tissues and must be identified, mobilized, and protected throughout the procedure.
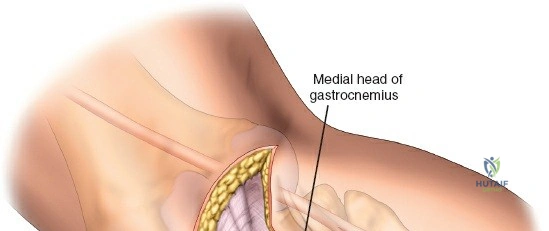
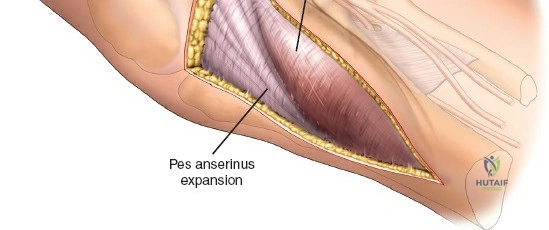
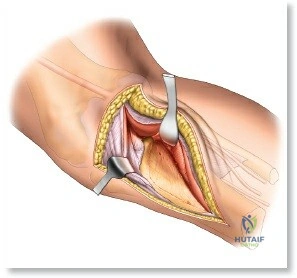
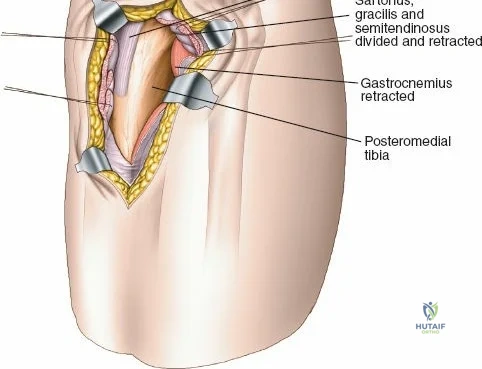
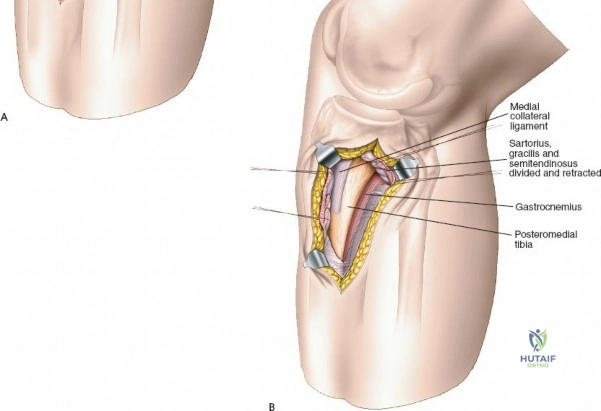
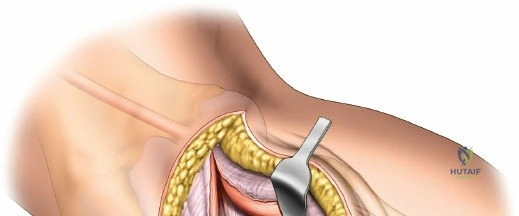
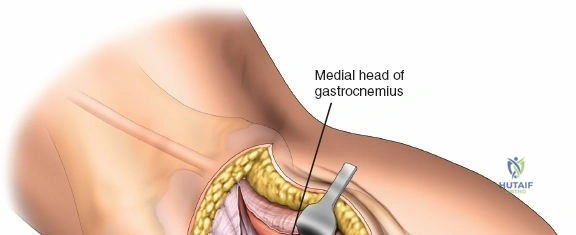
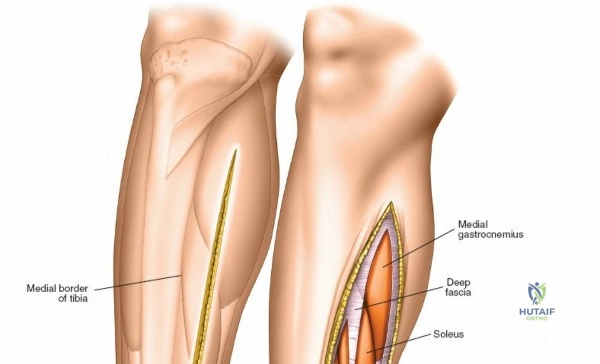
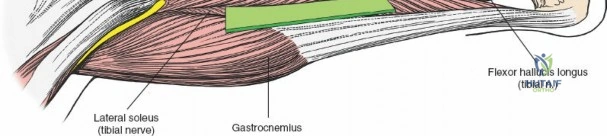
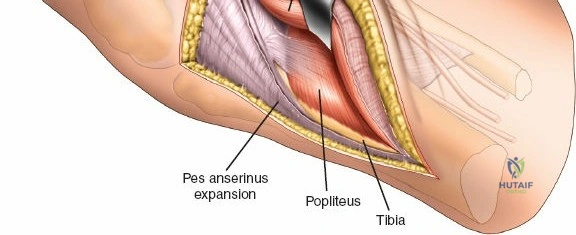
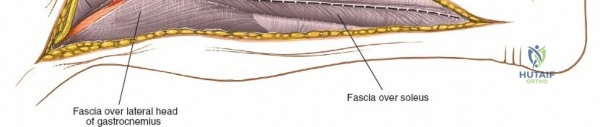
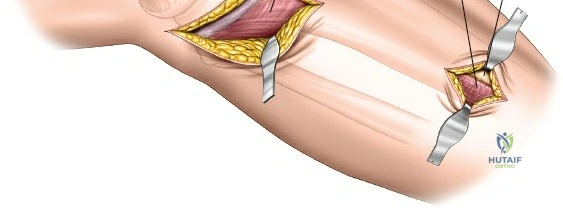
The deep fascial incision is made in line with the skin incision. The surgeon identifies the interval between the medial head of the gastrocnemius muscle posteriorly and the pes anserinus (sartorius, gracilis, semitendinosus) anteriorly. The medial head of the gastrocnemius is bluntly retracted laterally and posteriorly. This maneuver protects the popliteal neurovascular bundle, which lies deep and lateral to the muscle belly. The pes anserinus is retracted anteriorly.
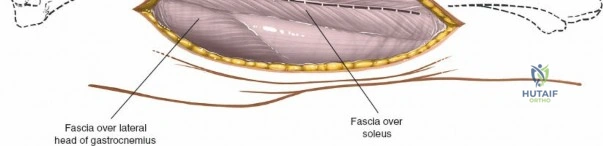
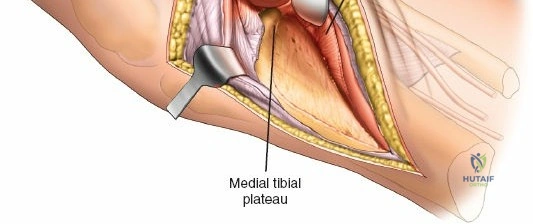
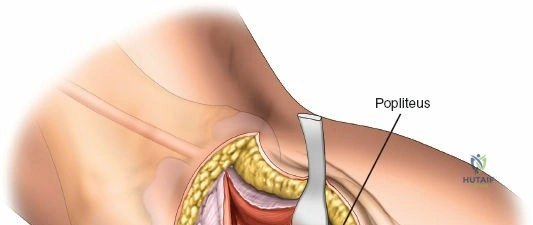
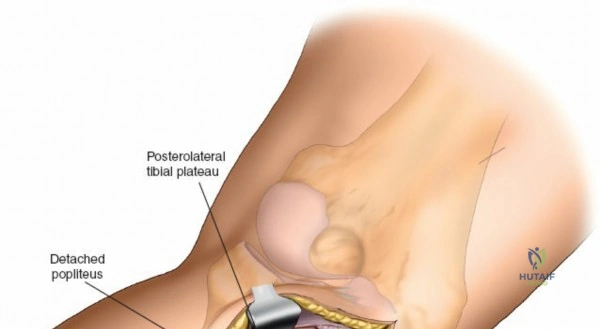
Deep dissection exposes the popliteus muscle and the fascia covering the soleus. The popliteus may need to be partially elevated or split to gain full access to the posteromedial articular fragment. Once the fracture is visualized, it is anatomically reduced using pointed reduction forceps. A pre-contoured posteromedial buttress plate (often an anti-glide plate) is applied to the apex of the fracture. Because this plate sits on the compression side of the mechanical axis, it effectively neutralizes the vertical shear forces that would otherwise lead to varus collapse.
The Posterolateral and Direct Posterior Approaches
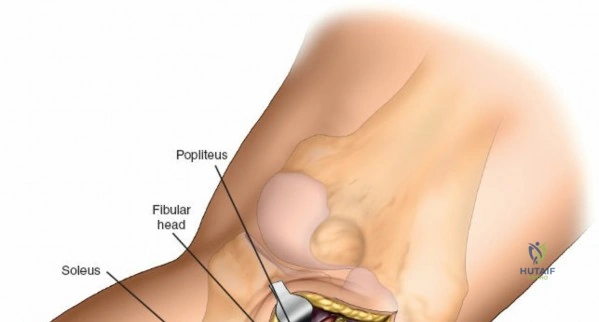
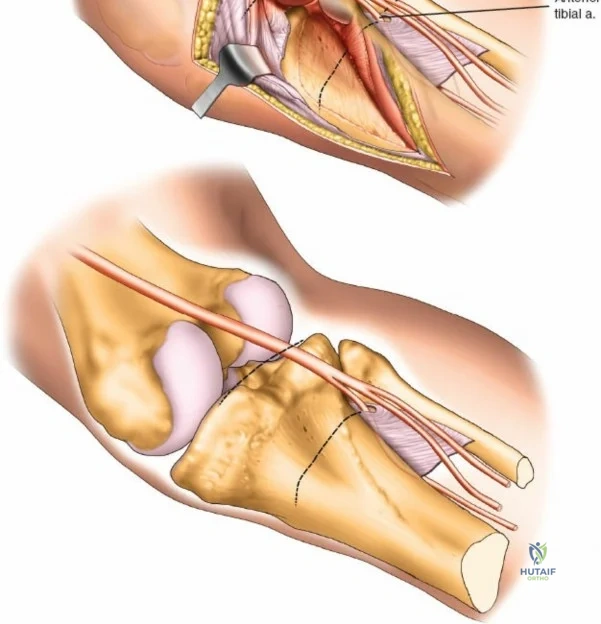
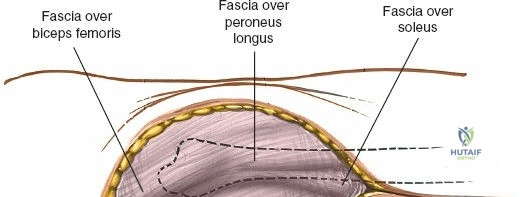
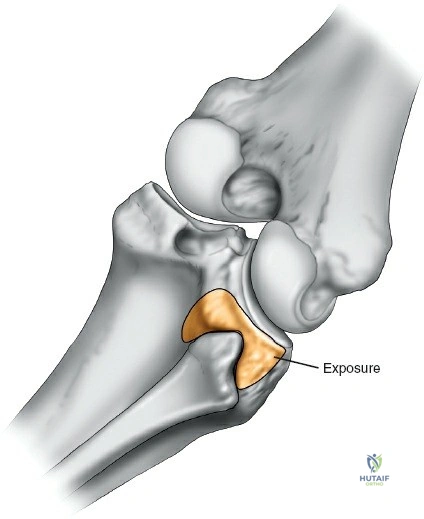
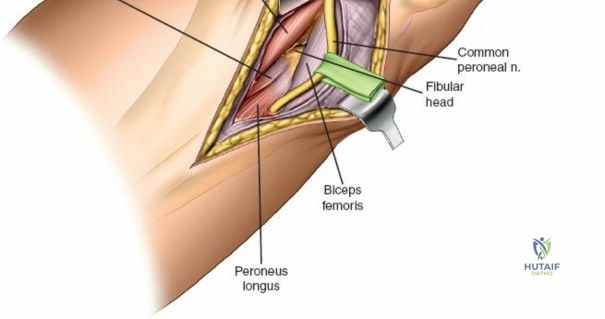
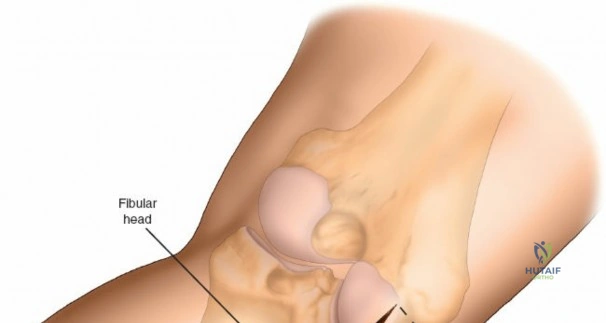
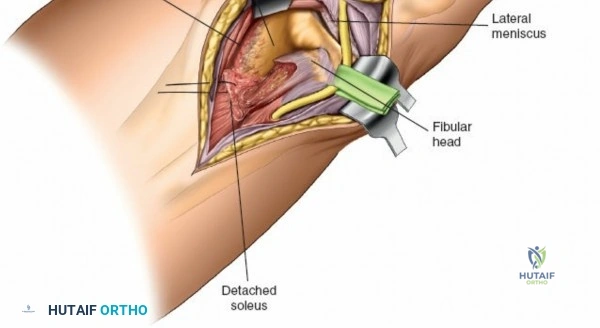
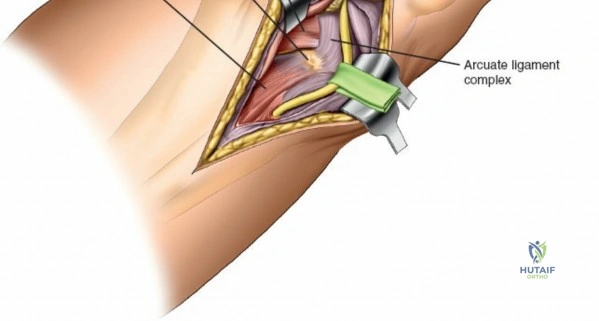
Accessing the posterolateral corner of the tibial plateau is technically demanding due to the presence of the fibular head, the lateral collateral ligament (LCL), and the common peroneal nerve. The traditional posterolateral approach requires a fibular neck osteotomy or the mobilization of the LCL and biceps femoris. The common peroneal nerve must be neurolysed and protected with a vessel loop. Once the fibular head is reflected superiorly, the posterolateral joint capsule is incised, granting access to the posterior aspect of the lateral plateau. Following fixation, the fibular osteotomy must be rigidly repaired with a lag screw or tension band wiring.
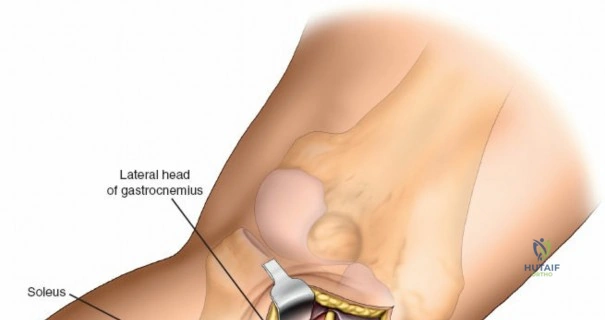
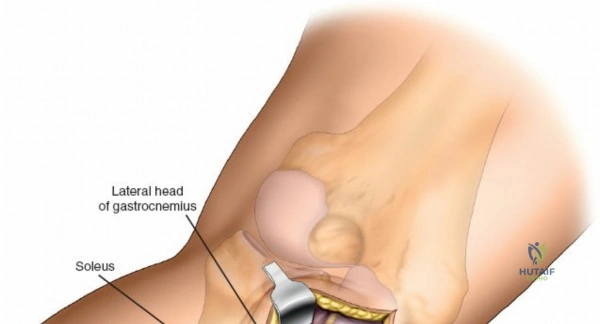
The direct posterior approach (Lobenhoffer approach) is utilized for isolated posterior shear fractures or avulsions of the posterior cruciate ligament (PCL). With the patient prone, an S-shaped incision is made across the popliteal fossa. The lesser saphenous vein and sural nerve are identified and protected. The deep fascia is incised, and the interval between the medial and lateral heads of the gastrocnemius is developed.
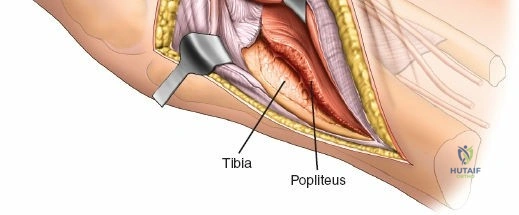
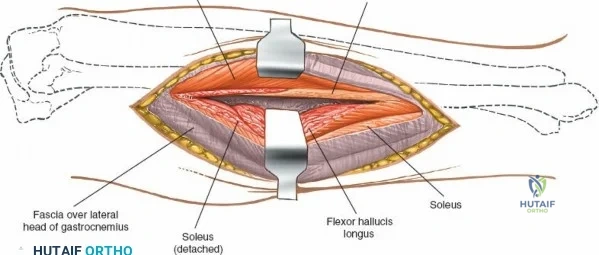
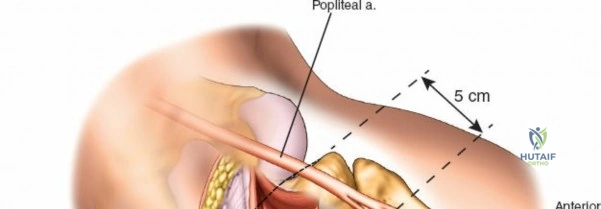
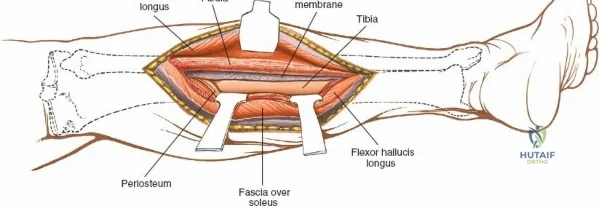
The popliteal neurovascular bundle (popliteal artery, popliteal vein, and tibial nerve) is the most critical structure in this field. It is carefully mobilized and retracted laterally. The soleus and popliteus muscles are elevated from the posterior surface of the tibia, exposing the posterior capsule and the bony posterior column. Fixation is typically achieved with small fragment T-plates or posterior buttress plates. Meticulous hemostasis is mandatory prior to closure to prevent the formation of a tension hematoma in the popliteal fossa.