Pelvis & Acetabulum Approaches: Unlocking the Posterior Superior Iliac
Key Takeaway
In this comprehensive guide, we discuss everything you need to know about Pelvis & Acetabulum Approaches: Unlocking the Posterior Superior Iliac. Surgical approaches to the pelvis and acetabulum are performed for bone grafting or fracture reconstruction. For instance, the **posterior superior iliac** crest approach is commonly used for bone graft harvest. Other complex methods, such as the ilioinguinal approach, access the anterior acetabulum, while posterior approaches target the posterior column. Each procedure requires precise anatomical assessment to suit specific pathologies.
Comprehensive Introduction and Patho-Epidemiology
The surgical management of the pelvis and acetabulum represents one of the most formidable challenges in modern orthopedic trauma and reconstructive surgery. The pelvis is a highly complex, tri-dimensional bony ring structurally reinforced by a dense network of interconnecting ligaments. It is composed of the two innominate bones, which articulate anteriorly at the pubic symphysis and posteriorly with the sacrum via the sacroiliac (SI) joints. This robust architecture is designed for axial load transmission from the spine to the lower extremities; consequently, disruption of this ring usually implies the transfer of massive kinetic energy.
Epidemiologically, pelvic ring and acetabular fractures follow a bimodal distribution. High-energy mechanisms, such as motor vehicle collisions or falls from significant heights, predominantly affect younger patients and are frequently associated with polytrauma, hemodynamic instability, and visceral injuries. Conversely, low-energy falls in the geriatric population, compounded by osteopenia or osteoporosis, result in fragility fractures of the pelvis (FFP) that present unique fixation challenges due to poor bone stock.
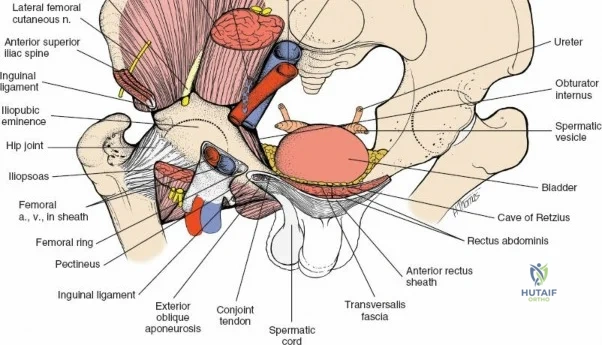
Approaches to the pelvis and acetabulum are inherently complex, demanding profound anatomical knowledge. The intra-abdominal and intrapelvic contents—including the lumbosacral plexus, major vascular axes (iliac vessels), and urogenital structures—make surgical exposure hazardous. However, the presence of large subcutaneous bony landmarks, particularly the anterior and posterior superior iliac spines and the iliac crest, provides strategic, safe corridors for surgical access. Unlocking these anatomical gateways is critical not only for the open reduction and internal fixation (ORIF) of pelvic and acetabular fractures but also for the harvest of high-quality autologous bone graft, which remains the gold standard for skeletal reconstruction and spinal arthrodesis.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of pelvic osteology, ligamentous restraints, and regional neurovascular anatomy is non-negotiable for the orthopedic surgeon. The innominate bone is formed by the confluence of the ilium, ischium, and pubis, which meet at the triradiate cartilage within the acetabulum.
Osteology and Columnar Biomechanics
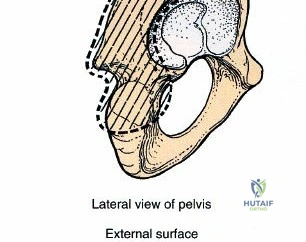
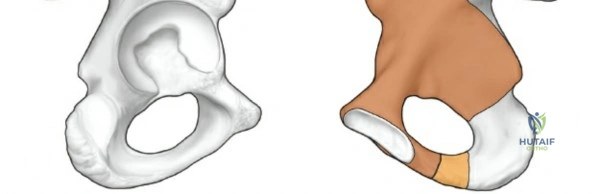
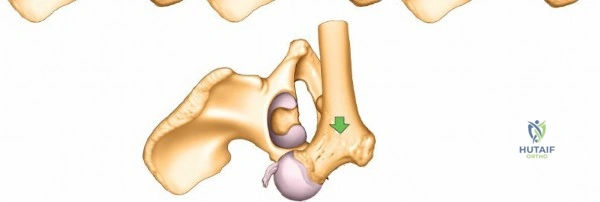
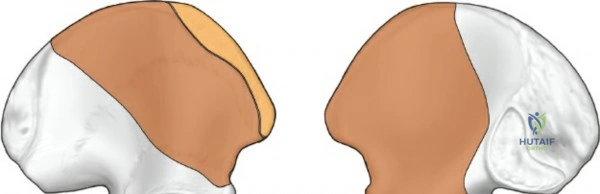
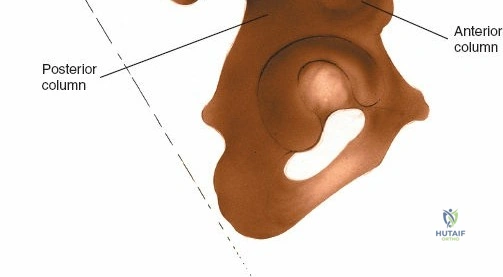
The acetabulum is best conceptualized biomechanically through the Letournel and Judet two-column theory.
1. The Anterior Column extends from the anterior iliac wing down to the pubic symphysis, encompassing the anterior half of the acetabulum.
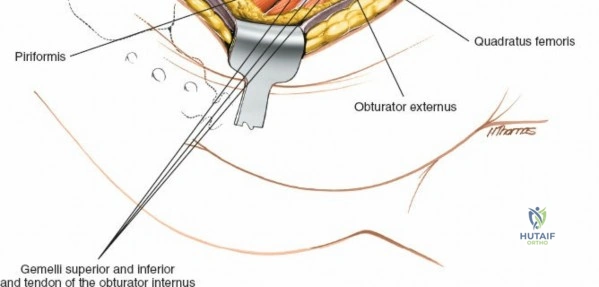
2. The Posterior Column is a massive, dense strut of bone extending from the dense bone of the sciatic notch down to the ischial tuberosity, containing the posterior half of the acetabulum.
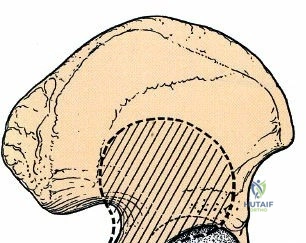
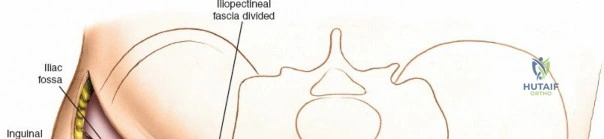
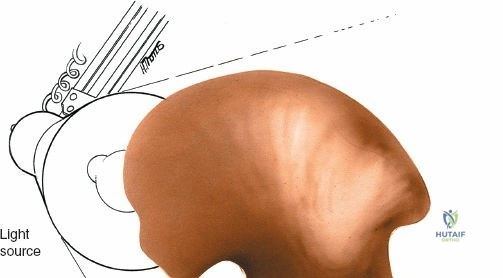
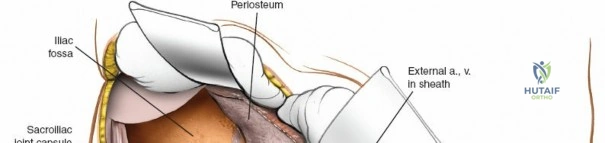
To truly appreciate the anatomy of these columns, one must examine a hemipelvis against a light source; the massive anterior and posterior columns stand in stark contrast to the translucent, thin central area of the iliac wing (the iliac fossa). This central thinning dictates where hardware can be safely placed and where bone graft can be harvested without causing iatrogenic cortical breaches.
Muscular and Internervous Planes
The iliac crest serves as a massive aponeurotic and muscular attachment site.
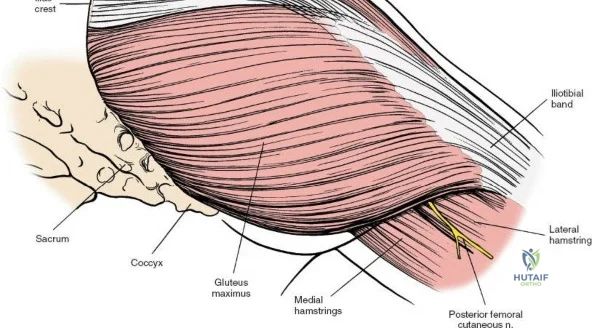
* Outer Table: Gives origin to the gluteal musculature (gluteus maximus, medius, and minimus) and the tensor fasciae latae (TFL). These are innervated by the superior and inferior gluteal nerves.
* Inner Table: Gives origin to the iliacus muscle, innervated by the femoral nerve.
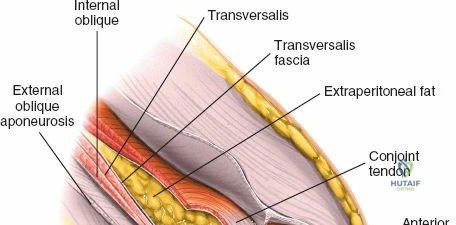
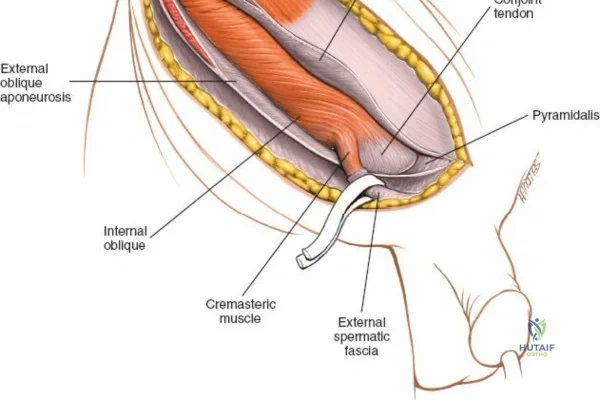
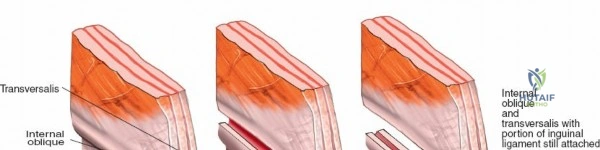
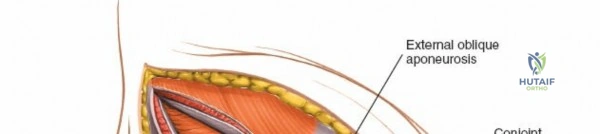
* Superior Crest: Serves as the insertion site for the abdominal wall musculature (external oblique, internal oblique, transversus abdominis), which are segmentally innervated.
Because muscles originate from or insert onto the crest but do not cross it, the crest itself represents a true internervous and intermuscular plane, allowing safe subperiosteal dissection.
Critical Neurovascular Structures
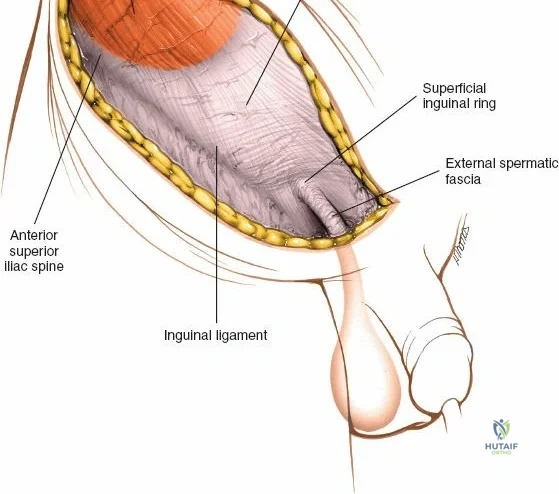
When approaching the anterior iliac crest, the Lateral Femoral Cutaneous Nerve (LFCN) is at significant risk. It typically exits the pelvis medial to the Anterior Superior Iliac Spine (ASIS) under the inguinal ligament, but anatomical variants exist where it crosses directly over the ASIS or through the sartorius origin.
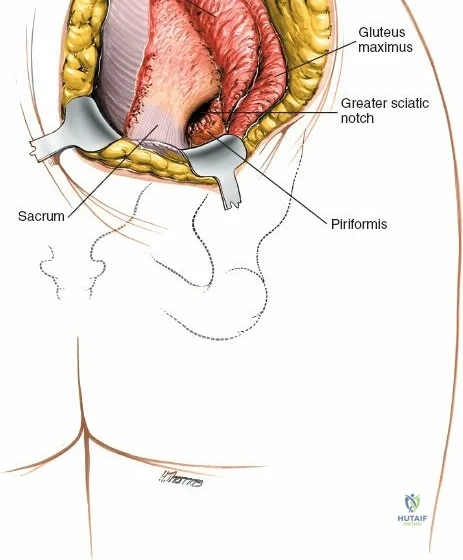
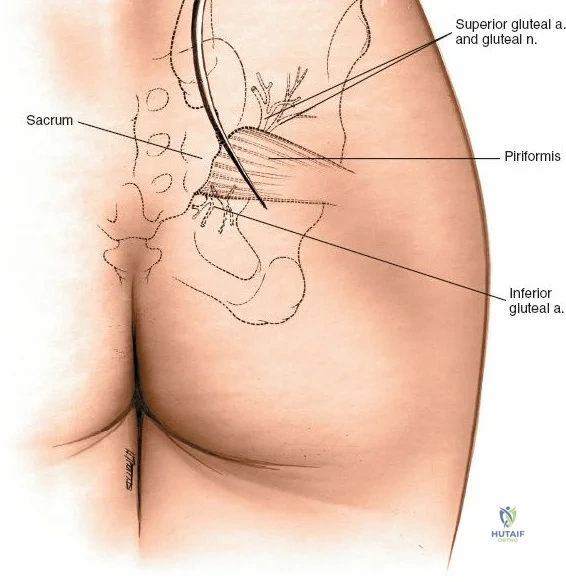
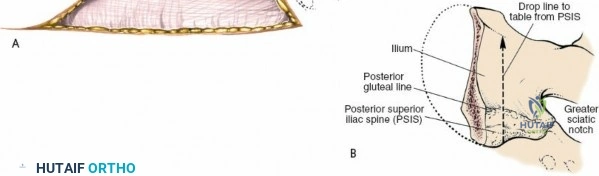
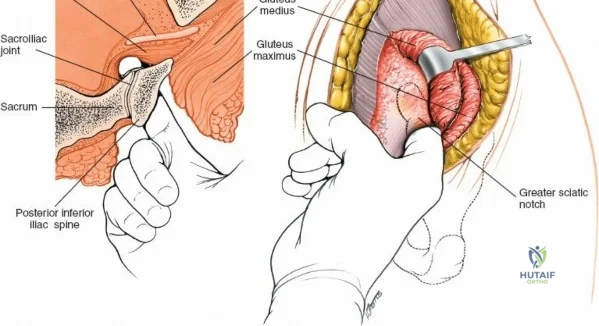
During posterior approaches to the ilium and sacroiliac joint, the Superior Cluneal Nerves (sensory branches from L1-L3 dorsal rami) cross the posterior iliac crest approximately 7 to 8 cm lateral to the Posterior Superior Iliac Spine (PSIS). Iatrogenic injury to these nerves can result in painful postoperative neuromas. Furthermore, the Superior Gluteal Artery exits the greater sciatic notch precisely at the inferior margin of the posterior sacroiliac joint, making it highly vulnerable during posterior pelvic ring exposures or errant retractor placement.
Exhaustive Indications and Contraindications
The decision to execute an approach to the pelvis or acetabulum must be carefully weighed against the patient's physiologic status and local tissue conditions. Below is a comprehensive breakdown of indications and contraindications.
| Surgical Approach / Procedure | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Anterior Iliac Crest Bone Graft | Non-unions, maxillofacial reconstruction, anterior cervical/lumbar fusion, structural pelvic defects. | Localized soft tissue infection, prior radiation therapy to the pelvis. | Severe osteoporosis, prior harvest from the same site, systemic coagulopathy. |
| Posterior Iliac Crest Bone Graft | Posterior spinal fusions (scoliosis, degenerative), massive structural graft requirements. | Overlying decubitus ulcers, local soft tissue infection (e.g., pilonidal cyst). | Prior extensive posterior pelvic ring trauma, severe malnutrition. |
| Ilioinguinal Approach | Anterior column/wall fractures, transverse fractures, anterior column with posterior hemitransverse. | Hemodynamic instability (damage control phase), unresuscitated patient. | Previous abdominal/pelvic radiation, presence of a colostomy in the surgical field. |
| Kocher-Langenbeck (Posterior) | Posterior column/wall fractures, certain transverse or T-type fractures with posterior displacement. | Unstable pelvic ring requiring anterior fixation first, severe Morel-Lavallée lesion. | Prolonged time since injury (>3 weeks) making reduction highly improbable without extensile access. |
Pre-Operative Planning, Templating, and Patient Positioning
Acetabular and pelvic ring surgeries are among the most demanding procedures in orthopedics. Success is predicated entirely on meticulous preoperative planning. There is rarely, if ever, an indication to perform these definitive approaches in an emergency setting; initial management should focus on hemodynamic stabilization (e.g., pelvic binders, external fixation, pre-peritoneal packing, or angioembolization).
Radiographic Evaluation and Templating
Standard radiographic evaluation requires an AP pelvis and the Judet views (Iliac Oblique and Obturator Oblique).
* The Iliac Oblique view profiles the posterior column and anterior wall.
* The Obturator Oblique view profiles the anterior column and posterior wall.
Modern surgical planning mandates thin-cut Computerized Tomography (CT) with 2D multiplanar reformats and 3D surface-rendered reconstructions. The surgeon must mentally or physically reconstruct the fracture using a 3D-printed bone model, which is invaluable for understanding the fracture lines, planning lag screw trajectories, and pre-contouring reconstruction plates.
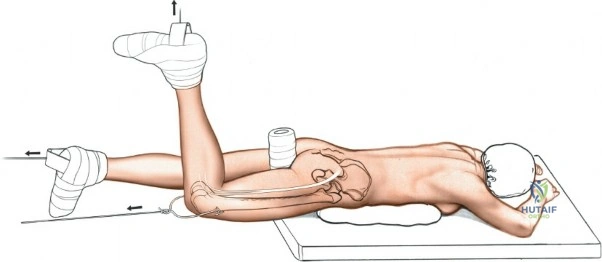
Patient Positioning: Anterior Approaches
For the anterior approach to the iliac crest or the ilioinguinal approach, the patient is placed supine on a radiolucent operating table.
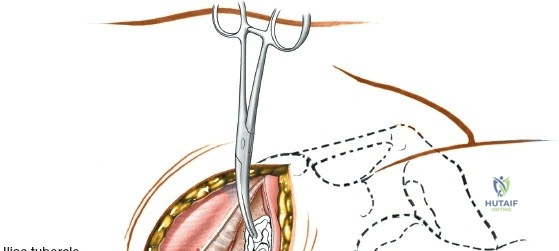
* Place a small sandbag or gel bump under the ipsilateral gluteal (cluneal) region. This elevates the hemipelvis and internally rotates the crest, bringing the iliac tubercle into a more prominent, accessible position.
* The entire ipsilateral lower extremity should be prepped and draped free to allow for intraoperative manipulation, which relaxes the iliopsoas and neurovascular structures during deep dissection.
* A Foley catheter is mandatory to decompress the bladder.
Patient Positioning: Posterior Approaches
For the posterior approach to the iliac crest or the Kocher-Langenbeck approach, the patient is placed prone.
* Utilize a Jackson spinal table or a standard radiolucent table with longitudinal chest and pelvic bolsters. This allows the abdomen to hang free, reducing intra-abdominal pressure and consequently decreasing epidural and pelvic venous bleeding.
* The drapes must be placed distally enough to visualize the gluteal cleft and the PSIS.
* For acetabular procedures, the ipsilateral knee is typically flexed to 90 degrees to relax the sciatic nerve.
Step-by-Step Surgical Approach and Fixation Technique
Because each approach provides access to only a limited sector of the pelvis or acetabulum, the execution must be precise. Tissues in the traumatized pelvis are often contused, and normal fascial planes may be obliterated by hematoma.
Anterior Approach to the Iliac Crest for Bone Graft
Anterior iliac crest bone grafts (AICBG) are the workhorse for autologous bone in orthopedic surgery. The crest provides access to high-quality cortical, cancellous, and corticocancellous bone.
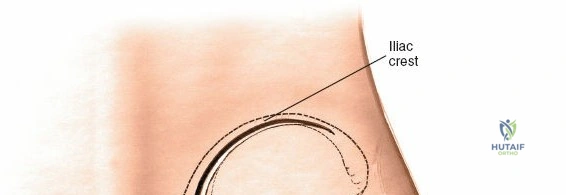
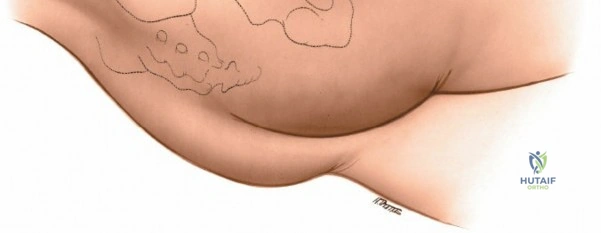
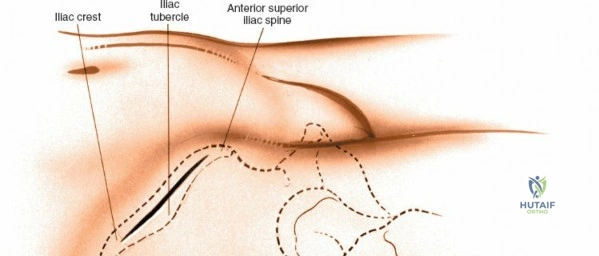
Landmarks and Incision
The subcutaneous ASIS is the primary landmark. Palpate posteriorly along the crest until its widest portion is reached—the iliac tubercle (approximately 5-7 cm posterior to the ASIS). The iliac tubercle marks the metaphyseal equivalent of the ilium, containing the largest volume of cancellous bone.
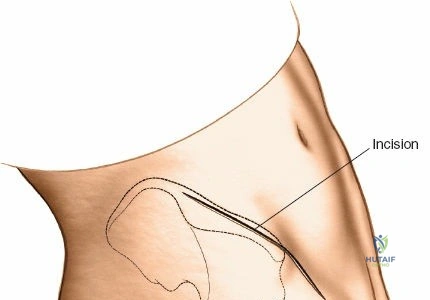
Make an 8-cm curvilinear incision parallel to the iliac crest, centered directly over the iliac tubercle.
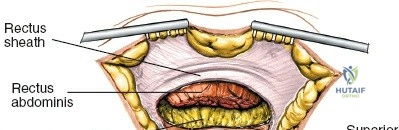
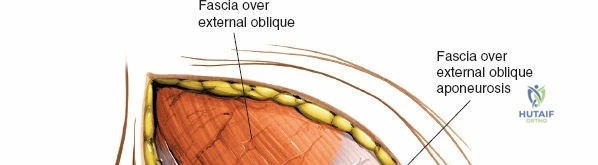
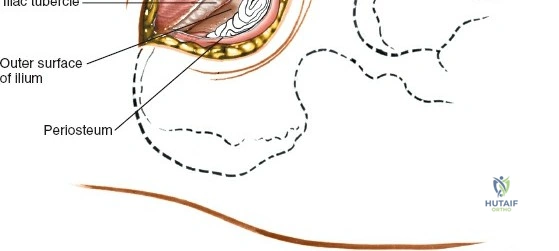
Superficial Surgical Dissection
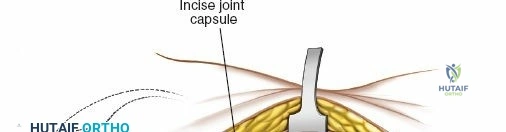
Incise the skin and subcutaneous fat down to the deep fascia overlying the iliac crest. Retract the skin edges to visualize the cartilaginous apophysis (in adolescents) or the dense periosteum of the crest (in adults).
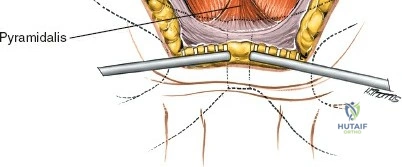
Make a bold, linear incision directly through the periosteum exactly along the midline of the crest. Surgical Pearl: Do not carry the incision anteriorly over the ASIS itself. Detachment of the sartorius or the inguinal ligament origin can result in a devastating postoperative inguinal hernia or LFCN injury.
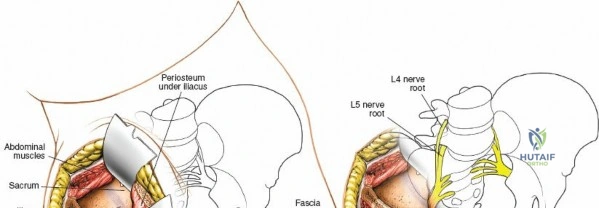
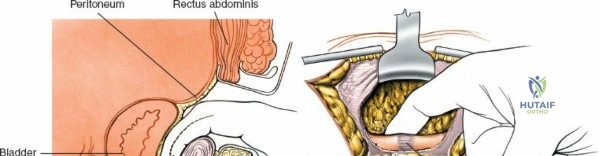
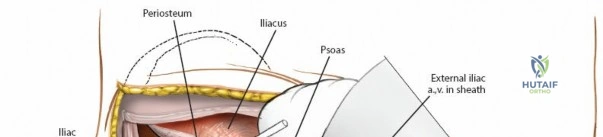
Deep Surgical Dissection
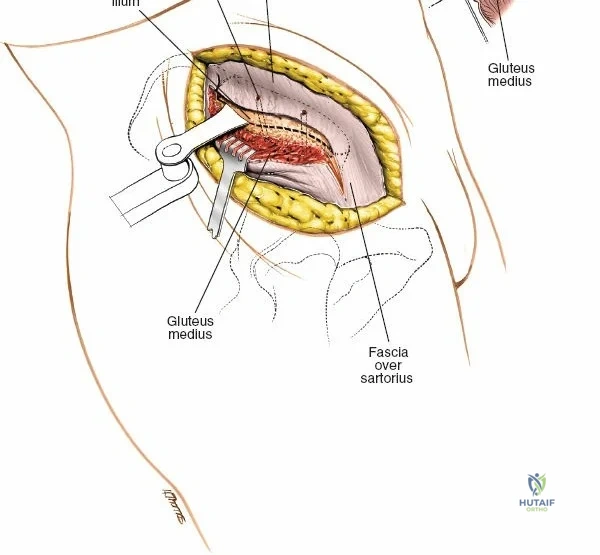
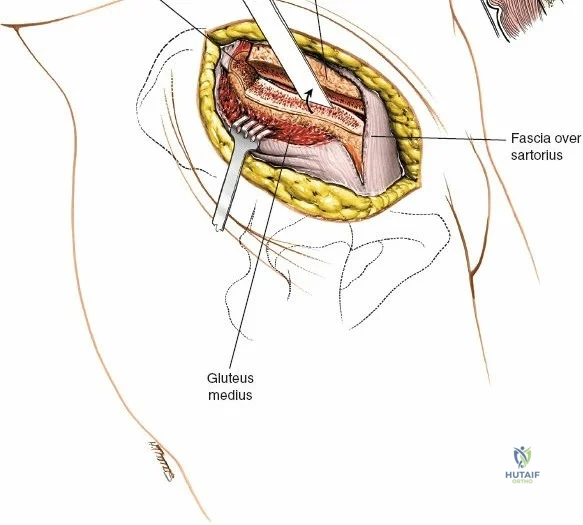
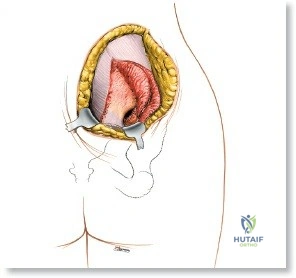
The dissection can proceed along either the inner table (iliacus fossa) or the outer table (gluteal surface).
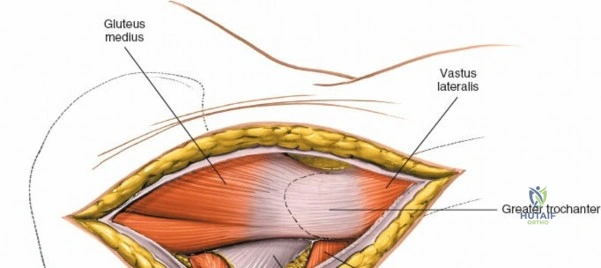
* Outer Table: Using a scalpel, sharply incise the periosteum and reflect the origins of the gluteus medius and minimus. Below the crest, the ilium narrows rapidly. Transition to a broad Cobb elevator to sweep the gluteal musculature inferiorly.
* Inner Table: Reflect the iliacus muscle subperiosteally.
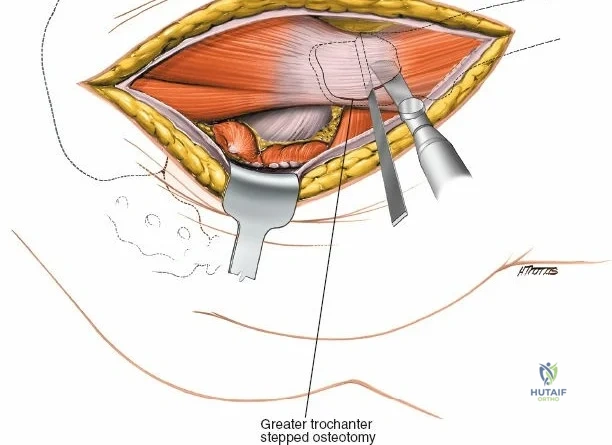
To maintain exposure, pack a laparotomy sponge into the developed interval. The sponge acts as a blunt tissue expander, mitigating bleeding from the nutrient foramina and protecting the muscle bellies from errant osteotome strikes.
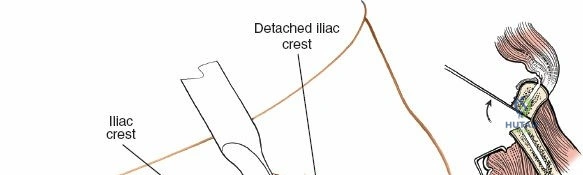
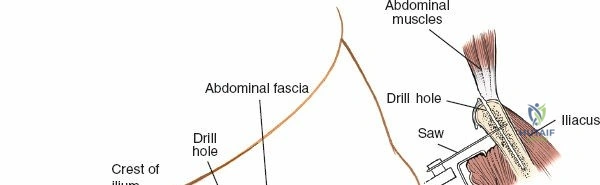
Graft Harvest
For cancellous strips, use a sharp osteotome to elevate a cortical window from the superior crest. Use curettes to harvest the rich cancellous bone from the tubercle region. For structural corticocancellous blocks, use an oscillating saw or sharp osteotomes to outline a block, ensuring the ASIS remains intact.
Closure
Closure is as critical as the approach. The thick fascial layers (gluteal fascia to abdominal fascia) must be meticulously reapproximated with heavy, interrupted absorbable sutures (e.g., #1 Vicryl) to prevent muscle herniation or avulsion.
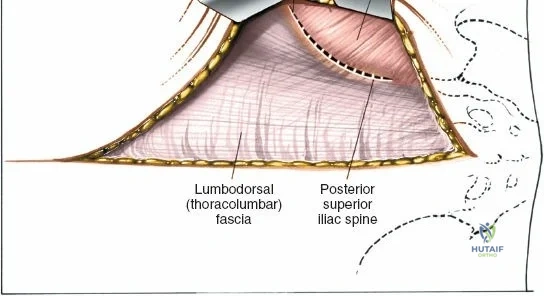
Posterior Approach to the Iliac Crest for Bone Graft
The posterior iliac crest provides a significantly larger volume of bone compared to the anterior crest and is the preferred harvest site for major spinal arthrodesis.
Landmarks and Incision
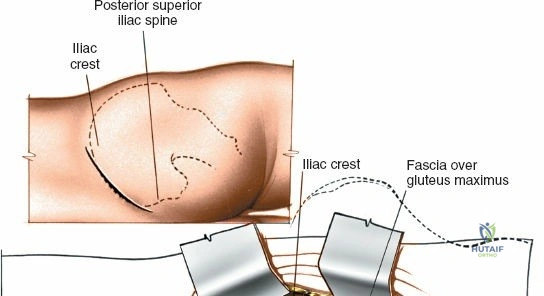
Identify the dimple overlying the PSIS. The subcutaneous posterior crest is easily palpable extending superolaterally from this point. Make an 8-cm oblique incision centered over the PSIS, running parallel to the posterior iliac crest.
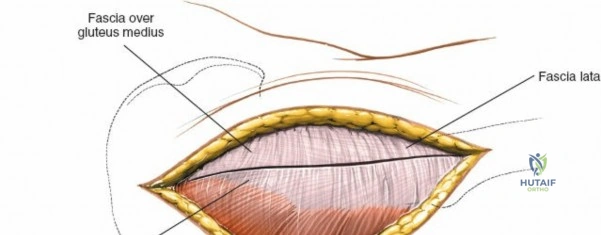
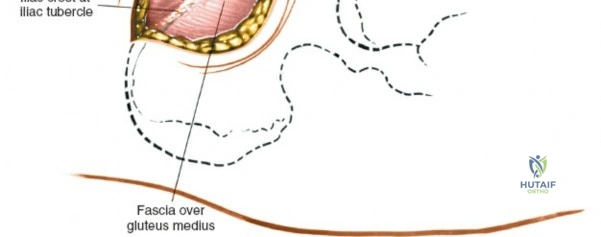
Internervous Plane and Dissection
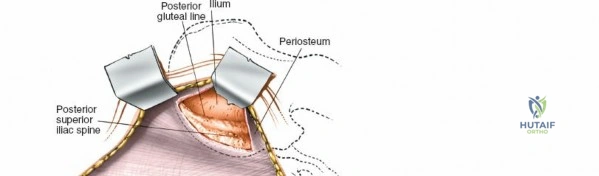
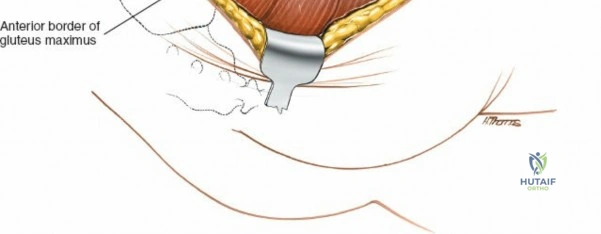
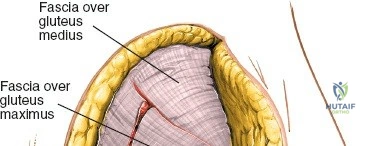
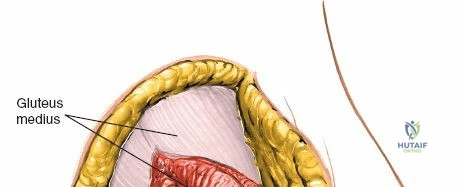
The outer border of the posterior iliac crest is a true internervous plane. The gluteus maximus, medius, and minimus take origin from the outer table (supplied by the gluteal nerves), while the erector spinae and multifidus attach medially (supplied by dorsal rami).
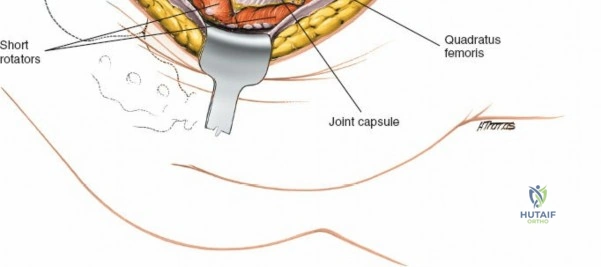
Incise the fascia directly over the crest. Using a Cobb elevator, strip the gluteus maximus subperiosteally from the outer table. The dissection must remain strictly subperiosteal to avoid massive hemorrhage from the superior gluteal artery, which exits the sciatic notch inferiorly.
Harvesting the Posterior Ilium
The bone here is exceptionally thick. A cortical window can be elevated, and large volumes of cancellous bone can be harvested using gouges and curettes. Care must be taken not to breach the sacroiliac joint medially, which could lead to chronic SI joint instability and pain.
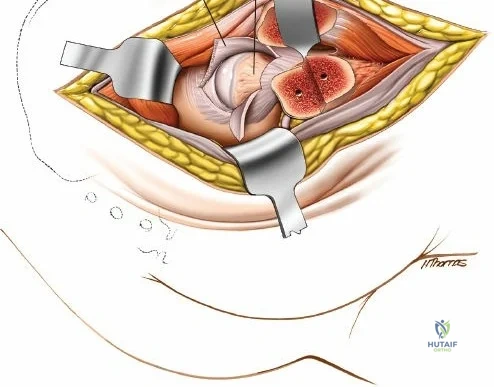
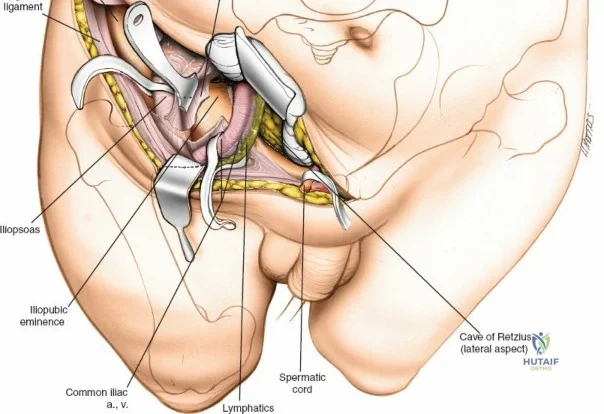
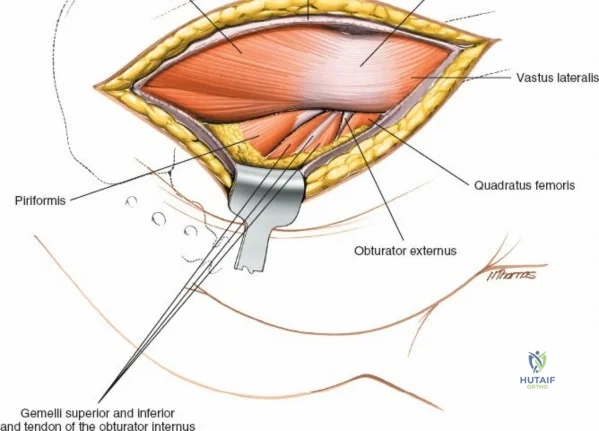
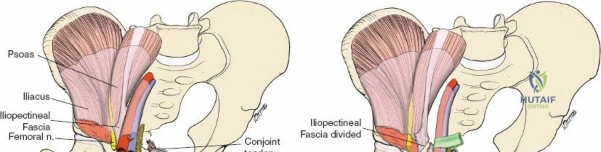
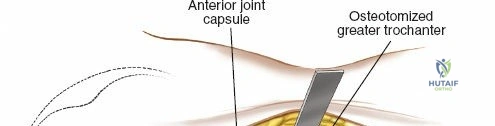
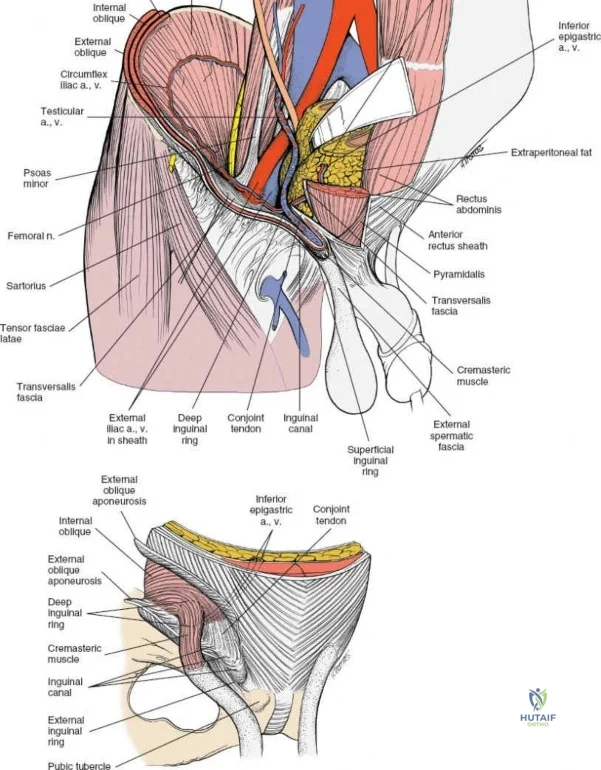
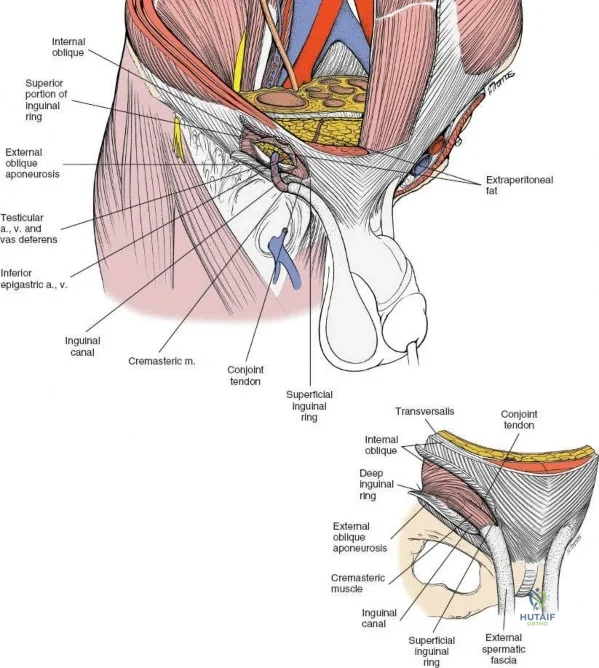
Ilioinguinal Approach to the Acetabulum (Overview)
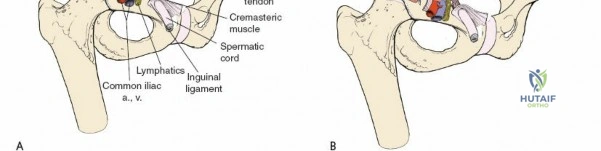
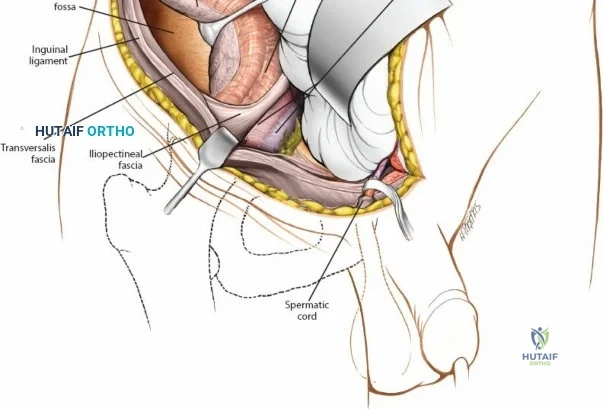
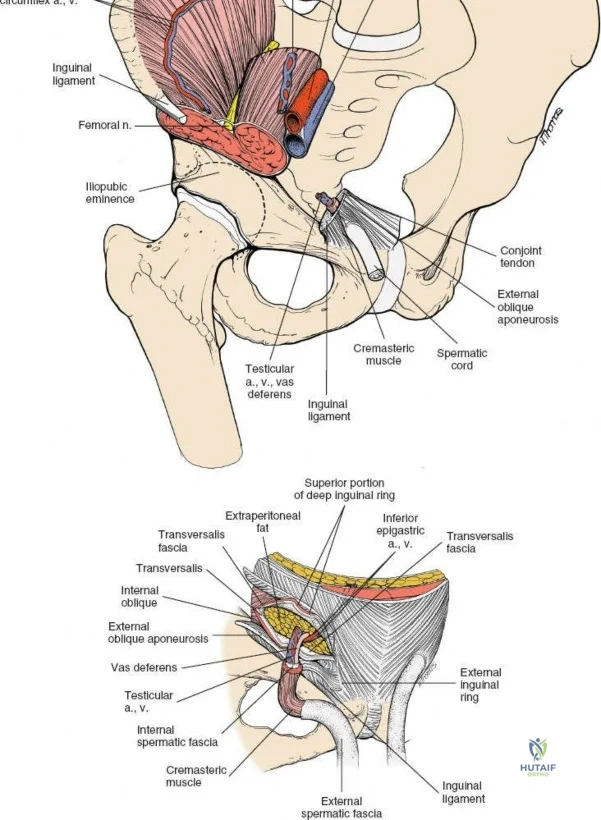
The ilioinguinal approach, pioneered by Letournel, is the gold standard for anterior column and anterior wall acetabular fractures. It allows visualization of the entire inner aspect of the innominate bone from the SI joint to the pubic symphysis.
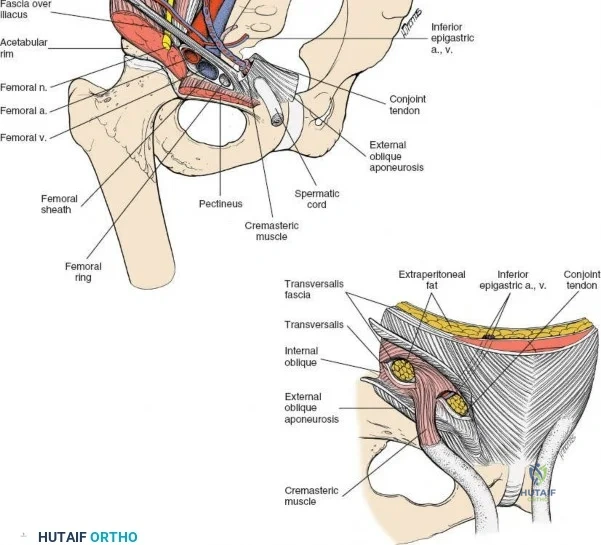
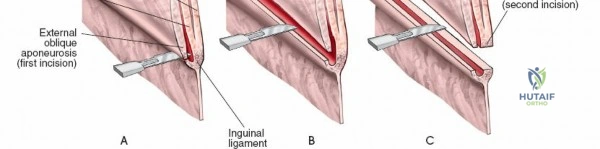
The approach involves opening three distinct anatomical "windows":
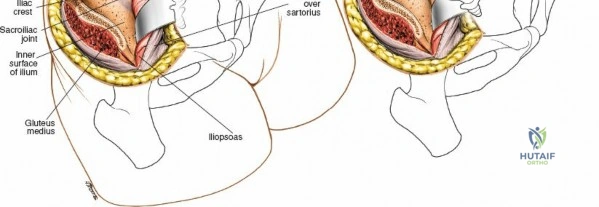
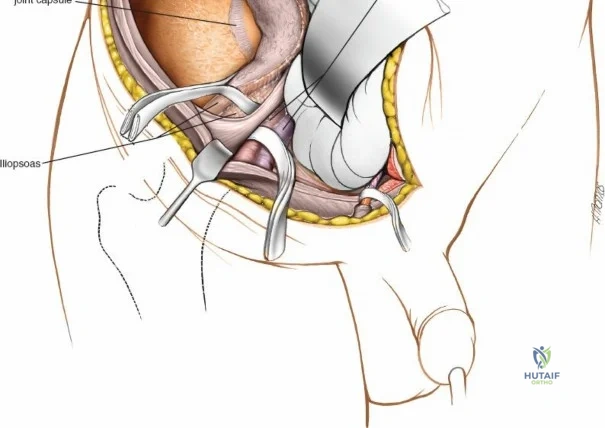
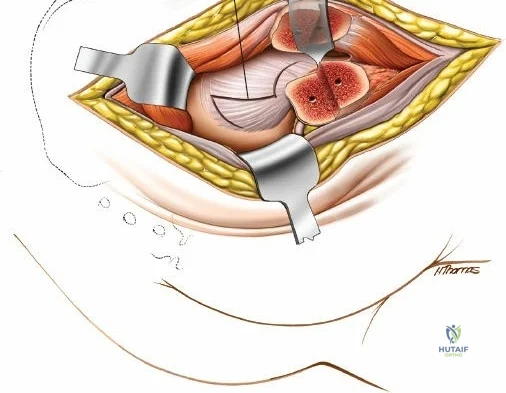
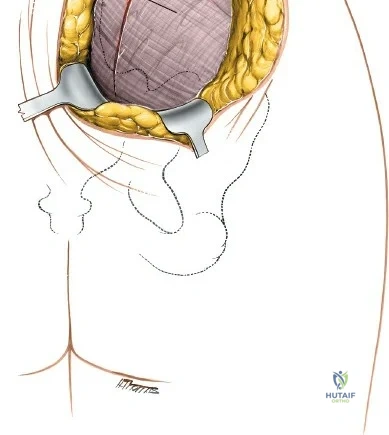
1. Lateral Window: Lateral to the iliopsoas muscle. Provides access to the iliac fossa and SI joint.
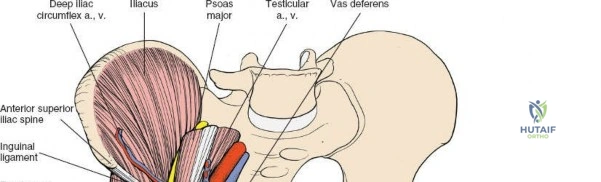
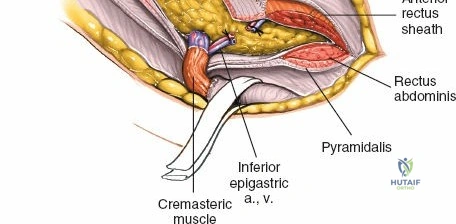
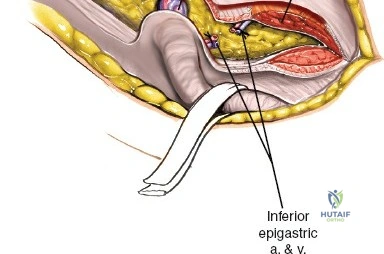
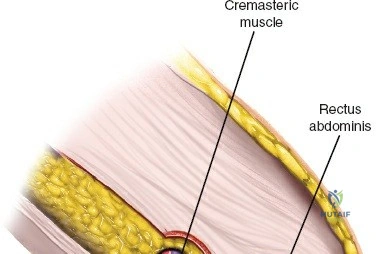
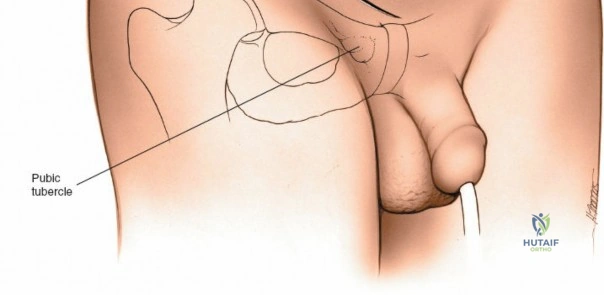
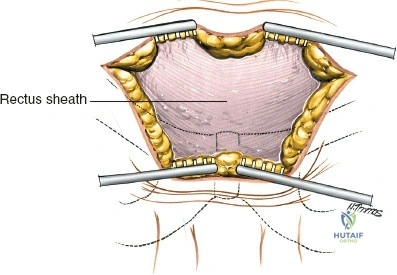
2. Middle Window: Between the iliopsoas/femoral nerve laterally and the external iliac vessels medially. Provides access to the pelvic brim and quadrilateral surface.
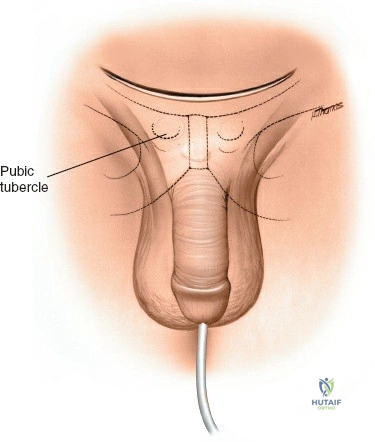
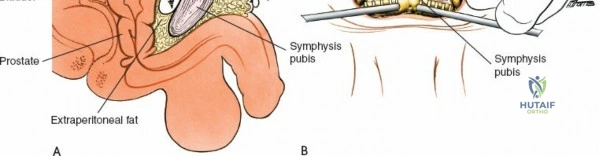
3. Medial Window: Medial to the external iliac vessels. Provides access to the superior pubic ramus and pubic symphysis.
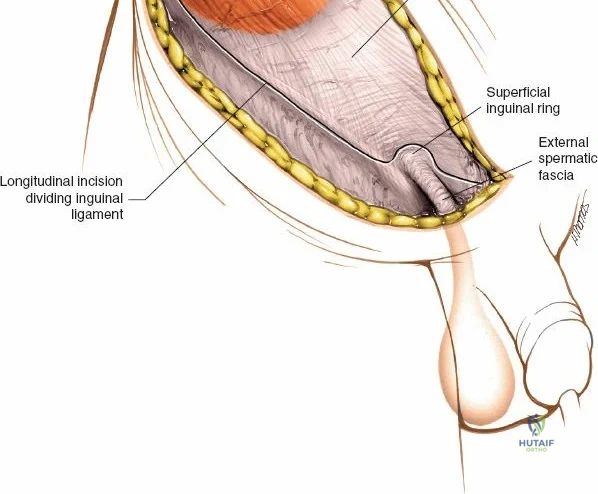
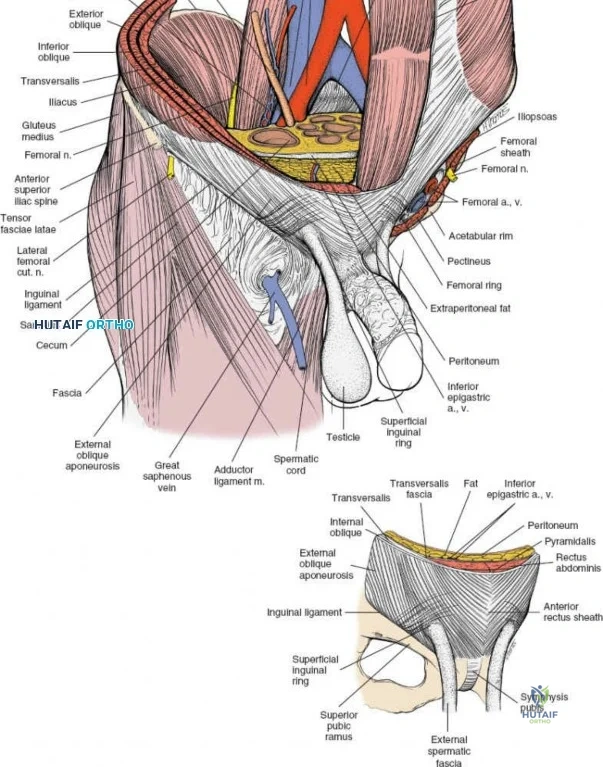
This approach is highly technical, requiring the mobilization and vessel-looping of the external iliac artery and vein, the femoral nerve, and the spermatic cord/round ligament. It does not allow direct access to the posterior column.
Complications, Incidence Rates, and Salvage Management
Surgical intervention in the pelvis and acetabulum carries a high risk of morbidity. The surgeon must be prepared to manage both approach-related and fracture-related complications.
| Complication | Estimated Incidence | Prevention and Salvage Management |
|---|---|---|
| Lateral Femoral Cutaneous Nerve (LFCN) Injury | 10% - 30% (Anterior approaches) | Prevention: Keep incision and dissection strictly lateral to the ASIS. Avoid heavy retractor pressure on the psoas. Salvage: Often resolves spontaneously. Neuromodulators (gabapentin) for painful meralgia paresthetica. |
| Superior Cluneal Nerve Neuroma | 5% - 10% (Posterior approaches) | Prevention: Limit lateral dissection on the posterior crest to <7 cm from the PSIS. Salvage: Local anesthetic/steroid injections; surgical excision and burying of the nerve stump in muscle if recalcitrant. |
| Hernia (Abdominal/Inguinal) | 1% - 3% | Prevention: Preserve the ASIS. Meticulous, multi-layer, heavy-suture closure of the abdominal fascia to the gluteal/iliacus fascia. Salvage: General surgery consultation for mesh herniorrhaphy. |
| Superior Gluteal Artery Laceration | 1% - 2% (Posterior/Sciatic notch) | Prevention: Subperiosteal dissection only. Avoid plunging retractors into the sciatic notch. Salvage: Immediate packing. If retracted into the pelvis, emergent endovascular angioembolization is required. |
| Iliac Wing Fracture | < 1% | Prevention: Avoid overly aggressive osteotome use; do not undercut the ASIS or PSIS during graft harvest. Salvage: Plate or screw fixation if structurally significant; otherwise, protected weight-bearing. |
| Deep Surgical Site Infection (SSI) | 2% - 5% | Prevention: Preoperative antibiotics, meticulous hemostasis to prevent hematoma, copious irrigation. Salvage: Aggressive surgical debridement, targeted IV antibiotics, hardware retention if stable. |
Phased Post-Operative Rehabilitation Protocols
Rehabilitation following pelvic and acetabular surgery is a prolonged process, requiring strict adherence to weight-bearing precautions to prevent hardware failure and loss of reduction.
Phase 1: Immediate Post-Operative (Weeks 0-6)
- Weight Bearing: Touch-down weight-bearing (TDWB) or non-weight-bearing (NWB) on the affected extremity. For bilateral injuries, wheelchair mobility is mandatory.
- DVT Prophylaxis: Pelvic trauma patients are at extremely high risk for venous thromboembolism (VTE). Chemical prophylaxis (e.g., LMWH or DOACs) is mandatory for at least 4-6 weeks unless contraindicated. Mechanical prophylaxis (SCDs) should be used bilaterally.
- Range of Motion (ROM): Passive and active-assisted ROM of the hip, knee, and ankle to prevent capsular contracture. Avoid combined hip flexion and internal rotation if a posterior wall fracture was repaired.
Phase 2: Intermediate Recovery (Weeks 6-12)
- Clinical/Radiographic Check: Obtain AP and Judet views at 6 weeks to assess callus formation and hardware integrity.
- Weight Bearing: If radiographic healing is progressing, advance to partial weight-bearing (PWB), progressing to full weight-bearing (FWB) by 10-12 weeks.
- Physical Therapy: Initiate active ROM, isometric gluteal and quadriceps strengthening, and aquatic therapy if incisions are fully healed.
Phase 3: Advanced Rehabilitation (Months 3-6+)
- Strengthening: Focus on abductor strengthening to eliminate Trendelenburg gait.
- Functional Return: Proprioceptive training, core stabilization, and gradual return to occupational duties. High-impact activities (running, jumping) are typically restricted until 6-9 months post-operatively.
Summary of Landmark Literature and Clinical Guidelines
The modern surgical treatment of the pelvis and acetabulum is built upon the foundational work of Emile Letournel and Robert Judet. Their seminal textbook, Fractures of the Acetabulum, established the anatomical classification system and the standard surgical approaches (Ilioinguinal and Kocher-Langenbeck) that remain in universal use today.
Recent literature has heavily scrutinized the morbidity associated with autologous bone graft harvest. Studies by Ahlmann et al. and Goulet et al. highlight that while autograft remains the gold standard for osteoinduction and osteoconduction, the complication rates (specifically chronic pain at the harvest site) can approach 15-30%. This has driven the evolution of orthobiologics, including Demineralized Bone Matrix (DBM), Bone Morphogenetic Proteins (BMP-2 and BMP-7), and synthetic ceramics (tricalcium phosphate). However, for massive structural defects in the pelvic ring, structural corticocancellous autograft from the posterior ilium remains unsurpassed.
Clinical guidelines from the Orthopaedic Trauma Association (OTA) and the American Academy of Orthopaedic Surgeons (AAOS) strongly recommend that complex acetabular and pelvic ring reconstructions be performed at Level I trauma centers by fellowship-trained pelvic/acetabular surgeons. The learning curve is exceptionally steep, and registry data consistently demonstrates that functional outcomes are directly proportional to the accuracy of the articular reduction (within 2 mm of anatomic step-off) and the volume of cases performed by the treating institution.
In conclusion, unlocking the posterior and anterior iliac crests, along with mastering the deep approaches to the true pelvis, requires an uncompromising dedication to surgical anatomy. Whether harvesting graft for a complex non-union or reconstructing a shattered acetabulum, the principles of meticulous soft tissue handling, precise internervous dissection, and rigid biomechanical fixation remain the cornerstones of successful orthopedic surgery.
Clinical & Radiographic Imaging Archive