Mastering Knee Approaches: Spotlight on Superficial Medial Ligament

Key Takeaway
In this comprehensive guide, we discuss everything you need to know about Mastering Knee Approaches: Spotlight on Superficial Medial Ligament. Knee approaches are surgical methods to access the joint, categorized as arthroscopic or open. The knee's superficial nature simplifies these procedures. A medial approach grants easier access to medial supporting structures like the superficial medial ligament, aiding in procedures for the posteromedial corner. Arthroscopic approaches are common for meniscal issues, while open approaches are used for trauma or comprehensive exposure, such as total joint replacement.
Comprehensive Introduction and Patho-Epidemiology
The knee is an incredibly complex, unconstrained synovial hinge joint that relies heavily on a sophisticated interplay of powerful muscular forces, dynamic tendinous insertions, and static ligamentous restraints to maintain stability across a wide range of motion. Unlike the hip, which derives substantial inherent stability from its deep ball-and-socket osseous architecture, the knee joint is relatively superficial on three of its four sides—anterior, medial, and lateral. This unique anatomic configuration renders the joint highly accessible for both open and arthroscopic surgical approaches. Over the past several decades, the evolution of orthopedic surgery has seen a paradigm shift; arthroscopic approaches have largely replaced traditional open arthrotomies for the management of intra-articular pathology. This transition has revolutionized the treatment of meniscal tears, anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL) ruptures, chondral defects, and the extraction of loose bodies, significantly reducing surgical morbidity and accelerating patient rehabilitation.
Despite the dominance of arthroscopy for intra-articular work, comprehensive knowledge of open surgical approaches remains absolutely paramount for the orthopedic surgeon. Open approaches are indispensable when dealing with high-energy trauma, complex intra-articular fractures, multiligamentous knee injuries, total joint arthroplasty, and scenarios where arthroscopic equipment is either unavailable or contraindicated. Furthermore, addressing extra-articular ligamentous pathology—particularly on the medial side of the knee—requires a masterful understanding of open dissection planes. The medial approach to the knee joint, which affords unparalleled access to the superficial medial collateral ligament (sMCL) and the posteromedial corner (PMC), is a critical technique for reconstructing the medial supporting structures following severe valgus and rotatory trauma.
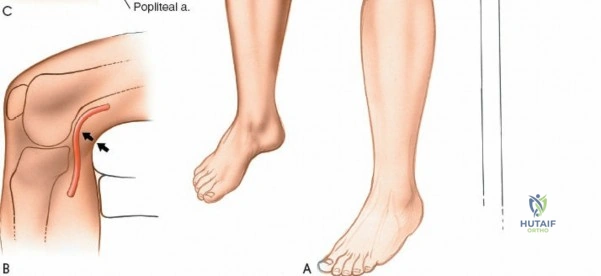
The epidemiology of knee injuries dictates a high frequency of surgical intervention in both athletic and degenerative populations. Medial-sided knee injuries, particularly those involving the sMCL, are among the most common ligamentous injuries encountered in sports medicine, often resulting from a direct valgus blow or a non-contact external rotation force applied to a flexed knee. While isolated sMCL injuries frequently heal with non-operative functional bracing, high-grade tears (Grade III), distal avulsions (Stener-like lesions of the knee), and those associated with multiligamentous trauma (such as the classic "unhappy triad") often necessitate meticulous open surgical repair or reconstruction. Understanding the precise topographic anatomy and the layered surgical approaches to these structures is essential to restore native joint kinematics and prevent chronic anteromedial rotatory instability (AMRI).
This chapter provides an exhaustive, step-by-step masterclass on the surgical approaches to the knee, bridging the gap between state-of-the-art arthroscopic techniques and foundational open arthrotomies. We will place a special spotlight on the medial approach and the superficial medial ligament, detailing the internervous planes, the layered dissection of the medial compartment, and the critical neurovascular structures that must be protected. By mastering these approaches, the orthopedic surgeon can confidently navigate the complex three-dimensional anatomy of the knee, ensuring optimal exposure, precise anatomic restoration, and superior clinical outcomes for their patients.
Detailed Surgical Anatomy and Biomechanics
Osteology and Articular Geometry
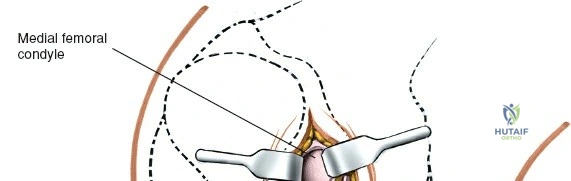
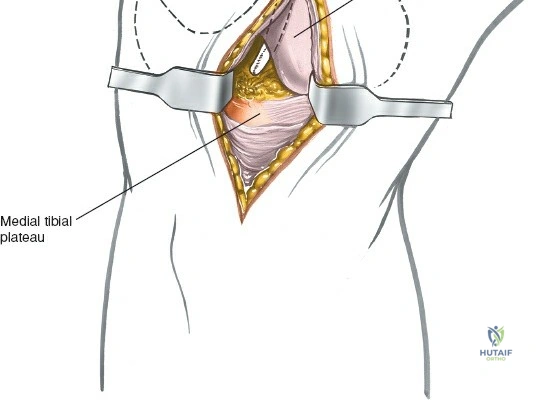
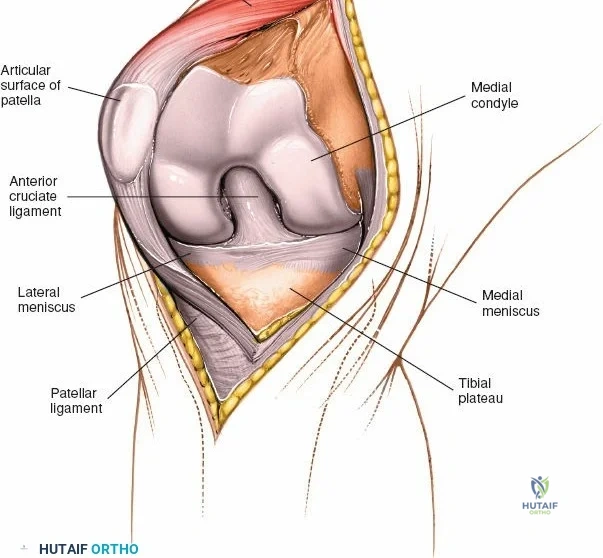
The osseous anatomy of the knee comprises the distal femur, the proximal tibia, and the patella, forming two distinct articulations: the tibiofemoral joint and the patellofemoral joint. The distal femur expands into the medial and lateral condyles, which are separated posteriorly by the deep intercondylar notch. The medial femoral condyle is larger, extends further distally, and possesses a more complex radius of curvature compared to the lateral condyle, which contributes to the "screw-home" mechanism during terminal extension. The proximal tibia features two distinct plateaus; the medial plateau is concave and larger, accommodating the medial femoral condyle, while the lateral plateau is convex, allowing for greater anteroposterior translation of the lateral meniscus and femoral condyle during flexion.
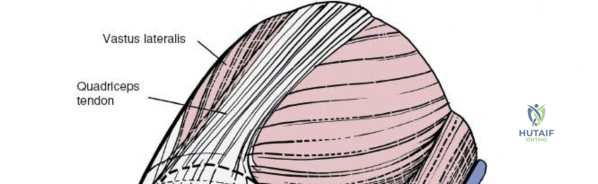
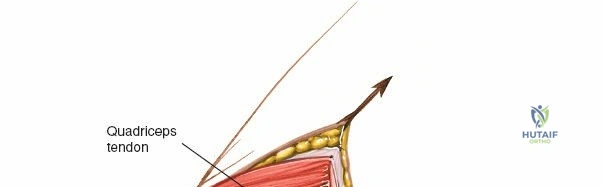
The patella, the largest sesamoid bone in the human body, rests within the trochlear groove of the anterior femur. Its articular surface is divided into medial and lateral facets by a vertical ridge, with an additional "odd facet" located on the far medial border. The tracking of the patella is governed by the complex interplay of the quadriceps vector (Q-angle), the geometry of the trochlea, and the medial patellofemoral ligament (MPFL). Because the anterior, medial, and lateral aspects of the knee are covered primarily by skin, subcutaneous fat, and retinacular tissue, surgical access to these osseous structures is remarkably direct. However, this superficial nature also means that surgical incisions must be carefully planned to avoid painful neuromas and to ensure adequate soft-tissue coverage over orthopedic implants.
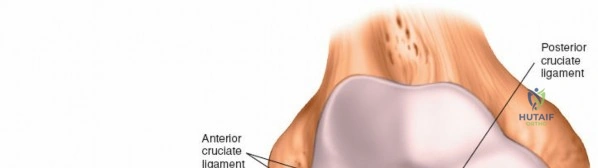
The biomechanics of the knee joint dictate that it is not a simple hinge but rather a dynamic joint that undergoes rolling, gliding, and rotational movements. As the knee flexes from full extension, the femoral condyles initially roll posteriorly on the tibial plateau, followed by a gliding motion governed by the tension in the cruciate ligaments. The anterior cruciate ligament (ACL) prevents anterior translation of the tibia, while the posterior cruciate ligament (PCL) prevents posterior translation. The menisci, which are fibrocartilaginous, wedge-shaped structures, serve to deepen the articular surfaces, distribute compressive loads, and provide secondary stabilization. Understanding these kinematics is crucial when performing arthroscopic evaluations, as dynamic manipulation of the joint is required to visualize the posterior horns of the menisci and the cruciate insertions.
Medial Compartment and Superficial Medial Ligament
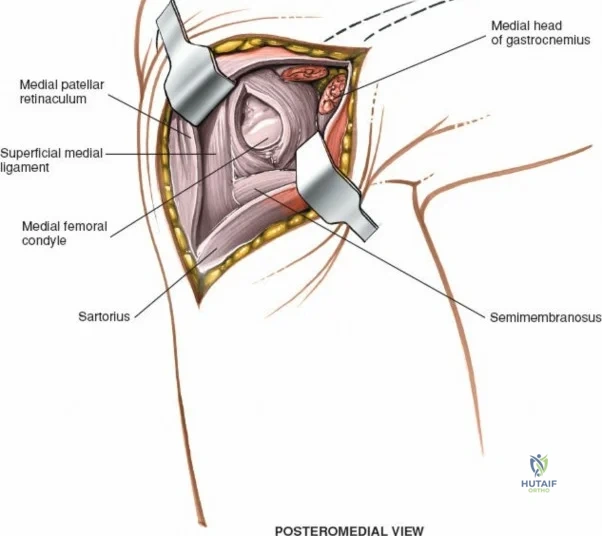
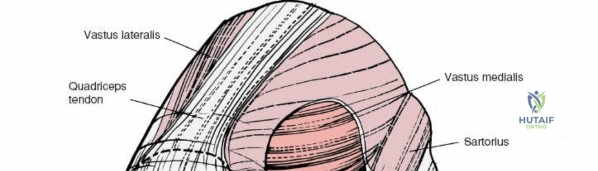
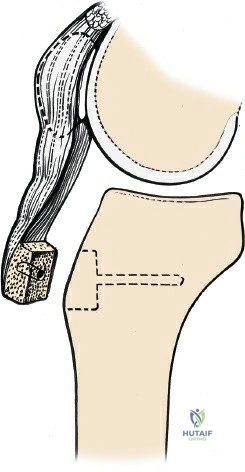
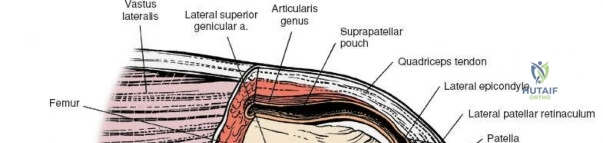
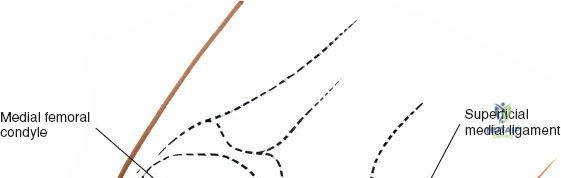
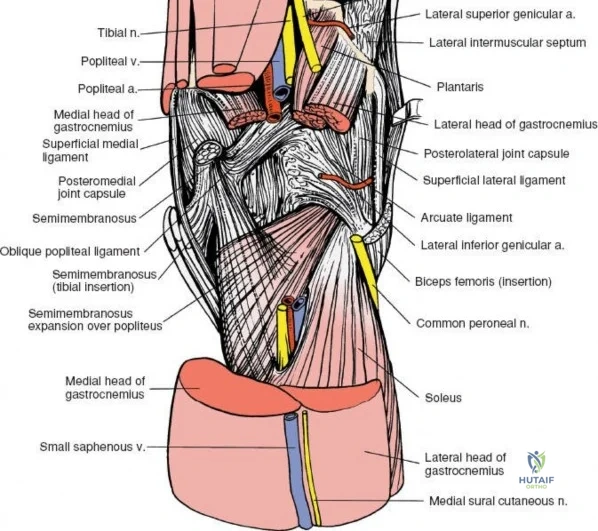
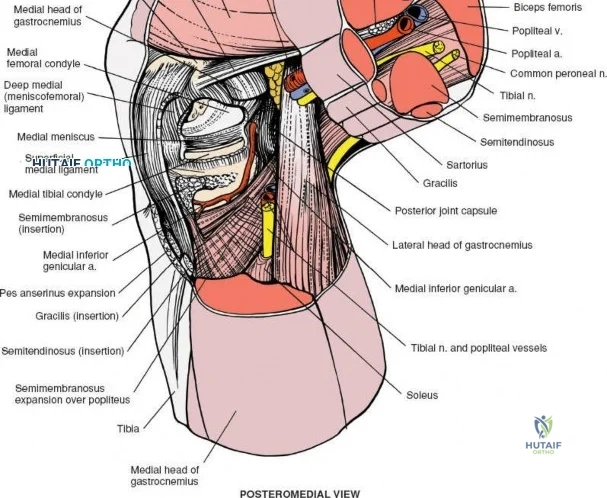
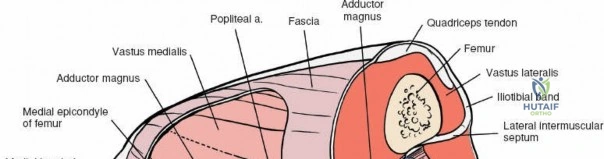
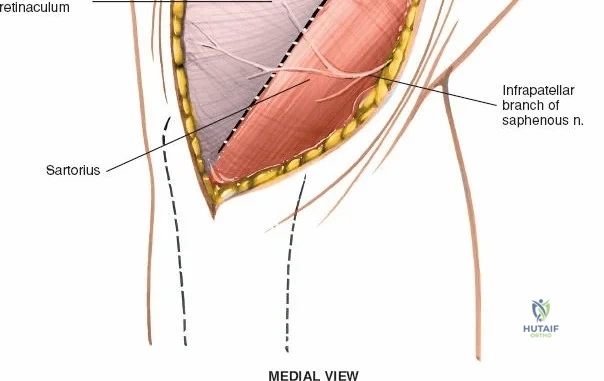
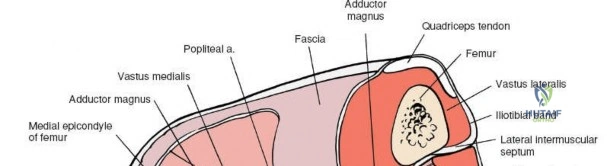
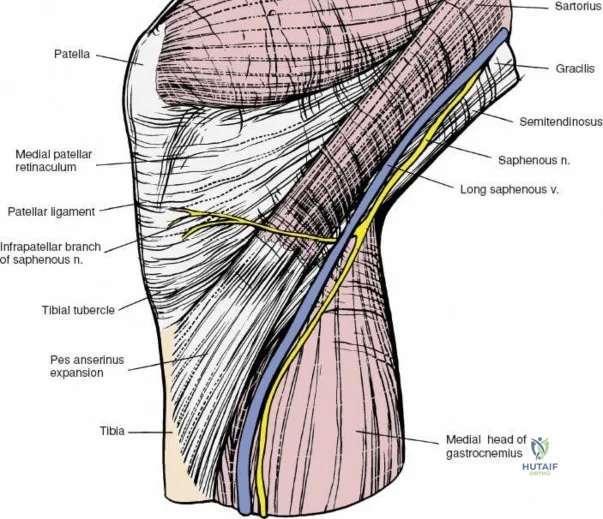
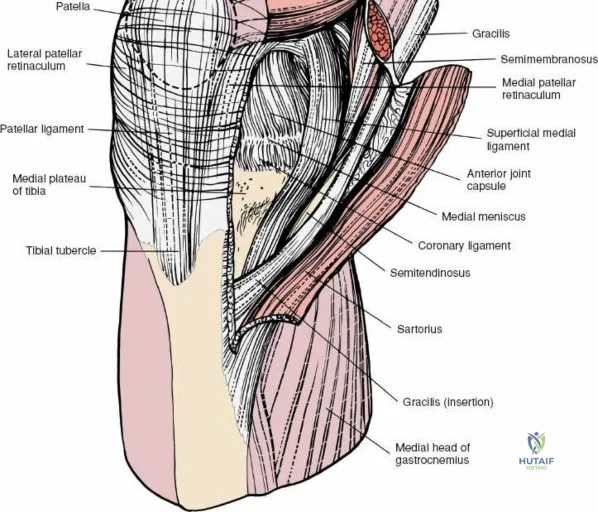
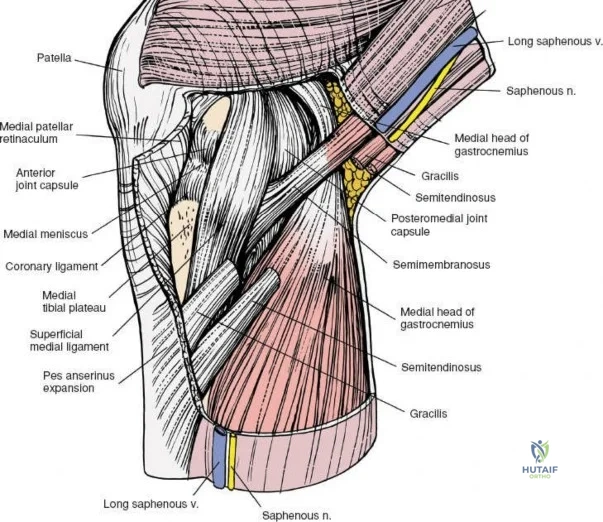
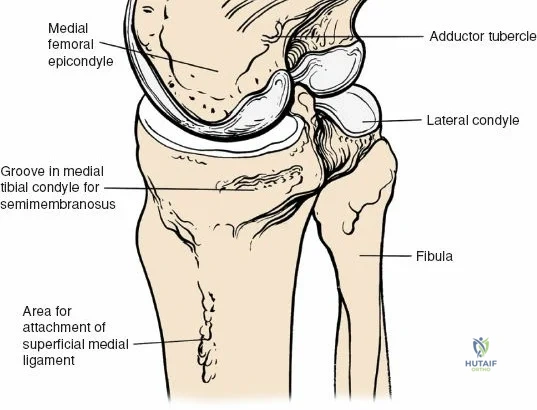
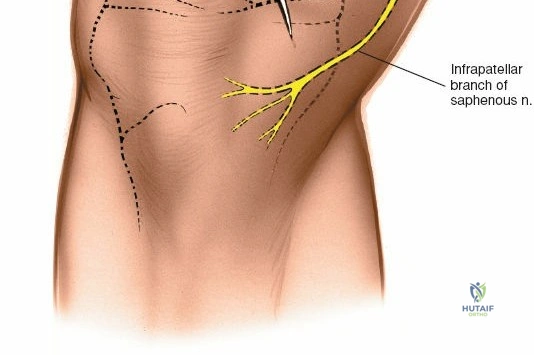
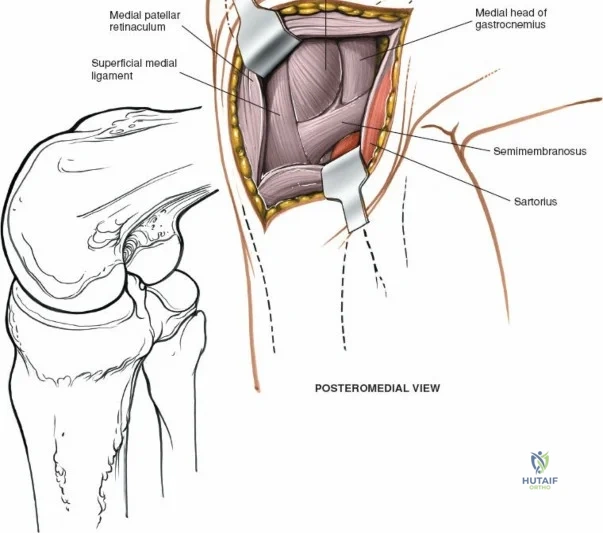
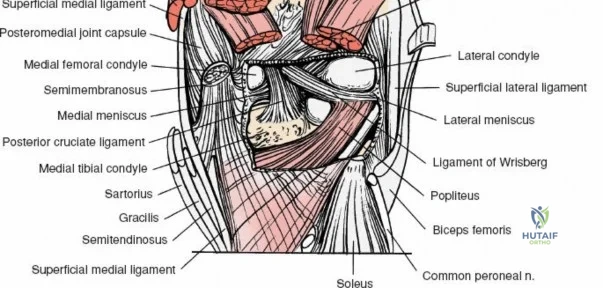
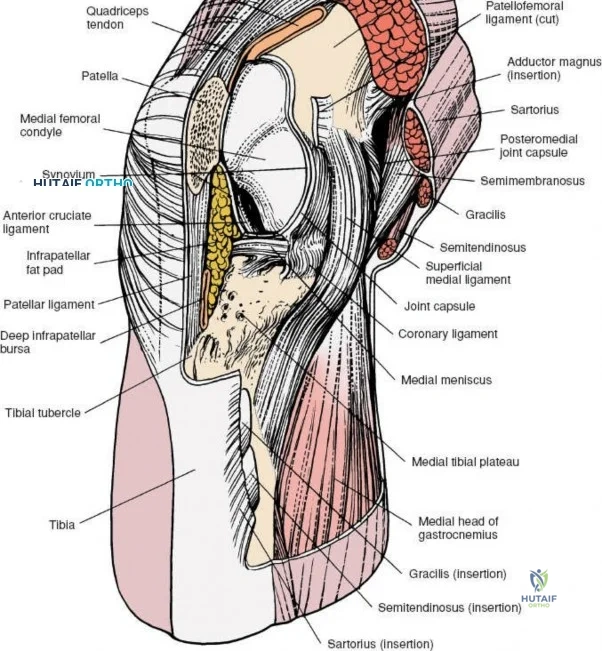
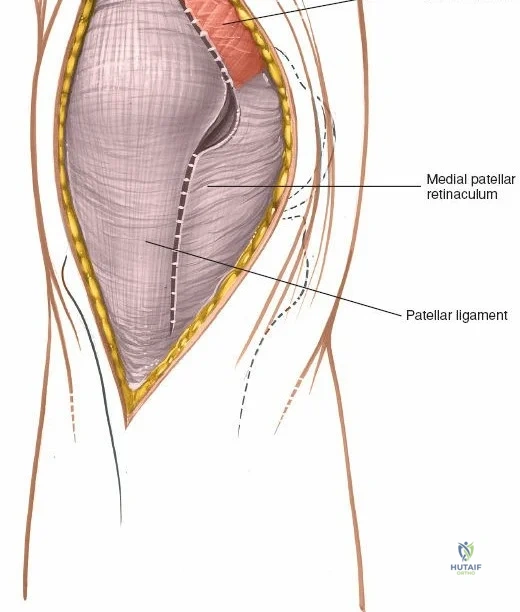
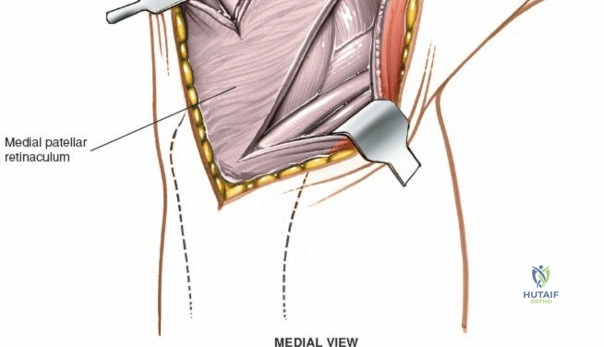
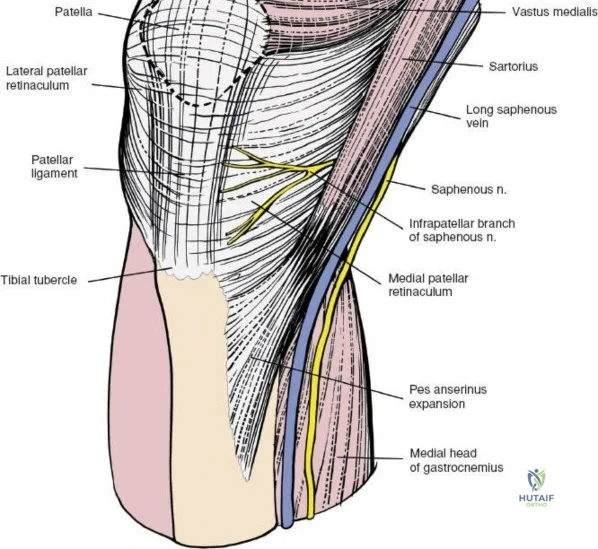
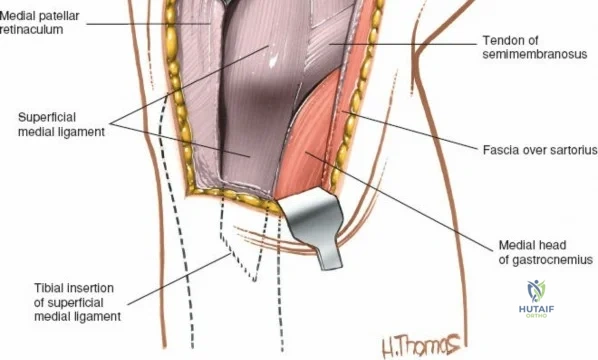
The medial side of the knee is anatomically organized into three distinct layers, as classically described by Warren and Marshall. Layer 1 is the most superficial, consisting of the deep crural fascia, which invests the sartorius muscle and covers the anterior structures. The saphenous nerve and its infrapatellar branch course between Layer 1 and Layer 2, making them highly susceptible to iatrogenic injury during medial incisions. Layer 2 contains the superficial medial collateral ligament (sMCL), the medial patellofemoral ligament (MPFL), and the posterior oblique ligament (POL). The sMCL is the primary static restraint to valgus stress. It originates from the medial femoral epicondyle, slightly proximal and posterior to the adductor tubercle, and courses distally to insert broadly on the medial aspect of the proximal tibia, deep to the pes anserinus tendons.
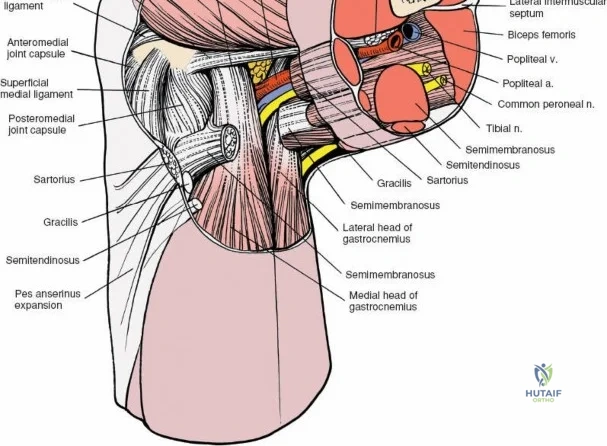
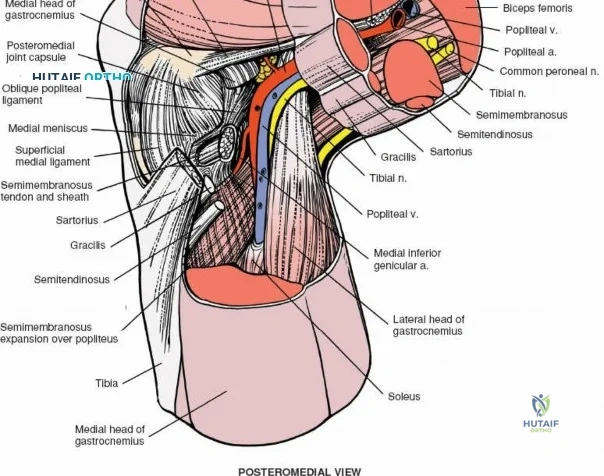
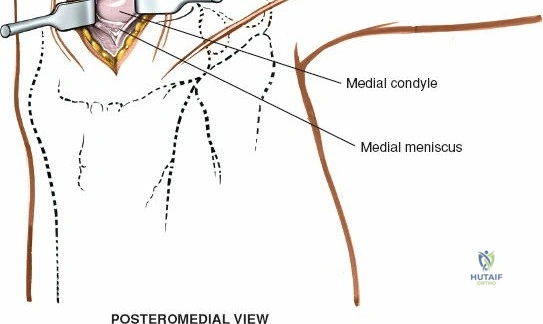
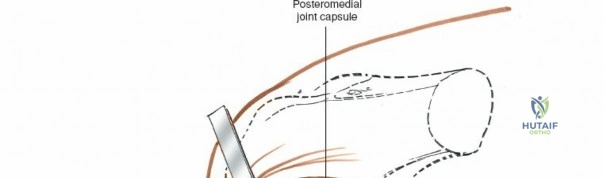
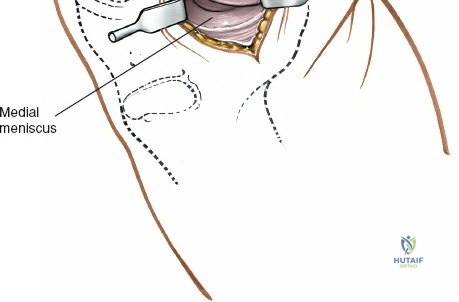
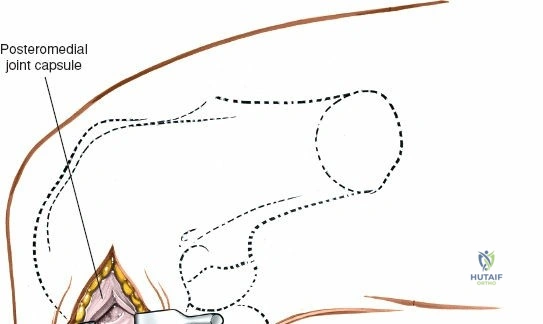
Layer 3 represents the true joint capsule and the deep medial collateral ligament (dMCL), which is further divided into meniscofemoral and meniscotibial (coronary) ligaments. The dMCL is intimately attached to the medial meniscus, anchoring it to the joint margin. Posteriorly, Layers 2 and 3 coalesce to form the posteromedial corner (PMC), a critical complex comprising the POL, the semimembranosus tendon expansions, and the oblique popliteal ligament. The PMC is the primary restraint to anteromedial rotatory instability and provides secondary valgus stabilization, particularly when the knee is near full extension.
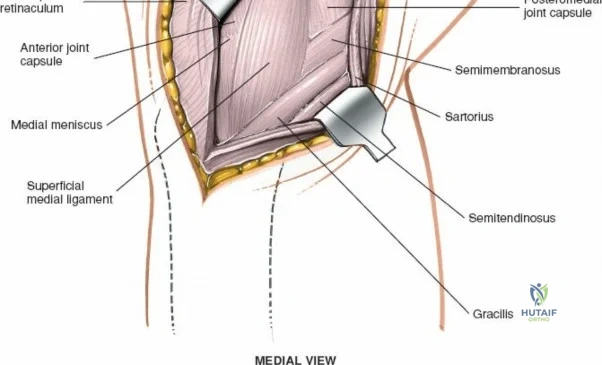
Biomechanically, the sMCL is tensioned throughout the range of motion. The anterior fibers of the sMCL are taut in flexion, whereas the posterior fibers and the POL become taut in extension. Consequently, clinical evaluation of the sMCL requires valgus stress testing at both 0 degrees and 30 degrees of flexion. An isolated sMCL injury will typically demonstrate laxity at 30 degrees but remain stable at 0 degrees due to the intact PMC and cruciate ligaments. Surgical approaches to the medial side must respect these layers. A direct medial approach allows the surgeon to elevate a full-thickness flap, providing access to the sMCL and the posteromedial corner for anatomic repair or reconstruction without compromising the vascular supply to the overlying skin.
Lateral and Posterior Compartments
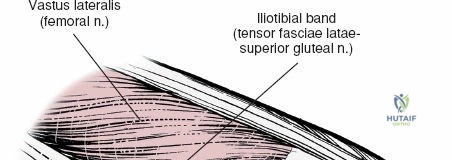
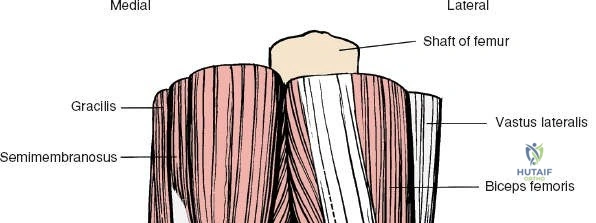
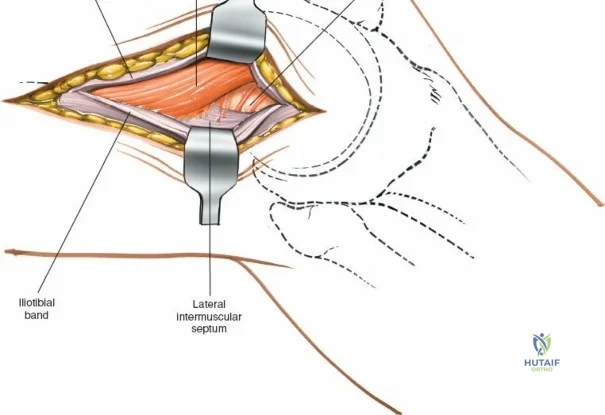
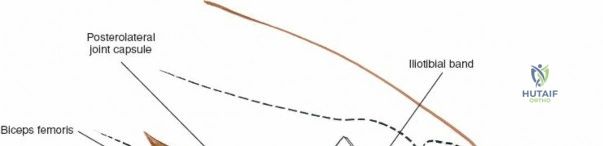
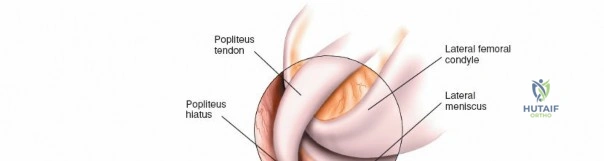
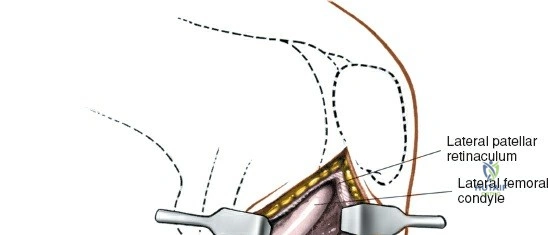
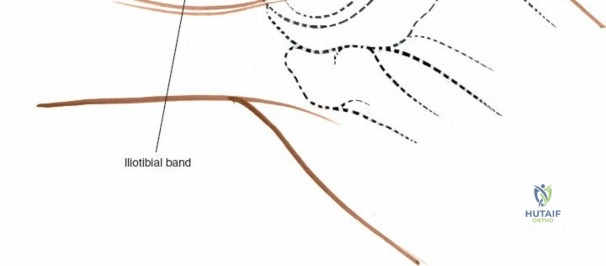
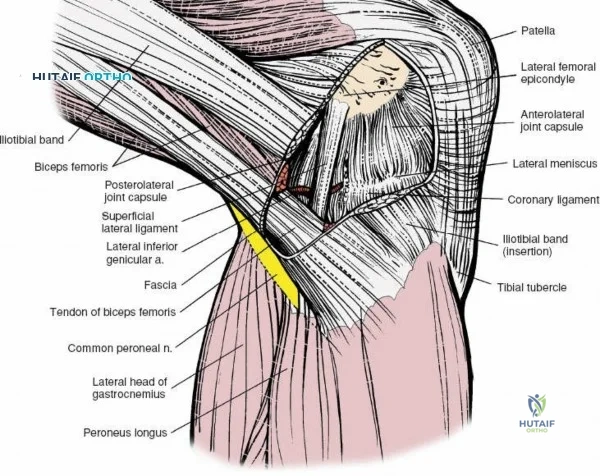
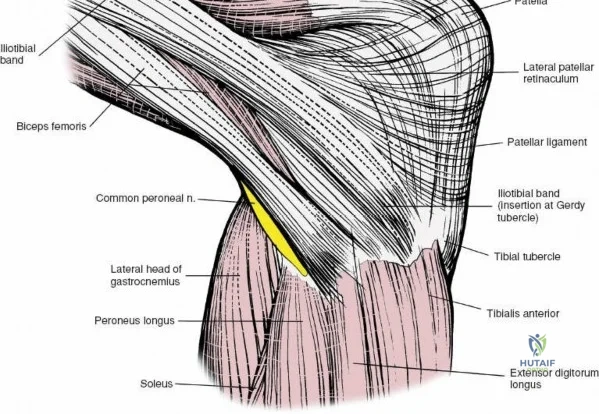
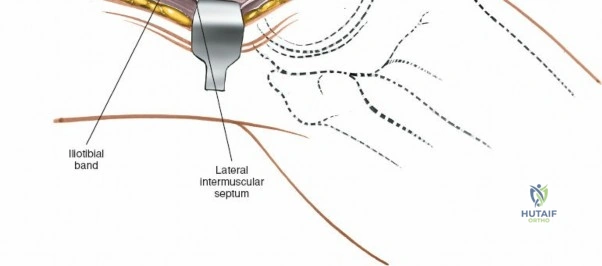
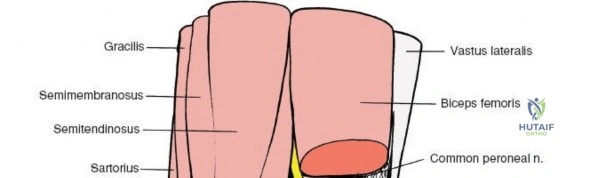
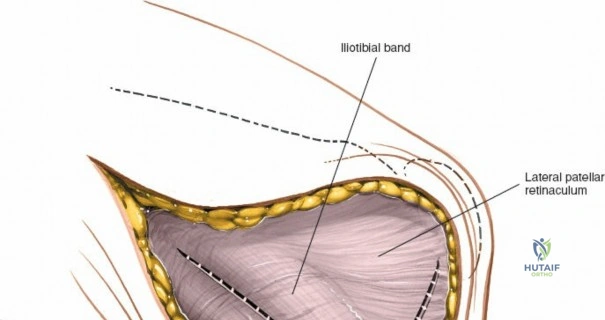
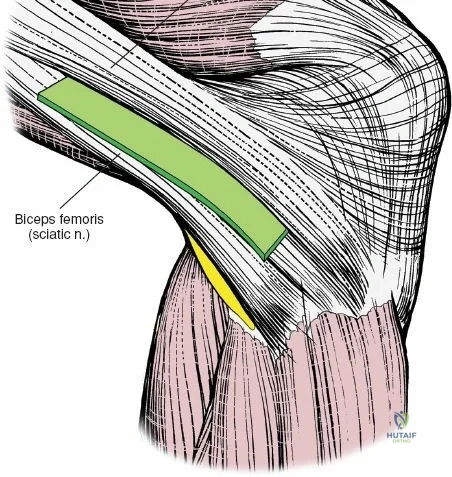
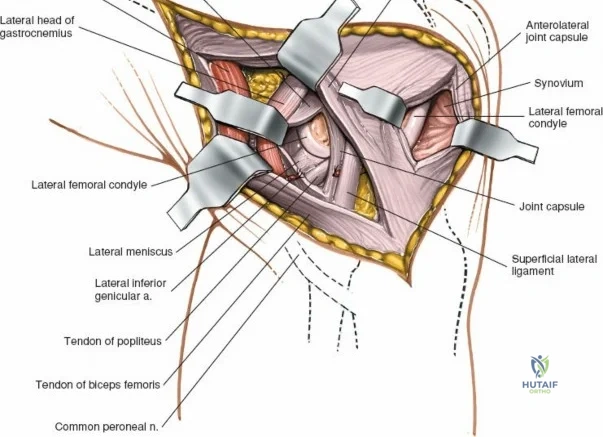
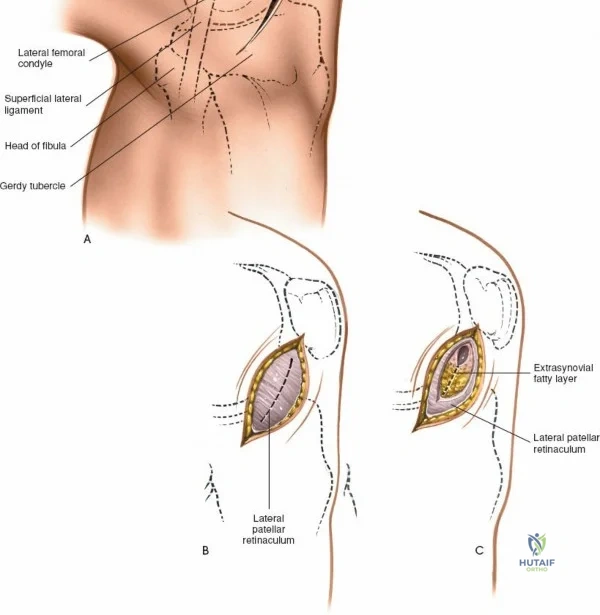
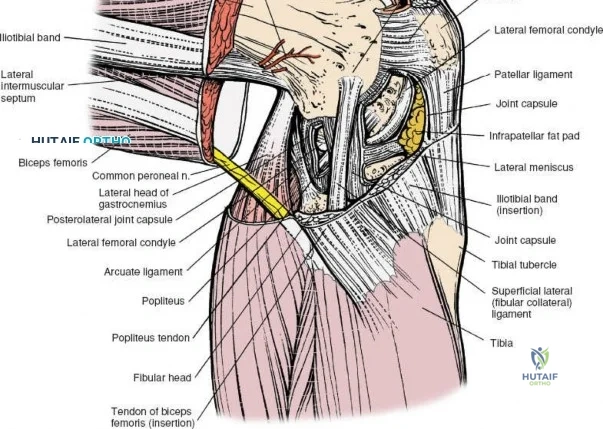
The lateral side of the knee is similarly layered but structurally distinct, designed to resist varus and posterolateral rotatory forces. The superficial layer consists of the iliotibial band (ITB) and the biceps femoris tendon. The middle layer includes the patellar retinaculum and the patellofemoral ligaments. The deep layer comprises the lateral collateral ligament (LCL), the popliteus tendon, and the popliteofibular ligament, which together form the posterolateral corner (PLC). The LCL originates from the lateral femoral epicondyle and inserts on the fibular head. Unlike the sMCL, the LCL is extra-capsular and is not attached to the lateral meniscus, which allows the lateral meniscus greater mobility and makes it less prone to tearing during rotational trauma.
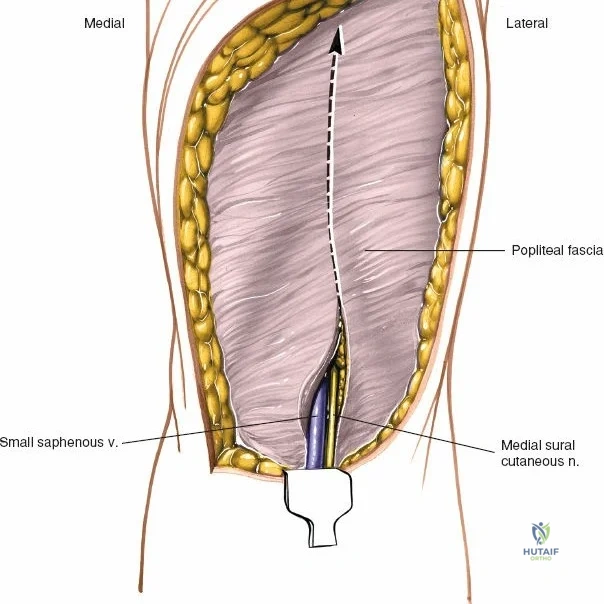
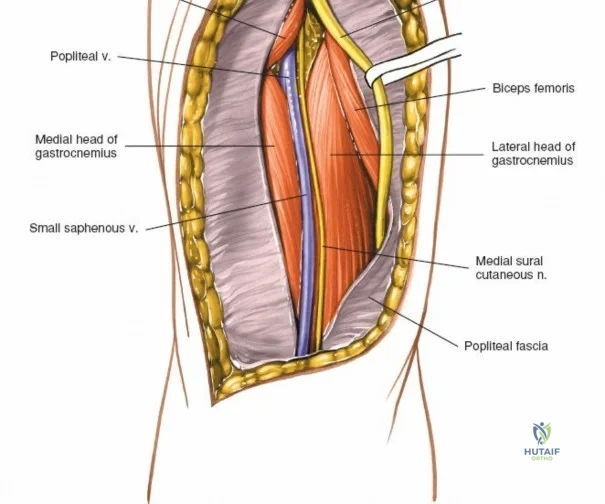
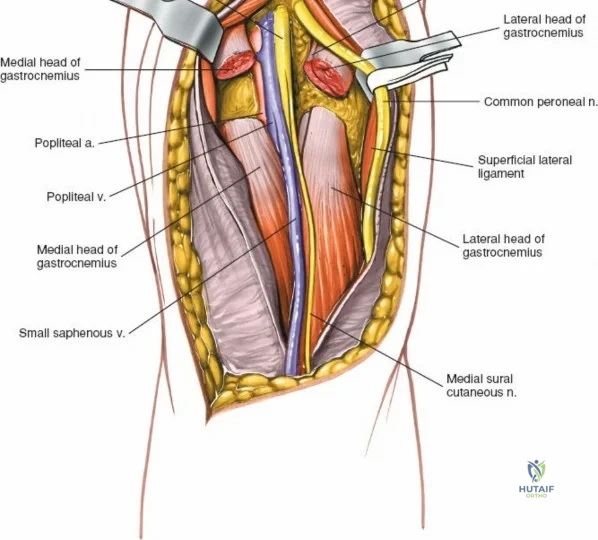
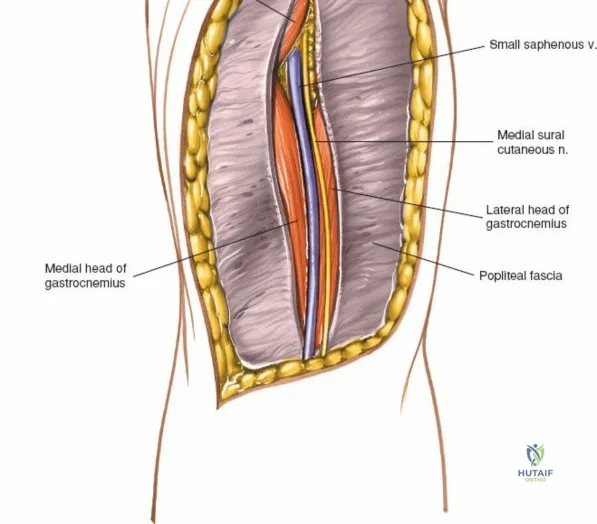
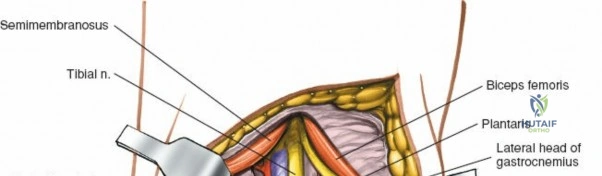
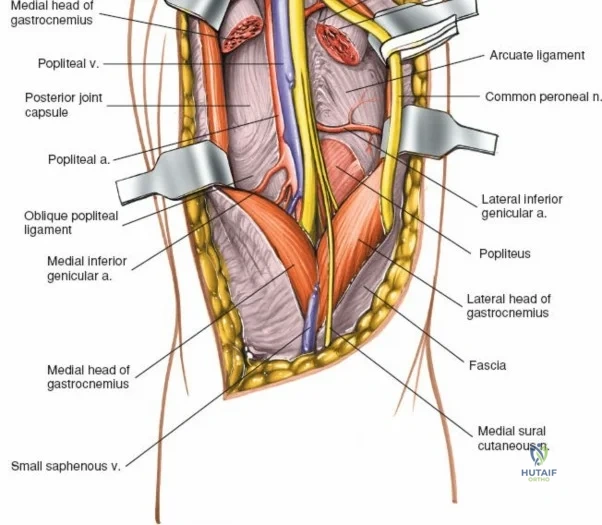
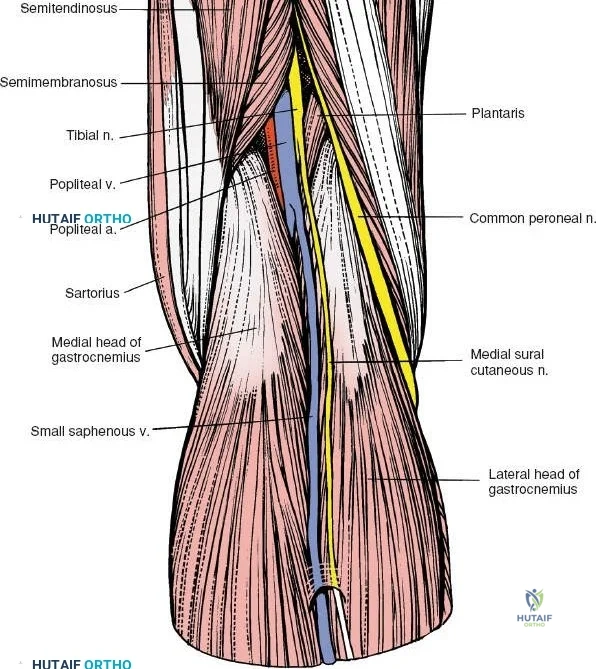
The posterior aspect of the knee is characterized by the popliteal fossa, a diamond-shaped space bounded by the hamstring tendons superiorly and the gastrocnemius heads inferiorly. This region houses the major neurovascular bundle of the lower extremity: the popliteal artery, popliteal vein, and the tibial nerve. Because these critical structures pass directly posterior to the joint capsule, posterior approaches to the knee are fraught with hazard and are generally reserved for specific indications, such as repair of neurovascular injuries, fixation of posterior tibial plateau shear fractures, or reconstruction of a tibial-sided PCL avulsion.

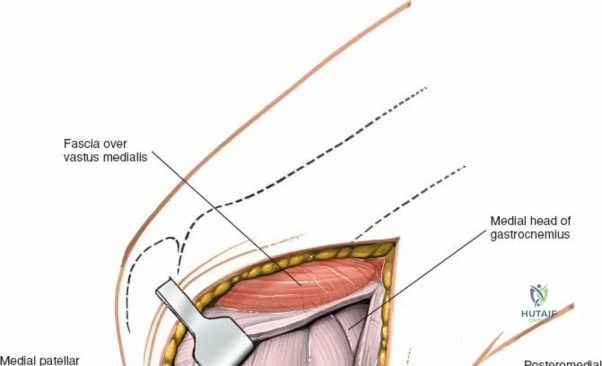
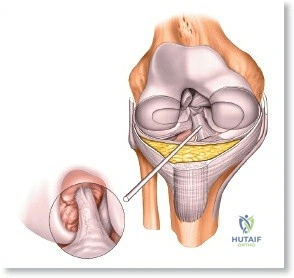
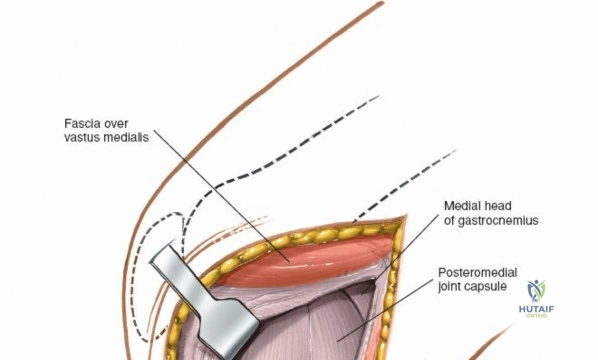
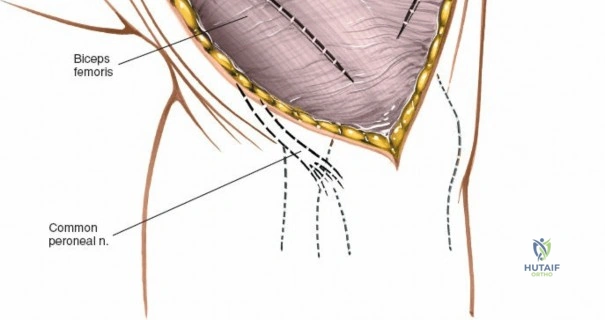
Arthroscopically, the posterior compartments can be accessed via posteromedial and posterolateral portals. The posteromedial portal is established by transilluminating the joint from the anterolateral portal and inserting a spinal needle posterior to the sMCL and anterior to the medial head of the gastrocnemius. This provides excellent visualization of the posterior horn of the medial meniscus, the PCL insertion, and the posterior capsule. The posterolateral portal is established similarly but requires extreme caution to avoid the common peroneal nerve, which courses posterior to the biceps femoris tendon and wraps around the fibular neck.
Exhaustive Indications and Contraindications
Arthroscopic Interventions
Arthroscopy of the knee has largely replaced open procedures for a vast array of intra-articular pathologies due to its minimally invasive nature, lower complication rates, and rapid postoperative recovery. Primary indications for knee arthroscopy include meniscal resection or repair, removal of loose bodies, reconstruction of the anterior or posterior cruciate ligaments, and synovial biopsy. It is also the gold standard for comprehensive synovectomy in patients with inflammatory arthropathies, debridement of early osteoarthritic knees (including microfracture or marrow stimulation techniques for focal chondral defects), and the management of osteochondritis dissecans (OCD) lesions. Furthermore, arthroscopically assisted repair of tibial plateau fractures allows for direct visualization of articular reduction without the morbidity of a large arthrotomy.
Contraindications to knee arthroscopy are relatively few but must be strictly respected. Absolute contraindications include active local soft-tissue infection (e.g., cellulitis) overlying the portal sites, which could introduce bacteria into the sterile joint space, and severe advanced osteoarthritis where arthroscopic debridement has been proven to offer no long-term clinical benefit over conservative management. Relative contraindications include severe joint stiffness (arthrofibrosis) that precludes safe insertion of the trochar, and compromised vascular status of the limb. Additionally, caution must be exercised in patients with significant bleeding diatheses or those on unyielding anticoagulant therapy, though many routine arthroscopies can be performed safely with appropriate perioperative medical management.
Open and Reconstructive Procedures
While the introduction of the operative arthroscope has almost ended the use of open approaches for isolated meniscectomies, open approaches remain the cornerstone of complex knee reconstruction and trauma management. The medial parapatellar approach is the workhorse incision for total knee arthroplasty (TKA), distal femoral osteotomies, and the fixation of complex intra-articular distal femur or proximal tibia fractures. The direct medial approach is specifically indicated for the acute repair or chronic reconstruction of the superficial medial collateral ligament and the posteromedial corner. This approach is essential when dealing with multiligamentous knee injuries, knee dislocations, or Grade III sMCL tears with intra-articular entrapment of the ligament ends (Stener-like lesions).
Contraindications to open medial approaches primarily revolve around poor soft-tissue envelopes. Operating through severely contused, blistered, or compromised skin significantly increases the risk of wound dehiscence and deep infection. In the setting of high-energy trauma, surgery should be delayed until the soft tissues have stabilized (the "wrinkle sign"). Additionally, a direct open approach may be contraindicated if a less invasive or arthroscopic-assisted technique can achieve the same biomechanical result with lower morbidity. The posterior approach to the knee is rarely performed and is contraindicated in the absence of a dedicated vascular or microsurgical team if neurovascular compromise is suspected, given the high risk of iatrogenic injury to the popliteal vessels.
| Surgical Approach | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Arthroscopic (AL/AM Portals) | Meniscal repair, ACL/PCL reconstruction, loose body removal, chondral procedures. | Overlying cellulitis, advanced global osteoarthritis (for debridement). | Severe arthrofibrosis, uncorrected coagulopathy. |
| Medial Parapatellar Arthrotomy | Total knee arthroplasty, complex intra-articular fractures, extensive synovectomy. | Inadequate soft-tissue envelope, active joint infection (unless for washout). | Prior lateral incisions (risk of skin bridge necrosis). |
| Direct Medial Approach (sMCL) | Grade III sMCL tears, PMC reconstruction, multiligamentous knee dislocation. | Severe medial soft-tissue compromise, isolated Grade I/II sprains. | Chronic isolated laxity without functional instability. |
| Posterior Approach | PCL tibial avulsion fixation, popliteal artery repair, posterior shear fractures. | Lack of microvascular support, extensive posterior soft-tissue injury. | Fractures amenable to anterior-to-posterior percutaneous fixation. |
Pre-Operative Planning, Templating, and Patient Positioning
Operating Room Setup and Patient Positioning
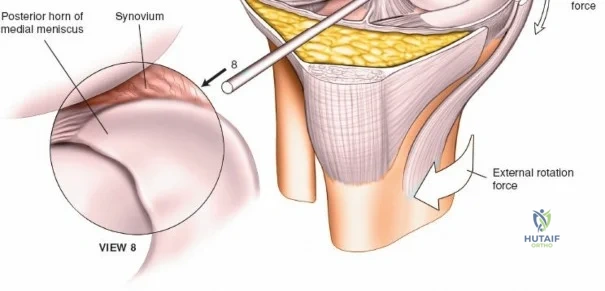
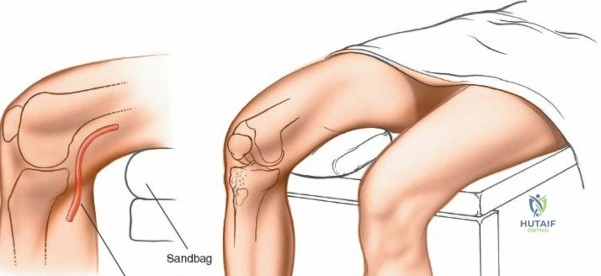
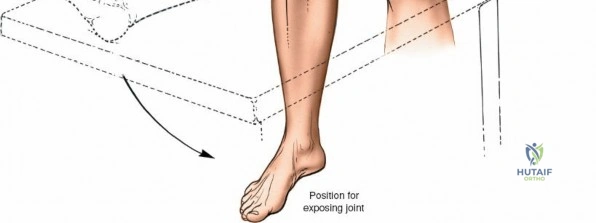
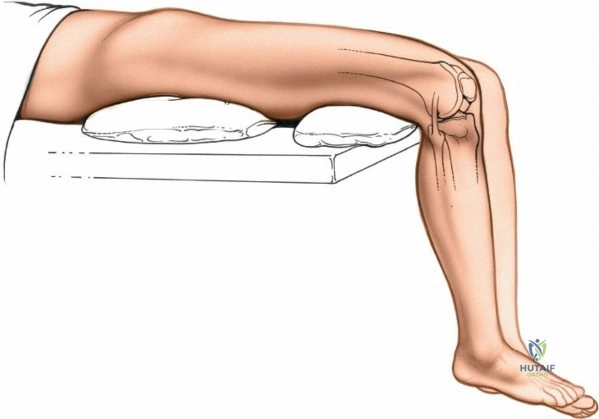
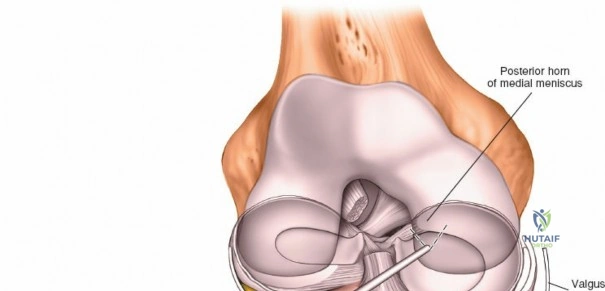
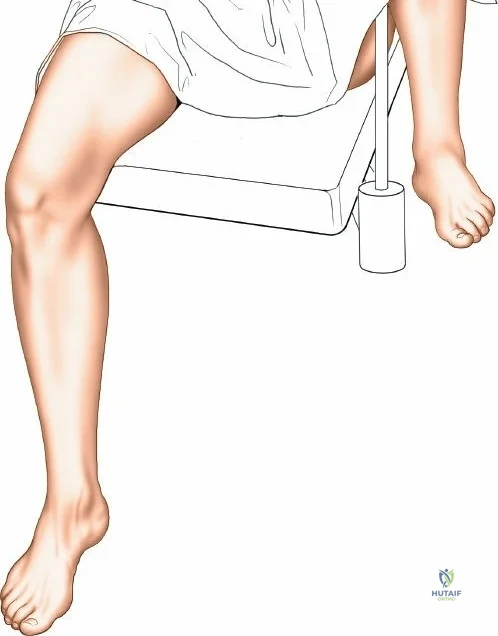
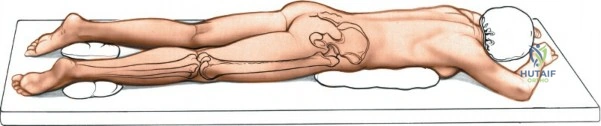
Meticulous preoperative planning and precise patient positioning are the foundational steps for successful knee surgery, whether arthroscopic or open. For arthroscopic procedures, the patient is placed supine on the operating table. The end of the table is typically removed or dropped to allow the surgeon to manipulate the knee freely through a full range of motion during surgery. A well-padded high-thigh tourniquet is applied to the operative leg. The use of an arthroscopic leg holder or a lateral post placed at the level of the tourniquet allows the surgeon to apply a valgus and external rotation force to the knee. This maneuver is absolutely critical for opening the medial compartment and facilitating access to the posterior horn of the medial meniscus and the medial femoral condyle.

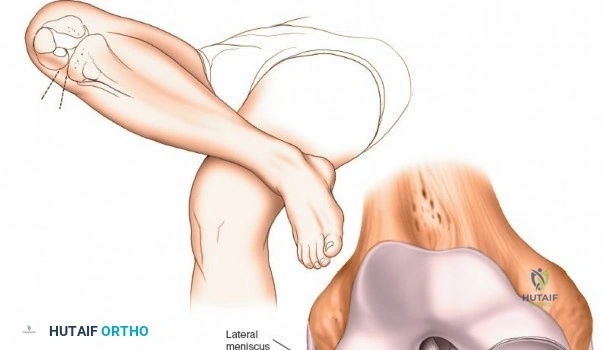
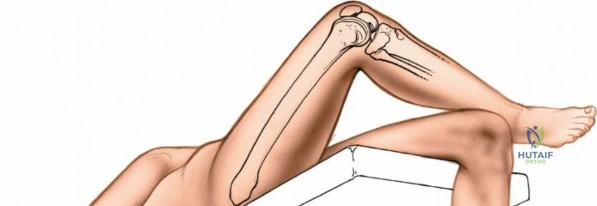
However, the use of a circumferential leg clamp can sometimes impede the ability to place the knee in the "figure-of-four" position (placing the lateral malleolus of the involved extremity on the opposite thigh). The figure-of-four position applies a varus and internal rotation stress, which is essential for opening the lateral compartment. If a skilled surgical assistant is available to manually provide the appropriate varus, valgus, and rotational forces, the use of a rigid clamp may be omitted in favor of a simple lateral post. The limb is prepped and draped in a standard sterile fashion, ensuring that the entire lower extremity from the tourniquet down to the toes is draped free to allow unhindered manipulation.
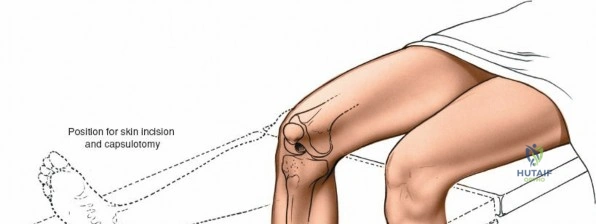
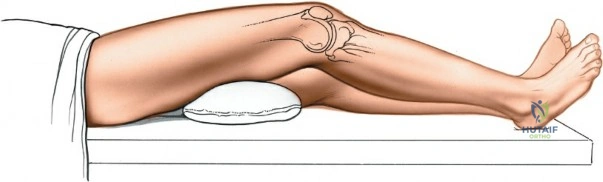
For open procedures, particularly the direct medial approach for sMCL reconstruction, the patient is similarly positioned supine. A bump may be placed under the ipsilateral hip to prevent external rotation of the leg, keeping the patella pointing directly toward the ceiling. The leg must be freely drapable to allow the surgeon to assess ligamentous tension and joint stability throughout the range of motion during the reconstruction. Preoperative templating using weight-bearing anteroposterior, lateral, and merchant view radiographs, along with advanced imaging such as MRI, is mandatory to delineate the exact tear location of the sMCL (femoral avulsion, midsubstance, or tibial avulsion) and to identify concomitant intra-articular pathology.
Surface Anatomy and Portal Landmarks
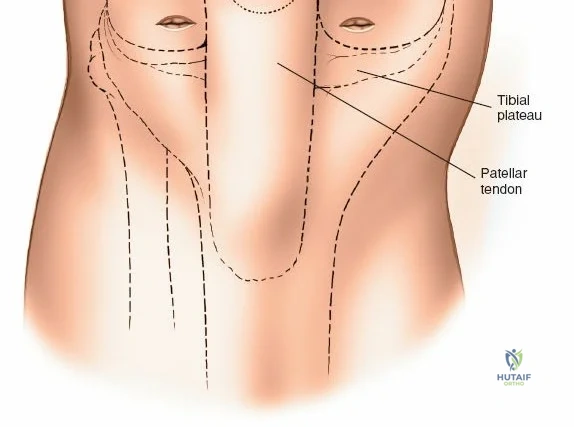
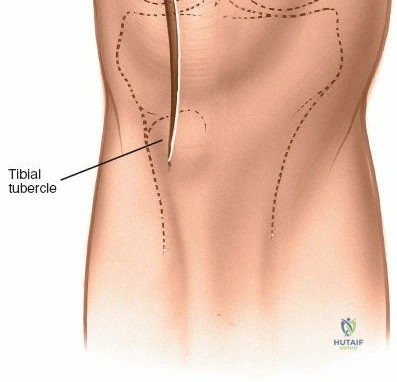
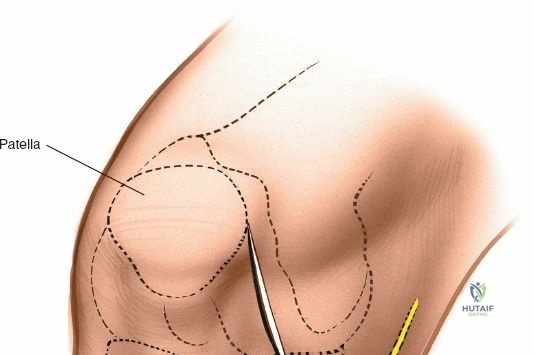
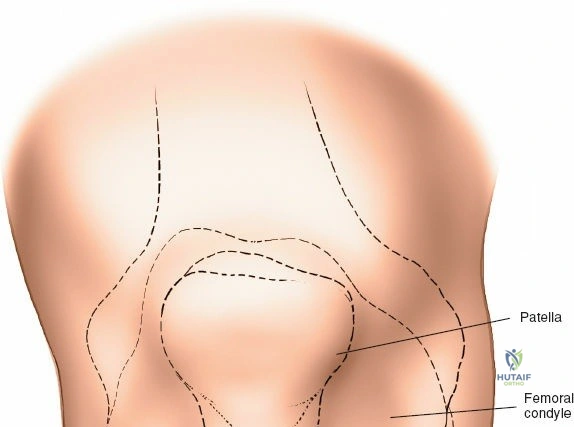
Accurate identification of surface landmarks is critical to avoid iatrogenic injury to the articular cartilage and menisci during portal placement. The primary landmarks include the inferior pole of the patella, the medial and lateral borders of the patellar tendon, and the medial and lateral joint lines. To locate the lateral joint line, the surgeon flexes and extends the knee while palpating with the thumb. Moving the thumb toward the midline reveals the resistance of the lateral edge of the patellar tendon. With the knee flexed to 90 degrees, a distinct recess is palpable between the lateral border of the patellar tendon and the lateral femoral condyle—this is the "soft spot."
The anterolateral portal, the workhorse portal for diagnostic viewing, is established by making an 8-mm transverse or vertical stab incision in this soft spot, approximately 1 cm to 1.5 cm above the lateral joint line and 5 mm lateral to the patellar tendon. Placing the portal too low endangers the anterior horn of the lateral meniscus, while placing it too close to the tendon risks damage to the infrapatellar fat pad, which can obscure visualization. The anteromedial portal is established in a similar fashion on the medial side. The surgeon palpates the medial joint line and the medial edge of the patellar tendon, creating an incision in the medial soft spot. This portal is primarily used for instrument insertion, though the arthroscope and instruments can be freely interchanged between the two portals depending on the compartment being addressed.
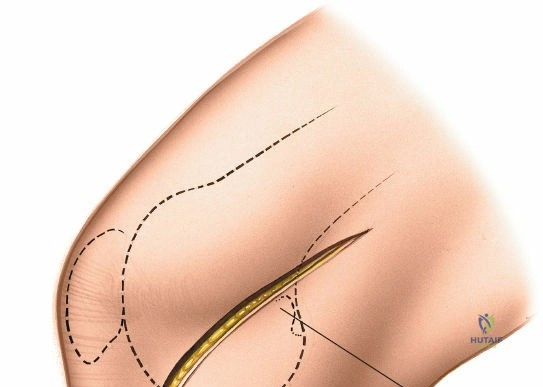
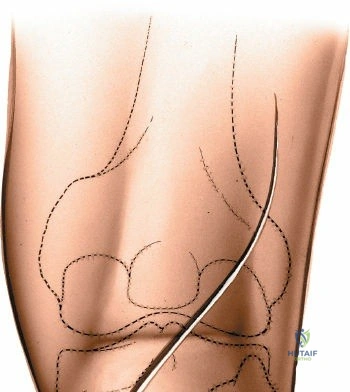
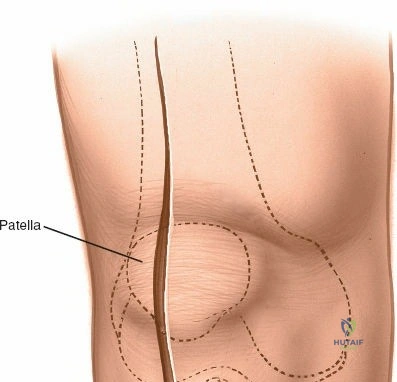
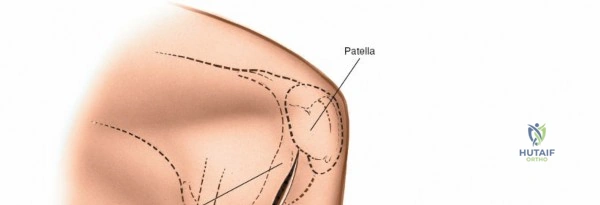
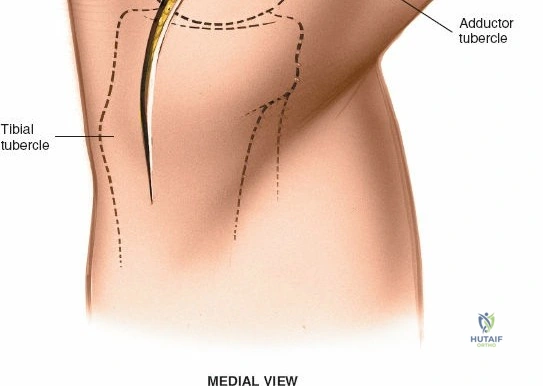
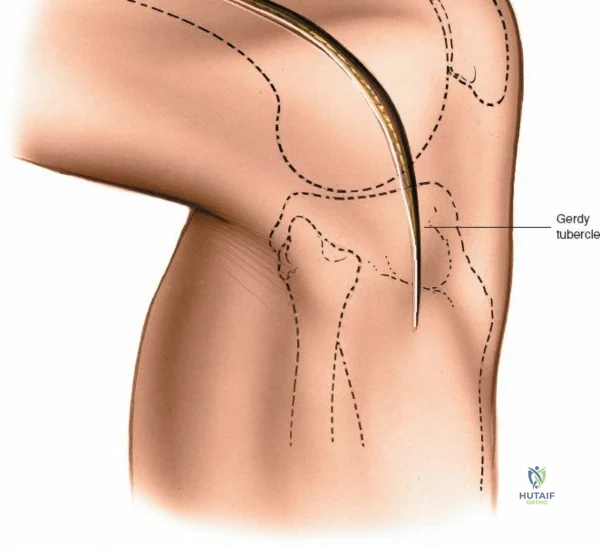
For open medial approaches, the landmarks include the medial epicondyle, the adductor tubercle, the joint line, and the pes anserinus insertion on the anteromedial proximal tibia. The incision for a direct medial approach typically begins slightly proximal to the medial epicondyle and extends distally, curving gently anteriorly toward the pes anserinus. This trajectory follows the anatomic course of the sMCL and allows for extensile exposure of both the femoral and tibial attachments while minimizing the risk of intersecting the saphenous nerve at a perpendicular angle.
Step-by-Step Surgical Approach and Fixation Technique
Arthroscopic Portal Placement and Dissection
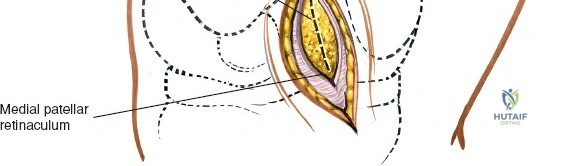
The anterolateral and anteromedial portals are the foundation of knee arthroscopy. There is no true internervous plane in these surgical approaches, as they consist of incisions made directly through the medial and lateral patellar retinacula and the underlying joint capsule. Fortunately, no major nerves are present in these immediate paratendinous areas. With the knee flexed to 90 degrees, the anterolateral skin incision is deepened using a sharp #11 blade. The blade is directed toward the intercondylar notch to avoid scoring the articular cartilage of the femoral condyles. As the retinaculum and capsule are incised, a sudden decrease in resistance is felt, indicating entry into the joint space.
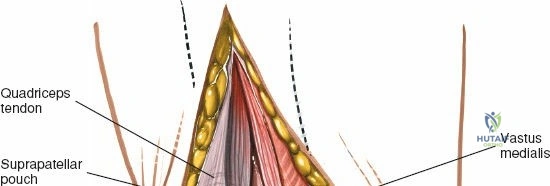
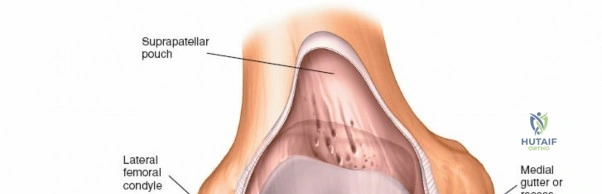
The scalpel is withdrawn, and the arthroscopic sheath equipped with a blunt trochar is inserted. The sheath is pushed into the anterolateral portion of the knee, aiming toward the notch. Once inside the joint, the surgeon carefully extends the knee while advancing the sheath superiorly into the suprapatellar pouch. This maneuver prevents the trochar from scraping the trochlear cartilage. The blunt trochar is then removed, and the 30-degree arthroscope is inserted. It is imperative to switch on the irrigation fluid before activating the high-intensity light source; the fluid provides necessary distension and cools the tip of the scope, preventing thermal necrosis of the delicate synovial lining.
The anteromedial portal is typically established under direct intra-articular visualization. The arthroscope is positioned in the intercondylar notch looking medially. A spinal needle is inserted through the planned anteromedial portal site. The trajectory of the needle is observed to ensure it clears the medial meniscus and provides an appropriate angle of attack for the intended pathology (e.g., reaching the posterior horn of the medial meniscus). Once the optimal position is confirmed, a stab incision is made, and the arthroscopic instruments are introduced.
Diagnostic Arthroscopy and Order of Scoping
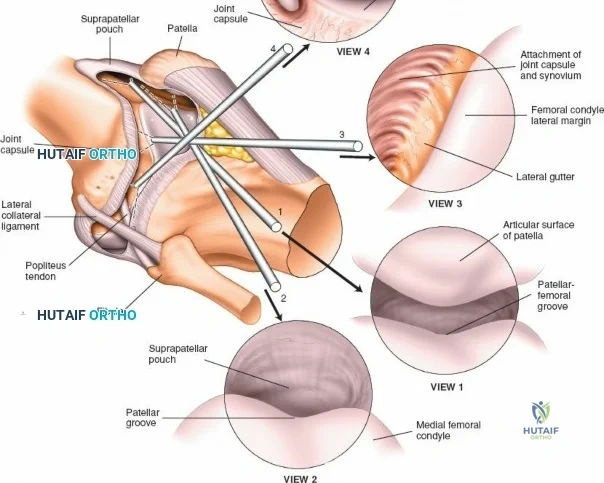
A systematic diagnostic sweep is mandatory to ensure that no concomitant pathology is missed. The standard order of scoping begins with the 30-degree arthroscope in the suprapatellar pouch (View 1). The surgeon examines the synovial lining for hypertrophy, plicae, or loose bodies. Keeping the knee fully extended, the scope is withdrawn into the patellofemoral joint (View 2). By rotating the light cord and manipulating the patella medially and laterally, the surgeon evaluates the articular cartilage of the patellar facets and the trochlear groove for chondromalacia or osteochondral defects.

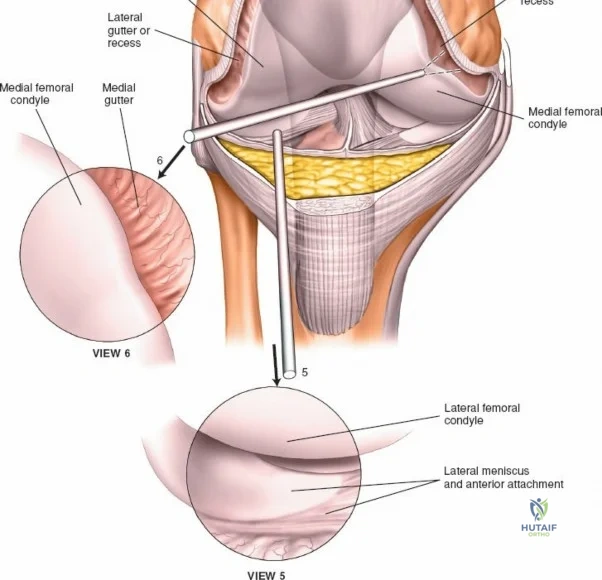
Next, the tip of the arthroscope is swept laterally into the lateral gutter, passing between the lateral femoral condyle and the lateral capsule (View 3). This recess is inspected for loose bodies. The scope is advanced inferiorly along the gutter to visualize the popliteal hiatus and the intra-articular portion of the popliteus tendon (View 4). With the knee still extended, the scope is swept across the joint into the lateral compartment to observe the anterior horn of the lateral meniscus (View 5). The scope is then directed medially and rotated to inspect the medial femoral recess and medial gutter (View 6).

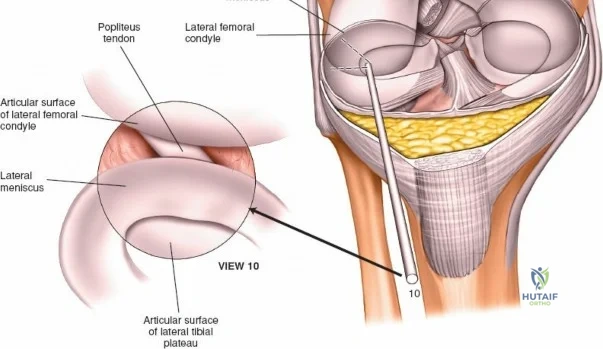
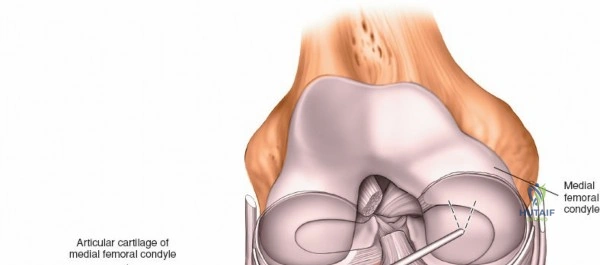
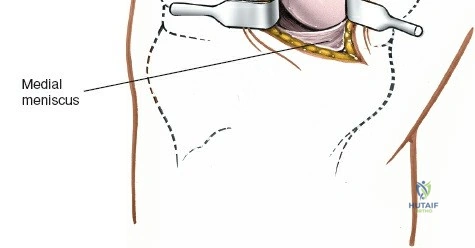
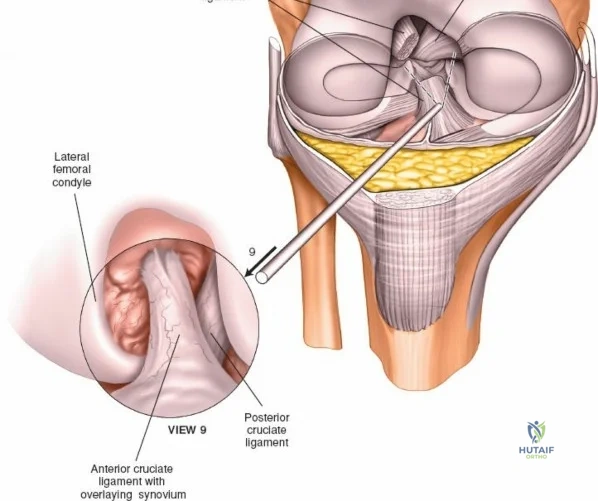
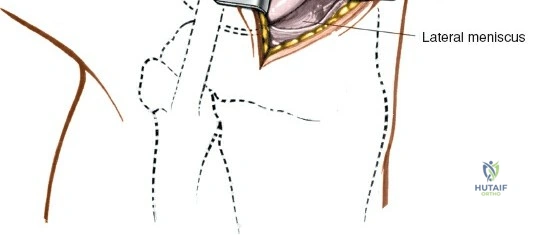
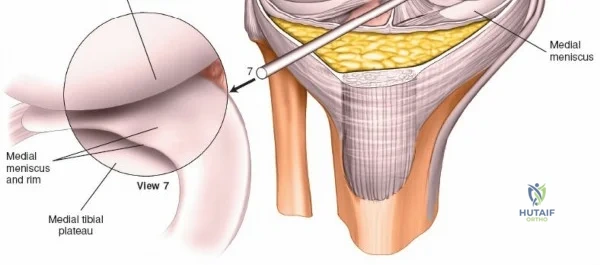
The arthroscope is then withdrawn into the central intercondylar notch, and the knee is flexed to 90 degrees. This allows the scope to enter the medial compartment (View 7). A valgus and external rotation force is applied to open the medial joint space, permitting inspection of the medial meniscus, the medial femoral condyle, and the medial tibial plateau. The scope is then moved back to the notch to evaluate the ACL and PCL (Views 8 and 9). Finally, the knee is placed in the figure-of-four position to open the lateral compartment, allowing visualization of the lateral meniscus and lateral articular surfaces (View 10). An arthroscopic probe, inserted via the anteromedial portal, is used systematically to palpate the menisci, cartilage, and ligaments, assessing their structural integrity.
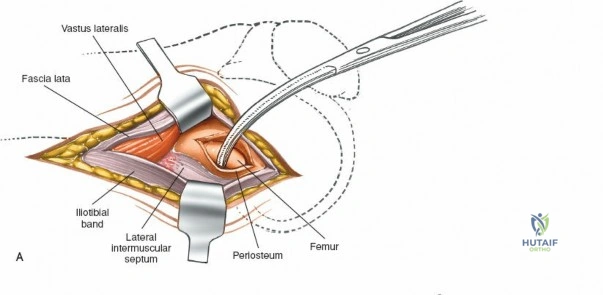
The Direct Medial Approach to the Superficial Medial Ligament
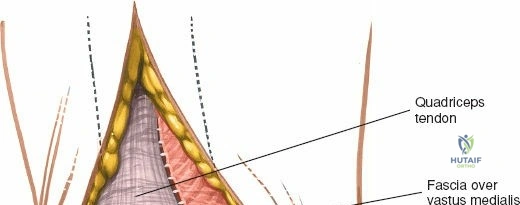
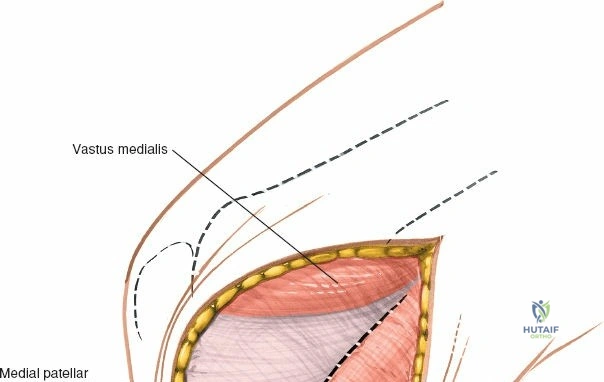
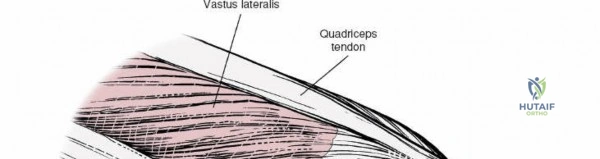
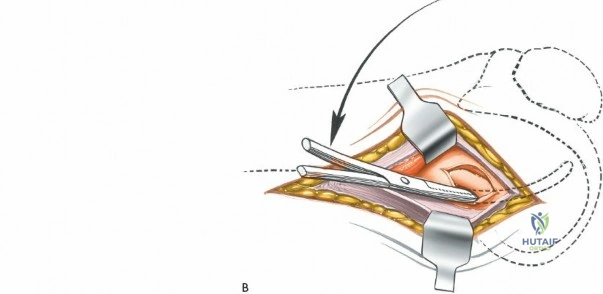
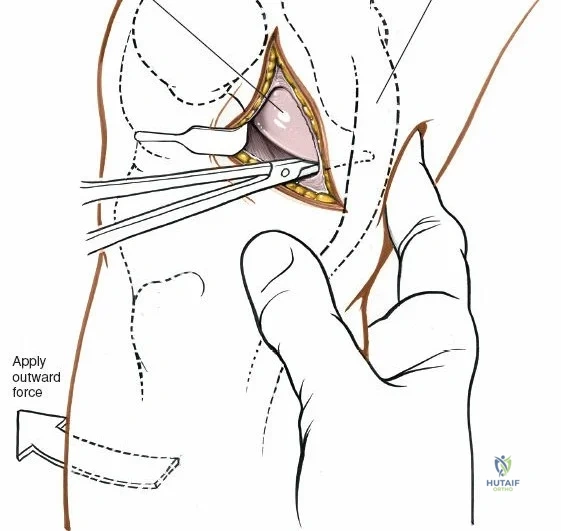
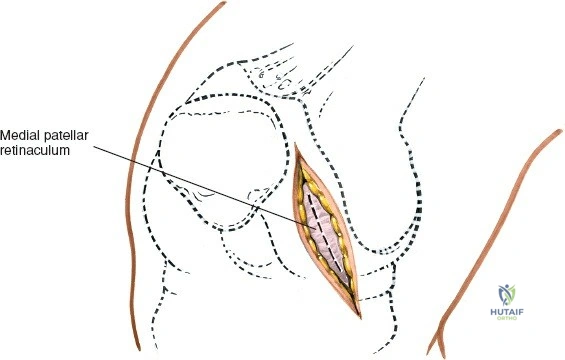
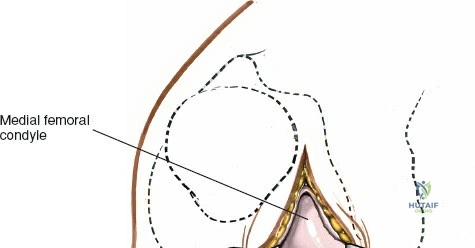
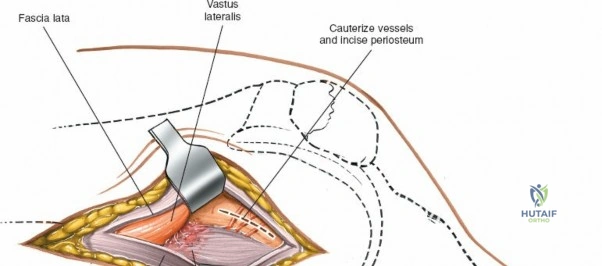
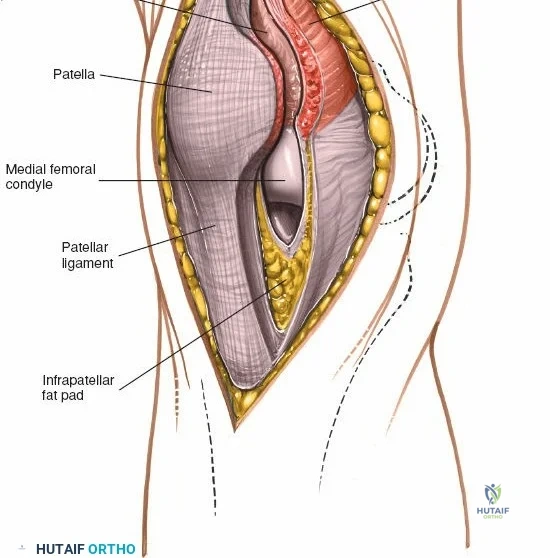
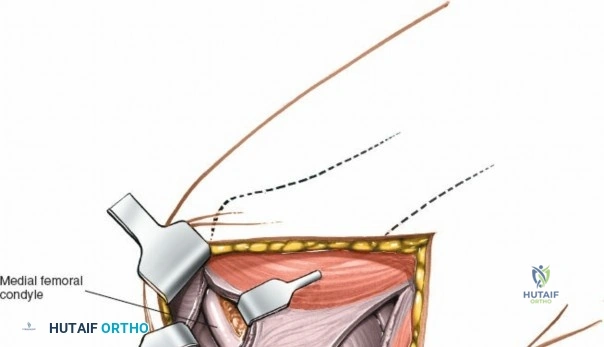
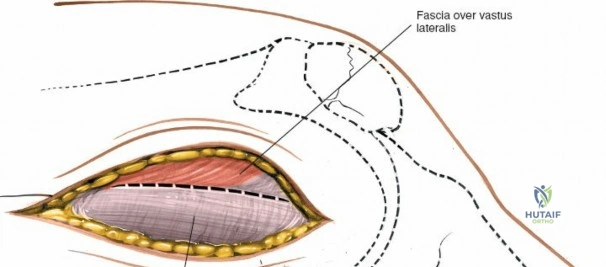
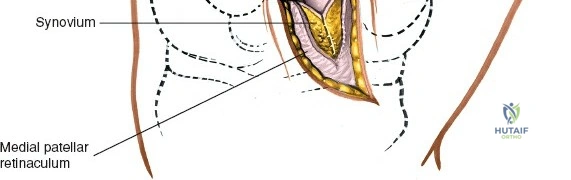
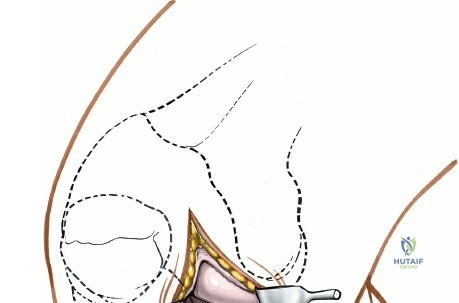
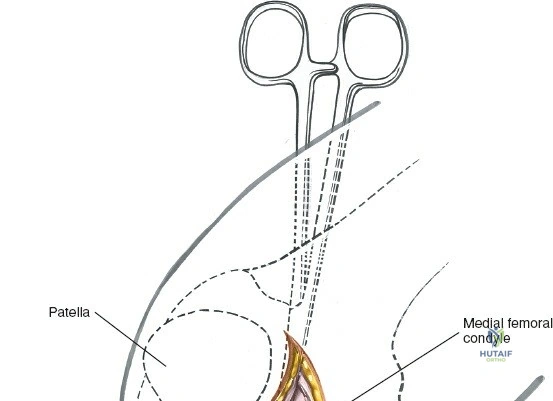
When addressing severe medial-sided trauma, the direct medial approach is utilized. The patient is supine, and the limb is exsanguinated. A longitudinal or slightly curved incision is made starting 2 cm proximal to the medial femoral epicondyle, extending distally across the joint line, and curving anteriorly to end 3-4 cm distal to the joint line at the pes anserinus. The subcutaneous tissue is dissected down to the deep crural fascia (Layer 1). Full-thickness fasciocutaneous flaps are elevated to protect the vascularity of the skin.

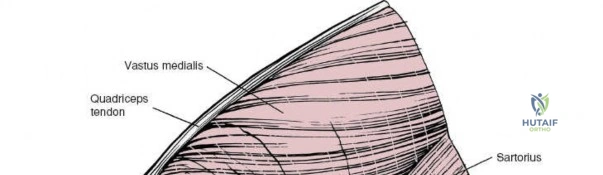
During the distal dissection, extreme vigilance is required to identify and protect the infrapatellar branch of the saphenous nerve, which courses transversely across the proximal tibia. The sartorius fascia is incised longitudinally, anterior to the palpable sMCL. Retracting the pes anserinus tendons posteriorly exposes the entire length of the sMCL (Layer 2). The femoral attachment is identified at the medial epicondyle, and the broad tibial insertion is identified deep to the pes. If a midsubstance tear is present, it is often repaired primarily with heavy non-absorbable sutures and augmented with an internal brace.