Unlocking Every Aspect of the Hip's Surgical Approaches

Key Takeaway
Discover the latest medical recommendations for Unlocking Every Aspect of the Hip's Surgical Approaches. Surgical approaches to the hip include anterior, anterolateral, lateral, posterior, and medial. These techniques provide access to the specific aspect of the hip required for procedures such as total joint replacement, hemiarthroplasty, and tumor surgery. While anterolateral and posterior are common for total hip replacement, the minimally invasive anterior approach is gaining popularity.
Comprehensive Introduction and Patho-Epidemiology
Operations on the hip joint represent some of the most frequently performed and highly successful surgical interventions in the field of modern orthopedics. Total hip arthroplasty (THA) for degenerative joint disease, in particular, has revolutionized the lives of millions of patients, offering profound pain relief and restoration of biomechanical function. Beyond elective arthroplasty, open surgical approaches to the hip joint are strictly required for a myriad of complex indications, including hemiarthroplasties for displaced femoral neck fractures, aggressive oncologic tumor resections, pelvic osteotomies, and the meticulous debridement and treatment of peri-prosthetic joint infections. The selection of the surgical approach is paramount, as it dictates the quality of articular exposure, the extent of soft tissue disruption, and the postoperative rehabilitation trajectory.

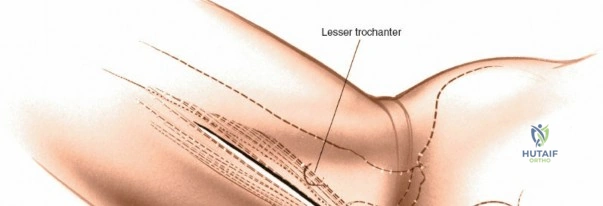
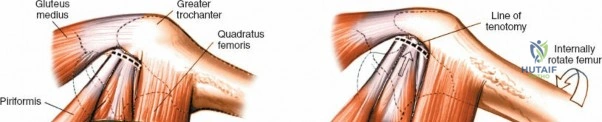
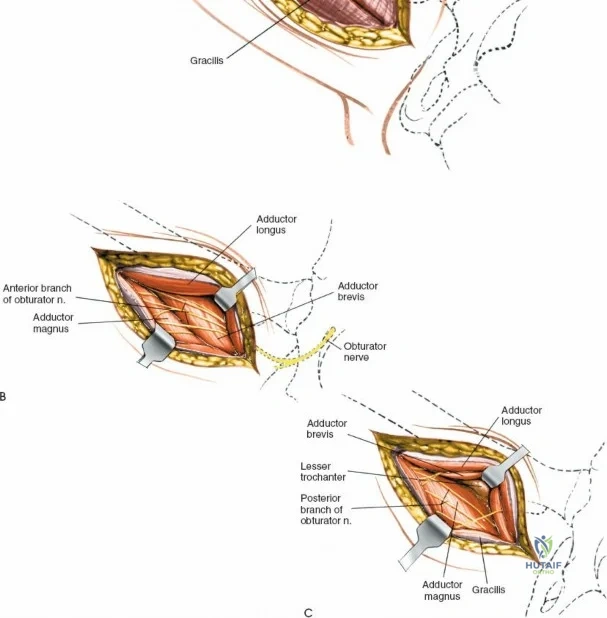
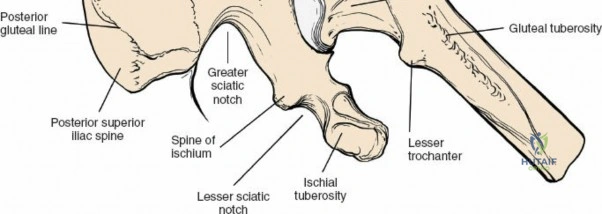
Historically, four fundamental approaches have dominated the orthopedic armamentarium: the anterior, anterolateral, lateral, and posterior approaches. The full anterior approach provides unparalleled access to the pelvis, the anterior column of the acetabulum, and the hip joint itself, exploiting a true internervous and intermuscular plane. The anterolateral approach, historically the workhorse for many arthroplasty surgeons, has numerous variations tailored to specific prosthetic designs and patient anatomies. The posterior approach remains the most universally utilized approach globally for both hemiarthroplasty and THA, lauded for its extensile nature, preservation of the abductor mechanism, and relative ease of execution with minimal assistance. Conversely, the medial approach is highly specialized and rarely utilized, reserved primarily for localized procedures on the lesser trochanter, obturator ring, and surrounding medial osseous structures.

In recent decades, minimally invasive surgical (MIS) approaches to the hip have surged in popularity, driven by patient demand for accelerated recovery and advanced surgical instrumentation. Most of these MIS techniques utilize the classical intermuscular intervals described in foundational anatomical texts but strictly limit the length of the cutaneous incision and the underlying soft tissue dissection. While minimally invasive surgery theoretically mitigates iatrogenic soft tissue trauma, it inherently compromises direct visualization of critical neurovascular and osseous structures. Consequently, these techniques are potentially more hazardous, particularly in obese or highly muscular patients. A profound, three-dimensional understanding of the underlying surgical anatomy is therefore exponentially more critical when executing MIS approaches compared to their traditional, extensile counterparts.
The epidemiological burden of hip pathology continues to escalate with an aging global population and rising rates of obesity. Osteoarthritis remains the leading indication for surgical intervention, followed closely by avascular necrosis, inflammatory arthropathies, and post-traumatic degenerative changes. As the demographic of patients undergoing hip surgery shifts toward both younger, highly active individuals demanding high-performance outcomes, and older, frail patients requiring rapid mobilization to prevent systemic complications, the surgeon's mastery of various hip approaches becomes critical. The ability to seamlessly transition from a minimally invasive anterior approach to an extensile pelvic exposure dictates the surgeon's capacity to manage complex primary cases, severe deformities, and catastrophic intraoperative complications.
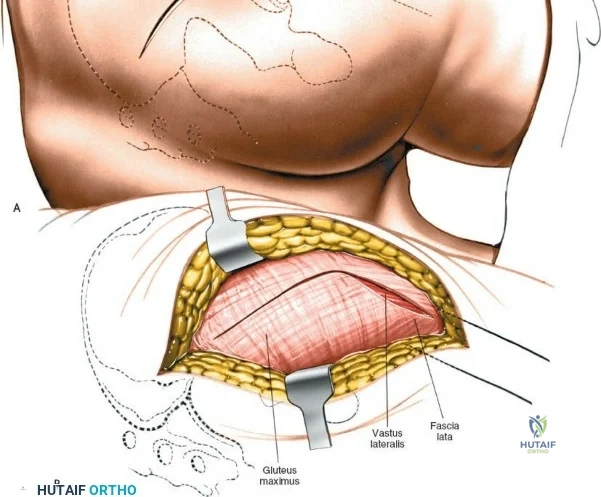
Detailed Surgical Anatomy and Biomechanics
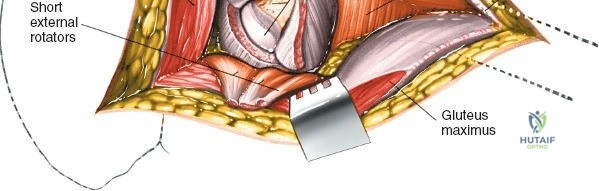
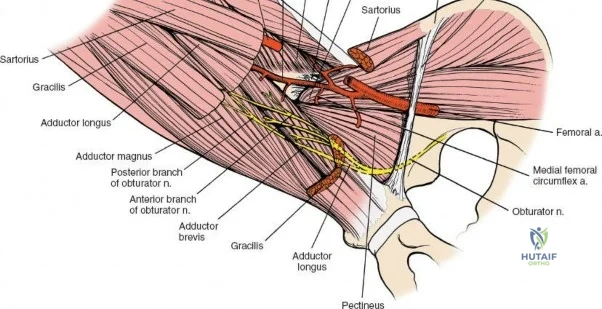
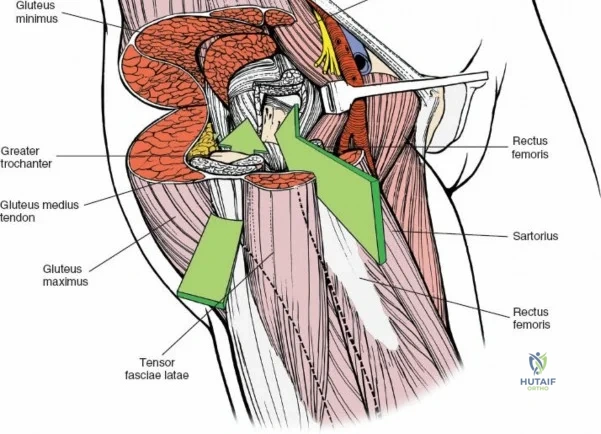
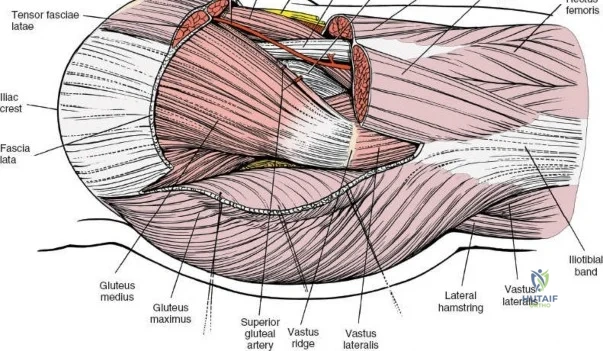
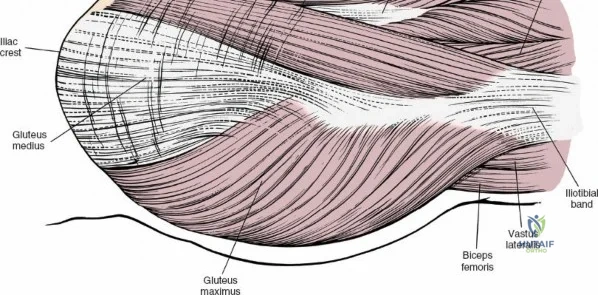
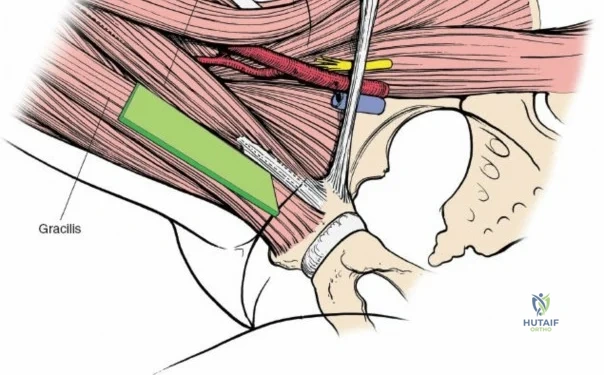
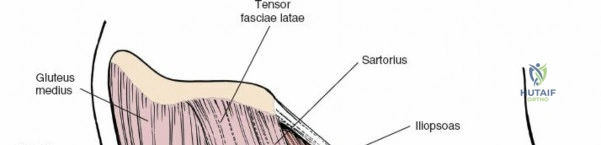
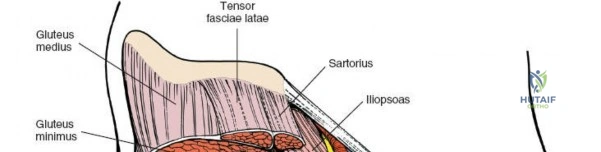
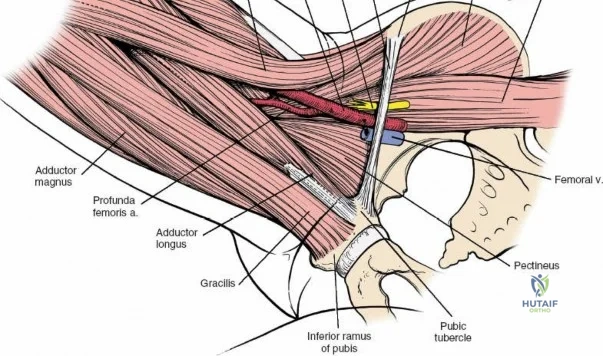
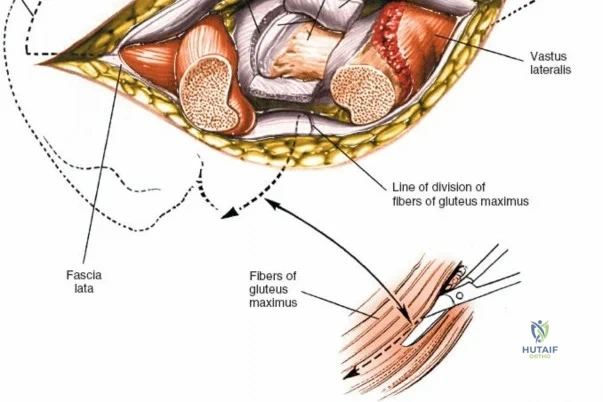
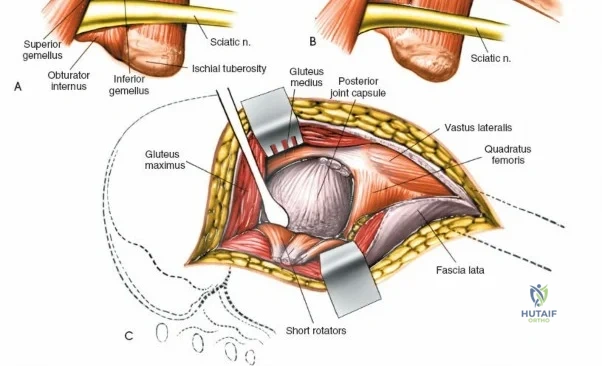
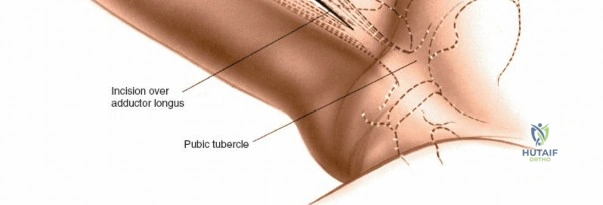
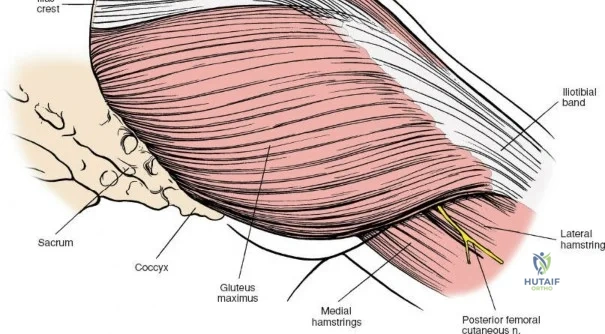
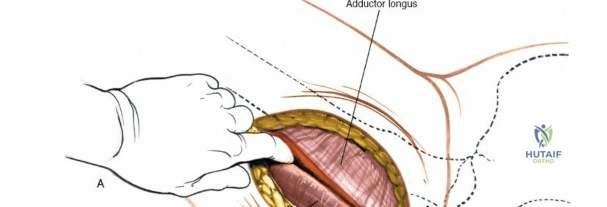
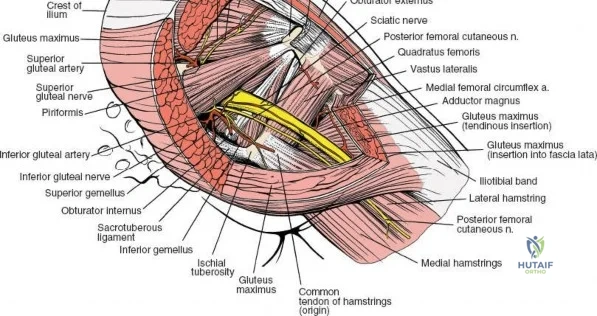
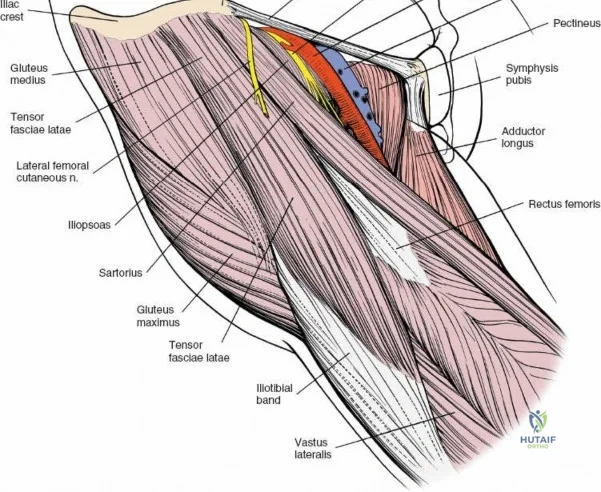
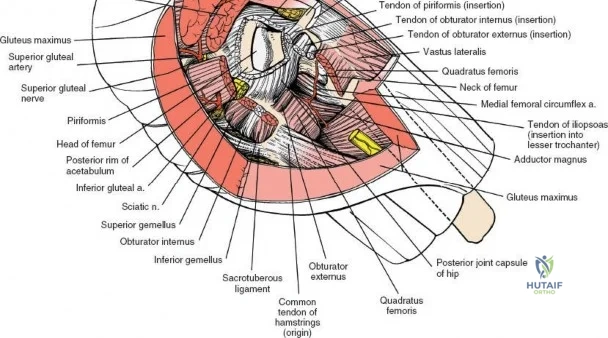
A rigorous comprehension of the intermuscular and internervous intervals surrounding the hip joint is the absolute foundation of safe orthopedic surgery. The four basic approaches to the hip strategically exploit these muscular intervals to minimize iatrogenic denervation and devascularization. The anterior approach utilizes the interval between the sartorius (innervated by the femoral nerve) and the tensor fasciae latae (innervated by the superior gluteal nerve). The anterolateral approach navigates the interval between the tensor fasciae latae and the gluteus medius (both innervated by the superior gluteal nerve, making this an intermuscular, but not internervous, plane). The posterior approach gains access either by splitting the gluteus maximus (inferior gluteal nerve) or by developing the interval between the gluteus medius and the gluteus maximus. Finally, the medial approach exploits the interval between the adductor longus (obturator nerve) and the gracilis (obturator nerve).
Superficial Anatomical Landmarks
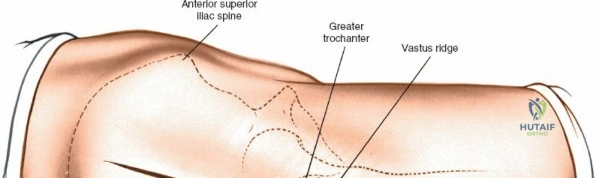
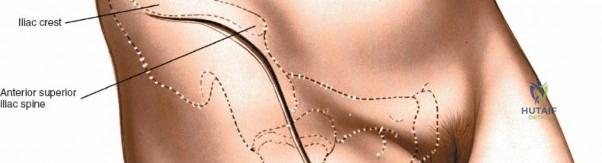
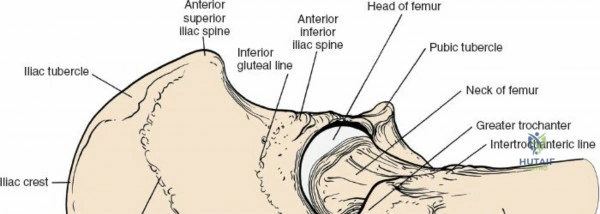
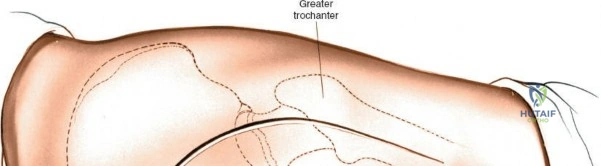
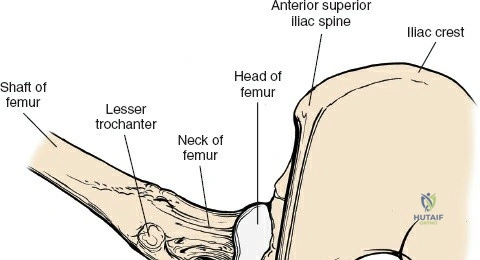
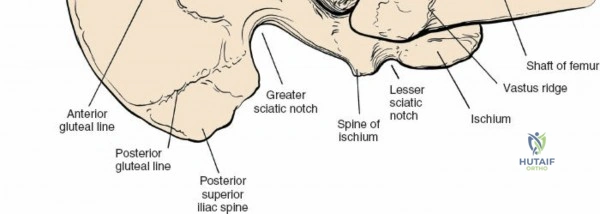
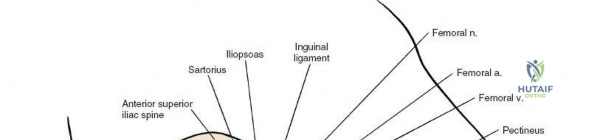
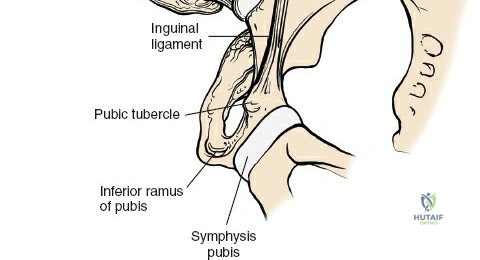
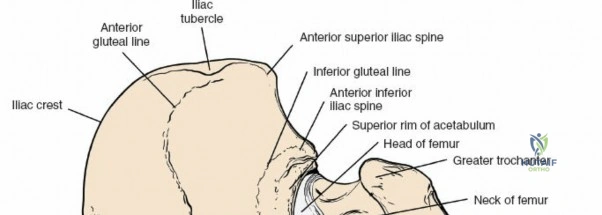
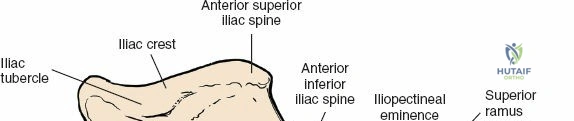
For the anterior approach, precise identification of superficial bony landmarks is mandatory for correct incision placement and orientation. The anterior superior iliac spine (ASIS) is subcutaneous and easily palpable in asthenic patients; however, in the obese demographic, it is often obscured by a dense layer of adipose tissue. Surgeons can locate it most reliably by palpating superiorly from beneath the bony protuberance of the anterior ilium. The iliac crest, extending posteriorly from the ASIS, remains strictly subcutaneous and serves as a critical point of origin and insertion for the abdominal and pelvic musculature. Because no muscles cross over the bony crest itself, it remains consistently available for palpation and serves as a reliable guide for extending the approach proximally during complex pelvic reconstructions.
Deep Muscular and Neurovascular Anatomy
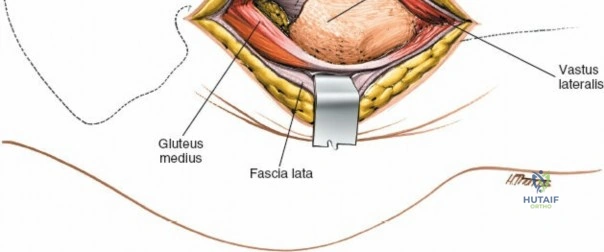
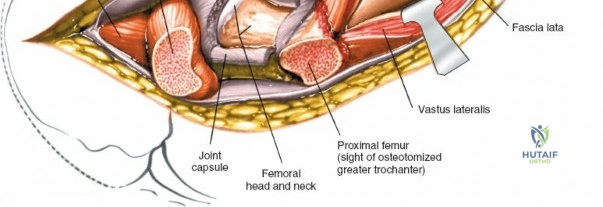
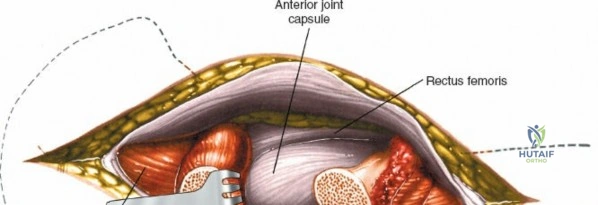
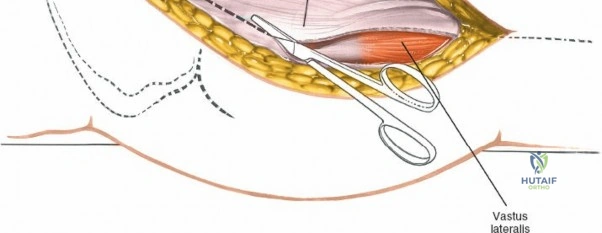
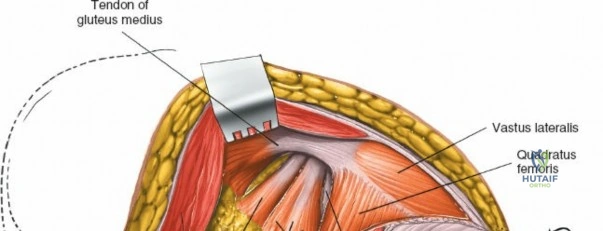
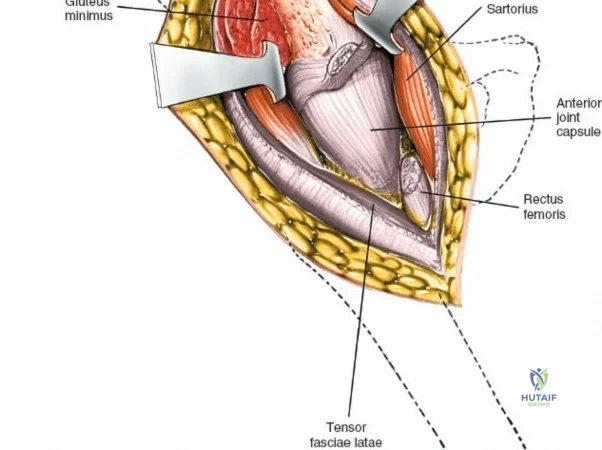
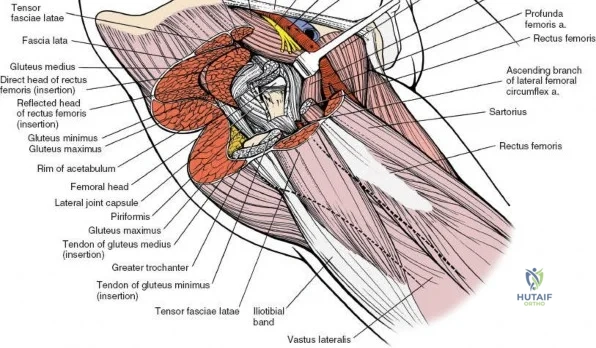
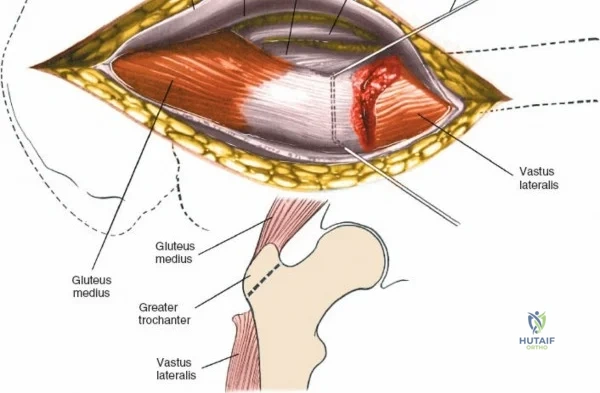
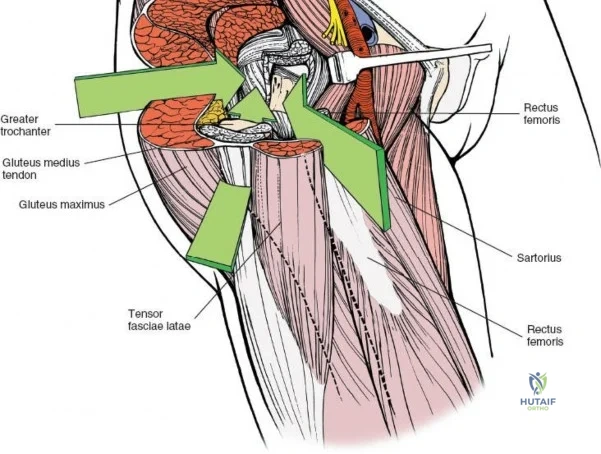
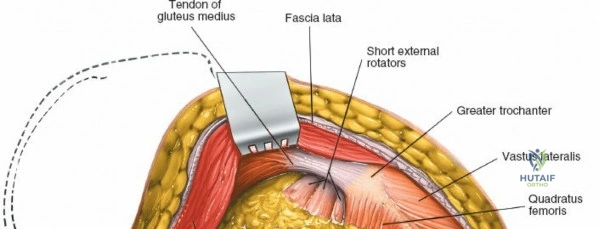
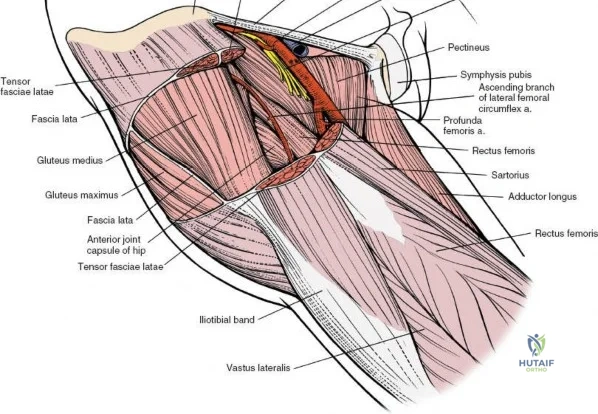
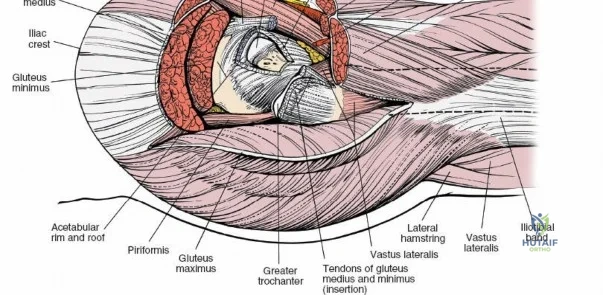
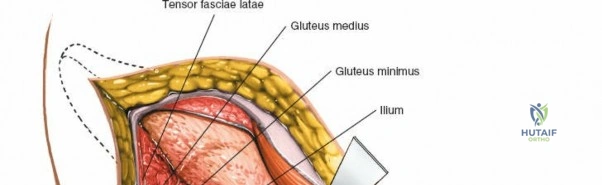
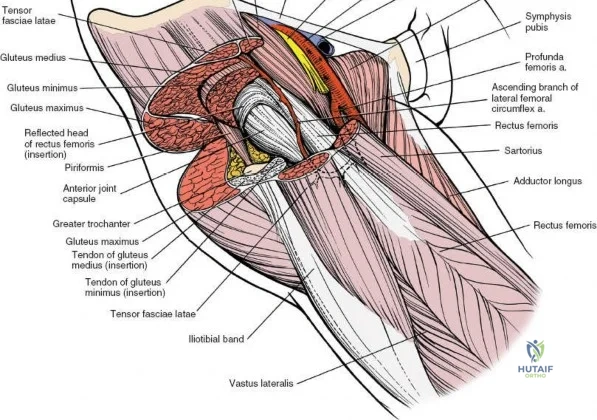
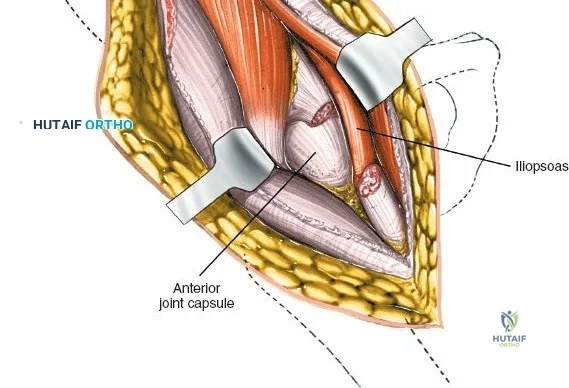
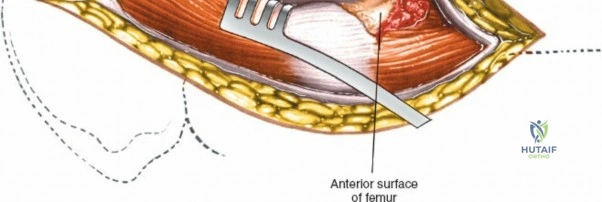
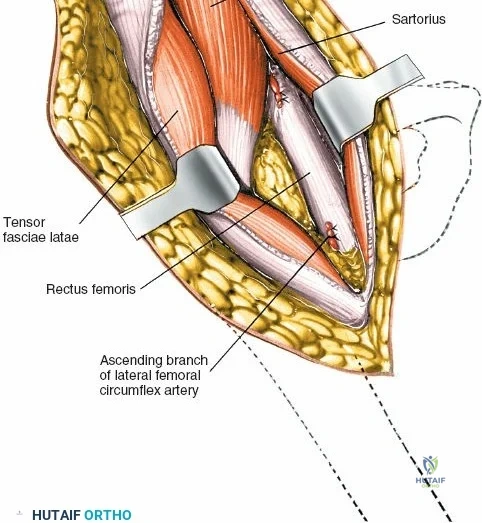
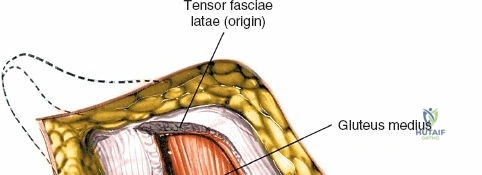
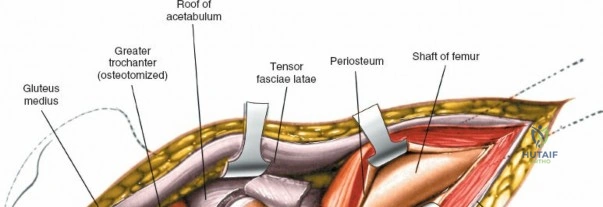
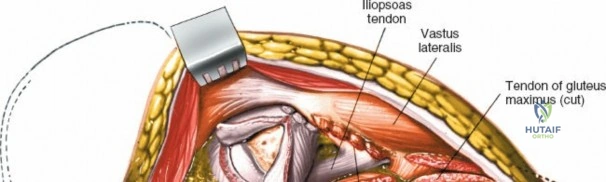
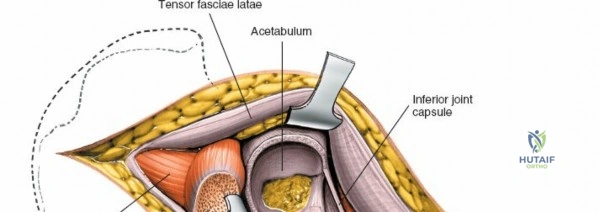
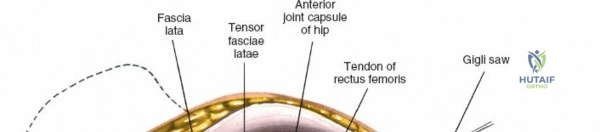
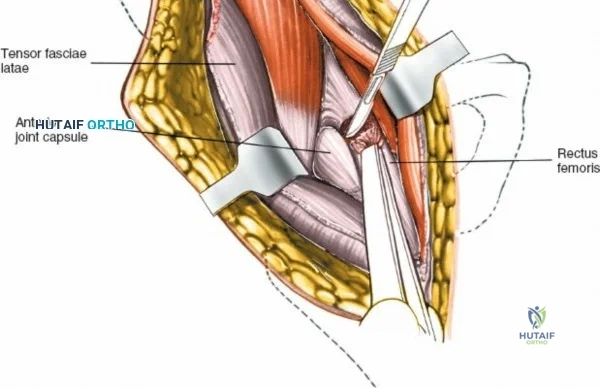
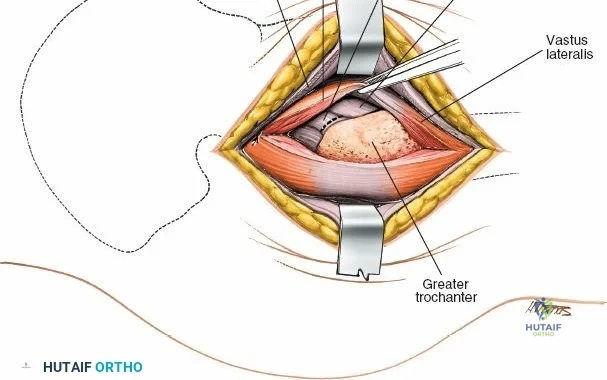
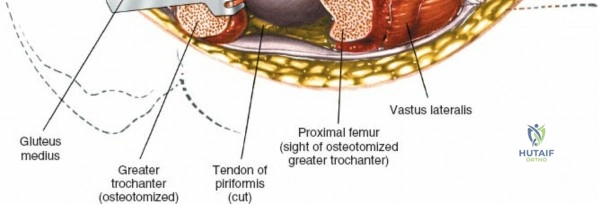
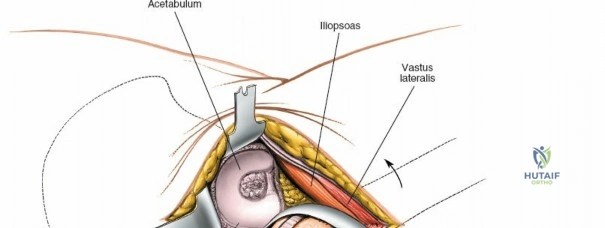
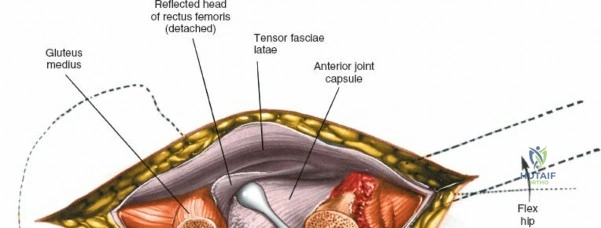
The deep surgical dissection of the anterior approach reveals a secondary, deeper internervous plane that must be respected. This deeper interval lies between the rectus femoris (femoral nerve) medially and the gluteus medius (superior gluteal nerve) laterally. The rectus femoris possesses a complex origin consisting of two distinct heads: the direct head, which originates from the anterior inferior iliac spine (AIIS), and the reflected head, which originates from the superior lip of the acetabulum and the anterior capsule of the hip joint. The reflected head is intimately blended with the capsular tissue, rendering dissection between the two structures technically demanding. Inferolaterally, the proximal shaft of the femur lies deep to the vastus lateralis, which must be carefully elevated or split if distal extension of the approach is required.

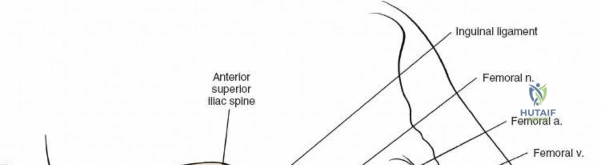
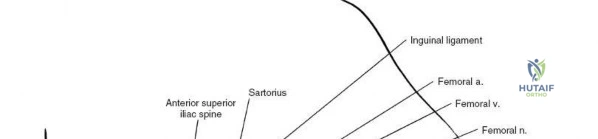
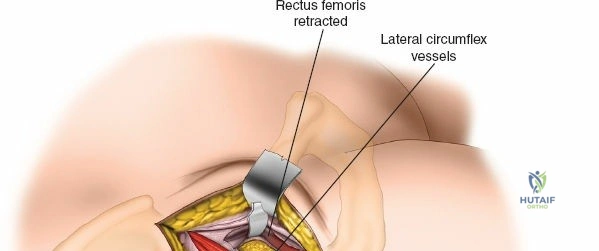
Neurovascular structures present significant hazards during the anterior approach. The lateral femoral cutaneous nerve (LFCN) is highly variable; it reaches the anterior thigh by passing over, under, or directly through the inguinal ligament, typically medial to the ASIS. It frequently courses over the fascia of the sartorius muscle. The surgeon must remain vigilant, as the nerve may arborize into multiple branches immediately distal to the inguinal ligament. Deeper in the surgical field, the ascending branch of the lateral femoral circumflex artery transverses the operative field, crossing the gap between the tensor fasciae latae and the sartorius/rectus femoris just distal to the intertrochanteric line. This vessel must be meticulously identified, isolated, and ligated or electrocoagulated to prevent robust postoperative hematoma formation. The femoral nerve and artery lie well medial to the operative field within the femoral triangle and are generally protected as long as the surgeon remains lateral to the sartorius.
Exhaustive Indications and Contraindications
The decision to utilize a specific surgical approach to the hip is multifactorial, depending heavily on the underlying pathology, the patient's anatomical habitus, the specific implant system being utilized, and the surgeon's training and comfort level. The anterior approach (Smith-Petersen or Hueter interval) is exceptionally versatile. It is primarily indicated for primary total hip arthroplasty, hemiarthroplasty for femoral neck fractures, synovial biopsies, intra-articular fusions, and the excision of benign or malignant tumors of the anterior pelvis and hip joint. Furthermore, the proximal extension of this approach provides excellent exposure for complex peri-acetabular osteotomies (e.g., Ganz osteotomy) used in the treatment of developmental dysplasia of the hip (DDH).
Despite its advantages, the anterior approach is not universally applicable. Absolute contraindications are rare but may include active cutaneous infection over the anterior groin or severe anatomical distortion that precludes safe identification of neurovascular landmarks. Relative contraindications are more common and include massive posterior column acetabular defects requiring structural allografting or plating, as the anterior approach offers limited to no visualization of the posterior acetabular wall. Additionally, in patients with severe, rigid external rotation contractures, dislocating the hip anteriorly can be exceedingly difficult and places the femur at high risk for iatrogenic spiral fracturing.
Patient morphology plays a critical role in approach selection. While the anterior approach is often touted as muscle-sparing, performing it on a morbidly obese patient with a large, overhanging abdominal pannus significantly increases the risk of wound maceration, delayed healing, and deep periprosthetic joint infection. In such cases, a lateral or posterior approach may be safer from a soft-tissue envelope perspective. Conversely, highly muscular individuals with hypertrophic tensor fasciae latae and rectus femoris muscles can present significant retraction challenges during the anterior approach, necessitating meticulous release of the rectus origin to prevent muscle tearing and neuropraxia of the femoral nerve.
| Approach Type | Primary Indications | Relative Contraindications | Key Advantages |
|---|---|---|---|
| Anterior (Smith-Petersen) | Primary THA, Pelvic Osteotomy, Synovial Biopsy, Anterior column tumors | Severe obesity (large pannus), Posterior acetabular defects, Complex revision THA | True internervous plane, supine positioning, easy fluoroscopic integration |
| Posterior (Moore/Southern) | Primary/Revision THA, Posterior wall/column fractures, Hemiarthroplasty | Severe hip flexion contractures (relative) | Extensile, excellent femoral exposure, preserves abductor mechanism |
| Anterolateral (Watson-Jones) | Primary THA, Open reduction of femoral neck fractures | Severe abductor deficiency | Excellent acetabular exposure, lower dislocation rate than posterior |
| Lateral (Hardinge) | Primary THA, Trochanteric fractures, DDH | Pre-existing abductor weakness, risk of postoperative limp | Direct visualization of acetabulum, versatile for complex femurs |
Pre-Operative Planning, Templating, and Patient Positioning
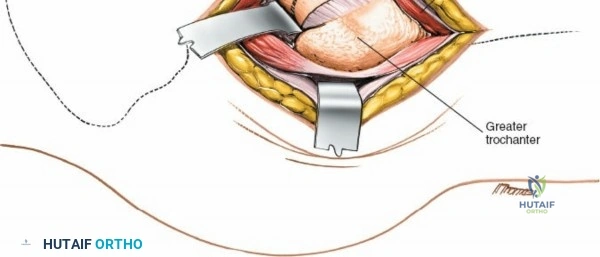
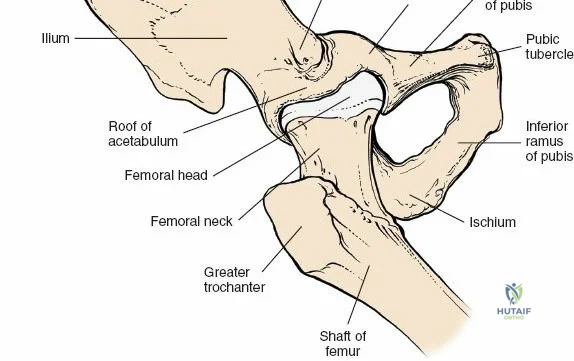
Thorough preoperative planning and digital templating are non-negotiable prerequisites for any surgical approach to the hip. High-quality, properly scaled anteroposterior (AP) pelvis and cross-table lateral radiographs are mandatory. The surgeon must template the anticipated center of rotation, carefully calculating the required offset and leg length restoration. For the anterior approach, templating helps anticipate the necessary depth of acetabular reaming and the specific femoral neck cut angle required to facilitate extraction of the femoral head without causing iatrogenic damage to the greater trochanter or the anterior acetabular rim.
Patient Positioning and Operating Table Selection
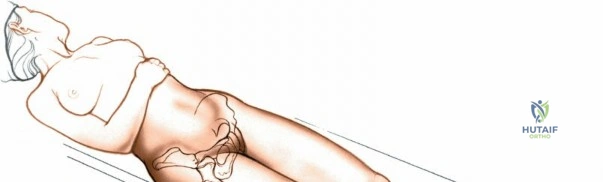
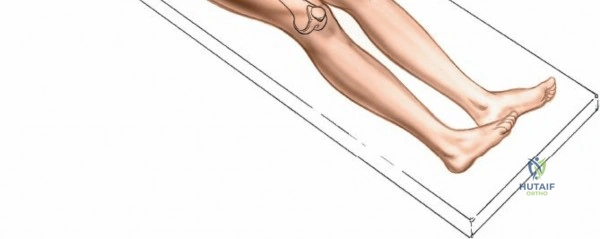
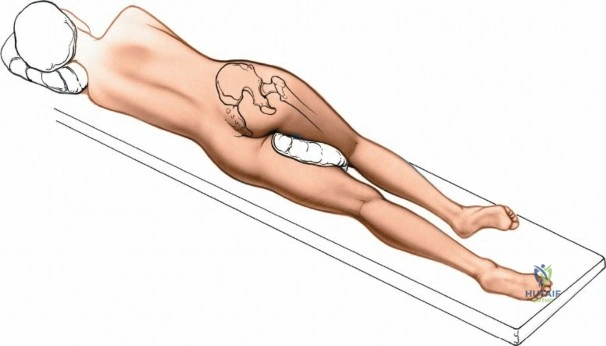
Positioning for the anterior approach depends on surgeon preference and institutional equipment availability. The patient is universally placed in the supine position. Many surgeons prefer a specialized orthopedic traction table (e.g., the Hana® or PROfx® table), which allows for independent manipulation of the operative leg, including precise control of traction, hyperextension, and external rotation. This specialized table facilitates femoral exposure by dropping the leg into extension, thereby relaxing the anterior soft tissues and allowing the proximal femur to be elevated via a specialized hook. Alternatively, the procedure can be performed on a standard radiolucent flat table. When using a flat table, the table is often broken at the level of the hip joint to allow for hyperextension, and the operative leg is prepped free to allow for manual manipulation by a dedicated assistant.
Draping and Intraoperative Imaging Setup
Meticulous draping is critical, particularly in obese patients. If an abdominal pannus is present, it must be retracted superiorly and medially using heavy adhesive tape or an Ioban drape to ensure the surgical field remains sterile and the incision site is not compromised by overhanging tissue. The ASIS, iliac crest, and greater trochanter must be easily palpable through the drapes. One of the primary advantages of the anterior approach in the supine position is the seamless integration of intraoperative fluoroscopy. The C-arm can be brought in from the contralateral side, allowing the surgeon to assess acetabular component positioning (inclination and anteversion), femoral broach sizing, and leg length/offset restoration in real-time without altering the patient's position.
Step-by-Step Surgical Approach and Fixation Technique
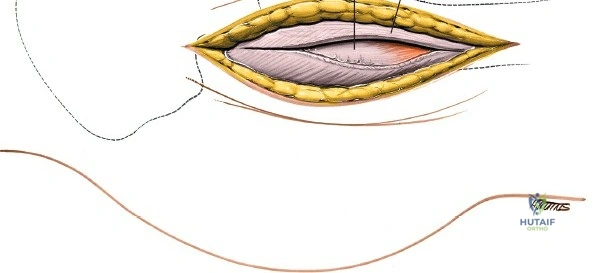
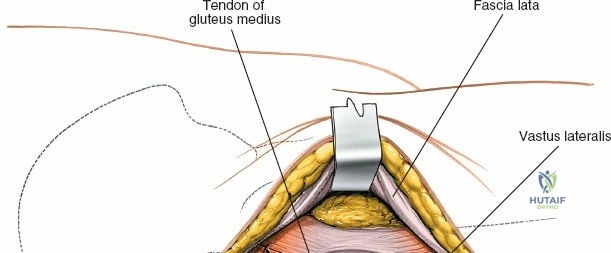
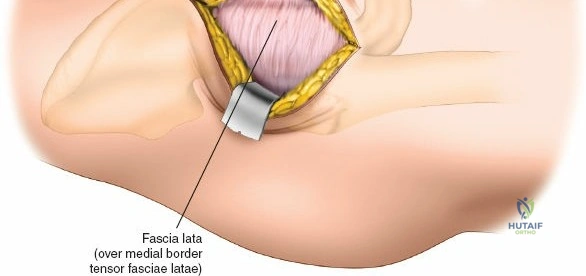
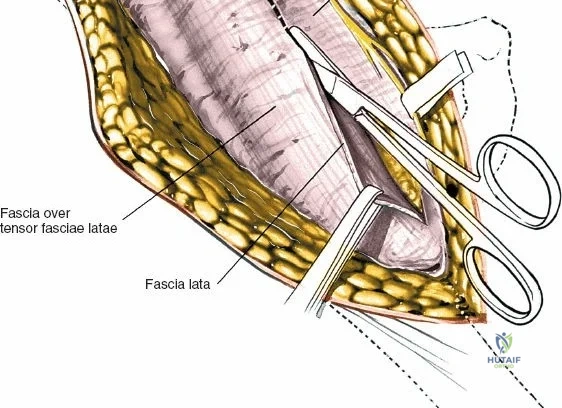
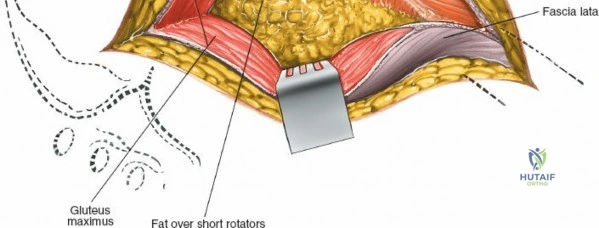
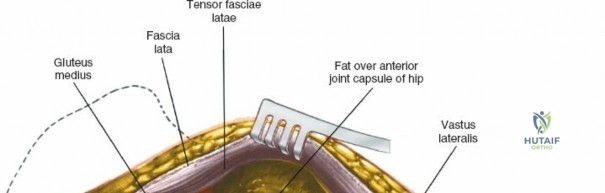
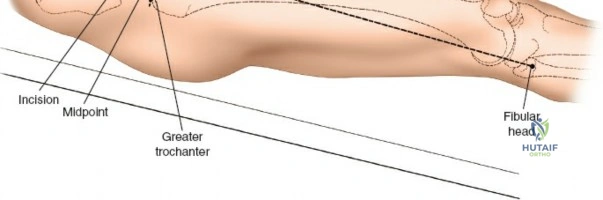
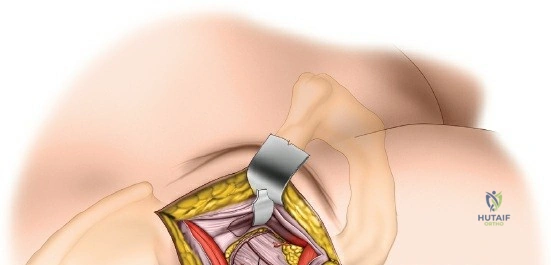
The surgical execution of the anterior approach demands a meticulous, layered dissection to protect vital neurovascular structures while achieving adequate osseous exposure. The skin incision typically begins approximately 2 to 3 centimeters distal and lateral to the ASIS. It extends distally and slightly laterally for 8 to 12 centimeters, aiming toward the lateral aspect of the patella or the fibular head. In minimally invasive variations, the incision is kept as short as 6 centimeters, though the surgeon must never compromise visualization for cosmesis. The subcutaneous fat is divided sharply down to the level of the deep fascia (fascia lata).

Superficial Dissection and LFCN Protection
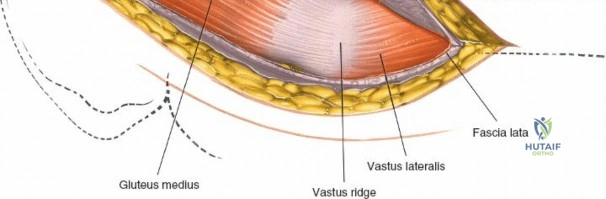
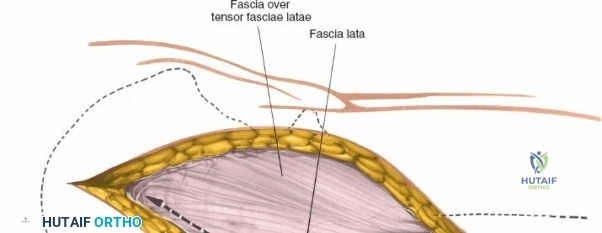
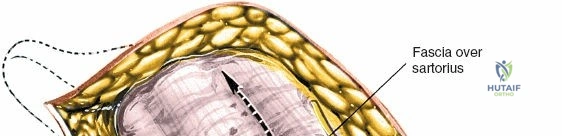
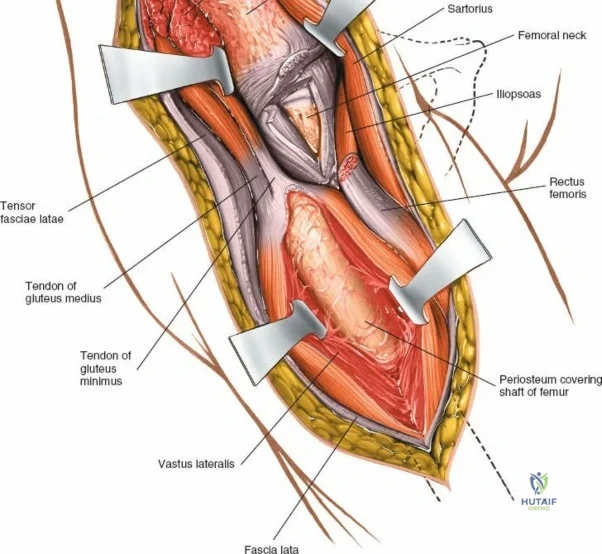
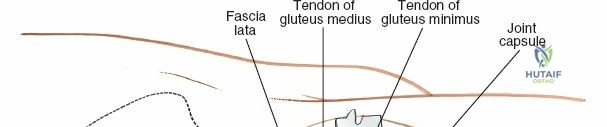
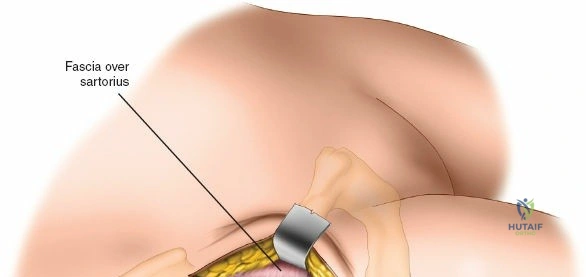
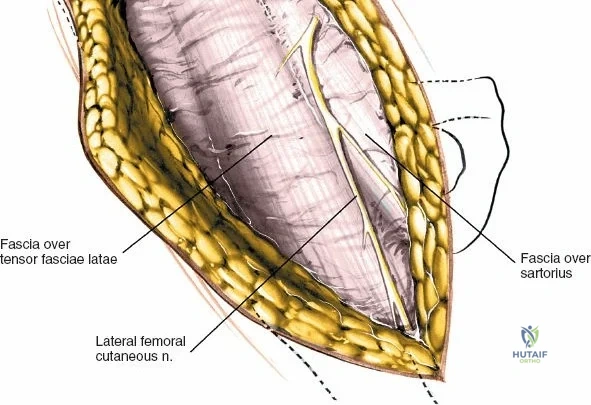
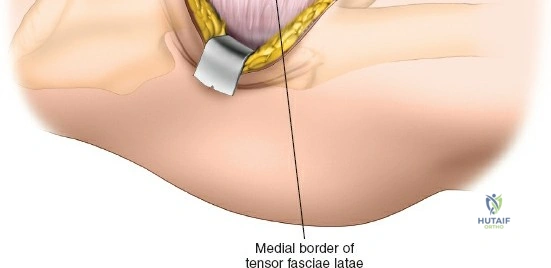
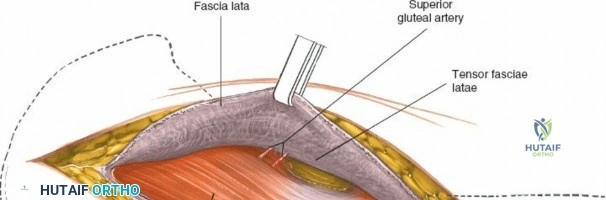
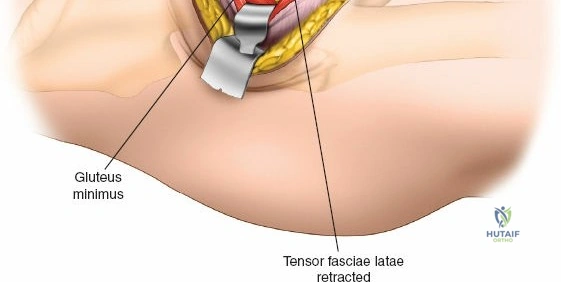
Once the fascia lata is exposed, the surgeon identifies the translucent fascial layer overlying the tensor fasciae latae (TFL) muscle. The fascia is incised longitudinally directly over the medial muscle belly of the TFL. It is a critical technical pearl to incise the fascia over the TFL rather than directly in the internervous interval. By staying within the fascial sheath of the TFL and sweeping the medial fascial flap toward the sartorius, the surgeon inherently protects the lateral femoral cutaneous nerve (LFCN), which typically courses over the fascia of the sartorius. Once the medial edge of the TFL is mobilized, the surgeon retracts the sartorius superiorly and medially, and the TFL inferiorly and laterally, thereby opening the primary superficial internervous plane.
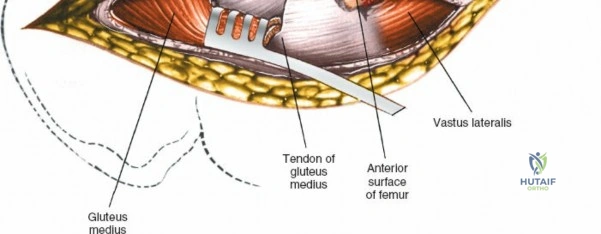
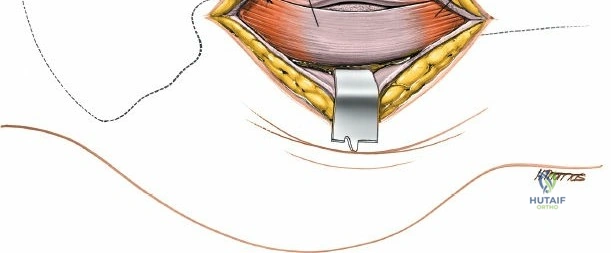
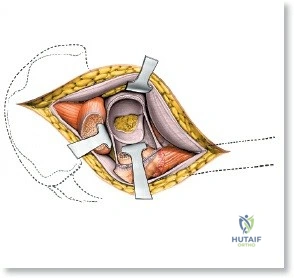
Deep Dissection and Vascular Control
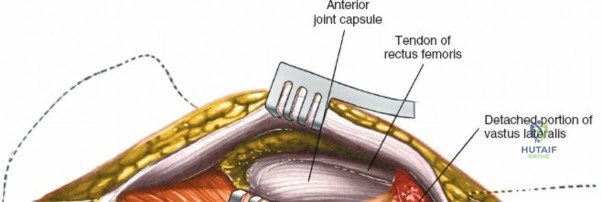
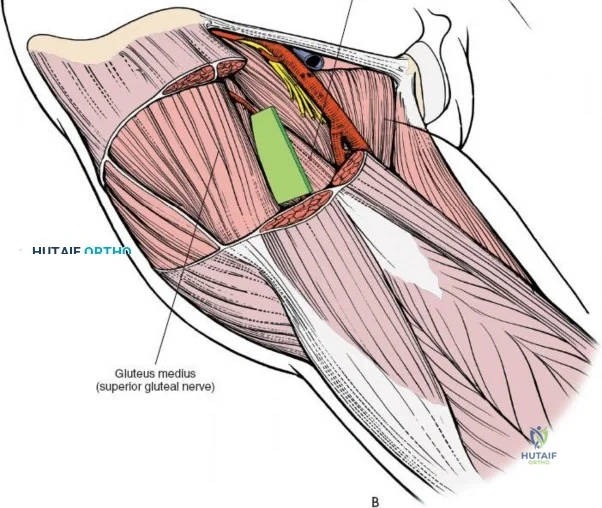
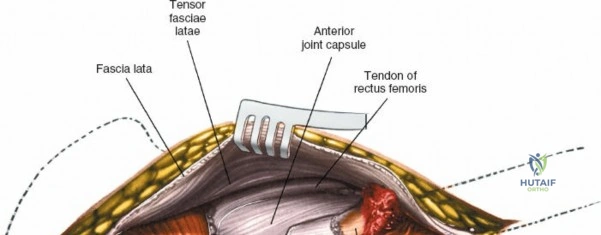
Retracting the superficial muscles exposes the deep layer of musculature: the rectus femoris medially and the gluteus medius laterally. As this deep plane is developed, the surgeon will encounter a leash of vessels crossing the operative field transversely. This is the ascending branch of the lateral femoral circumflex artery and its associated veins. These vessels must be definitively managed; bipolar electrocautery is often insufficient for the larger arterial branches, and formal suture ligation or the use of surgical clips is highly recommended to prevent catastrophic postoperative bleeding. Once the vessels are ligated, the rectus femoris is retracted medially. To enhance exposure, especially of the superior acetabulum, the direct head of the rectus femoris can be released from the AIIS, though many modern MIS techniques aim to preserve this origin.
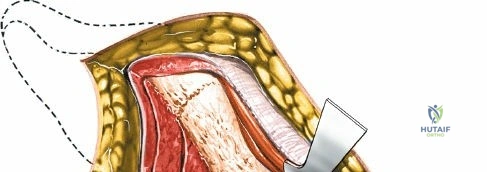
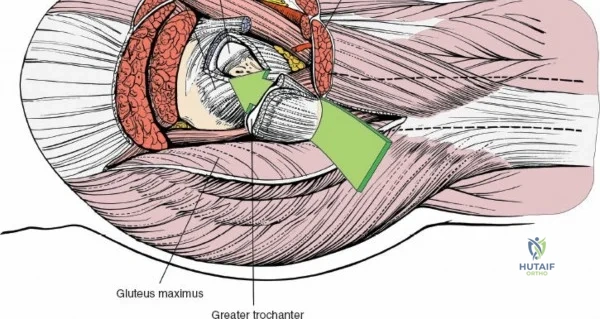
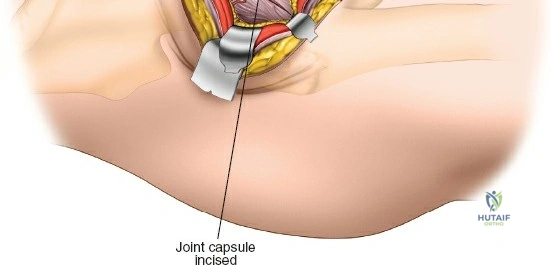
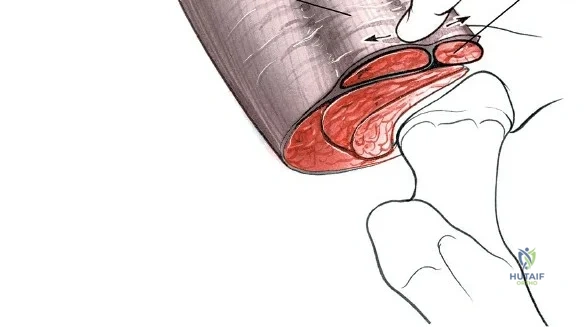
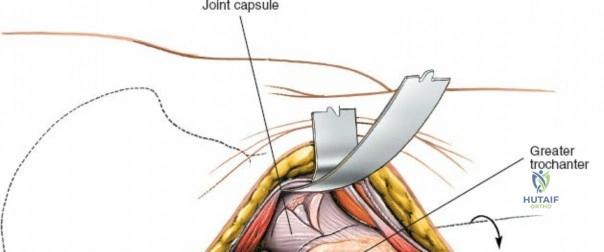
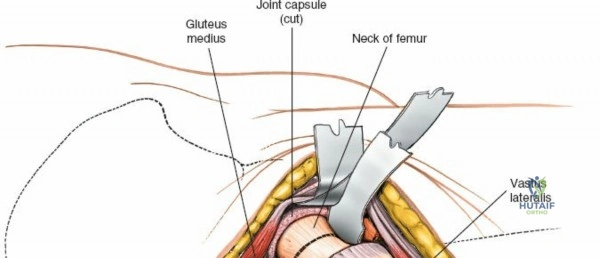
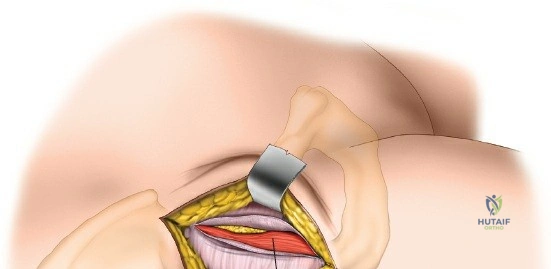
Capsulotomy and Joint Dislocation
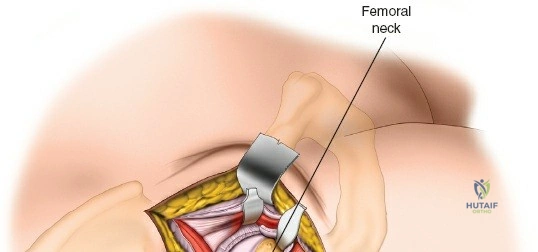
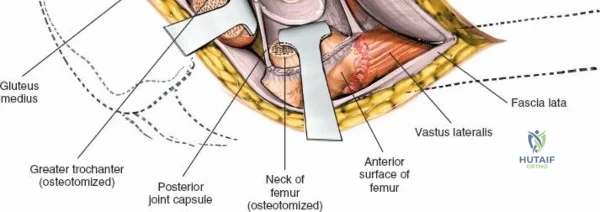
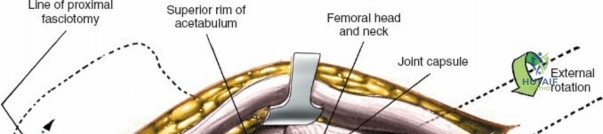
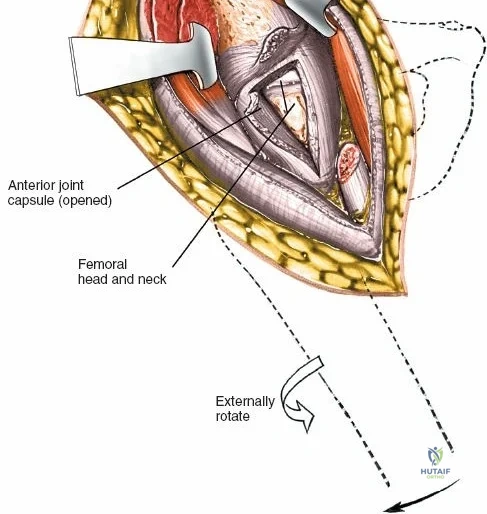
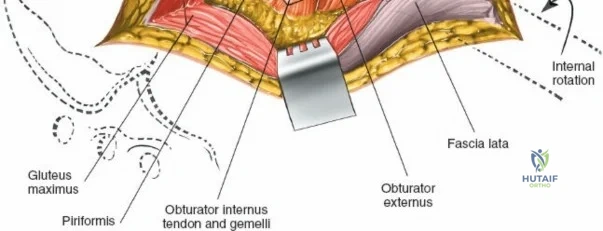
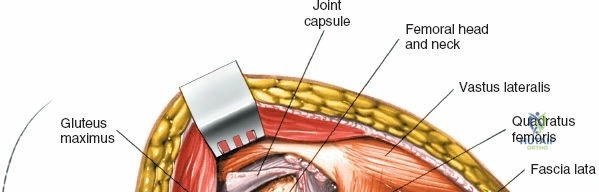
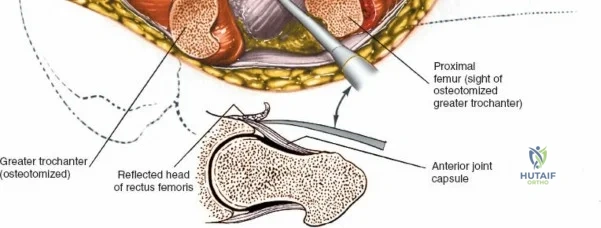
Deep to the rectus femoris lies the anterior capsule of the hip joint, covered by a layer of pericapsular fat. The reflected head of the rectus femoris, which blends with the anterior capsule, is elevated or excised. A thorough anterior capsulectomy or an H-shaped capsulotomy is performed, depending on surgeon preference regarding capsular repair. The labrum is identified and excised if arthroplasty is being performed. To dislocate the hip, the operative leg is placed into external rotation. If the femoral neck is to be cut in situ (common in THA to avoid the trauma of dislocation), a retractor is placed superior to the femoral neck and another inferiorly. The neck is cut with an oscillating saw based on preoperative templating, and the femoral head is extracted using a corkscrew.
Complications, Incidence Rates, and Salvage Management
While the anterior approach offers numerous benefits, it is associated with a unique profile of intraoperative and postoperative complications that the orthopedic surgeon must be prepared to manage. The most frequently cited complication specific to this approach is injury to the lateral femoral cutaneous nerve (LFCN), resulting in meralgia paresthetica. This presents as numbness, dysesthesia, or burning pain over the anterolateral thigh. The incidence of LFCN neuropraxia varies widely in the literature, ranging from 2% to over 15%, though permanent, debilitating neuralgia is rare (less than 1%). Prevention relies strictly on the fascial splitting technique over the TFL, avoiding blind retractor placement medially.

Vascular complications, though less common, can be life-threatening. Failure to adequately secure the ascending branch of the lateral femoral circumflex artery can lead to massive deep hematoma formation, requiring urgent surgical evacuation. More catastrophically, straying medial to the psoas muscle or placing self-retaining retractors too deep medially can result in laceration of the major femoral vessels. Intraoperative hemorrhage must be managed immediately with direct pressure, extension of the incision, and vascular surgical consultation if the femoral artery or vein is breached.

Periprosthetic fractures represent another significant hurdle, particularly during femoral elevation and broaching. Because the femur must be mobilized anteriorly and laterally out of the wound bed, excessive leverage with femoral elevators can cause fractures of the greater trochanter or the posterior calcar. If a calcar fracture occurs during broaching, it must be recognized immediately; the broach is left in place, and a cerclage wire or cable is passed around the proximal femur to stabilize the fracture before final stem impaction.
| Complication | Estimated Incidence | Mechanism of Injury | Salvage / Prevention Strategy |
|---|---|---|---|
| LFCN Neuropraxia | 2% - 15% | Traction, direct transection, or compression by retractors | Incise fascia over TFL; avoid medial retractor pressure; gabapentin for post-op pain. |
| Intraoperative Femoral Fracture | 1% - 3% | Excessive leverage during femoral elevation; over-broaching | Adequate capsular release; sequential broaching; prophylactic cerclage cabling. |
| Deep Hematoma | < 1% | Unsecured ascending branch of lateral femoral circumflex artery | Suture ligation of vessels; meticulous hemostasis prior to closure; judicious use of drains. |
| Wound Healing Complications | 1% - 4% | Maceration in obese patients (pannus); excessive skin tension | Pannus taping; negative pressure wound therapy (NPWT) dressings; meticulous layered closure. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol following a hip procedure is heavily influenced by the surgical approach utilized. One of the primary drivers for the adoption of the anterior approach is the theoretical acceleration of the early rehabilitation phase. Because the major abductor muscles (gluteus medius and minimus) and the posterior soft-tissue envelope are not detached or split, patients often experience less immediate postoperative pain and demonstrate a faster return to independent ambulation. In the immediate postoperative phase (Days 0-14), patients are typically allowed to weight-bear as tolerated (WBAT) with an assistive device. Early mobilization is initiated on the day of surgery to mitigate the risks of deep vein thrombosis (DVT) and pulmonary embolism.
During the intermediate phase (Weeks 2-6), physical therapy focuses on normalizing the gait pattern, weaning off assistive devices, and initiating gentle strengthening. Unlike the posterior approach, which traditionally requires strict adherence to posterior hip precautions (avoiding flexion past 90 degrees, adduction, and internal rotation), the anterior approach generally allows for unrestricted hip flexion. However, patients are often cautioned against extreme extension combined with external rotation, as this maneuver stresses the anterior capsular repair and the anterior soft tissue envelope, potentially precipitating an anterior dislocation.

The advanced rehabilitation phase (Weeks 6-12) focuses on maximizing abductor strength, core stability, and proprioception. Patients are gradually introduced to low-impact aerobic activities such as stationary cycling, swimming, and elliptical training. Return to high-impact sports or heavy manual labor is highly individualized and depends on the fixation method (cemented vs. cementless), the patient's baseline fitness, and radiographic evidence of biologic ingrowth. Throughout all phases, the surgeon and physical therapist must maintain open communication to monitor for signs of implant subsidence, infection, or tendinopathy.

Summary of Landmark Literature and Clinical Guidelines
The evolution of surgical approaches to the hip is deeply rooted in anatomical study and progressive clinical innovation. The anterior approach was originally described by Carl Hueter in 1881 and later popularized in the English-speaking orthopedic community by Marius Smith-Petersen in 1917. Smith-Petersen's original descriptions focused on the utility of the approach for congenital hip dislocations and joint debridement. For decades, the approach was largely overshadowed by the Charnley trans-trochanteric approach and the Moore posterior approach due to the technical challenges of femoral exposure without specialized instrumentation.


In the modern era, the resurgence of the anterior approach for total hip arthroplasty is largely credited to the pioneering work of surgeons like Joel Matta, who refined the technique using a specialized traction table. Landmark comparative studies in the early 2000s began to demonstrate that while the anterior approach possessed a steeper learning curve, it offered statistically significant improvements in early functional milestones, such as time to discontinue walking aids and early postoperative pain scores, when compared to the posterior approach. However, long-term registry data consistently show that by six months to one year postoperatively, functional outcomes and patient satisfaction scores equalize across all major surgical approaches.

Current clinical guidelines from the American Academy of Orthopaedic Surgeons (AAOS) and the American Association of Hip and Knee Surgeons (AAHKS) emphasize that the choice of surgical approach should be dictated by the surgeon's experience and the specific needs of the patient, rather than a dogmatic adherence to a single technique. The integration of Enhanced Recovery After Surgery (ERAS) protocols—which include multimodal analgesia, tranexamic acid (TXA) for blood conservation, and rapid mobilization—has dramatically improved outcomes regardless of the incision used. Ultimately, a master orthopedic surgeon must possess a comprehensive, three-dimensional understanding of hip anatomy, allowing them to safely and effectively deploy the anterior, posterior, lateral, or medial approach as the clinical scenario demands.
Clinical & Radiographic Imaging Archive