Optimized Approaches to the Dorsum of the Foot & Ankle
Key Takeaway
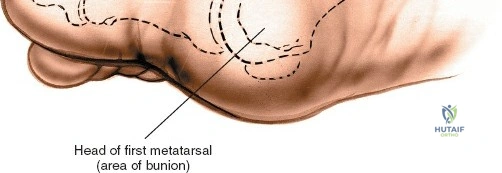
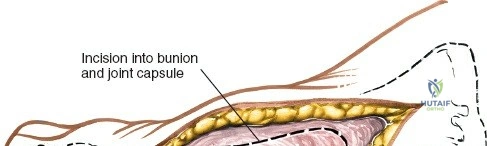
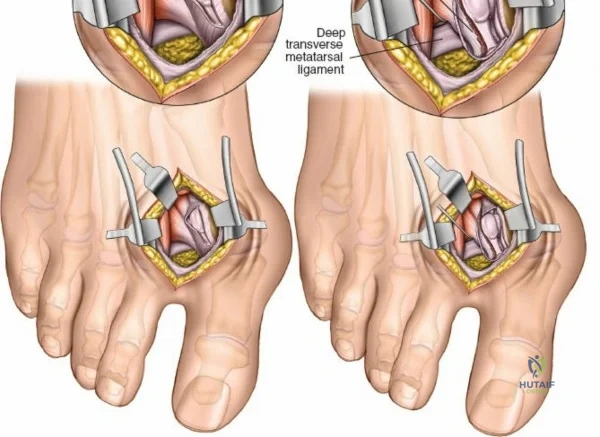
In this comprehensive guide, we discuss everything you need to know about Optimized Approaches to the Dorsum of the Foot & Ankle. Surgical approaches to the foot and ankle include anterior, lateral, medial, and posterior incisions for the ankle and hindfoot. Dorsal approaches are specifically utilized for the midfoot and forefoot, often targeting the **dorsum of the foot** for procedures such as bunion surgery, Morton neuroma, or joint exploration. Circulation evaluation is vital for healing.
Comprehensive Introduction and Patho-Epidemiology
Approaches to the structures of the ankle and foot are generally considered anatomically straightforward, as the osseous and articular structures requiring exploration are commonly superficial, if not entirely subcutaneous. However, the apparent simplicity of the surgical anatomy belies the profound clinical challenges inherent to this region. Apart from the technical complexities associated with the osseous reconstruction or arthrodesis itself, the most common and devastating complication in foot and ankle surgery is catastrophic wound failure. The soft tissue envelope surrounding the distal tibia, ankle joint, and hindfoot is notoriously thin, lacking the robust muscle bellies that provide vascular collateralization and soft tissue coverage in more proximal anatomic zones. Consequently, meticulous handling of this fragile envelope is the paramount principle governing all surgical approaches to the foot and ankle.

For this reason, it is absolutely critical to exhaustively evaluate both the macro- and micro-circulation, as well as the sensory integrity of the foot, prior to any surgical intervention. Ischemic or neuropathic feet heal poorly and represent a frequent and formidable contraindication to elective reconstructive surgery. In the diabetic patient population, ischemia and peripheral neuropathy frequently coexist, creating a synergistic environment for wound dehiscence, deep infection, and ultimately, amputation. All feet of such patients must be evaluated carefully with non-invasive vascular studies (such as Ankle-Brachial Indices, Toe-Brachial Indices, and transcutaneous oxygen tension measurements) and Semmes-Weinstein monofilament testing before any surgical incision is planned. Furthermore, tobacco use is a profound relative, and often absolute, contraindication to elective surgery, especially in high-risk procedures such as the open reduction and internal fixation of complex calcaneal or pilon fractures, due to the microvascular vasoconstriction and impaired cellular healing mechanisms induced by nicotine.

Wound healing in this region is also directly dictated by the geometric design and thickness of the surgically elevated skin flaps. It is a fundamental surgical axiom that flaps must be elevated as full-thickness fasciocutaneous units to preserve the delicate subdermal vascular plexus. The surgeon must assiduously avoid forceful or prolonged static retraction, which can induce focal ischemia and subsequent marginal necrosis. Counterintuitively, longer extensile incisions require significantly less forceful retraction to achieve identical deep exposure compared to shorter, "minimally invasive" incisions that are aggressively stretched. As a result, appropriately planned long incisions are often safer and exhibit superior healing profiles. It is imperative to remember that skin incisions heal from side to side, dependent on local oxygen tension and collagen cross-linking, and not from end to end; therefore, the length of the incision does not inherently dictate the time to clinical healing.
This chapter focuses on optimized approaches to the anterior ankle and the medial malleolus, providing the foundational knowledge required for safe and effective exposure of these critical zones. The anterior approach to the ankle is a workhorse extensile exposure utilized heavily for tibiotalar arthrodesis, total ankle arthroplasty, and the management of complex intra-articular distal tibia (pilon) fractures. It offers unparalleled, direct visualization of the anterior compartment of the ankle joint and the talar dome. Conversely, the approaches to the medial malleolus—both anterior and posterior variants—are commonly utilized incisions providing specific, targeted access to the distal medial tibia and the deltoid ligament complex. Mastery of these approaches requires not only a deep understanding of the normal anatomy but also an appreciation for the pathologic distortions introduced by trauma, chronic deformity, and prior surgical interventions.
Detailed Surgical Anatomy and Biomechanics
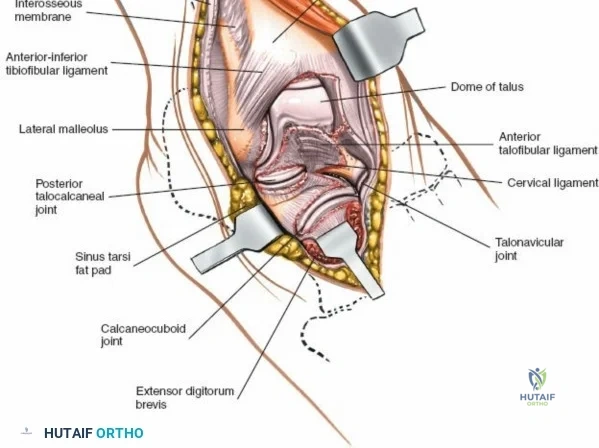
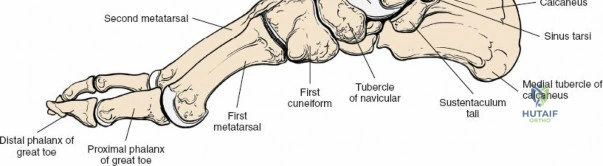
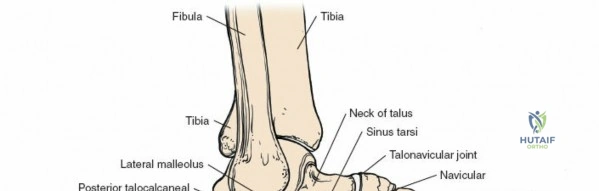
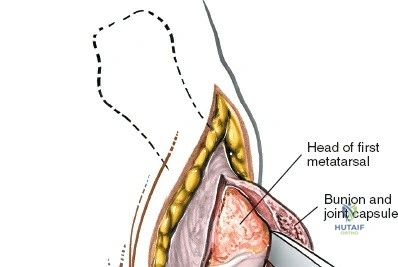
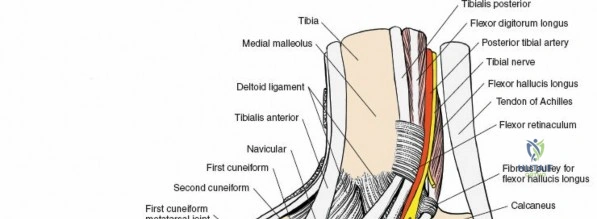
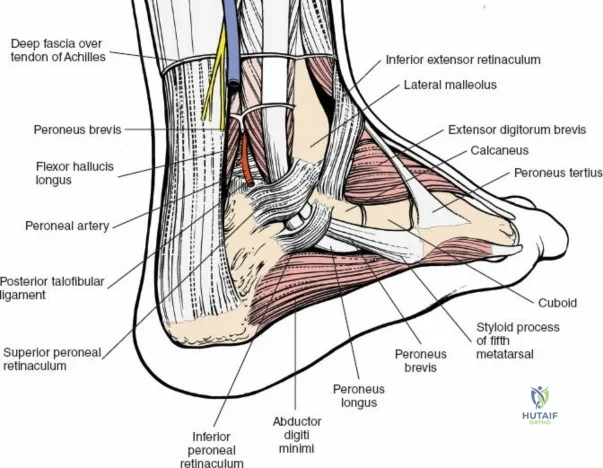
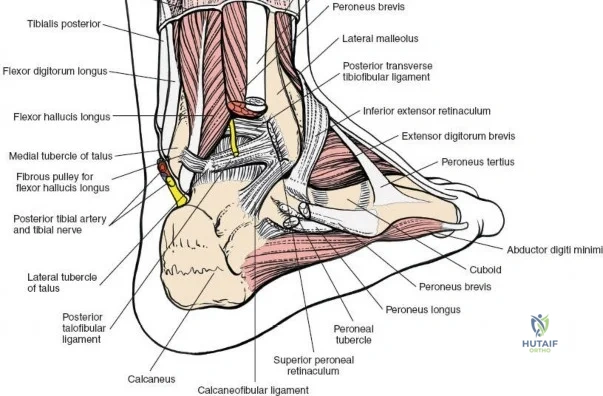
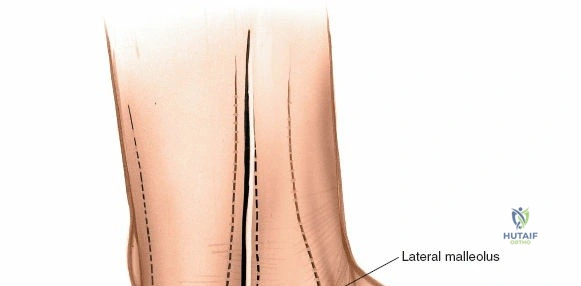
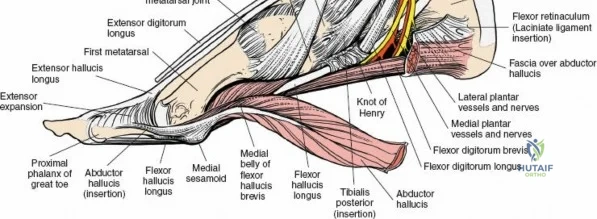
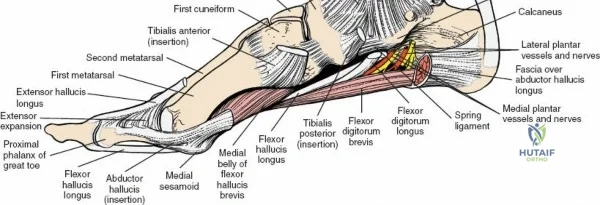
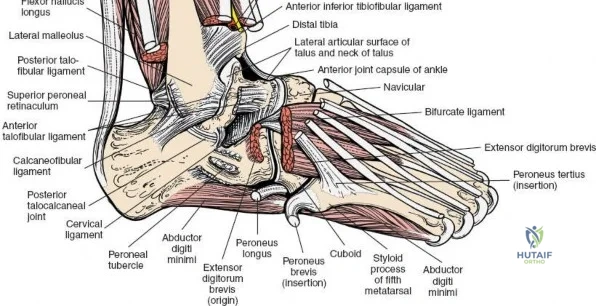
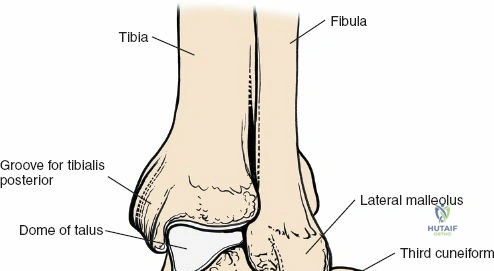
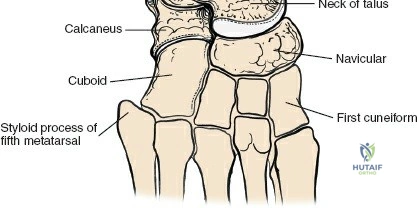
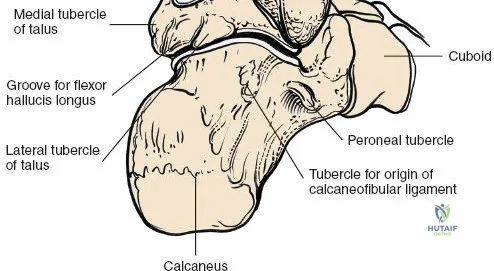
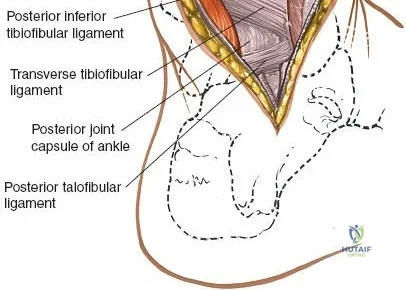
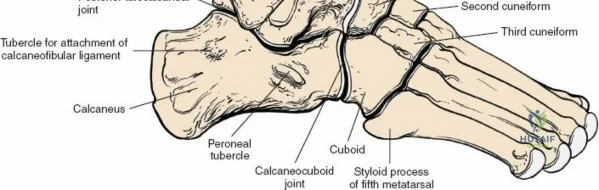
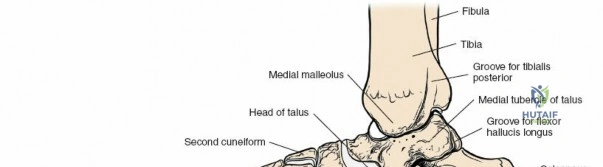
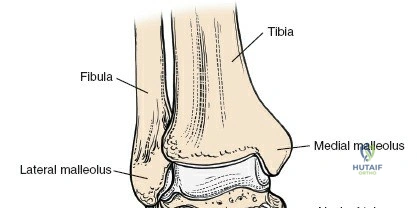
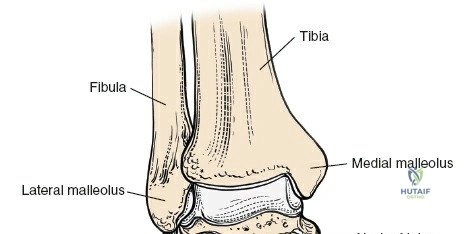
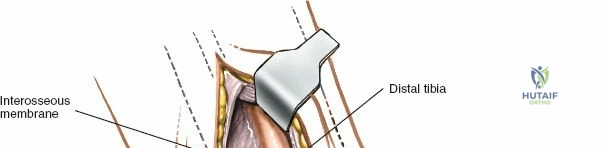
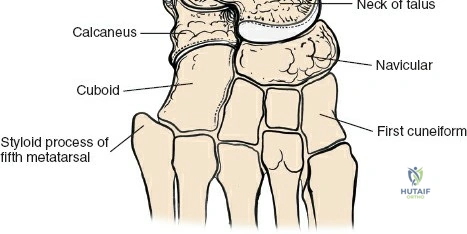
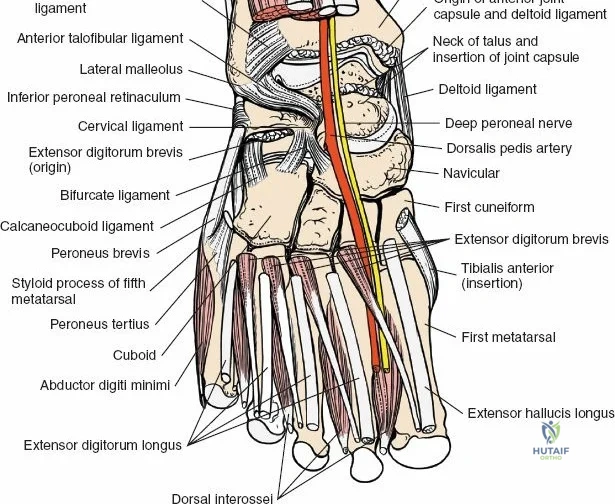
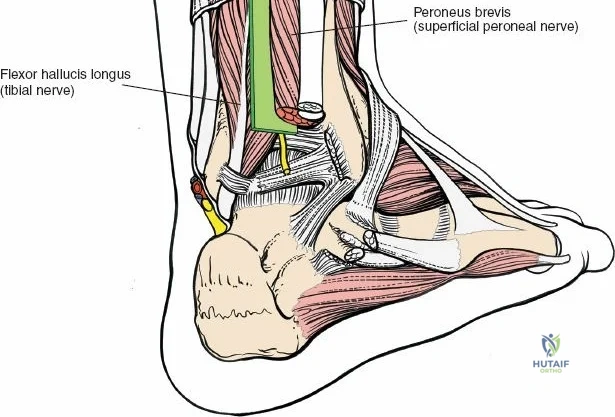
The surgical anatomy of the anterior ankle and dorsum of the foot is defined by a complex arrangement of superficial nerves, dense retinacular structures, and a critical central neurovascular bundle. The distal tibia flares to form the medial malleolus, a bulbous, subcutaneous osseous prominence that serves as the primary medial stabilizer of the ankle mortise and the origin of the robust deltoid ligament. Laterally, the fibula extends distally to form the lateral malleolus, extending further inferiorly and posteriorly than its medial counterpart. The talus, a unique bone devoid of any muscular attachments, sits perfectly constrained within this mortise, relying entirely on its articular geometry and ligamentous restraints for biomechanical stability. The anterior capsule of the ankle joint is relatively thin and redundant, allowing for physiologic plantarflexion, but it is intimately related to the overlying extensor tendons and neurovascular structures.
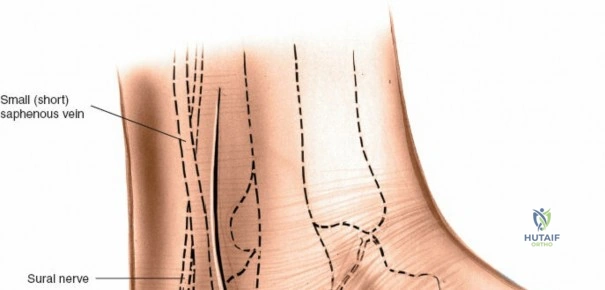
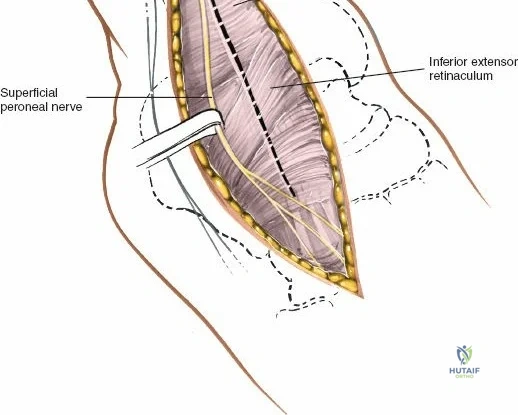
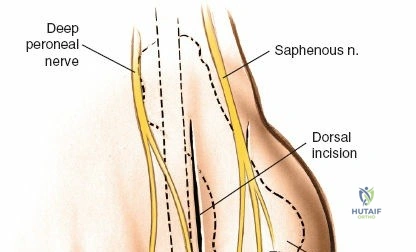
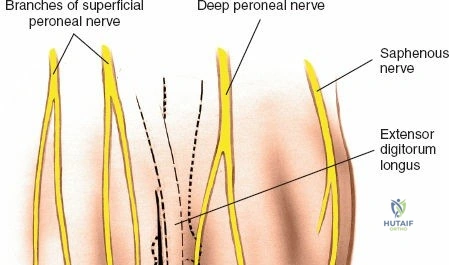
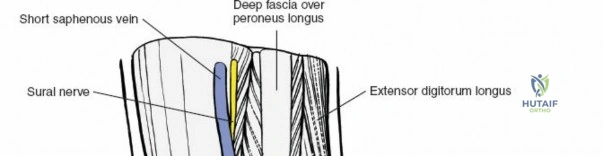
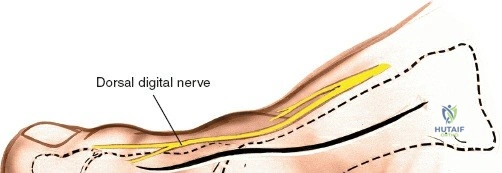
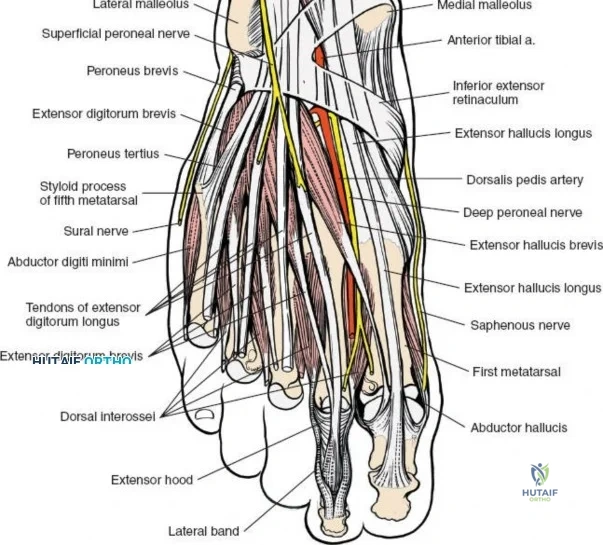
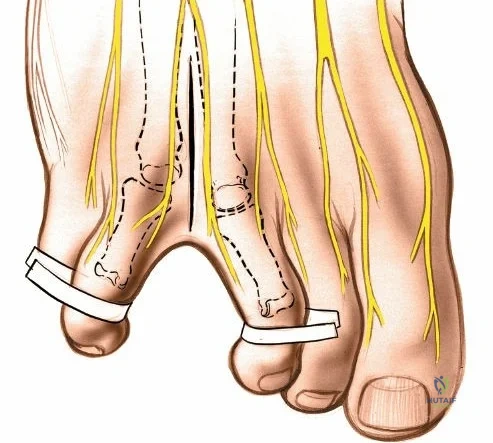
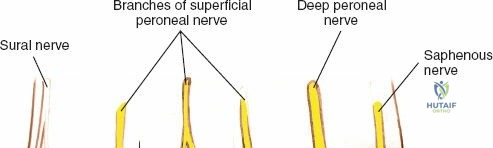
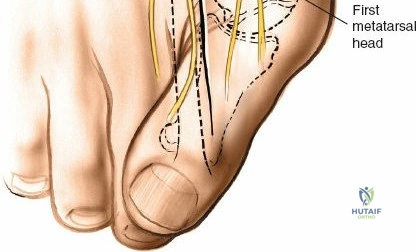
Superficially, the anatomy is dominated by the superficial peroneal nerve (SPN) and the saphenous nerve. The SPN pierces the deep crural fascia in the anterolateral third of the leg, approximately 10 to 12 centimeters proximal to the tip of the lateral malleolus. It subsequently bifurcates into the medial and intermediate dorsal cutaneous nerves, which arborize across the anterior ankle joint to provide sensation to the dorsum of the foot. These branches are highly variable in their course and are at extreme risk during the initial skin incision of the anterior approach. Medially, the long saphenous vein and the accompanying saphenous nerve travel anterior to the medial malleolus. The saphenous nerve provides sensation to the medial aspect of the foot and must be meticulously protected during medial approaches to prevent painful postoperative neuromas.
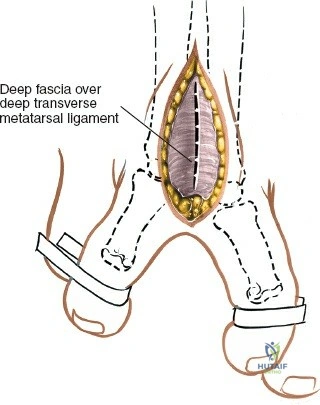
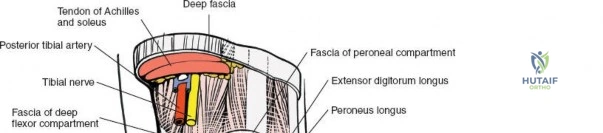
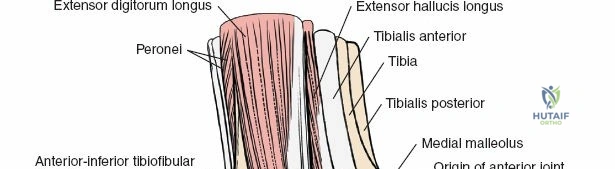
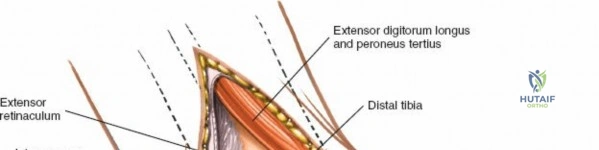
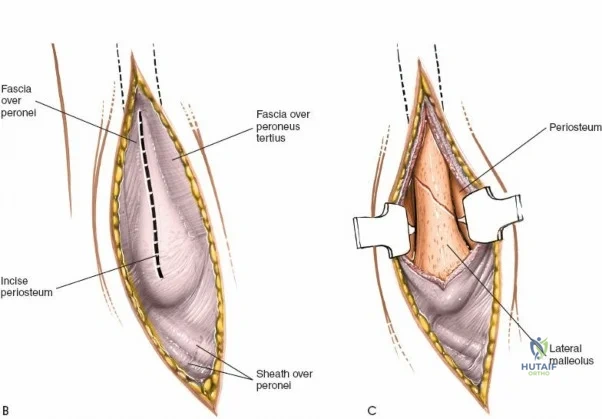
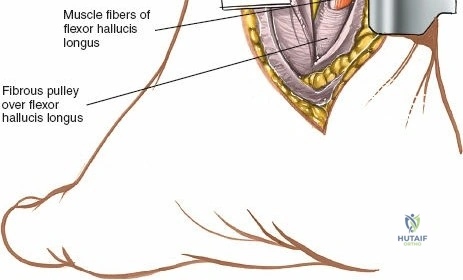
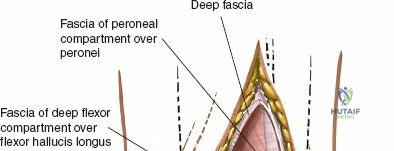
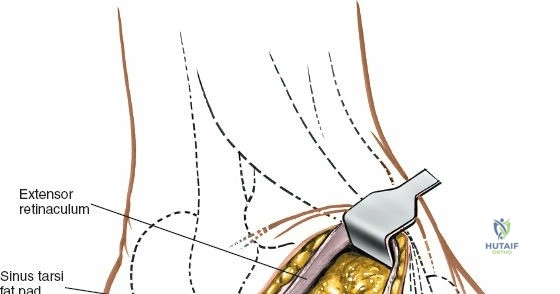
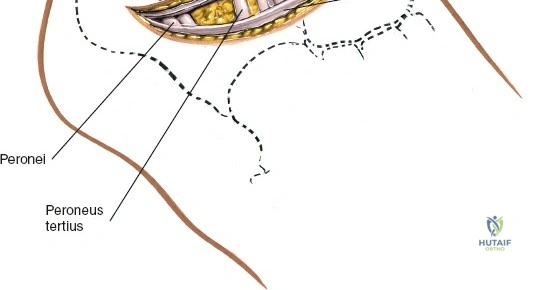
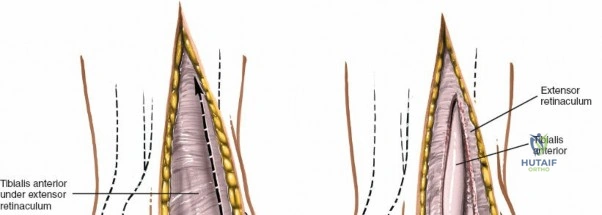
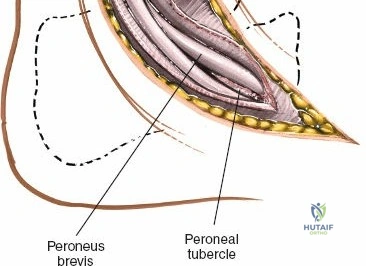
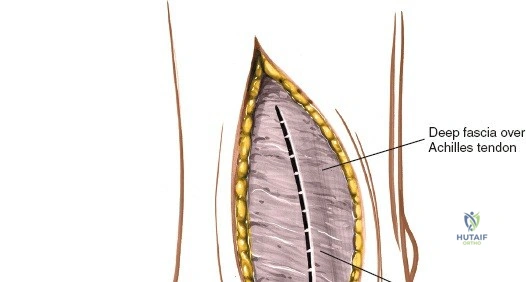
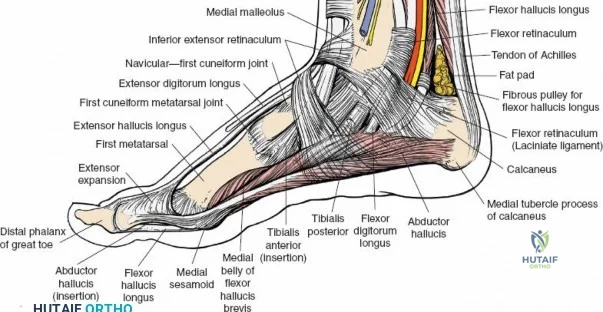
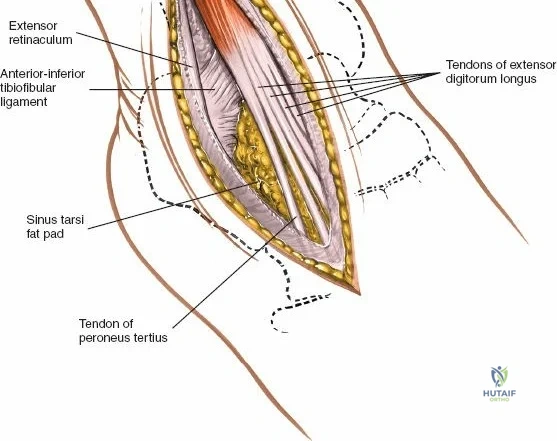
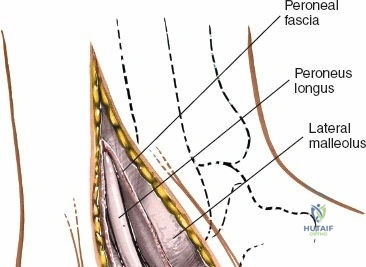
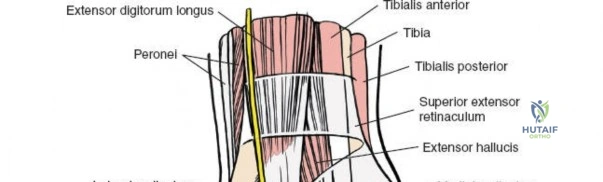
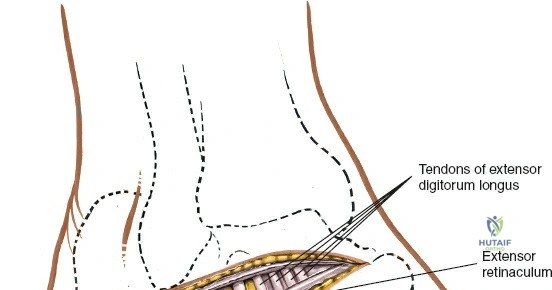
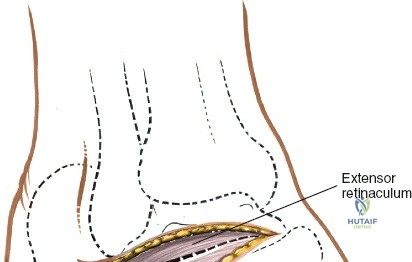
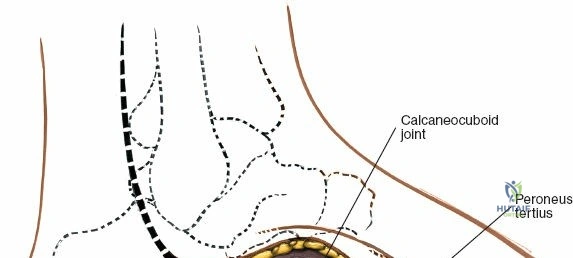
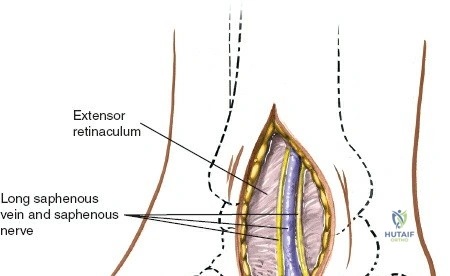
Deep to the subcutaneous tissues lies the extensor retinaculum, a specialized thickening of the deep crural fascia divided into superior and inferior components. The superior extensor retinaculum binds down the extensor tendons proximal to the ankle joint, while the Y-shaped inferior extensor retinaculum stabilizes them over the dorsum of the foot. These retinacula prevent tendon bowstringing during active dorsiflexion. Passing deep to these retinacular bands are the four primary tendons of the anterior compartment: from medial to lateral, the tibialis anterior (TA), the extensor hallucis longus (EHL), the extensor digitorum longus (EDL), and the peroneus tertius. Each tendon is enclosed within its own synovial sheath, which must be respected and, when incised, carefully repaired or bypassed to prevent postoperative adhesions.
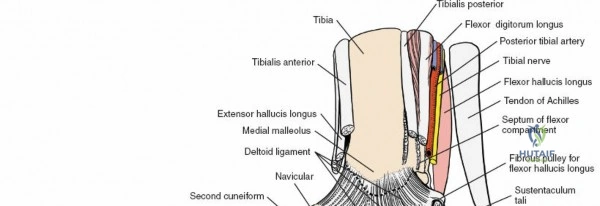
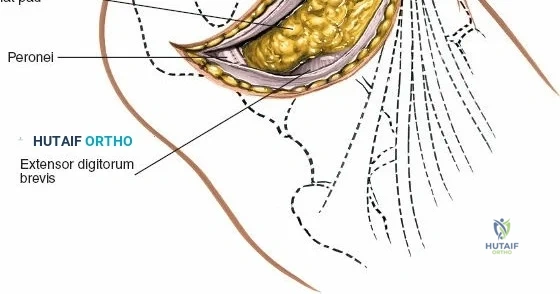
The most critical deep anatomic structure in the anterior approach is the anterior neurovascular bundle, comprising the anterior tibial artery and the deep peroneal nerve. Proximal to the ankle joint, this bundle lies deeply situated between the TA and the EHL. However, as the structures cross the anterior ankle joint line, the EHL tendon crosses obliquely over the neurovascular bundle from lateral to medial. Consequently, at the level of the joint line, the neurovascular bundle lies precisely between the EHL and the EDL. The deep peroneal nerve provides motor innervation to the extensor digitorum brevis and sensation to the first dorsal web space. The anterior tibial artery continues distally as the dorsalis pedis artery. Precise identification, mobilization, and protection of this bundle are the sine qua non of a safe anterior approach to the ankle.
Exhaustive Indications and Contraindications
The decision to utilize a specific surgical approach to the ankle and foot is dictated by the underlying pathology, the required osseous exposure, the condition of the regional soft tissues, and the surgeon's preoperative reconstructive plan. The anterior approach to the ankle is a highly versatile, extensile exposure. Its primary indications include tibiotalar arthrodesis, where it provides unparalleled access for joint preparation and the application of anterior plating systems. It is also the approach of choice for total ankle arthroplasty, allowing for precise, central alignment of the cutting jigs. In the realm of orthopedic trauma, the anterior approach is frequently utilized for the open reduction and internal fixation of complex, comminuted distal tibial fractures (pilon fractures), particularly those with central or anterior articular impaction. Additional indications include the drainage of deep intra-articular infections, extensive synovectomy, and the removal of large anterior loose bodies or osteophytes.
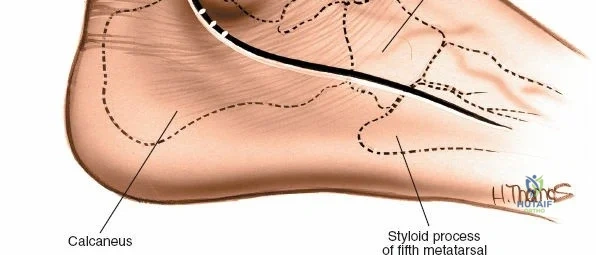
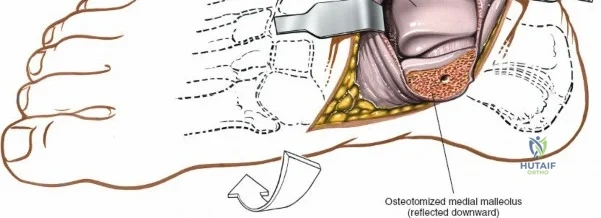
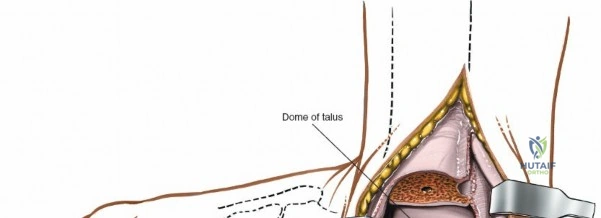
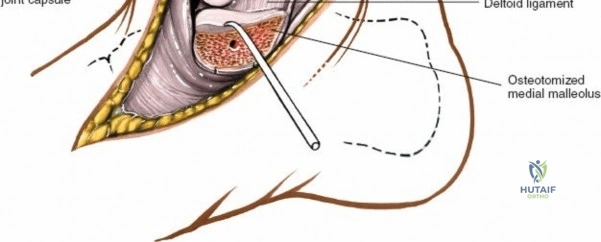
Conversely, approaches to the medial malleolus are more focal and targeted. The anterior incision to the medial malleolus is exceptionally useful for the direct visualization and fixation of medial malleolar fractures, specifically transverse or short oblique fracture patterns. It also permits limited inspection of the anteromedial ankle joint and the anteromedial aspect of the talar dome, making it useful for addressing medial osteochondral lesions of the talus (OLTs) when a medial malleolar osteotomy is planned. The posterior incision to the medial malleolus is specifically indicated for the reduction and fixation of posterior-exiting medial malleolar fractures, access to the posterior margin of the tibia (posterior malleolus), and exploration or repair of the posterior tibialis tendon and the deep deltoid ligament complex.
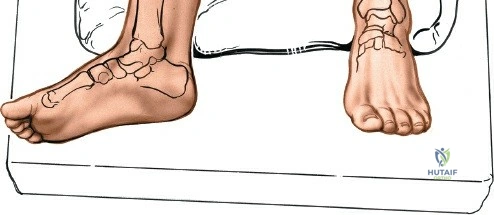
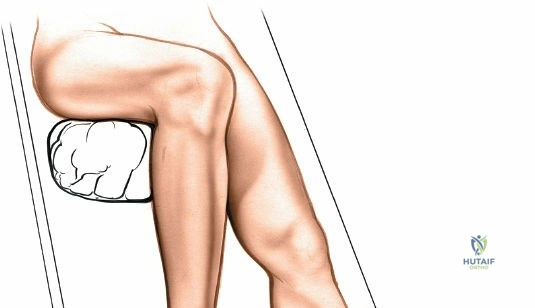
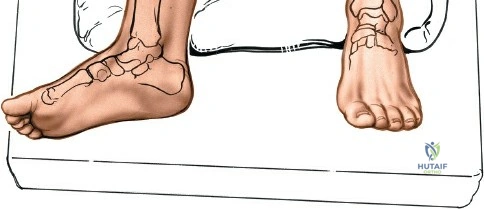
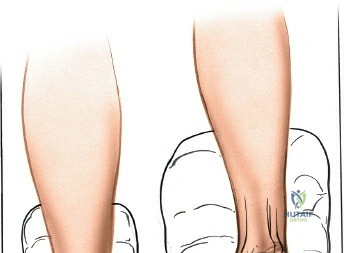
Contraindications to these approaches must be rigorously respected to prevent catastrophic complications. Absolute contraindications include the presence of active, untreated soft tissue infection overlying the planned surgical incision, and severe, un-revascularizable peripheral arterial disease (PAD). Operating through ischemic tissue guarantees wound necrosis and subsequent deep infection. Relative contraindications are numerous and require careful preoperative optimization. These include poorly controlled diabetes mellitus (HbA1c > 8.0%), active tobacco use, chronic systemic corticosteroid use, and profound peripheral neuropathy (Charcot arthropathy), which severely compromises postoperative compliance and bone healing. In the setting of acute trauma, severe fracture blisters or profound soft tissue edema represent a temporary contraindication; surgery must be delayed until the "wrinkle sign" returns, indicating that the soft tissue envelope has sufficiently recovered to tolerate surgical insult.
| Clinical Parameter | Anterior Approach Indications | Medial Malleolar Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|---|
| Trauma | Pilon fractures (anterior impaction) | Medial malleolar fractures | Active overlying infection | Severe soft tissue edema |
| Reconstruction | Total Ankle Arthroplasty | Medial talar dome OLTs | Non-reconstructable ischemia | Uncontrolled Diabetes Mellitus |
| Arthrodesis | Tibiotalar or Tibiotalocalcaneal | Medial column stabilization | Charcot neuroarthropathy (acute) | Active tobacco smoking |
| Infection/Other | Septic ankle joint drainage | Deltoid ligament avulsion | Inadequate soft tissue coverage | Chronic corticosteroid therapy |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the foundation of a successful surgical outcome in foot and ankle surgery. Advanced imaging is virtually mandatory in the modern era. For complex trauma, such as pilon fractures, fine-cut computed tomography (CT) with two-dimensional multiplanar reconstructions and three-dimensional surface rendering is essential to understand the fracture morphology, the location of articular impaction, and the trajectory of fracture lines. This allows the surgeon to precisely plan the surgical incision to access the critical pathology while avoiding compromised soft tissues. For reconstructive procedures, weight-bearing radiographs are critical for assessing alignment. Magnetic resonance imaging (MRI) is utilized to evaluate the integrity of the tendinous structures, the extent of osteochondral lesions, and the presence of avascular necrosis of the talus. Digital templating software should be utilized to plan implant size, osteotomy trajectories, and screw lengths.

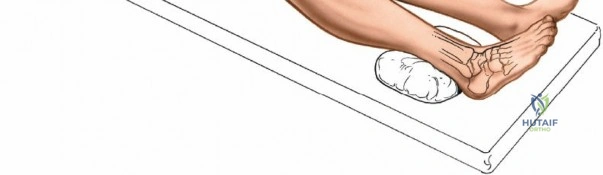
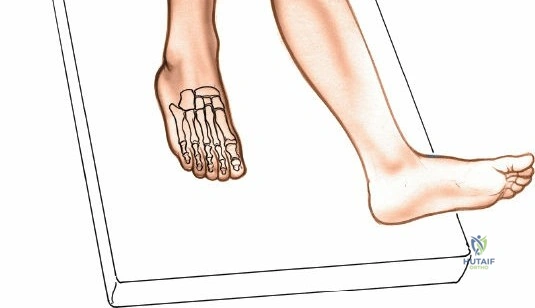
Patient positioning for the anterior approach to the ankle is typically supine on a radiolucent operating table. A bump (usually a folded blanket or sandbag) is placed under the ipsilateral hip to correct the natural external rotation of the lower extremity, bringing the foot and ankle into a neutral, strictly anterior-facing position. This ensures that the surgeon's view of the ankle mortise is orthogonal. The foot is partially exsanguinated either by elevating it for 3 to 5 minutes or by applying a soft rubber bandage (Esmarch) loosely to the foot and binding it firmly to the calf before inflating a pneumatic thigh tourniquet. Partial exsanguination is a highly useful technique; it allows the neurovascular bundle to be more easily identified during deep dissection, as the venous structures will remain engorged and appear blue, contrasting with the surrounding white tendinous and fascial tissues. Some continuous vascular oozing must be expected and managed with bipolar electrocautery.
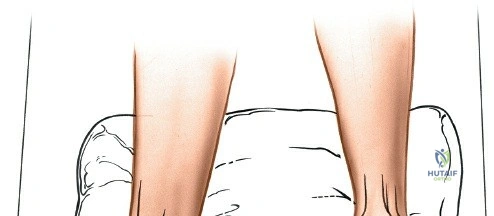
For approaches to the medial malleolus, the patient is also placed supine. However, the ipsilateral hip bump is omitted. The leg is allowed to fall naturally into a few degrees of external rotation, which perfectly exposes the medial aspect of the ankle and the medial malleolus to the surgeon. The contralateral leg must be adequately padded and secured. The fluoroscopy unit (C-arm) is typically brought in from the contralateral side of the table, allowing for unobstructed anteroposterior, mortise, and lateral imaging of the ankle throughout the procedure. Strict attention must be paid to padding all bony prominences, particularly the fibular head to protect the common peroneal nerve, and the heel, to prevent intraoperative decubitus ulcers.
Step-by-Step Surgical Approach and Fixation Technique
The Anterior Approach to the Ankle
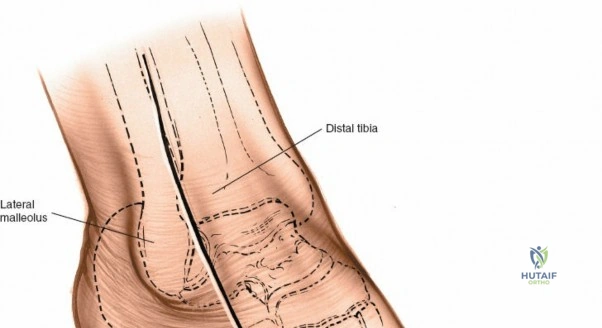
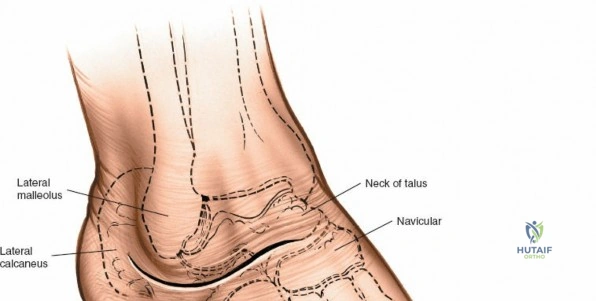
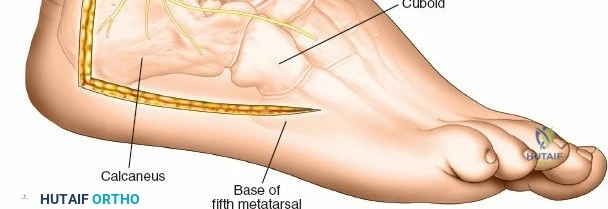
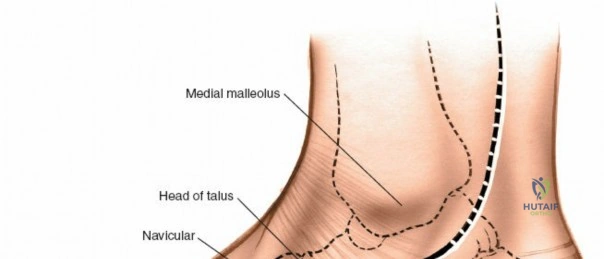
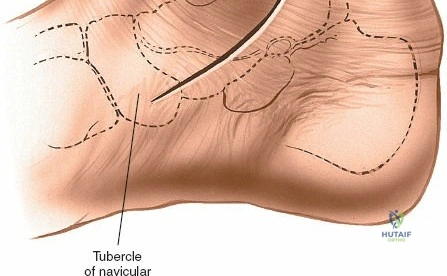
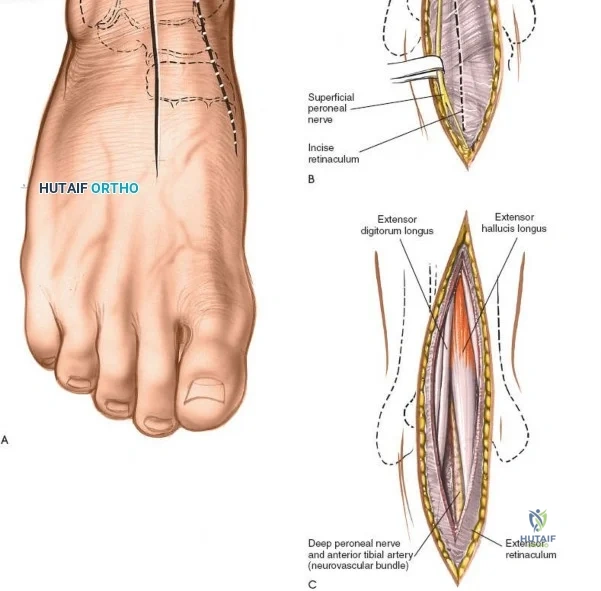
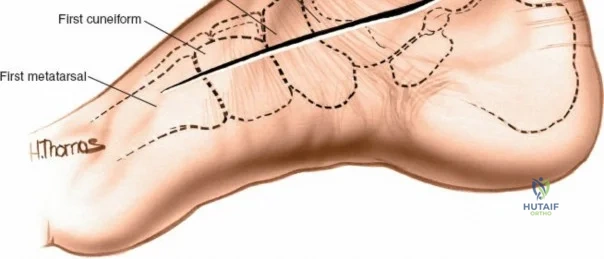
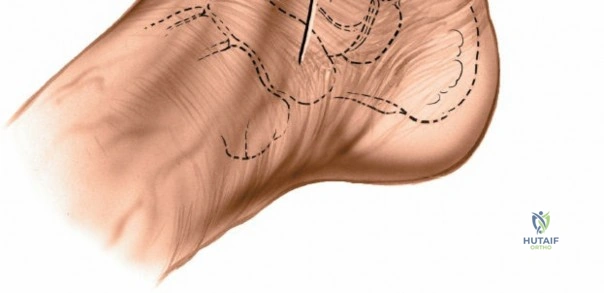
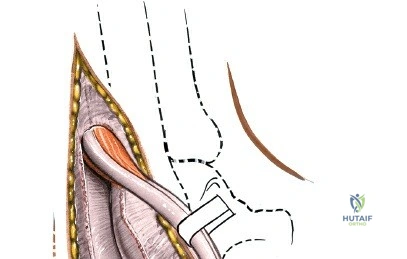
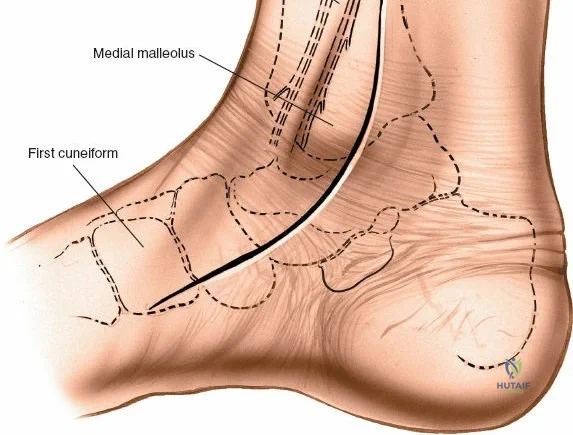
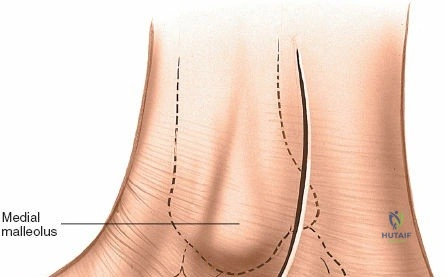
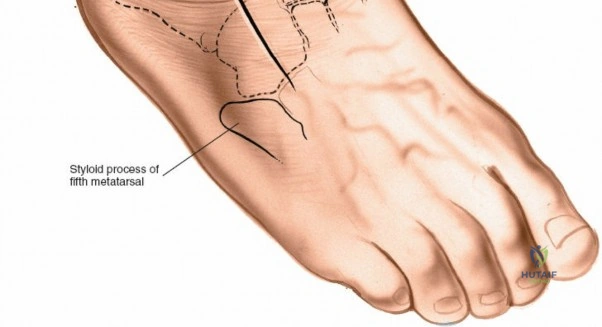
The anterior approach relies on exploiting the internervous and intertendinous planes of the anterior compartment. The primary landmarks are the medial malleolus (the bulbous, subcutaneous distal end of the tibia) and the lateral malleolus (the subcutaneous distal end of the fibula). The joint line lies approximately 1 to 2 centimeters proximal to the tip of the medial malleolus. Make a longitudinal incision exactly in the midline over the anterior aspect of the ankle joint. The incision typically spans 10 to 15 centimeters, centered over the joint line, extending from the distal tibia to the base of the talonavicular joint.
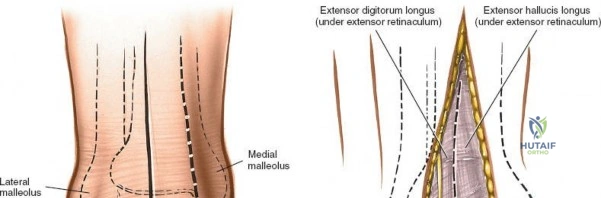
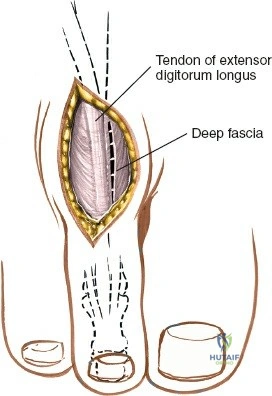
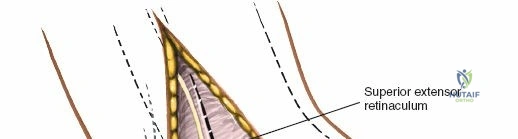
Superficial surgical dissection begins with careful deepening of the incision through the subcutaneous fat. Cutaneous branches of the superficial peroneal nerve run close to the line of the skin incision just under the skin. Take extreme care not to transect them during the initial knife stroke. Blunt dissection with a hemostat or careful spreading with scissors is recommended to identify and protect these nerve branches, mobilizing them laterally with the skin flap. Once the superficial nerves are protected, identify the superior and inferior extensor retinacula. Incise the extensor retinaculum in line with the skin incision.
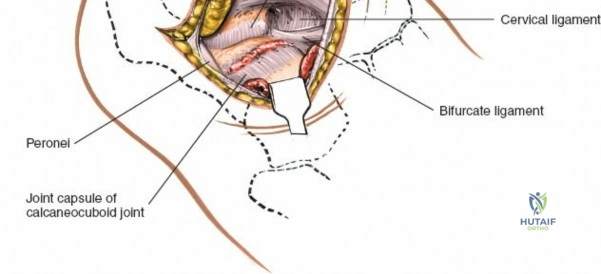
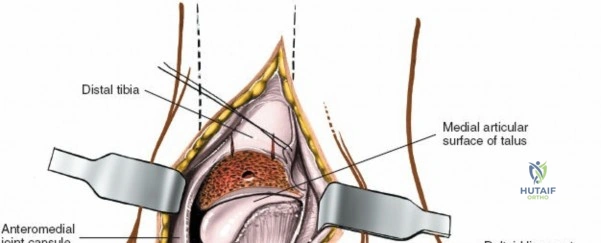
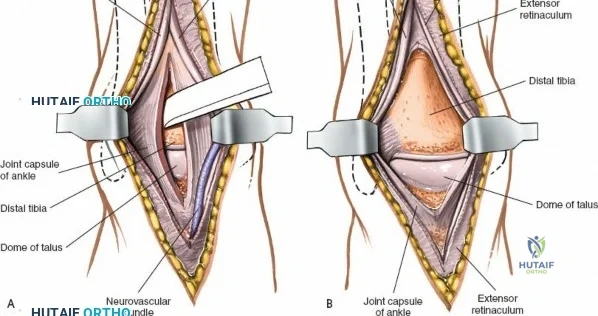
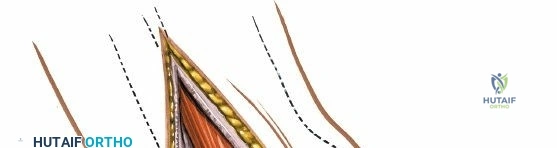
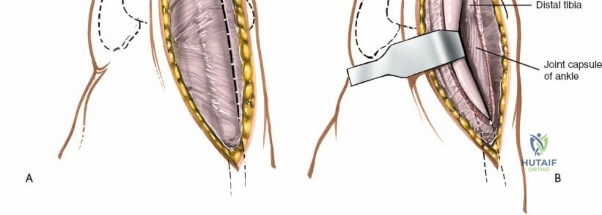
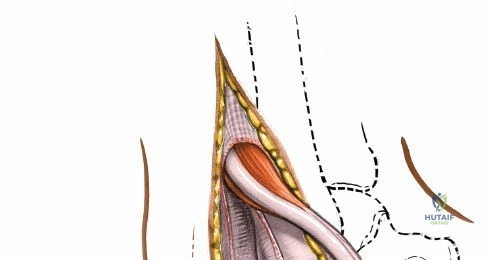
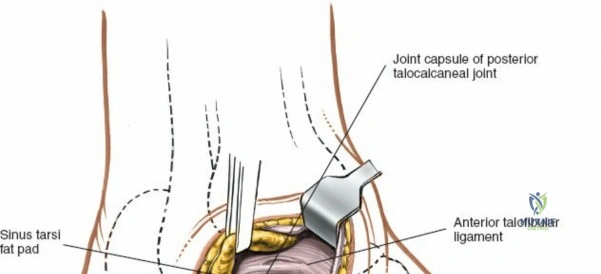
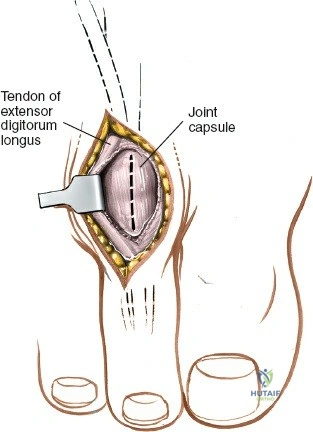
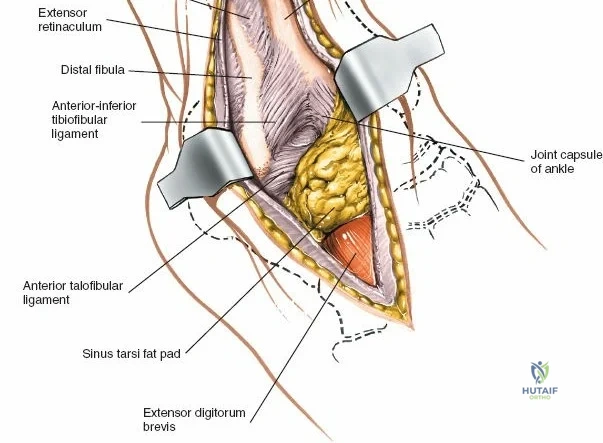
Deep surgical dissection involves identifying the plane between the extensor hallucis longus (EHL) and the extensor digitorum longus (EDL). Note the neurovascular bundle (deep peroneal nerve and anterior tibial artery) lying precisely between them at the level of the joint. Trace the bundle distally until it crosses the front of the ankle joint behind the tendon of the EHL. Carefully mobilize the neurovascular bundle. Retract the tendon of the EHL medially, together with the neurovascular bundle. Retract the tendon of the EDL laterally. The tendons become mobile after the retinaculum has been cut, but the neurovascular bundle adheres to the underlying capsular tissues and requires meticulous sharp and blunt mobilization. Once the bundle is protected, incise the joint capsule longitudinally and retract it medially and laterally to expose the anterior tibial plafond, the talar dome, and the medial and lateral gutters. If the approach is used in fracture surgery, take great care to preserve as much soft tissue attachment to bone fragments as possible to prevent avascular necrosis.
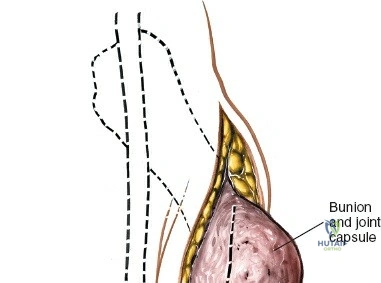
The Anterior Incision to the Medial Malleolus
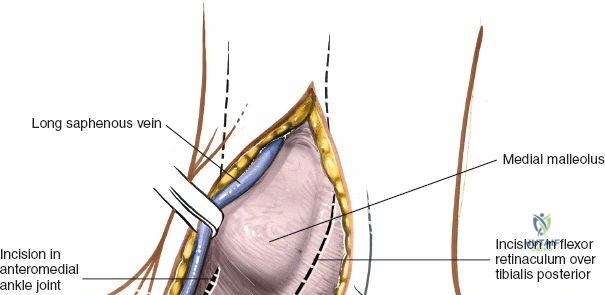
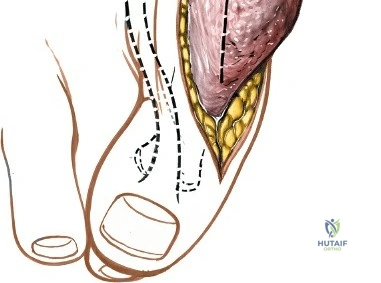
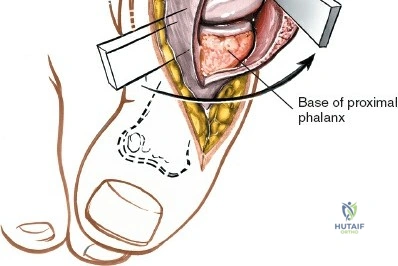
The anterior incision to the medial malleolus is designed to provide direct, subcutaneous access to the bone. Begin by palpating the medial malleolus and the anterior joint line. Make a longitudinal or slightly curved 10-cm incision centered over the anterior half of the medial malleolus. Keep the incision just anterior to the tip of the medial malleolus to avoid the bulk of the deltoid ligament insertion and to optimize the trajectory for lag screw insertion perpendicular to a standard transverse fracture line.
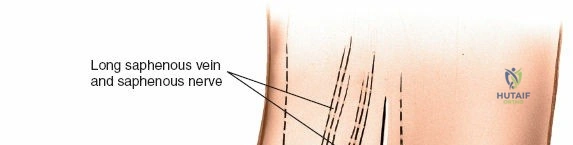
During superficial dissection, gently mobilize the full-thickness skin flaps. It is critical to identify and preserve the long saphenous vein, which lies just anterior to the medial malleolus in the subcutaneous tissues. Accurately locating the skin incision will make it unnecessary to mobilize the skin flaps extensively, thereby preserving their vascularity. Immediately adjacent to the vein runs the saphenous nerve, which frequently gives off two or more branches that are intimately bound to the adventitia of the vein. Take great care not to damage the saphenous nerve, as injury here will result in a painful neuroma directly over the medial footwear wear-zone. Retract the vein and nerve anteriorly as a single unit.
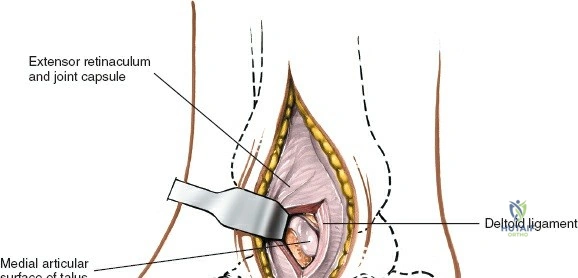
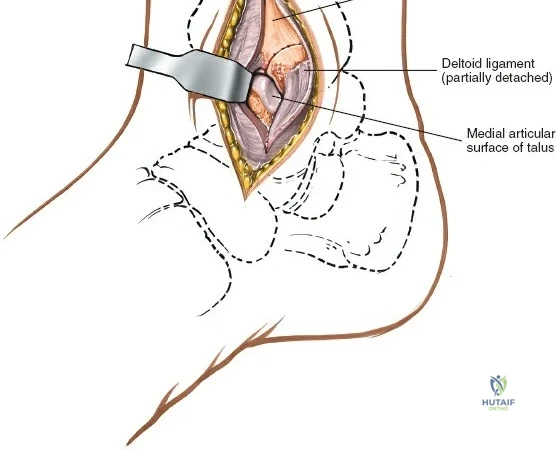
Deep dissection is relatively straightforward as no true internervous plane exists; the approach cuts down directly onto subcutaneous bone. In cases of fracture, the periosteum is already breached by the trauma. The surgeon must minimize further periosteal stripping. Protect as many soft tissue attachments to the bone fragment as possible, particularly the deltoid ligament distally, to preserve the fragment's blood supply. Clear the fracture hematoma, inspect the anteromedial corner of the joint for interposed periosteum or osteochondral fragments, and proceed with anatomic reduction and internal fixation.
The Posterior Incision to the Medial Malleolus
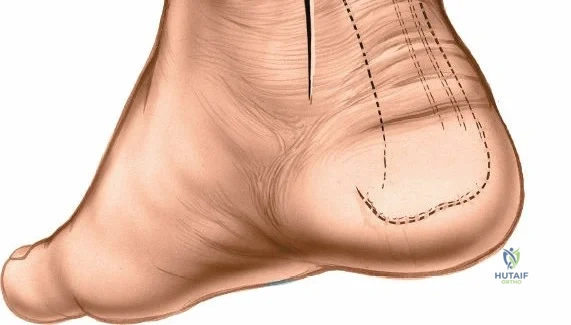
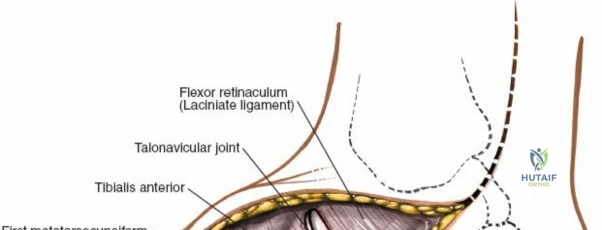
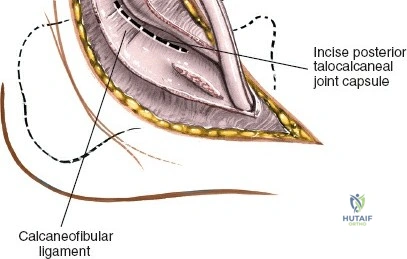
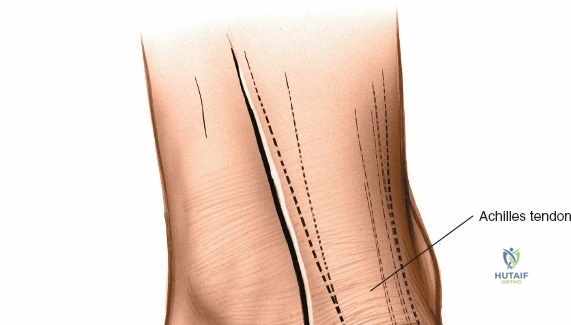
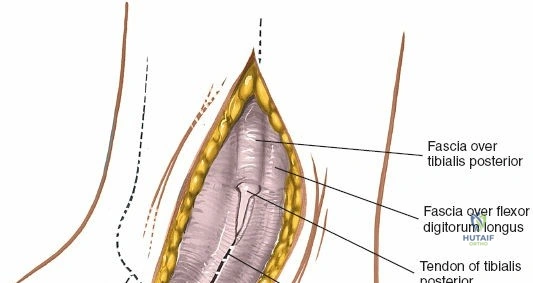
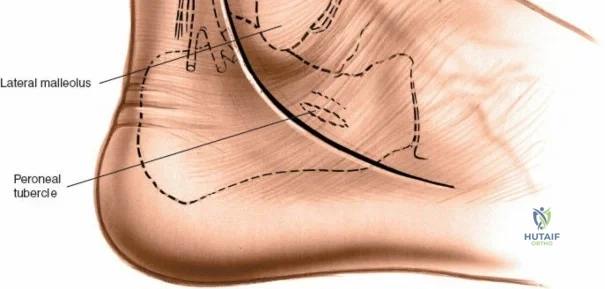
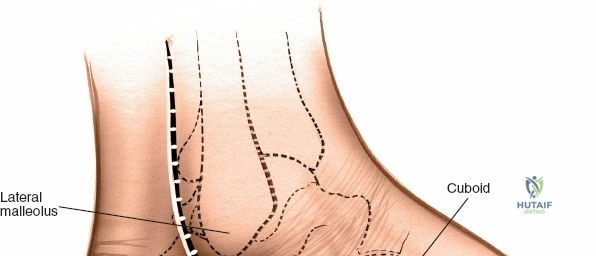
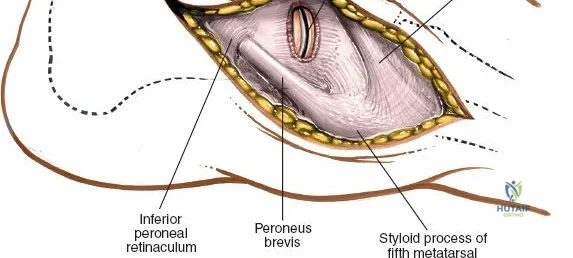
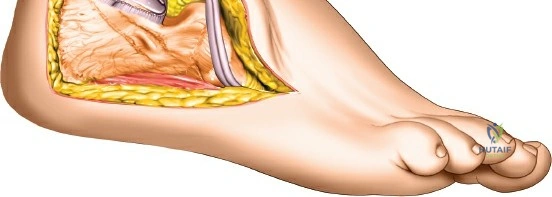
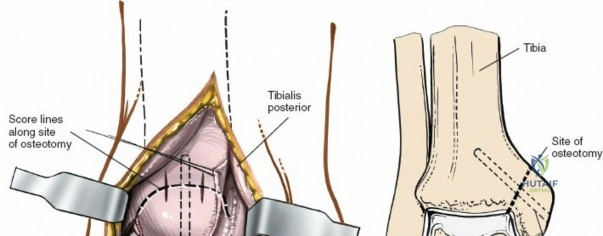
The posterior incision is utilized when access to the posterior aspect of the medial malleolus or the posterior malleolus itself is required. Make a 10-cm incision on the medial side of the ankle. Begin 5 cm above the ankle on the posterior border of the tibia, and curve the incision downward, following the posterior border of the medial malleolus. Curve the incision forward below the medial malleolus to end 5 cm distal to the malleolus, tracing the course of the tibialis posterior tendon.
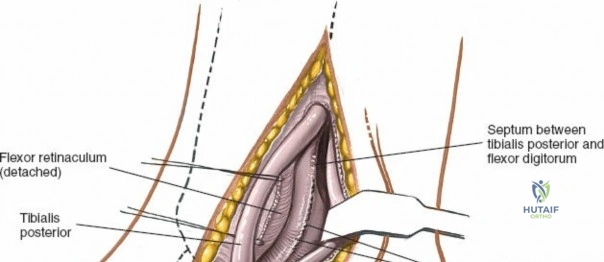
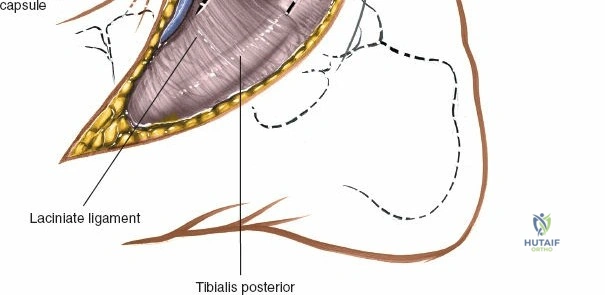
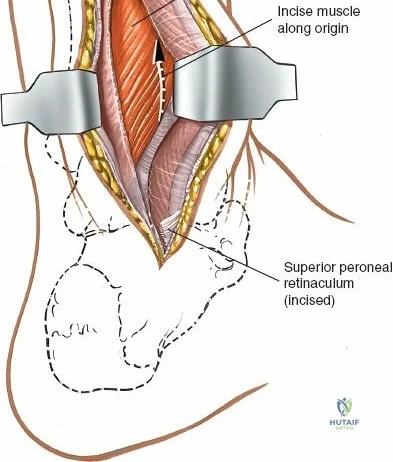
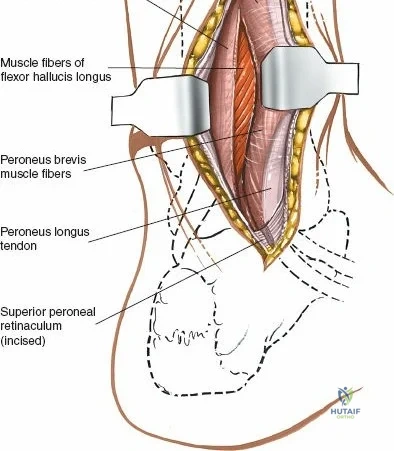
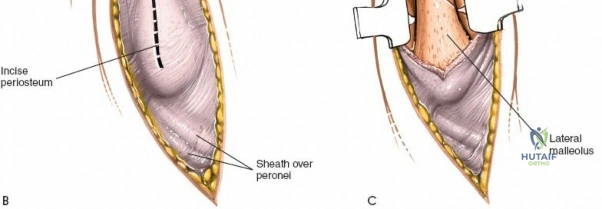
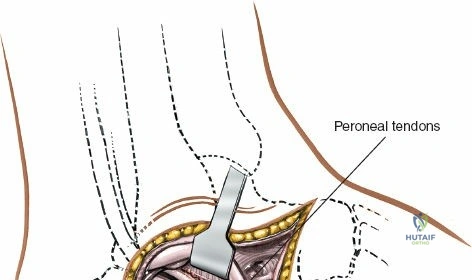
Superficial dissection involves elevating the skin flaps. Because the incision is located posteriorly, the saphenous nerve and vein are generally not in danger, provided the anterior flap is not aggressively retracted. The primary structure at risk during the deep dissection of this approach is the tendon of the tibialis posterior muscle.
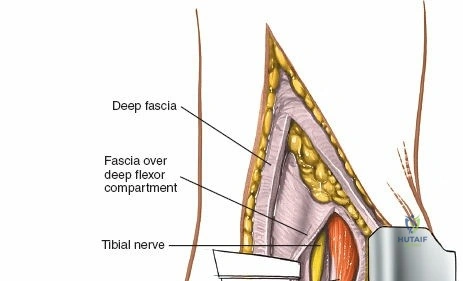
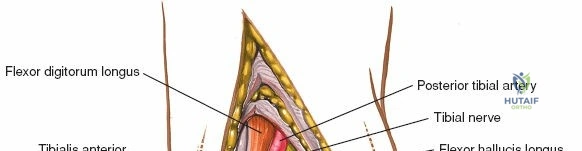
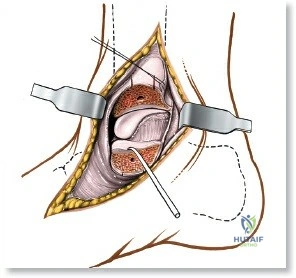
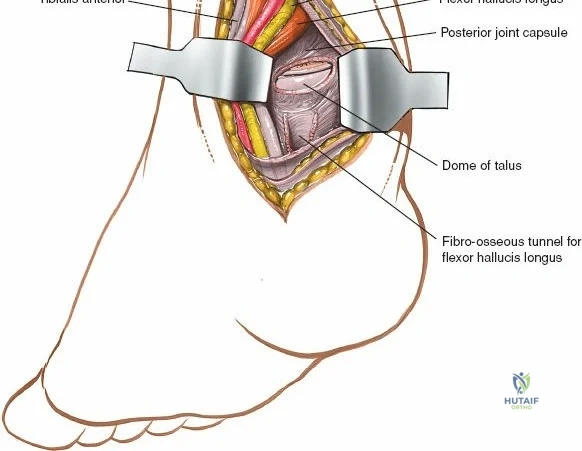
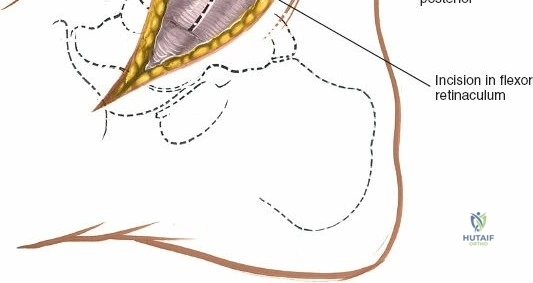
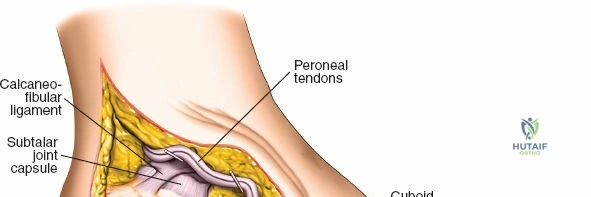
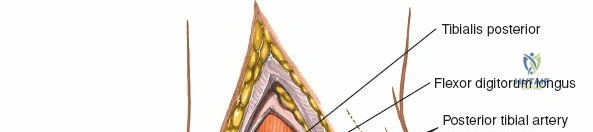
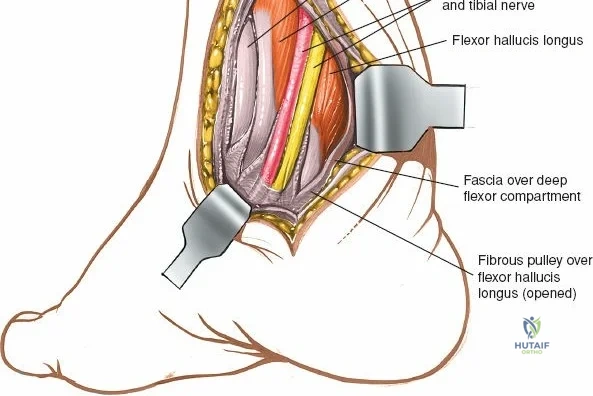
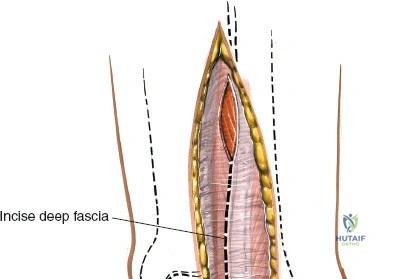
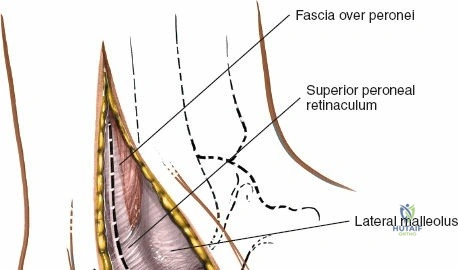
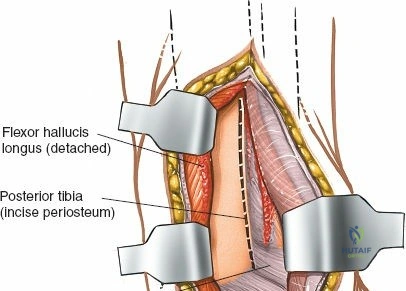
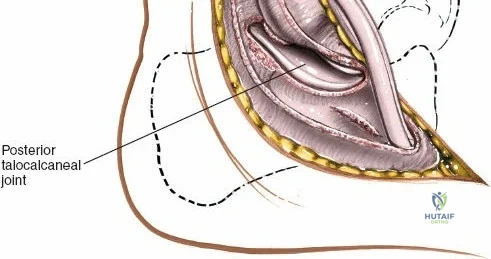
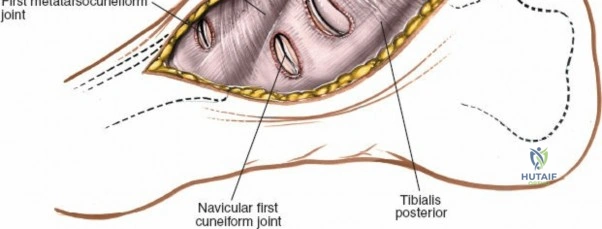
Incise the deep fascia and the flexor retinaculum (laciniate ligament) carefully. The tibialis posterior tendon lies immediately posterior to the medial malleolus in the most anterior compartment of the tarsal tunnel. Take care not to cut the tendon or aggressively strip its synovial sheath. Retract the tibialis posterior tendon posteriorly to expose the posterior aspect of the medial malleolus and the posterior tibial margin. If access to the posterior malleolus is required, further posterior retraction of the flexor digitorum longus (FDL) and the posterior tibial neurovascular bundle may be necessary, demanding extreme caution to prevent traction neuropraxia to the tibial nerve.
Complications, Incidence Rates, and Salvage Management
Surgical approaches to the dorsum of the foot and ankle are fraught with potential complications, primarily due to the unforgiving nature of the local soft tissue envelope. Wound healing complications, ranging from superficial dehiscence to full-thickness flap necrosis, are the most frequent and feared morbidities. The incidence of wound complications following the anterior approach for pilon fractures historically approached 15-20%, though modern staged protocols (spanning external fixation followed by delayed internal fixation) have reduced this. Marginal necrosis occurs due to excessive retractor tension, creating localized ischemia. Management of superficial dehiscence involves local wound care and oral antibiotics. However, full-thickness necrosis exposing tendons, neurovascular structures, or orthopedic implants is a surgical emergency. Salvage management requires aggressive serial debridement, utilization of negative pressure wound therapy (NPWT/VAC), and often necessitates complex soft tissue coverage, such as a rotational sural artery flap or a free anterolateral thigh (ALT) flap, executed in conjunction with microvascular plastic surgery teams.
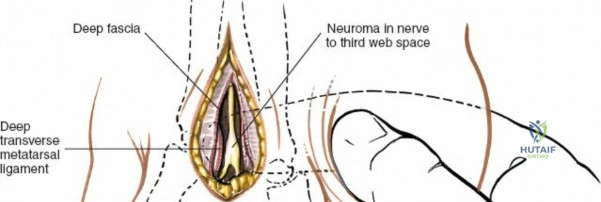
Iatrogenic nerve injury is another significant complication. The superficial peroneal nerve (SPN) is highly vulnerable during the initial skin incision of the anterior approach. Transection or aggressive traction leads to a painful terminal neuroma, which can be profoundly debilitating, preventing the patient from wearing standard footwear. The incidence of SPN injury ranges from 3% to 10% depending on the specific procedure. Similarly, the saphenous nerve is at risk during anterior medial malleolar approaches. Deep peroneal nerve entrapment or injury can occur during deep dissection or secondary to aggressive retraction, resulting in a first web space sensory deficit and potential extensor digitorum brevis weakness. Salvage for painful neuromas often involves surgical excision of the neuroma and burying the proximal nerve stump deep into local muscle bellies or bone to prevent recurrent surface irritation.

Vascular complications, particularly injury to the anterior tibial artery, can occur during the deep dissection of the anterior approach if the neurovascular bundle is not meticulously mobilized. While the foot possesses robust collateral circulation via the posterior tibial and peroneal arteries, inadvertent transection of the anterior tibial artery can compromise the viability of the anterior skin flaps and, in patients with pre-existing peripheral vascular disease, threaten the viability of the foot. If transected, primary microvascular repair should be attempted if feasible; otherwise, secure ligation is required, followed by close monitoring of distal perfusion.
| Complication Type | Estimated Incidence | Primary Etiology | Salvage Management Strategy |
|---|---|---|---|
| Superficial Dehiscence | 5 - 15% | Ischemia, early suture removal | Local wound care, prolonged immobilization |
| Deep Flap Necrosis | 2 - 5% | Aggressive retraction, smoking, DM | Serial debridement, NPWT, Free Tissue Transfer |
| SPN Neuroma | 3 - 10% | Iatrogenic transection/traction | Neuroma excision, proximal stump burying |
| Deep Infection (Septic Joint) | 1 - 3% | Contiguous spread from wound | I&D, hardware removal (if united), IV antibiotics |